
Impact of a Primary Care Antimicrobial Stewardship Program on Bacterial Resistance Control and Ecological Imprint in Urinary Tract Infections

 , , , , , , , , , , add
Show full author list
, , , , , , , , , , add
Show full author list
Abstract
1. Introduction
2. Materials and Methods
2.1. Design, Setting, and Study Periods
2.2. Sources of Information
2.3. Measurement of Consumption and Microbiological and Economic Impact
2.4. Evaluation Methods
2.5. Statistical Analysis
3. Results
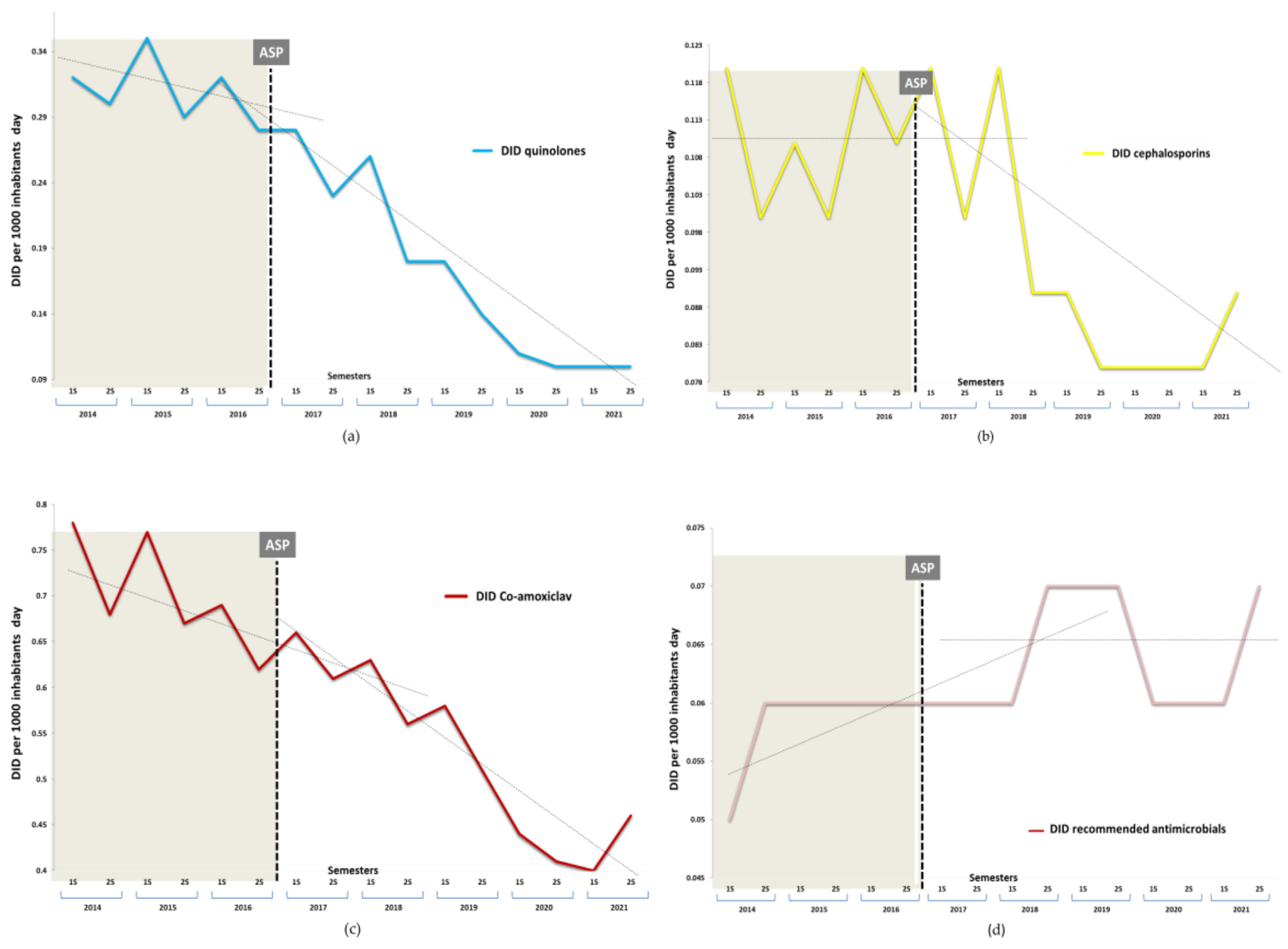
3.1. Impact of Antibiotic Consumption
3.2. Impact on Antimicrobial Resistance
3.3. Economic Impact
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Spellberg, B.; Guidos, R.; Gilbert, D.; Bradley, J.; Boucher, H.W.; Scheld, W.M.; Bartlett, J.G.; Edwards, J., Jr. The Infectious Diseases Society of America. The Epidemic of Antibiotic-Resistant Infections: A Call to Action for the Medical Community from the Infectious Diseases Society of America. Clin. Infect. Dis. 2008, 46, 155–164. [Google Scholar] [CrossRef]
- Antimicrobial Resistance Collaborators. Global burden of bacterial antimicrobial resistance in 2019: A systematic analysis. Lancet 2022, 399, 629–655. [Google Scholar] [CrossRef] [PubMed]
- Antimicrobial Resistance Collaborators. The burden of bacterial antimicrobial resistance in the WHO European region in 2019: A cross-country systematic analysis. Lancet Public Health 2022, 7, e897–e913. [Google Scholar] [CrossRef]
- Bell, B.G.; Schellevis, F.; Stobberingh, E.; Goossens, H.; Pringle, M. A systematic review and meta-analysis of the effects of antibiotic consumption on antibiotic resistance. BMC Infect. Dis. 2014, 14, 13. [Google Scholar] [CrossRef]
- Garau, J.; Nicolau, D.P.; Wullt, B.; Bassetti, M. Antibiotic stewardship challenges in the management of community-acquired infections for prevention of escalating antibiotic resistance. J. Glob. Antimicrob. Resist. 2014, 2, 245–253. [Google Scholar] [CrossRef] [PubMed]
- Dyar, O.J.; Huttner, B.; Schouten, J.; Pulcini, C.; ESGAP (ESCMID Study Group for Antimicrobial stewardship). What is antimicrobial stewardship? Clin. Microbiol. Infect. 2017, 23, 793–798. [Google Scholar] [CrossRef]
- Rice, L.B. Antimicrobial Stewardship and Antimicrobial Resistance. Med. Clin. N. Am. 2018, 102, 805–818. [Google Scholar] [CrossRef] [PubMed]
- Buckel, W.R.; Veillette, J.; Vento, T.J.; Stenehjem, E. Antimicrobial Stewardship in Community Hospitals. Med. Clin. North Am. 2018, 102, 913–928. [Google Scholar] [CrossRef]
- Davey, P.A.; Marwick, C.; Scott, C.L.; Charani, E.; McNeil, K.; Brown, E.; Gould, I.M.; Ramsay, C.R.; Michie, S. Interventions to improve antibiotic prescribing practices for hospital inpatients. Cochrane Database Syst. Rev. 2017, 2, CD003543. [Google Scholar] [CrossRef]
