
Treatment Outcomes of Tocilizumab in Critically-Ill COVID-19 Patients, Single-Centre Retrospective Study

 ,
, 
 , and
, and
Abstract
:1. Introduction
2. Results
2.1. Demographic and Clinical Characteristics of the Study Population
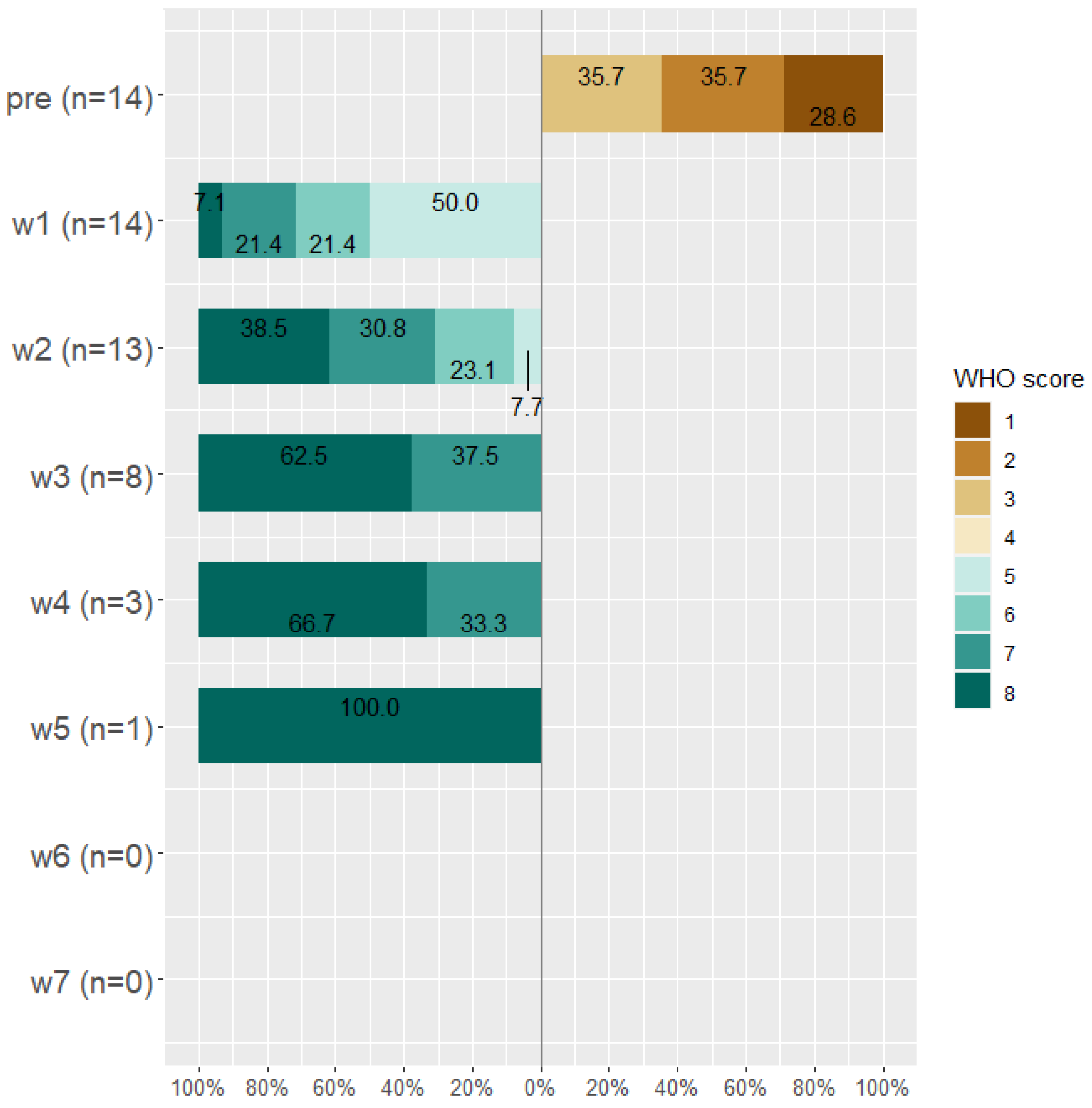
2.2. Classification of Patients before and after Treatment according to WHO Scale
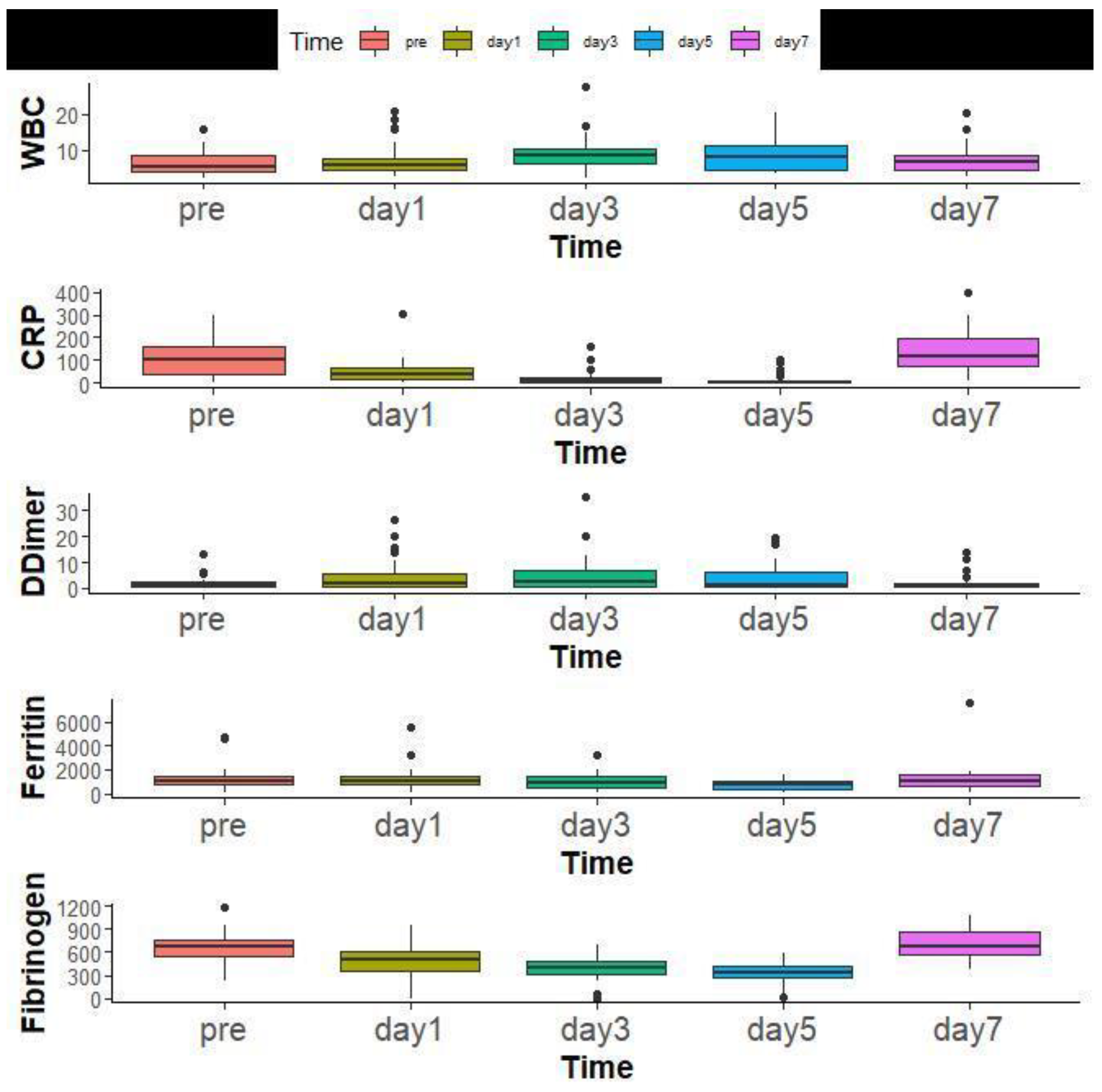
2.3. Laboratory Findings before and after Tocilizumab Therapy
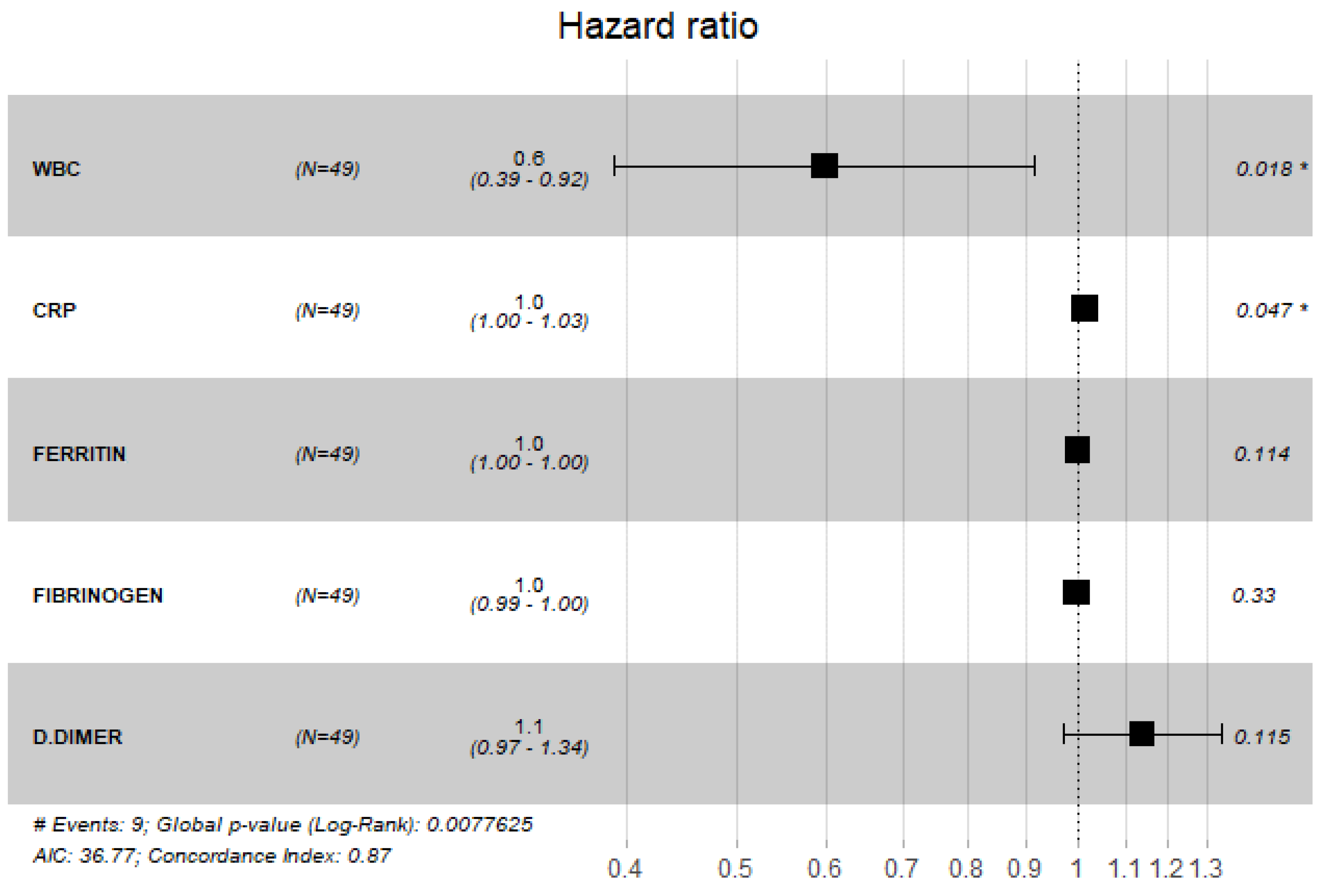
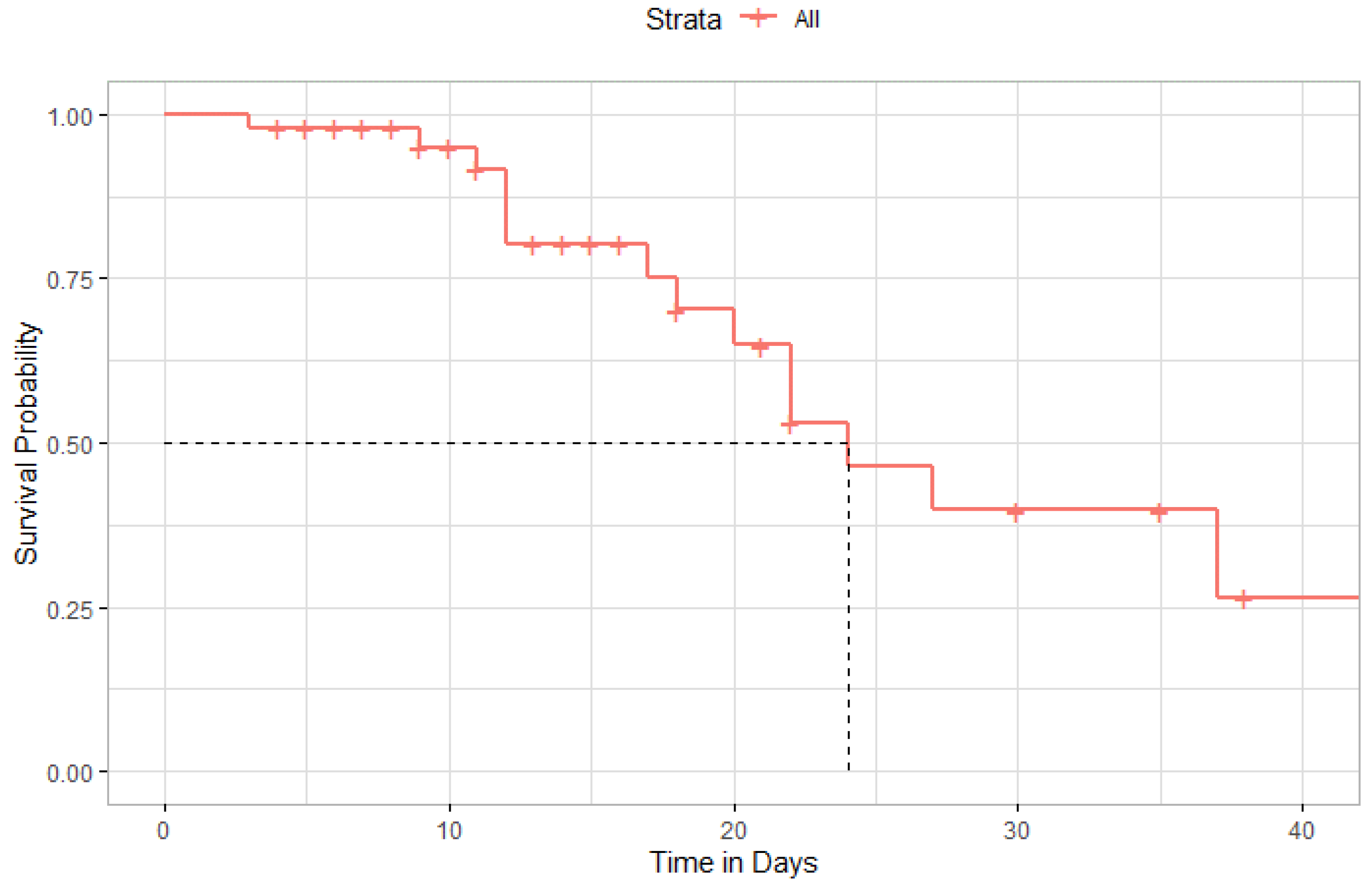
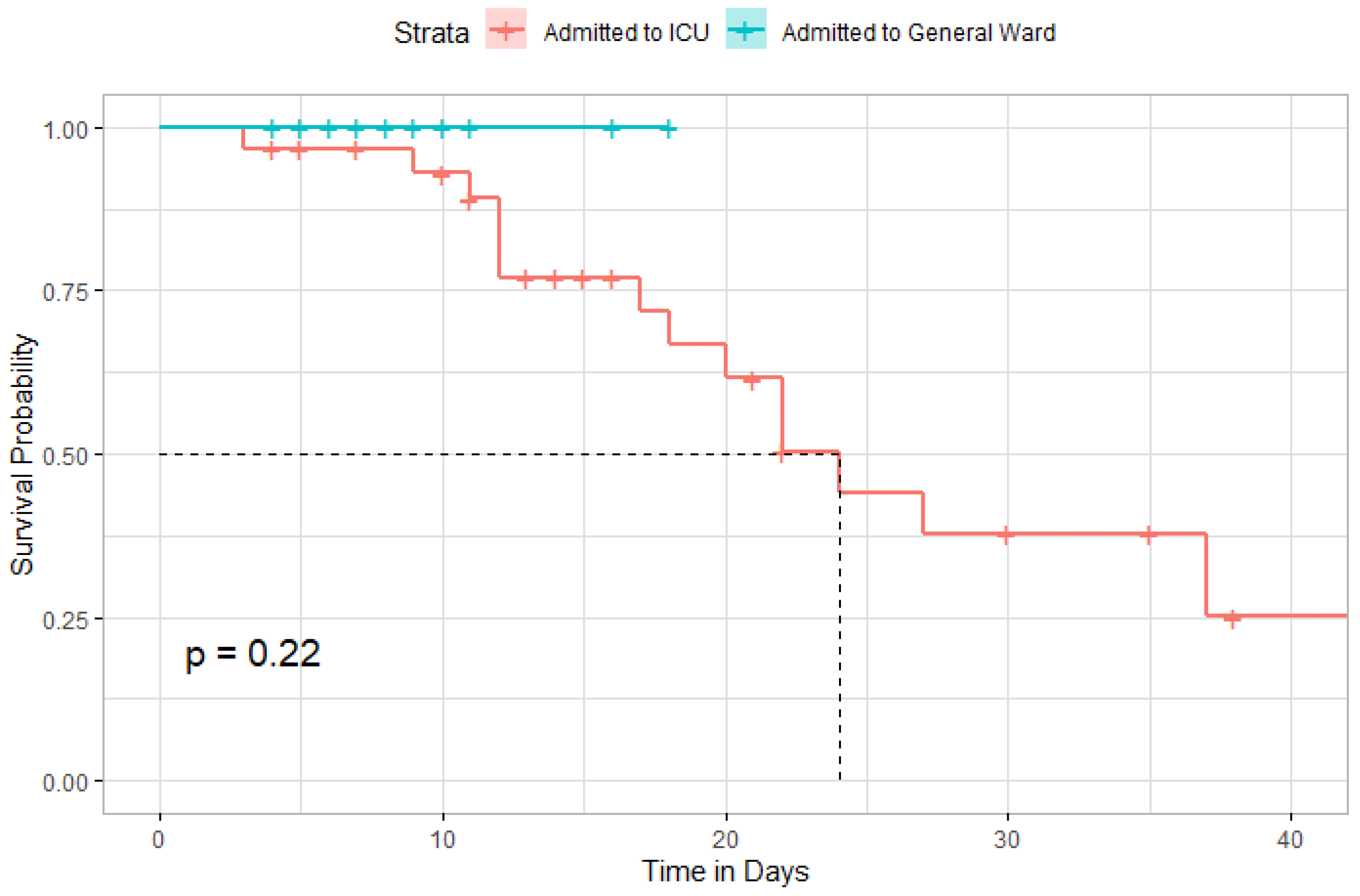
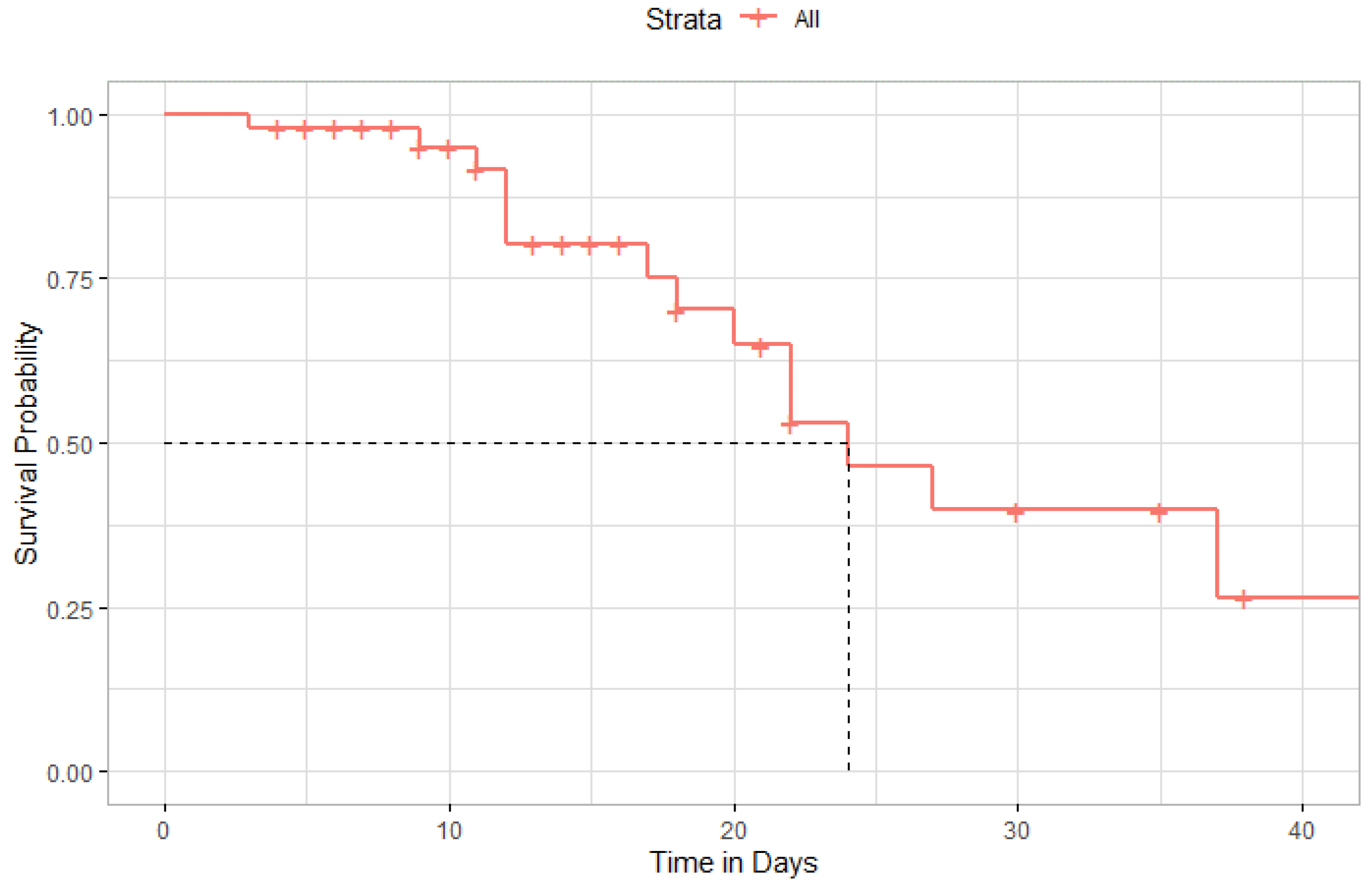
2.4. Kaplan–Meier Survival Curves after Tocilizumab Therapy
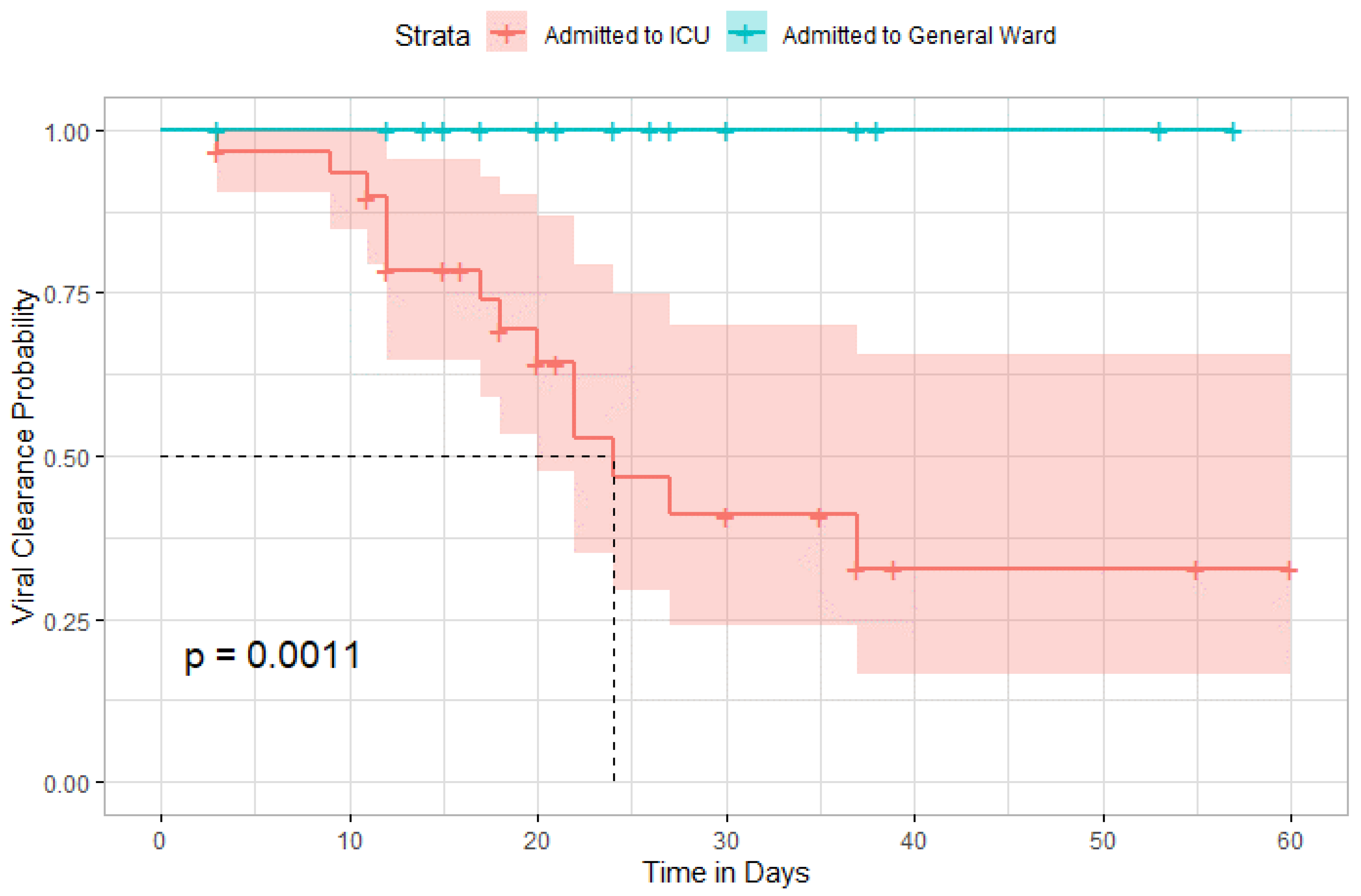
2.5. The Time until Viral Clearance between ICU Patients and General Ward
2.6. Safety Findings
3. Discussion
4. Materials and Methods
4.1. Institutional Review Board IRB
4.2. Study Design and Study Population
4.3. Treatment
4.4. Data Collection
4.5. Study Outcomes
4.6. Statistical Analysis
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Wang, C.; Horby, P.W.; Hayden, F.G.; Gao, G.F. A Novel Coronavirus Outbreak of Global Health Concern. Lancet 2020, 395, 470–473. [Google Scholar] [CrossRef] [Green Version]
- Huang, C.; Wang, Y.; Li, X.; Ren, L.; Zhao, J.; Hu, Y.; Zhang, L.; Fan, G.; Xu, J.; Gu, X.; et al. Clinical Features of Patients Infected with 2019 Novel Coronavirus in Wuhan, China. Lancet 2020, 395, 497–506. [Google Scholar] [CrossRef] [Green Version]
- Jin, Y.; Yang, H.; Ji, W.; Wu, W.; Chen, S.; Zhang, W.; Duan, G. Virology, Epidemiology, Pathogenesis, and Control of COVID-19. Viruses 2020, 12, 372. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pasrija, R.; Naime, M. The Deregulated Immune Reaction and Cytokines Release Storm (CRS) in COVID-19 Disease. Int. Immunopharmacol. 2021, 90, 107225. [Google Scholar] [CrossRef] [PubMed]
- Teachey, D.T.; Lacey, S.F.; Shaw, P.A.; Melenhorst, J.J.; Maude, S.L.; Frey, N.; Pequignot, E.; Gonzalez, V.E.; Chen, F.; Finklestein, J.; et al. Identification of Predictive Biomarkers for Cytokine Release Syndrome after Chimeric Antigen Receptor T-Cell Therapy for Acute Lymphoblastic Leukemia. Cancer Discov. 2016, 6, 664–679. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alrahmany, D.; Ghazi, I.M. Cytokine Storm Is the Cryptic Killer behind Coronavirus Disease-2019 Infections, Review of the Current Evidence to Identify Therapeutic Options. Rev. Res. Med. Microbiol. 2021, 32, 57–65. [Google Scholar] [CrossRef]
- Chen, G.; Wu, D.; Guo, W.; Cao, Y.; Huang, D.; Wang, H.; Wang, T.; Zhang, X.; Chen, H.; Yu, H.; et al. Clinical and Immunological Features of Severe and Moderate Coronavirus Disease 2019. J. Clin. Invest. 2020, 130, 2620–2629. [Google Scholar] [CrossRef] [Green Version]
- Chen, L.; Liu, H.G.; Liu, W.; Liu, J.; Liu, K.; Shang, J.; Deng, Y.; Wei, S. Analysis of clinical features of 29 patients with 2019 novel coronavirus pneumonia. Chin. J. Tuberc. Respir. Dis. 2020, 43, 203–208. [Google Scholar] [CrossRef]
