



Comparison between Ceftriaxone and Sulbactam-Ampicillin as Initial Treatment of Community-Acquired Pneumonia: A Systematic Review and Meta-Analysis

 ,
,  , and
, and
Abstract
1. Introduction
2. Results
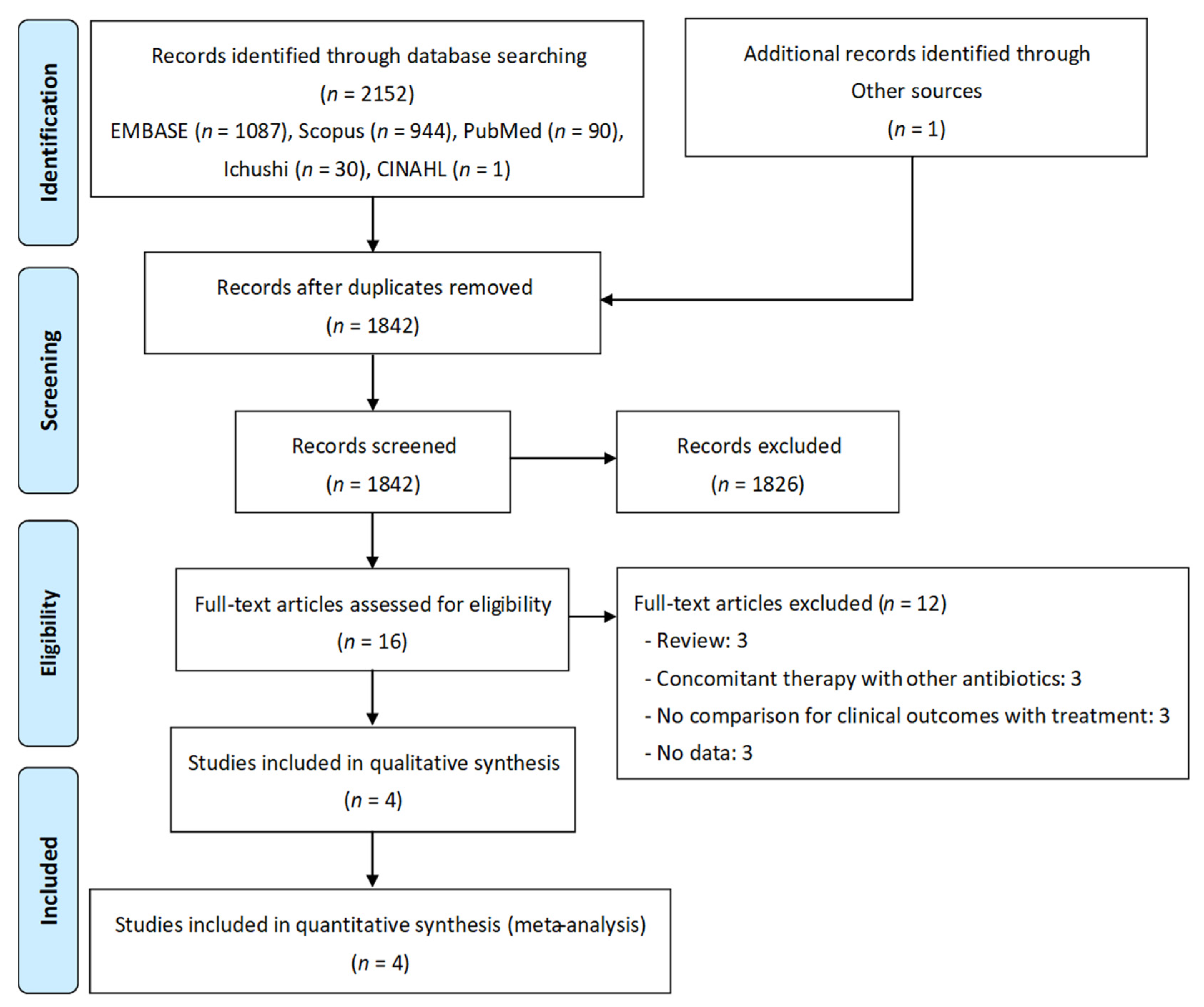
2.1. Systematic Review
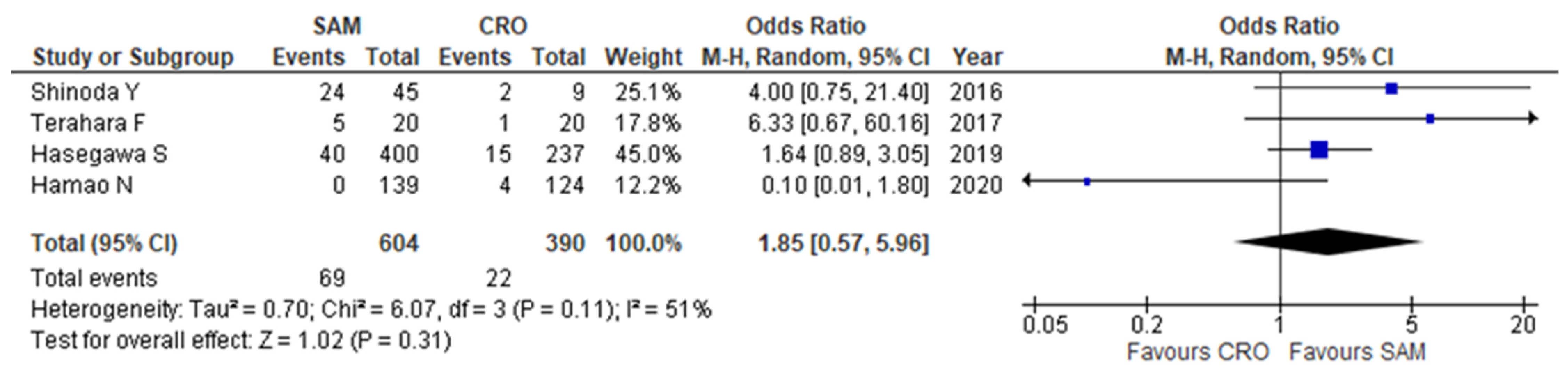
2.2. Meta-Analysis
3. Discussion
4. Materials and Methods
4.1. Study Design, Data Sources, and Search Strategy
4.2. Study Selection
4.3. Eligibility Criteria
4.4. Data Extraction and Risk of Bias Assessment
4.5. Data Synthesis and Analysis
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Torres, A.; Peetermans, W.E.; Viegi, G.; Blasi, F. Risk factors for community-acquired pneumonia in adults in Europe: A literature review. Thorax 2013, 10, 1136. [Google Scholar] [CrossRef] [PubMed]
- McLaughlin, J.M.; Johnson, M.H.; Kagan, S.A.; Baer, S.L. Clinical and economic burden of community-acquired pneumonia in the Veterans Health Administration, 2011: A retrospective cohort study. Infection 2015, 10, 1007. [Google Scholar] [CrossRef] [PubMed]
- Tichopad, A.; Roberts, C.; Gembula, I.; Hajek, P.; Skocynska, A.; Hryniewicz, W.; Jahnz-Rozyk, K.; Prymula, R.; Solovic, I.; Kolek, V. Clinical and economic burden of community-acquired pneumonia among adults in the Czech Republic, Hungary, Poland and Slovakia. PLoS ONE 2013, 10, e71375. [Google Scholar] [CrossRef] [PubMed]
- Center for Disease Control and Prevention. NAMCS/NHAMCS-About the Ambulatory Health Care Surveys; Center for Disease Control and Prevention: Atlanta, GA, USA, 2017.