- Steinberg, D.I. Interventions improve hospital antibiotic prescribing and reduce hospital stay but do not affect mortality. Ann. Intern. Med. 2017, 166, JC59. [Google Scholar] [CrossRef] [PubMed]
- Baur, D.; Gladstone, B.P.; Burkert, F.; Carrara, E.; Foschi, F.; Döbele, S.; Tacconelli, E. Effect of antibiotic stewardship on the incidence of infection and colonisation with antibiotic-resistant bacteria and Clostridium difficile infection: A systematic review and meta-analysis. Lancet Infect. Dis. 2017, 17, 990–1001. [Google Scholar] [CrossRef]
- Fleming-Dutra, K.E.; Hersh, A.L.; Shapiro, D.J.; Bartoces, M.; Enns, E.A.; File, T.M., Jr.; Finkelstein, J.A.; Gerber, J.S.; Hyun, D.Y.; Linder, J.A.; et al. Prevalence of Inappropriate Antibiotic Prescriptions among US Ambulatory Care Visits, 2010–2011. JAMA 2016, 315, 1864–1873. [Google Scholar] [CrossRef]
- Hammond, A.; Stuijfzand, B.; Avison, M.B.; Hay, A.D. Antimicrobial resistance associations with national primary care antibiotic stewardship policy: Primary care-based, multilevel analytic study. PLoS ONE 2020, 15, e0232903. [Google Scholar] [CrossRef]
- Gágyor, I.; Hay, A.D. Outcome selection in primary care antimicrobial stewardship research. J. Antimicrob. Chemother. 2021, 77, 7–12. [Google Scholar] [CrossRef]
- Avent, M.L.; Cosgrove, S.E.; Price-Haywood, E.G.; Van Driel, M.L. Antimicrobial stewardship in the primary care setting: From dream to reality? BMC Fam. Pract. 2020, 21, 134. [Google Scholar] [CrossRef] [PubMed]
- Castanheira, M.; Simner, P.J.; Bradford, P.A. Extended-spectrum β-lactamases: An update on their characteristics, epidemiology and detection. JAC Antimicrob. Resist. 2021, 3, dlab092. [Google Scholar] [CrossRef]
- Bevan, E.R.; Jones, A.M.; Hawkey, P.M. Global epidemiology of CTX-M β-lactamases: Temporal and geographical shifts in genotype. J. Antimicrob. Chemother. 2017, 72, 2145–2155. [Google Scholar] [CrossRef]
- Cantón, R.; Loza, E.; Aznar, J.; Barrón-Adúriz, R.; Calvo, J.; Castillo, F.J.; Cercenado, E.; Cisterna, R.; González-Romo, F.; López-Hontangas, J.L.; et al. Antimicrobial susceptibility trends and evolution of isolates with extended spectrum β-lactamases among Gram-negative organisms recovered during the SMART study in Spain (2011–2015). Rev. Esp. Quimioter. 2018, 31, 136–145. [Google Scholar] [PubMed]
- Cantón, R.; Loza, E.; Aznar, J.; Castillo, F.J.; Cercenado, E.; Fraile-Ribot, P.A.; González-Romo, F.; López-Hontangas, J.L.; Rodríguez-Lozano, J.; Suárez-Barrenechea, A.I.; et al. Monitoring the antimicrobial susceptibility of Gram-negative organisms involved in intraabdominal and urinary tract infections recovered during the SMART study (Spain, 2016 and 2017). Rev. Esp. Quimioter. 2019, 32, 145–155. [Google Scholar] [PubMed]
- Fasugba, O.; Gardner, A.; Mitchell, B.G.; Mnatzaganian, G. Ciprofloxacin resistance in community- and hospital-acquired Escherichia coli urinary tract infections: A systematic review and meta-analysis of observational studies. BMC Infect. Dis. 2015, 15, 545. [Google Scholar] [CrossRef]