- Wang, Z.; Yang, B.; Li, Q.; Wen, L.; Zhang, R. Clinical Features of 69 Cases With Coronavirus Disease 2019 in Wuhan, China. Clin. Infect. Dis. Off. Publ. Infect. Dis. Soc. Am. 2020, 71, 769–777. [Google Scholar] [CrossRef] [Green Version]
- Coomes, E.A.; Haghbayan, H. Interleukin-6 in Covid-19: A Systematic Review and Meta-analysis. Rev. Med. Virol. 2020, 30, e2141. [Google Scholar] [CrossRef]
- Tanaka, T.; Narazaki, M.; Kishimoto, T. IL-6 in Inflammation, Immunity, and Disease. Cold Spring Harb. Perspect. Biol. 2014, 6, a016295. [Google Scholar] [CrossRef] [PubMed]
- Gabay, C. Interleukin-6 and Chronic Inflammation. Arthritis Res. Ther. 2006, 8, S3. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, C.; Wu, Z.; Li, J.-W.; Zhao, H.; Wang, G.-Q. Cytokine Release Syndrome in Severe COVID-19: Interleukin-6 Receptor Antagonist Tocilizumab May Be the Key to Reduce Mortality. Int. J. Antimicrob. Agents 2020, 55, 105954. [Google Scholar] [CrossRef]
- Rose-John, S. IL-6 Trans-Signaling via the Soluble IL-6 Receptor: Importance for the Pro-Inflammatory Activities of IL-6. Int. J. Biol. Sci. 2012, 8, 1237–1247. [Google Scholar] [CrossRef]
- Su, H.; Lei, C.-T.; Zhang, C. Interleukin-6 Signaling Pathway and Its Role in Kidney Disease: An Update. Front. Immunol. 2017, 8, 405. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, W.; Ye, L.; Ye, L.; Li, B.; Gao, B.; Zeng, Y.; Kong, L.; Fang, X.; Zheng, H.; Wu, Z.; et al. Up-Regulation of IL-6 and TNF-Alpha Induced by SARS-Coronavirus Spike Protein in Murine Macrophages via NF-KappaB Pathway. Virus Res. 2007, 128, 1–8. [Google Scholar] [CrossRef]
- Thachil, J.; Tang, N.; Gando, S.; Falanga, A.; Cattaneo, M.; Levi, M.; Clark, C.; Iba, T. ISTH Interim Guidance on Recognition and Management of Coagulopathy in COVID-19. J. Thromb. Haemost. JTH 2020, 18, 1023–1026. [Google Scholar] [CrossRef]
- Calabrese, L.H.; Rose-John, S. IL-6 Biology: Implications for Clinical Targeting in Rheumatic Disease. Nat. Rev. Rheumatol. 2014, 10, 720–727. [Google Scholar] [CrossRef]
- Garbers, C.; Aparicio-Siegmund, S.; Rose-John, S. The IL-6/Gp130/STAT3 Signaling Axis: Recent Advances towards Specific Inhibition. Curr. Opin. Immunol. 2015, 34, 75–82. [Google Scholar] [CrossRef]
- Ogata, A.; Kato, Y.; Higa, S.; Yoshizaki, K. IL-6 Inhibitor for the Treatment of Rheumatoid Arthritis: A Comprehensive Review. Mod. Rheumatol. 2019, 29, 258–267. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Song, S.-N.J.; Yoshizaki, K. Tocilizumab for Treating Rheumatoid Arthritis: An Evaluation of Pharmacokinetics/Pharmacodynamics and Clinical Efficacy. Expert Opin. Drug Metab. Toxicol. 2015, 11, 307–316. [Google Scholar] [CrossRef]
- Maude, S.L.; Barrett, D.; Teachey, D.T.; Grupp, S.A. Managing Cytokine Release Syndrome Associated with Novel T Cell-Engaging Therapies. Cancer J. Sudbury Mass 2014, 20, 119–122. [Google Scholar] [CrossRef] [PubMed]