- Kurotschka, P.K.; Fulgenzio, C.; Da Cas, R.; Traversa, G.; Ferrante, G.; Massidda, O.; Gágyor, I.; Aschbacher, R.; Moser, V.; Pagani, E.; et al. Effect of Fluoroquinolone Use in Primary Care on the Development and Gradual Decay of Escherichia coli Resistance to Fluoroquinolones: A Matched Case-Control Study. Antibiotics 2022, 11, 822. [Google Scholar] [CrossRef]
- Wood, F.; Phillips, C.; Brookes-Howell, L.; Hood, K.; Verheij, T.; Coenen, S.; Little, P.; Melbye, H.; Godycki-Cwirko, M.; Jakobsen, K.; et al. Primary care clinicians’ perceptions of antibiotic resistance: A multi-country qualitative interview study. J. Antimicrob. Chemother. 2013, 68, 237–243. [Google Scholar] [CrossRef] [PubMed]
- Gupta, K.; Hooton, T.M.; Naber, K.G.; Wullt, B.; Colgan, R.; Miller, L.G.; Moran, G.J.; Nicolle, L.E.; Raz, R.; Schaeffer, A.J.; et al. International Clinical Practice Guidelines for the Treatment of Acute Uncomplicated Cystitis and Pyelonephritis in Women: A 2010 Update by the Infectious Diseases Society of America and the European Society for Microbiology and Infectious Diseases. Clin. Infect. Dis. 2011, 52, e103–e120. [Google Scholar] [CrossRef]
- Jover-Sáenz, A.; Ramírez-Hidalgo, M.F.; Vidal, M.V.; González, M.G.; Marrón, S.M.C.; Arias, A.E.; Sacrest, M.F.; Translational Research Group on Infectious Diseases of Lleida (Head Group, TRIDLE-IRBLleida); Castellana-Perelló, D.; Barcenilla-Gaite, F. Antimicrobial stewardship program at a tertiary care academic medical hospital: Clinical, microbiological and economic impact. A 5-year temporary descriptive study. Infect. Prev. Pract. 2020, 2, 100048. [Google Scholar] [CrossRef]
- Jover-Sáenz, A. Grup d’estudi i equip PROAP. P-ILERDA -Programa integrat local extrahospitalari de racionalització, millora i desprescripció antibiòtica a Lleida-. Primers resultats d’un programa d’optimització d’ús d’antimicrobians (PROA) en atenció primària. Ann. Med. 2018, 4, 160–166. (In Catalan) [Google Scholar]
- Rodríguez-Baño, J.; Paño-Pardo, J.R.; Alvarez-Rocha, L.; Asensio, A.; Calbo, E.; Cercenado, E.; Cisneros, J.M.; Cobo, J.; Delgado, O.; Garnacho-Montero, J.; et al. Programs for optimizing the use of antibiotics (PROA) in Spanish hospitals: GEIH-SEIMC, SEFH and SEMPSPH consensus document. Enferm. Infecc. Microbiol. Clin. 2012, 22, e1–e22+e23. [Google Scholar] [CrossRef]
- Bakhit, M.; Hoffmann, T.; Scott, A.M.; Beller, E.; Rathbone, J.; Del Mar, C. Resistance decay in individuals after antibiotic exposure in primary care: A systematic review and meta-analysis. BMC Med. 2018, 16, 126. [Google Scholar] [CrossRef]
- Magiorakos, A.-P.; Srinivasan, A.; Carey, R.B.; Carmeli, Y.; Falagas, M.E.; Giske, C.G.; Harbarth, S.; Hindler, J.F.; Kahlmeter, G.; Olsson-Liljequist, B.; et al. Multidrug-resistant, extensively drug-resistant and pandrug-resistant bacteria: An international expert proposal for interim standard definitions for acquired resistance. Clin. Microbiol. Infect. 2012, 18, 268–281. [Google Scholar] [CrossRef] [PubMed]
- Patel, J.B. Clinical and Laboratory Standards Institute. In Performance Standards for Antimicrobial Susceptibility Testing; Clinical and Laboratory Standards Institute: Wayne, PA, USA, 2016; p. MS100–26. [Google Scholar]
- The European Committee on Antimicrobial Susceptibility Testing, Breakpoint Tables for Interpretation of MICs and Zone Diameters, Version 8.0. 2018. Available online: https://www.eucast.org/clinical_breakpoints/ (accessed on 8 September 2022).
- Boel, J.; Andreasen, V.; Jarløv, J.O.; Østergaard, C.; Gjørup, I.; Bøggild, N.; Arpi, M. Impact of antibiotic restriction on resistance levels of Escherichia coli: A controlled interrupted time series study of a hospital-wide antibiotic stewardship programme. J. Antimicrob. Chemother. 2016, 71, 2047–2051. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Livermore, D.M.; Hope, R.; Reynolds, R.; Blackburn, R.; Johnson, A.P.; Woodford, N. Declining cephalosporin and fluoroquinolone non-susceptibility among bloodstream Enterobacteriaceae from the UK: Links to prescribing change? J. Antimicrob. Chemother. 2013, 68, 2667–2674. [Google Scholar] [CrossRef]
- Muanda, F.T.; Sood, M.M.; Weir, M.A.; Sontrop, J.M.; Ahmadi, F.; Yoo, E.; Kim, R.B.; Silverman, M.S.; Knoll, G.A.; Garg, A.X. Association of Higher-Dose Fluoroquinolone Therapy with Serious Adverse Events in Older Adults with Advanced Chronic Kidney Disease. JAMA Netw. Open 2022, 5, e2224892. [Google Scholar] [CrossRef]
- Claeys, K.C.; Hopkins, T.L.; Vega, A.D.; Heil, E.L. Fluoroquinolone Restriction as an Effective Antimicrobial Stewardship Intervention. Curr. Infect. Dis. Rep. 2018, 20, 7. [Google Scholar] [CrossRef]
- Hernandez-Santiago, V.; Marwick, C.A.; Patton, A.; Davey, P.G.; Donnan, P.T.; Guthrie, B. Time series analysis of the impact of an intervention in Tayside, Scotland to reduce primary care broad-spectrum antimicrobial use. J. Antimicrob. Chemother. 2015, 70, 2397–2404. [Google Scholar] [CrossRef]
- Llor, C. Antibiotics Use in Primary Care during COVID-19. Antibiotics 2022, 11, 744. [Google Scholar] [CrossRef] [PubMed]
- Peñalva, G.; Fernández-Urrusuno, R.; Turmo, J.M.; Hernández-Soto, R.; Pajares, I.; Carrión, L.; Vázquez-Cruz, I.; Botello, B.; García-Robredo, B.; Cámara-Mestres, M.; et al. Long-term impact of an educational antimicrobial stewardship programme in primary care on infections caused by extended-spectrum β-lactamase-producing Escherichia coli in the community: An interrupted time-series analysis. Lancet Infect. Dis. 2020, 20, 199–207. [Google Scholar] [CrossRef] [PubMed]