- Sato, K.; Tsuchiya, M.; Saldanha, J.; Koishihara, Y.; Ohsugi, Y.; Kishimoto, T.; Bendig, M.M. Reshaping a Human Antibody to Inhibit the Interleukin 6-Dependent Tumor Cell Growth. Cancer Res. 1993, 53, 851–856. [Google Scholar]
- Kaly, L.; Rosner, I. Tocilizumab—A Novel Therapy for Non-Organ-Specific Autoimmune Diseases. Best Pract. Res. Clin. Rheumatol. 2012, 26, 157–165. [Google Scholar] [CrossRef] [PubMed]
- Xu, X.; Han, M.; Li, T.; Sun, W.; Wang, D.; Fu, B.; Zhou, Y.; Zheng, X.; Yang, Y.; Li, X.; et al. Effective Treatment of Severe COVID-19 Patients with Tocilizumab. Proc. Natl. Acad. Sci. USA 2020, 117, 10970–10975. [Google Scholar] [CrossRef]
- Campochiaro, C.; Della-Torre, E.; Cavalli, G.; De Luca, G.; Ripa, M.; Boffini, N.; Tomelleri, A.; Baldissera, E.; Rovere-Querini, P.; Ruggeri, A.; et al. Efficacy and Safety of Tocilizumab in Severe COVID-19 Patients: A Single-Centre Retrospective Cohort Study. Eur. J. Intern. Med. 2020, 76, 43–49. [Google Scholar] [CrossRef] [PubMed]
- Luo, P.; Liu, Y.; Qiu, L.; Liu, X.; Liu, D.; Li, J. Tocilizumab Treatment in COVID-19: A Single Center Experience. J. Med. Virol. 2020, 92, 814–818. [Google Scholar] [CrossRef] [PubMed]
- Guaraldi, G.; Meschiari, M.; Cozzi-Lepri, A.; Milic, J.; Tonelli, R.; Menozzi, M.; Franceschini, E.; Cuomo, G.; Orlando, G.; Borghi, V.; et al. Tocilizumab in Patients with Severe COVID-19: A Retrospective Cohort Study. Lancet Rheumatol. 2020, 2, e474–e484. [Google Scholar] [CrossRef]
- Klopfenstein, T.; Zayet, S.; Lohse, A.; Balblanc, J.-C.; Badie, J.; Royer, P.-Y.; Toko, L.; Mezher, C.; Kadiane-Oussou, N.J.; Bossert, M.; et al. Tocilizumab Therapy Reduced Intensive Care Unit Admissions and/or Mortality in COVID-19 Patients. Med. Mal. Infect. 2020, 50, 397–400. [Google Scholar] [CrossRef]
- Hermine, O.; Mariette, X.; Tharaux, P.-L.; Resche-Rigon, M.; Porcher, R.; Ravaud, P. CORIMUNO-19 Collaborative Group Effect of Tocilizumab vs Usual Care in Adults Hospitalized With COVID-19 and Moderate or Severe Pneumonia: A Randomized Clinical Trial. JAMA Intern. Med. 2021, 181, 32–40. [Google Scholar] [CrossRef]
- Salvarani, C.; Dolci, G.; Massari, M.; Merlo, D.F.; Cavuto, S.; Savoldi, L.; Bruzzi, P.; Boni, F.; Braglia, L.; Turrà, C.; et al. Effect of Tocilizumab vs Standard Care on Clinical Worsening in Patients Hospitalized With COVID-19 Pneumonia: A Randomized Clinical Trial. JAMA Intern. Med. 2021, 181, 24–31. [Google Scholar] [CrossRef] [PubMed]
- Sciascia, S.; Aprà, F.; Baffa, A.; Baldovino, S.; Boaro, D.; Boero, R.; Bonora, S.; Calcagno, A.; Cecchi, I.; Cinnirella, G.; et al. Pilot Prospective Open, Single-Arm Multicentre Study on off-Label Use of Tocilizumab in Patients with Severe COVID-19. Clin. Exp. Rheumatol. 2020, 38, 529–532. [Google Scholar] [PubMed]
- Tomasiewicz, K.; Piekarska, A.; Stempkowska-Rejek, J.; Serafińska, S.; Gawkowska, A.; Parczewski, M.; Niścigorska-Olsen, J.; Łapiński, T.W.; Zarębska-Michaluk, D.; Kowalska, J.D.; et al. Tocilizumab for Patients with Severe COVID-19: A Retrospective, Multi-Center Study. Expert Rev. Anti Infect. Ther. 2021, 19, 93–100. [Google Scholar] [CrossRef] [PubMed]