- Abbott, I.J.; Peel, T.N.; Cairns, K.A.; Stewardson, A.J. Antibiotic management of urinary tract infections in the post-antibiotic era: A narrative review highlighting diagnostic and antimicrobial stewardship. Clin. Microbiol. Infect. 2022. [Google Scholar] [CrossRef]
- Luu, T.; Albarillo, F.S. Asymptomatic Bacteriuria: Prevalence, Diagnosis, Management, and Current Antimicrobial Stewardship Implementations. Am. J. Med. 2022, 135, e236–e244. [Google Scholar] [CrossRef]
- Abbott, I.J.; van Gorp, E.; Wyres, K.L.; Wallis, S.C.; Roberts, J.A.; Meletiadis, J.; Peleg, A.Y. Oral fosfomycin activity against Klebsiella pneumoniae in a dynamic bladder infection in vitro model. J. Antimicrob. Chemother. 2022, 77, 1324–1333. [Google Scholar] [CrossRef] [PubMed]
- Marchese, A.; Gualco, L.; Debbia, E.A.; Schito, G.C.; Schito, A.M. In vitro activity of fosfomycin against Gram-negative urinary pathogens and the biological cost of fosfomycin resistance. Int. J. Antimicrob. Agents 2003, 22, 53–59. [Google Scholar] [CrossRef]
- Drekonja, D.; Filice, G.; Greer, N.; Olson, A.; Macdonald, R.; Rutks, I.; Wilt, T.J. Antimicrobial Stewardship Programs in Outpatient Settings: A Systematic Review. Infect Control Hosp. Epidemiol. 2015, 36, 142–152. [Google Scholar] [CrossRef] [PubMed]
- Dyar, O.J.; Beović, B.; Vlahović-Palčevski, V.; Verheij, T.; Pulcini, C. How can we improve antibiotic prescribing in primary care? Expert Rev. Anti. Infect. Ther. 2016, 14, 403–413. [Google Scholar] [CrossRef]
- McNulty, C.; Hawking, M.; Lecky, D.; Jones, L.; Owens, R.; Charlett, A.; Butler, C.; Moore, P.; Francis, N. Effects of primary care antimicrobial stewardship outreach on antibiotic use by general practice staff: Pragmatic randomized controlled trial of the TARGET antibiotics workshop. J. Antimicrob. Chemother. 2018, 73, 1423–1432. [Google Scholar] [CrossRef]
- Hincapié, M.A.; Gallego, J.C.; Gempeler, A.; Piñeros, J.A.; Nasner, D.; Escobar, M.F. Implementation and Usefulness of Telemedicine During the COVID-19 Pandemic: A Scoping Review. J. Prim. Care Community Health 2020, 11, 2150132720980612. [Google Scholar] [CrossRef]
- Melendo-Pérez, S.; Fenoy-Alejandre, M.; Morey-Olivé, M.; Soler-Palacín, P.; y Grupo PROA-NEN; Miembros del Grupo PROA-NEN. Evaluation of perceived quality in non-restrictive interventions within the antimicrobial stewardship program in pediatrics (PROA-NEN). Enferm. Infecc Microbiol. Clin. 2019, 37, 215–217. [Google Scholar] [CrossRef] [PubMed]
- Ziv-On, E.; Friger, M.; Saidel-Odes, L.; Borer, A.; Shimoni, O.; Nikonov, A.; Nesher, L. Impact of an Antibiotic Stewardship Program on the Incidence of Resistant Escherichia coli: A Quasi-Experimental Study. Antibiotics 2021, 10, 179. [Google Scholar] [CrossRef]
- Santiago, V.H.; Davey, P.G.; Nathwani, D.; Marwick, C.A.; Guthrie, B. Changes in resistance among coliform bacteraemia associated with a primary care antimicrobial stewardship intervention: A population-based interrupted time series study. PLOS Med. 2019, 16, e1002825. [Google Scholar] [CrossRef]
- Gottesman, B.S.; Carmeli, Y.; Shitrit, P.; Chowers, M. Impact of Quinolone Restriction on Resistance Patterns of Escherichia coli Isolated from Urine by Culture in a Community Setting. Clin. Infect. Dis. 2009, 49, 869–875. [Google Scholar] [CrossRef] [PubMed]
- Low, M.; Neuberger, A.; Hooton, T.M.; Green, M.S.; Raz, R.; Balicer, R.D.; Almog, R. Association between urinary community-acquired fluoroquinolone-resistant Escherichia coli and neighbourhood antibiotic consumption: A population-based case-control study. Lancet Infect. Dis. 2019, 19, 419–428. [Google Scholar] [CrossRef] [PubMed]
- Peragine, C.; Walker, S.; Simor, A.; Walker, S.E.; Kiss, A.; Leis, J.A. Impact of a comprehensive antimicrobial stewardship program on institutional burden of antimicrobial resistance: A 14-Year controlled interrupted time-series study. Clin. Infect. Dis. 2019, 71, 2897–2904. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Prescribed Antibiotic | DID Pre-Intervention Period | Relative Change First Semester 2017 | Relative Change First Semester 2019 | Relative Change Second Semester 2021 | Absolute Effect Post-Intervention Period | Relative Effect (%) |
|---|---|---|---|---|---|---|
| Total antibiotics (J01) | 2.496 | 0.892 (0.890 to 0.894) | 0.790 (0.787 to 0.781) | 0.670 (0.668 to 0.672) | −0.688 (−0.691 to −0.685) | 27.57 (27.65 to 27.49) |
| Total of non-recommended antibiotics (NRA) | 1.126 | 0.842 (0.839 to 0.845) | 0.649 (0.646 to 0.652) | 0.583 (0.581 to 0.586) | −0.412 (−0.414 to −0.410) | 36.59 (36.70 to 36.48) |
| Co-amoxiclav (J01CR02) | 0.704 | 0.866 (0.862 to 0.870) | 0.726 (0.722 to 0.730) | 0.660 (0.657 to 0.663) | −0.227 (−0.229 to 0.226) | 32.27 (32.42 to 32.12) |
| Quinolones (J01M) | 0.311 | 0.754 (0.748 to 0.759) | 0.439 (0.435 to 0.443) | 0.328 (0.325 to 0.312) | −0.158 (−0.159 to −0.157) | 50.91 (51.09 to 50.74) |
| Ciprofloxacin (J01MA02) | 0.114 | 0.779 (0.770 to 0.788) | 0.556 (0.549 to 0.564) | 0.439 (0.433 to 0.446) | −0.052 (−0.052 to −0.051) | 45.39 (45.70 to 45.07) |
| Levofloxacin (J01MA12) | 0.132 | 0.828 (0.819 to 0.837) | 0.457 (0.451 to 0.464) | 0.338 (0.332 to 0.343) | −0.061 (−0.061 to 0.060) | 45.89 (46.18 to 45.60) |
| Cephalosporins (J01D) | 0.111 | 0.936 (0.925 to 0.947) | 0.749 (0.740 to 0.758) | 0.807 (0.798 to 0.817) | −0.026 (−0.027 to −0.026) | 23.90 (24.31 to 23.49) |
| Cefuroxime (J01DC02) | 0.061 | 0.739 (0.726 to 0.751) | 0.614 (0.603 to 0.625) | 0.433 (0.424 to 0.442) | −0.025 (−0.025 to −0.025) | 40.96 (41.41 to 40.50) |
| Third-generation cephalosporins (J01DD) | 0.046 | 1.241 (1.222 to 1.261) | 0.935 (0.919 to 0.951) | 1.275 (1.256 to 1.295) | 0.0003 (−0.0003 to 0.0004) | 0.07 (−0.73 to 0.87) |
| Total recommended antibiotics (RA) | 0.059 | 1.107 (1.092 to 1.123) | 1.267 (1.250 to 1.284) | 1.130 (1.114 to 1.146) | 0.0001 (−0.0004 to 0.0005) | 0.10 (−0.60 to 0.80) |