- Corominas, H.; Castellví, I.; Pomar, V.; Antonijoan, R.; Mur, I.; Matas, L.; Gich, I.; de Benito, N.; Laiz, A.; Castillo, D.; et al. Effectiveness and Safety of Intravenous Tocilizumab to Treat COVID-19-Associated Hyperinflammatory Syndrome: Covizumab-6 Observational Cohort. Clin. Immunol. 2021, 223, 108631. [Google Scholar] [CrossRef] [PubMed]
- Atallah, B.; El Nekidy, W.; Mallah, S.I.; Cherfan, A.; AbdelWareth, L.; Mallat, J.; Hamed, F. Thrombotic Events Following Tocilizumab Therapy in Critically Ill COVID-19 Patients: A Façade for Prognostic Markers. Thromb. J. 2020, 18, 22. [Google Scholar] [CrossRef]
- Stone, R.L.; Nick, A.M.; McNeish, I.A.; Balkwill, F.; Han, H.D.; Bottsford-Miller, J.; Rupairmoole, R.; Armaiz-Pena, G.N.; Pecot, C.V.; Coward, J.; et al. Paraneoplastic Thrombocytosis in Ovarian Cancer. N. Engl. J. Med. 2012, 366, 610–618. [Google Scholar] [CrossRef] [Green Version]
- Zhang, Y.; Zhang, Z.; Wei, R.; Miao, X.; Sun, S.; Liang, G.; Chu, C.; Zhao, L.; Zhu, X.; Guo, Q.; et al. IL (Interleukin)-6 Contributes to Deep Vein Thrombosis and Is Negatively Regulated by MiR-338-5p. Arterioscler. Thromb. Vasc. Biol. 2020, 40, 323–334. [Google Scholar] [CrossRef]
- Jewell, P.; Ansorge, O.; Kuker, W.; Irani, S.R.; Zamboni, G. Tocilizumab-Associated Multifocal Cerebral Thrombotic Microangiopathy. Neurol. Clin. Pract. 2016, 6, e24–e26. [Google Scholar] [CrossRef] [Green Version]
- Nosaka, M.; Ishida, Y.; Kimura, A.; Kuninaka, Y.; Taruya, A.; Ozaki, M.; Tanaka, A.; Mukaida, N.; Kondo, T. Crucial Involvement of IL-6 in Thrombus Resolution in Mice via Macrophage Recruitment and the Induction of Proteolytic Enzymes. Front. Immunol. 2019, 10, 3150. [Google Scholar] [CrossRef]
- The ATTACC, ACTIV-4a, and REMAP-CAP Investigators. Therapeutic Anti-coagulation with Heparin in Noncritically Ill Patients with Covid-19. N. Engl. J. Med. 2021, 385, 790–802. [Google Scholar] [CrossRef]
- Spyropoulos, A.C.; Goldin, M.; Giannis, D.; Diab, W.; Wang, J.; Khanijo, S.; Mignatti, A.; Gianos, E.; Cohen, M.; Sharifova, G.; et al. Efficacy and Safety of Therapeutic-Dose Heparin vs Standard Prophylactic or Intermediate-Dose Heparins for Thromboprophylaxis in High-Risk Hospitalized Patients With COVID-19: The HEP-COVID Randomized Clinical Trial. JAMA Intern. Med. 2021, 181, 1612–1620. [Google Scholar] [CrossRef]
- Sholzberg, M.; Tang, G.H.; Rahhal, H.; AlHamzah, M.; Kreuziger, L.B.; Áinle, F.N.; Alomran, F.; Alayed, K.; Alsheef, M.; AlSumait, F.; et al. Effectiveness of Therapeutic Heparin versus Prophylactic Heparin on Death, Mechanical Ventilation, or Intensive Care Unit Admission in Moderately Ill Patients with Covid-19 Admitted to Hospital: RAPID Randomised Clinical Trial. BMJ 2021, 375, n2400. [Google Scholar] [CrossRef] [PubMed]