| Fosfomycin trometamol (J01XX01) | 0.042 | 1.026 (1.007 to 1.044) | 1.137 (1.118 to 1.156) | 1.150 (1.131 to 1.169) | −0.001 (−0.002 to −0.001) | 3.15 (3.96 to 2.33) |
| Nitrofurantoin (J01XE01) | 0.018 | 1.300 (1.268 to 1.332) | 1.574 (1.539 to 1.610) | 1.082 (1.054 to 1.111) | 0.001 (0.001 to 0.002) | 7.21 (6.03 to 8.39) |
| Antimicrobial Resistance | Comparisons by Semester (S) | ||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Second S 2016 vs. Second S 2017 | Second S 2016 vs. Second S 2019 | Second S 2016 vs. First S 2022 | |||||||||||||
| % (n/N) Pre- Intervention Resistance | % (n/N) Post- Intervention Resistance | OR CI 95% | p | % (n/N) Pre- Intervention Resistance | % (n/N) Post- Intervention Resistance | OR CI 95% | p | Prevented Rate (%) | % (n/N) Pre- Intervention Resistance | % (n/N) Post- Intervention Resistance | OR CI 95% | p | Prevented Rate (%) | ||
| E. coli | ESBL-producing | 10.73 (138/1285) | 7.69 (96/1248) | 0.68 (0.52–0.90) | 0.007 | 10.73 (138/1285) | 7.11 (83/1167) | 0.63 (0.47–0.84) | <0.001 | 33.8 (14.1–48.5) | 10.73 (138/1285) | 6.13 (72/1174) | 0.54 (0.40–0.73) | <0.001 | 45.7 (27.8–59.1) |
| Ciprofloxacin | 36.89 (474/1285) | 31.81 (397/1248) | 0.79 (0.67–0.94) | 0.004 | 36.89 (474/1285) | 21.67 (253/1167) | 0.47 (0.39–0.56) | <0.001 | 41.2 (33.0–48.4) | 36.89 (474/1285) | 17.46 (205/1174) | 0.36 (0.29–0.43) | <0.001 | 52.7 (45.3–59.0) | |
| Co-amoxiclav | 20.46 (263/1285) | 18.72 (233/1248) | 0.89 (0.73–1.09) | NS | 20.46 (263/1285) | 13.36 (156/1167) | 0.59 (0.48–0.74) | <0.001 | 34.7 (21.7–45.5) | 20.46 (263/1285) | 13.71 (161/1174) | 0.61 (0.49–0.76) | <0.001 | 33.0 (19.8–44.0) | |
| K. pneumoniae | ESBL-producing | 9.62 (23/239) | 13.95 (30/215) | 1.52 (0.88–2.71) | NS | 9.62 (23/239) | 14.17 (37/1167) | 1.05 (0.89–2.69) | NS | NA | 9.62 (23/239) | 8.80 (22/250) | 0.90 (0.49–1.67) | NS | NA |
| Ciprofloxacin | 14.64 (35/239) | 17.67 (38/215) | 1.25 (0.75–2.06) | NS | 14.64 (35/239) | 19.92 (52/1167) | 1.45 (0.90–2.32) | NS | NA | 14.64 (35/239) | 10.40 (26/250) | 0.67 (0.39–1.16) | NS | NA | |
| Co-amoxiclav | 14.64 (35/239) | 18.13 (39/215) | 1.29 (0.78–2.12) | NS | 14.64 (35/239) | 15.70 (41/1167) | 1.08 (0.66–1.77) | NS | NA | 14.64 (35/239) | 10.00 (25/250) | 0.64 (0.37–1.11) | NS | NA | |
| Antimicrobial Resistance | ID Pre-Intervention Period | Relative Change Second Semester 2017 | Relative Change Second Semester 2019 | Relative Change First Semester 2022 | Absolute Effect Post-Intervention Period | Relative Preventable Effect (%) |
|---|---|---|---|---|---|---|
| E. Coli | ||||||
| ESBL-producing | 0.370 (0.369 to 0.371) | 0.762 (0.757 to 0.768) | 0.656 (0.652 to 0.662) | 0.556 (0.552 to 0.560) | −0.115 (−0.116 to −0.114) | 31.01 (31.22 to 30.80) |