- Lopes, R.D.; de Barros E Silva, P.G.M.; Furtado, R.H.M.; Macedo, A.V.S.; Bronhara, B.; Damiani, L.P.; Barbosa, L.M.; de Aveiro Morata, J.; Ramacciotti, E.; de Aquino Martins, P.; et al. Therapeutic versus Prophylactic Anti-coagulation for Patients Admitted to Hospital with COVID-19 and Elevated D-Dimer Concentration (ACTION): An Open-Label, Multicentre, Randomised, Controlled Trial. Lancet 2021, 397, 2253–2263. [Google Scholar] [CrossRef]
- The REMAP-CAP, ACTIV-4a, and ATTACC Investigators. Therapeutic Anti-coagulation with Heparin in Critically Ill Patients with Covid-19. N. Engl. J. Med. 2021, 385, 777–789. [Google Scholar] [CrossRef]
- Gupta, S.; Wang, W.; Hayek, S.S.; Chan, L.; Mathews, K.S.; Melamed, M.L.; Brenner, S.K.; Leonberg-Yoo, A.; Schenck, E.J.; Radbel, J.; et al. Association Between Early Treatment With Tocilizumab and Mortality Among Critically Ill Patients With COVID-19. JAMA Intern. Med. 2021, 181, 41–51. [Google Scholar] [CrossRef] [PubMed]
- Quartuccio, L.; Sonaglia, A.; McGonagle, D.; Fabris, M.; Peghin, M.; Pecori, D.; De Monte, A.; Bove, T.; Curcio, F.; Bassi, F.; et al. Profiling COVID-19 Pneumonia Progressing into the Cytokine Storm Syndrome: Results from a Single Italian Centre Study on Tocilizumab versus Standard of Care. J. Clin. Virol. 2020, 129, 104444. [Google Scholar] [CrossRef]
- Antinori, S.; Bonazzetti, C.; Gubertini, G.; Capetti, A.; Pagani, C.; Morena, V.; Rimoldi, S.; Galimberti, L.; Sarzi-Puttini, P.; Ridolfo, A.L. Tocilizumab for Cytokine Storm Syndrome in COVID-19 Pneumonia: An Increased Risk for Candidemia? Autoimmun. Rev. 2020, 19, 102564. [Google Scholar] [CrossRef]
- Van Vught, L.A.; Klein Klouwenberg, P.M.C.; Spitoni, C.; Scicluna, B.P.; Wiewel, M.A.; Horn, J.; Schultz, M.J.; Nürnberg, P.; Bonten, M.J.M.; Cremer, O.L.; et al. Incidence, Risk Factors, and Attributable Mortality of Secondary Infections in the Intensive Care Unit After Admission for Sepsis. JAMA 2016, 315, 1469–1479. [Google Scholar] [CrossRef] [Green Version]
- Beumer, M.C.; Koch, R.M.; van Beuningen, D.; OudeLashof, A.M.; van de Veerdonk, F.L.; Kolwijck, E.; van der Hoeven, J.G.; Bergmans, D.C.; Hoedemaekers, C.W.E. Influenza Virus and Factors That Are Associated with ICU Admission, Pulmonary Co-Infections and ICU Mortality. J. Crit. Care 2019, 50, 59–65. [Google Scholar] [CrossRef]
- Vikse, J.; Henry, B.M. Tocilizumab in COVID-19: Beware the Risk of Intestinal Perforation. Int. J. Antimicrob. Agents 2020, 56, 106009. [Google Scholar] [CrossRef]
- Serviddio, G.; Villani, R.; Stallone, G.; Scioscia, G.; Foschino-Barbaro, M.P.; Lacedonia, D. Tocilizumab and Liver Injury in Patients with COVID-19. Ther. Adv. Gastroenterol. 2020, 13, 1756284820959183. [Google Scholar] [CrossRef]
- Tanaka, T.; Narazaki, M.; Kishimoto, T. Immunotherapeutic Implications of IL-6 Blockade for Cytokine Storm. Immunotherapy 2016, 8, 959–970. [Google Scholar] [CrossRef]
- Shang, J.; Wan, Y.; Luo, C.; Ye, G.; Geng, Q.; Auerbach, A.; Li, F. Cell Entry Mechanisms of SARS-CoV-2. Proc. Natl. Acad. Sci. USA 2020, 117, 11727–11734. [Google Scholar] [CrossRef] [PubMed]
- Aleksova, A.; Gagno, G.; Sinagra, G.; Beltrami, A.P.; Janjusevic, M.; Ippolito, G.; Zumla, A.; Fluca, A.L.; Ferro, F. Effects of SARS-CoV-2 on Cardiovascular System: The Dual Role of Angiotensin-Converting Enzyme 2 (ACE2) as the Virus Receptor and Homeostasis Regulator-Review. Int. J. Mol. Sci. 2021, 22, 4526. [Google Scholar] [CrossRef] [PubMed]
- Mishra, H.K.; Ma, J.; Walcheck, B. Ectodomain Shedding by ADAM17: Its Role in Neutrophil Recruitment and the Impairment of This Process during Sepsis. Front. Cell. Infect. Microbiol. 2017, 7, 138. [Google Scholar] [CrossRef]
- Patra, T.; Meyer, K.; Geerling, L.; Isbell, T.S.; Hoft, D.F.; Brien, J.; Pinto, A.K.; Ray, R.B.; Ray, R. SARS-CoV-2 Spike Protein Promotes IL-6 Trans-Signaling by Activation of Angiotensin II Receptor Signaling in Epithelial Cells. PLoS Pathog. 2020, 16, e1009128. [Google Scholar] [CrossRef]
- Lin, L.; Liu, Y.; Tang, X.; He, D. The Disease Severity and Clinical Outcomes of the SARS-CoV-2 Variants of Concern. Front. Public Health 2021, 9, 775224. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | Overall (n = 49) | Improved or Stable (n = 35) (1) | Worsened or Deceased (n = 14) (1) | p-Value (2) |
|---|---|---|---|---|
| Age | 47 (41, 58) | 45 (40, 54) | 60 (47, 66) | 0.013 |
| SEX | 0.7 | |||
| Female | 8 (16%) | 5 (14%) | 3 (21%) | |
| Male | 41 (84%) | 30 (86%) | 11 (79%) | |
| Race/ethnicity | 0.3 | |||
| Asian | 31 (63%) | 24 (69%) | 7 (50%) | |
| Black | 2 (4.1%) | 1 (2.9%) | 1 (7.1%) | |
| White | 16 (33%) | 10 (29%) | 6 (43%) | |
| Hypertension | 0.031 | |||
| NIL | 4 (8.2%) | 3 (8.6%) | 1 (7.1%) | |
| No | 27 (55%) | 23 (66%) | 4 (29%) | |
| Yes | 18 (37%) | 9 (26%) | 9 (64%) | |
| Diabetes Mellitus | 0.5 | |||
| NIL | 4 (8.2%) | 3 (8.6%) | 1 (7.1%) | |
| No | 27 (55%) | 21 (60%) | 6 (43%) | |
| Yes | 18 (37%) | 11 (31%) | 7 (50%) | |
| Cardiovascular Diseases | 0.4 | |||
| NIL | 6 (12%) | 3 (8.6%) | 3 (21%) | |
| No | 34 (69%) | 26 (74%) | 8 (57%) | |
| Yes | 9 (18%) | 6 (17%) | 3 (21%) | |
| BMI | 25 (13, 33) | 25 (12, 34) | 24 (16, 28) | 0.6 |
| WHO scale before receiving Tocilizumab | 0.005 | |||
| 4 | 26 (53%) | 22 (63%) | 4 (29%) | |
| 5 | 17 (35%) | 12 (34%) | 5 (36%) | |
| 6 | 6 (12%) | 1 (2.9%) | 5 (36%) | |
| Time to viral Clearance (from first positive till first negative) | 20 (12, 27) | 20 (15, 32) | 18 (12, 22) | 0.2 |
| Drugs Taken by Patients | Overall (n = 49) (1) | Improved or Stable (n = 35) (1) | Worsened or Deceased (n = 14) (1) | p-Value (2) |
|---|---|---|---|---|
| HCQ Azithromycin | 4 (8%) | 4 (11.5%) | 0 (0%) | 0.3 |
| HCQ Favipiravir | 23 (47%) | 16 (46%) | 7 (50%) | 0.9 |
| HCQ. Azithromycin Favipiravir | 11 (22%) | 7 (20%) | 4 (28.5%) | >0.9 |
| HCQ Favipiravir Lopinavir/Ritonavir | 6 (12%) | 4 (11.5%) | 2 (14%) | >0.9 |
| HCQ. Favipiravir Lopinavir/Ritonavir Azithromycin | 4 (8%) | 4 (11.5%) | 0 (0%) |