| Ciprofloxacin | 1.445 (1.443 to 1.447) | 0.808 (0.805 to 0.810) | 0.513 (0.511 to 0.515) | 0.406 (0.404 to 0.407) | −0.595 (−0.596 to −0.593) | 41.20 (41.29 to 41.10) |
| Co-amoxiclav | 0.583 (0.582 to 0.585) | 1.186 (1.181 to 1.191) | 0.783 (0.779 to 0.787) | 0.789 (0.785 to 0.793) | −0.102 (−0.103 to −0.101) | 17.46 (17.65 to 17.26) |
| K. pneumoniae | ||||||
| ESBL-producing | 0.067 (0.067 to 0.067) | 1.326 (1.310 to 1.343) | 1.614 (1.595 to 1.632) | 0.937 (0.923 to 0.950) | 0.018 (0.017 to 0.018) | 20.84 (20.34 to 21.35) |
| Ciprofloxacin | 0.104 (0.104 to 0.105) | 1.080 (1.069 to 1.092) | 1.458 (1.445 to 1.472) | 0.712 (0.702 to 0.721) | 0.013 (0.012 to 0.014) | 11.13 (10.67 to 11.59) |
| Co-amoxiclav | 0.081 (0.080 to 0.081) | 1.437 (1.422 to 1.453) | 1.490 (1.474 to 1.506) | 0.887 (0.875 to 0.899) | 0.027 (0.026 to 0.027) | 24.81 (24.38 to 25.25) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jover-Sáenz, A.; Ramírez-Hidalgo, M.; Bellés Bellés, A.; Ribes Murillo, E.; Batlle Bosch, M.; Cayado Cabanillas, J.; Garrido-Calvo, S.; Gracia Vilas, M.I.; Gros Navés, L.; Javierre Caudevilla, M.J.; et al. Impact of a Primary Care Antimicrobial Stewardship Program on Bacterial Resistance Control and Ecological Imprint in Urinary Tract Infections. Antibiotics 2022, 11, 1776. https://doi.org/10.3390/antibiotics11121776
Jover-Sáenz A, Ramírez-Hidalgo M, Bellés Bellés A, Ribes Murillo E, Batlle Bosch M, Cayado Cabanillas J, Garrido-Calvo S, Gracia Vilas MI, Gros Navés L, Javierre Caudevilla MJ, et al. Impact of a Primary Care Antimicrobial Stewardship Program on Bacterial Resistance Control and Ecological Imprint in Urinary Tract Infections. Antibiotics. 2022; 11(12):1776. https://doi.org/10.3390/antibiotics11121776
Chicago/Turabian StyleJover-Sáenz, Alfredo, María Ramírez-Hidalgo, Alba Bellés Bellés, Esther Ribes Murillo, Meritxell Batlle Bosch, José Cayado Cabanillas, Sònia Garrido-Calvo, María Isabel Gracia Vilas, Laura Gros Navés, María Jesús Javierre Caudevilla, and et al. 2022. "Impact of a Primary Care Antimicrobial Stewardship Program on Bacterial Resistance Control and Ecological Imprint in Urinary Tract Infections" Antibiotics 11, no. 12: 1776. https://doi.org/10.3390/antibiotics11121776
APA StyleJover-Sáenz, A., Ramírez-Hidalgo, M., Bellés Bellés, A., Ribes Murillo, E., Batlle Bosch, M., Cayado Cabanillas, J., Garrido-Calvo, S., Gracia Vilas, M. I., Gros Navés, L., Javierre Caudevilla, M. J., Mari López, A., Montull Navarro, L., Ortiz Valls, M., Terrer Manrique, G., Vaqué Castilla, P., Ichart Tomás, J. J., Justribó Sánchez, E., Andreu Mayor, E., Carrera Guiu, J., ... on behalf of Translational Research Group on Infectious Diseases of Lleida (Head Group, TRIDLE-IRBLleida). (2022). Impact of a Primary Care Antimicrobial Stewardship Program on Bacterial Resistance Control and Ecological Imprint in Urinary Tract Infections. Antibiotics, 11(12), 1776. https://doi.org/10.3390/antibiotics11121776