| Laboratory Findings (Median, IQR) | Before Tocilizumab (n = 47) | Day 1 (n = 47) | Day 3 (n = 47) | Day 5 (n = 47) | Day 7 (n = 47) | Total | p-Value |
|---|---|---|---|---|---|---|---|
| Hemoglobin Level (g/L) | 13.7 (9.00, 16.7) | 13.2 (7.80, 16.1) | 12.6 (8.20, 16.2) | 12.7 (6.30, 15.7) | 13.1 (7.30, 16.5) | 13.2 (6.30, 16.7) | 0.546 |
| White Blood Cell Count (×109/L) | 6.79 (2.40, 20.3) | 5.30 (2.10, 15.8) | 5.47 (2.31, 20.8) | 8.57 (2.21, 27.6) | 8.60 (3.39, 20.9) | 6.72 (2.10, 27.6) | 0.007 |
| Neutrophils (×109/L) | 75.1 (35.5, 95.0) | 74.0 (24.6, 93.2) | 69.7 (20.5, 92.3) | 71.6 (31.4, 94.3) | 63.1 (17.4, 94.6) | 72.6 (17.4, 95.0) | 0.599 |
| Lymphocytes (×109/L) | 18.8 (2.20, 52.6) | 18.4 (3.50, 65.2) | 18.8 (4.60, 70.8) | 16.9 (3.40, 58.2) | 24.7 (3.50, 63.4) | 18.8 (2.20, 70.8) | 0.818 |
| Neutrophil–Lymphocyte Ratio | 4.10 (0.600, 43.1) | 4.00 (0.300, 26.6) | 3.60 (0.290, 19.5) | 4.20 (0.540, 27.7) | 2.50 (0.200, 27.0) | 3.80 (0.200, 43.1) | 0.801 |
| C-Reactive Protein (mg/L) | 120 (12.0, 400) | 109 (2.00, 302) | 39.0 (4.00, 302) | 10.5 (0.310, 164) | 4.50 (0.150, 102) | 39.0 (0.150, 400) | <0.001 |
| D-Dimer (ng/mL) | 0.940 (0.140, 14.1) | 1.15 (0.200, 13.5) | 1.95 (0.150, 26.6) | 2.49 (0.270, 35.2) | 1.22 (0.100, 19.3) | 1.21 (0.100, 35.2) | 0.017 |
| Ferritin (ng/mL) | 1000 (120, 7620) | 1080 (145, 4750) | 1010 (74.4, 5520) | 921 (73.6, 3180) | 704 (49.8, 1650) | 932 (49.8, 7620) | 0.032 |
| Lactate Dehydrogenase (U/L) | 434 (194, 1390) | 472 (271, 1080) | 531 (207, 1550) | 430 (270, 1720) | 361 (83.0, 2530) | 454 (83.0, 2530) | 0.241 |
| Fibrinogen (mg/dL) | 664 (370, 1100) | 667 (235, 1180) | 514 (5.28, 973) | 402 (3.40, 711) | 334 (17.6, 636) | 514 (3.40, 1180) | <0.001 |
| Laboratory Findings for Improved Patients | Before Toci. (n = 34) (1) | Day 1 after Toci. (n = 34) (1) | Day 3 after Toci. (n = 34) (1) | Day 5 after Toci. (n = 34) (1) | Day 7 after Toci. (n = 34) (1) | p-Value (2) |
|---|---|---|---|---|---|---|
| Haemoglobin(g/L) | 13.80 (12.30, 14.38) | 13.20 (11.90, 14.00) | 13.20 (12.05, 13.83) | 13.70 (11.80, 14.10) | 13.15 (12.07, 14.53) | 0.8 |
| White blood cells count (×109/L) | 6.8 (4.0, 8.1) | 5.6 (3.9, 9.4) | 5.7 (4.0, 10.0) | 8.6 (6.0, 12.2) | 7.3 (5.0, 10.6) | 0.063 |
| Neutrophils count (×109/L) | 74 (58, 84) | 74 (63, 81) | 68 (54, 80) | 71 (57, 82) | 60 (42, 80) | 0.4 |
| Lymphocytes Count (×109/L) | 20 (10, 35) | 18 (12, 28) | 20 (14, 32) | 17 (11, 28) | 29 (12, 44) | 0.5 |
| Neutrophil Lymphocyte ratio | 3.7 (1.5, 8.3) | 4.0 (2.3, 6.6) | 3.5 (1.7, 5.5) | 4.2 (2.0, 7.8) | 2.0 (0.9, 7.1) | 0.5 |
| C-reactive protein (mg/L) | 119 (70, 197) | 106 (40, 146) | 39 (17, 64) | 13 (4, 23) | 4 (4, 12) | <0.001 |
| D-Dimer (ng/mL) | 0.9 (0.5, 2.2) | 1.1 (0.6, 2.0) | 1.7 (0.8, 6.1) | 1.8 (0.5, 4.3) | 0.8 (0.3, 3.8) | 0.088 |
| Ferritin (ng/mL) | 1000 (437, 1644) | 996 (670, 1491) | 950 (714, 1381) | 891 (527, 1353) | 639 (382, 945) | 0.046 |
| Lactate dehydrogenase (U/L) | 420 (375, 512) | 456 (383, 579) | 505 (395, 593) | 406 (340, 540) | 309 (266, 583) | 0.05 |
| Fibrinogen (mg/dL) | 644 (574, 833) | 672 (526, 741) | 514 (417, 595) | 419 (319, 480) | 347 (278, 453) | <0.001 |
| Laboratory Findings for Worsened Cases | Before Toci (n = 13) (1) | Day 1 after Toci (n = 13) (1) | Day 3 after Toci (n = 13) (1) | Day 5 after Toci (n = 13) (1) | Day 7 after Toci (n = 13) (1) | p-Value (2) |
|---|---|---|---|---|---|---|
| Haemoglobin (g/L) | 13.40 (12.50, 13.90) | 12.50 (11.30, 13.70) | 12.00 (11.23, 13.12) | 12.55 (11.60, 13.75) | 12.55 (10.83, 13.40) | 0.6 |
| White blood cells count (×109/L) | 6.8 (4.6, 9.9) | 4.6 (4.2, 6.7) | 5.4 (4.5, 6.7) | 7.6 (4.0, 9.7) | 9.6 (4.4, 13.2) | 0.3 |
| Neutrophils count (×109/L) | 78 (70, 86) | 75 (65, 78) | 78 (66, 81) | 70 (54, 74) | 69 (50, 86) | 0.6 |
| Lymphocytes Count (×109/L) | 15 (10, 24) | 19 (16, 26) | 16 (14, 26) | 19 (14, 35) | 21 (10, 34) | 0.8 |
| Neutrophils lymphocytes ratio | 5.0 (2.8, 8.3) | 4.0 (2.4, 4.7) | 4.8 (2.5, 5.9) | 3.5 (1.5, 5.5) | 3.6 (1.5, 8.4) | 0.8 |
| C-reactive protein (mg/L) | 125 (81, 191) | 119 (74, 171) | 39 (25, 58) | 8 (4, 28) | 4 (4, 14) | <0.001 |
| D-Dimer (ng/mL) | 1.0 (0.5, 1.3) | 1.2 (0.6, 2.5) | 2.5 (1.0, 5.3) | 4.0 (0.9, 8.7) | 2.2 (0.7, 12.2) | 0.2 |
| Ferritin (ng/mL) | 858 (742, 1304) | 1133 (863, 1469) | 1128 (854, 1485) | 938 (648, 1395) | 872 (642, 1040) | 0.4 |
| Lactate dehydrogenase (U/L) | 509 (455, 604) | 550 (469, 810) | 630 (411, 696) | 538 (378, 802) | 441 (319, 855) | >0.9 |
| Fibrinogen (mg/dL) | 671 (556, 860) | 629 (564, 790) | 544 (310, 639) | 400 (275, 457) | 294 (246, 356) | <0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hafez, W.; Ziade, M.A.; Arya, A.; Saleh, H.; Abdelshakor, M.; Fadl Alla, O.; Agrawal, P.; Ali, S.; Rao, S.R.; Gupta, S.; et al. Treatment Outcomes of Tocilizumab in Critically-Ill COVID-19 Patients, Single-Centre Retrospective Study. Antibiotics 2022, 11, 241. https://doi.org/10.3390/antibiotics11020241
Hafez W, Ziade MA, Arya A, Saleh H, Abdelshakor M, Fadl Alla O, Agrawal P, Ali S, Rao SR, Gupta S, et al. Treatment Outcomes of Tocilizumab in Critically-Ill COVID-19 Patients, Single-Centre Retrospective Study. Antibiotics. 2022; 11(2):241. https://doi.org/10.3390/antibiotics11020241
Chicago/Turabian StyleHafez, Wael, Mohamad Azzam Ziade, Arun Arya, Husam Saleh, Mahmoud Abdelshakor, Osman Fadl Alla, Pragati Agrawal, Sara Ali, Srinivasa Raghu Rao, Subrata Gupta, and et al. 2022. "Treatment Outcomes of Tocilizumab in Critically-Ill COVID-19 Patients, Single-Centre Retrospective Study" Antibiotics 11, no. 2: 241. https://doi.org/10.3390/antibiotics11020241
APA StyleHafez, W., Ziade, M. A., Arya, A., Saleh, H., Abdelshakor, M., Fadl Alla, O., Agrawal, P., Ali, S., Rao, S. R., Gupta, S., Abdelli, I., Sebastian, H., Ali, M., Gador, M., Al Baha, Z., & Abdelrahman, A. (2022). Treatment Outcomes of Tocilizumab in Critically-Ill COVID-19 Patients, Single-Centre Retrospective Study. Antibiotics, 11(2), 241. https://doi.org/10.3390/antibiotics11020241