- Brown, J.D.; Harnett, J.; Chambers, R.; Sato, R. The relative burden of community-acquired pneumonia hospitalizations in older adults: A retrospective observational study in the United States. BMC Geriatr. 2018, 10, 1186. [Google Scholar] [CrossRef]
- Ho, J.; Ip, M. Antibiotic-resistant community-acquired bacterial pneumonia. Infect. Dis. Clin. N. Am. 2019, 33, 1087–1103. [Google Scholar] [CrossRef]
- Cao, B.; Qu, J.X.; Yin, Y.D.; Eldere, J.V. Overview of antimicrobial options for Mycoplasma pneumoniae pneumonia: Focus on macrolide resistance. Clin. Respir. J. 2017, 11, 419–429. [Google Scholar] [CrossRef]
- Ishida, T.; Hashimoto, T.; Arita, M.; Tojo, Y.; Tachibana, H.; Jinnai, M. A 3-year prospective study of a urinary antigen-detection test for Streptococcus pneumoniae in community-acquired pneumonia: Utility and clinical impact on the reported etiology. J. Infect. Chemother. 2004, 10, 359–363. [Google Scholar] [CrossRef]
- American Thoracic Society; Infectious Diseases Society of America. Guidelines for the management of adults with hospital-acquired, ventilator-associated, and healthcare-associated pneumonia. Am. J. Respir. Crit. Care Med. 2005, 171, 388–416. [Google Scholar] [CrossRef]
- Barlett, J.G.; Dowell, S.F.; Mandell, L.A.; File, T.M., Jr.; Musher, D.M.; Fine, M.J. Practice guidelines for the management of community-acquired pneumonia in adults. Clin. Infect. Dis. 2000, 31, 347–382. [Google Scholar] [CrossRef]
- Schaberg, T.; Torres, A. Guidelines for management of adult community-acquired lower respiratory tract infections. Eur. Respir. J. 1998, 11, 986–991. [Google Scholar]
- Finegold, S.M. Aspiration pneumonia. Rev. Infect. Dis. 1991, 13, S737–S742. [Google Scholar] [CrossRef] [PubMed]
- Bartlett, J.G. How important are anaerobic bacteria in aspiration pneumonia: When should they be treated and what is optimal therapy. Infect. Dis. Clin. N. Am. 2013, 27, 149–155. [Google Scholar] [CrossRef] [PubMed]
- Citron, D.M.; Tyrrell, K.L.; Merriam, C.V.; Goldstein, E.J. In Vitro activity of ceftaroline against 623 diverse strains of anaerobic bacteria. Antimicrob. Agents Chemother. 2010, 54, 1627–1632. [Google Scholar] [CrossRef] [PubMed]
- Lupisan, S.; Suzuki, A.; Macalalad, N.; Egos, R.; Sombrero, L.; Okamoto, M.; Dapat, C.; Mondoy, M.; Galang, H.; Zeta, V.; et al. Etiology and epidemiology of community-acquired pneumonia in adults requiring hospital admission: A prospective study in rural Central Philippines. Int. J. Infect. Dis. 2019, 80, 46–53. [Google Scholar] [CrossRef] [PubMed]
- Farahat, F.; Bukhari, O.; Basfar, I.; Alammari, A.; Zaatari, A.; Alsaedi, A.; Alshamrani, M. Clinical characteristics and outcomes of community-acquired pneumonia in western Saudi Arabia: A four-year retrospective analysis of medical records. J. Infect. Public Health 2021, 14, 960–966. [Google Scholar] [CrossRef]
- Pichichero, M.E.; Casey, J.R. Safe use of selected cephalosporins in penicillin-allergic patients: A meta-analysis. Otolaryngol. Head Neck Surg. 2007, 136, 340–347. [Google Scholar] [CrossRef]
- Bai, F.; Li, X. Comparing several treatments with antibiotics for community-acquired pneumonia: A systematic review and meta-analysis of randomized controlled trials. Iran. J. Public Health 2021, 50, 1108–1119. [Google Scholar]
- Shinoda, Y.; Matsuoka, T.; Mori, T.; Yoshida, S.; Ohashi, K.; Yoshimura, T.; Sugiyama, T. Antibacterial therapy of aspiration pneumonia in patients with methicillin-resistant Staphylococcus aureus-positive sputum: Identification of risk factors. Pharmazie 2016, 71, 109–112. [Google Scholar]
- Terahara, F.; Kisa, K.; Yamada, K.; Yokokawa, Y.; Saito, S. Efficacy of ceftriaxone in aspiration pneumonia; propensity score matched retrospective observational study, compared with sulbactam/ampicillin. Jpn. J. Pharm. Health Care Sci. 2017, 43, 306–312. [Google Scholar] [CrossRef]
- Hasegawa, S.; Shiraishi, A.; Yaegashi, M.; Hosokawa, N.; Morimoto, K.; Mori, T. Ceftriaxone versus ampicillin/sulbactam for the treatment of aspiration-associated pneumonia in adults. J. Comp. Eff. Res. 2019, 8, 1275–1284. [Google Scholar] [CrossRef]
- Hamano, N.; Ito, I.; Konishi, S.; Tanabe, N.; Shirata, M.; Oi, I.; Tsukino, M.; Matsumoto, H.; Yasutomo, Y.; Kadowaki, S.; et al. Comparison of ceftriaxone plus macrolide and ampicillin/sulbactam plus macrolide in treatment for patients with community-acquired pneumonia without risk factors for aspiration: An open-label, quasi-randomized, controlled trial. BMC. Pulm. Med. 2020, 20, 160. [Google Scholar]
- Xaba, S.N.; Greeff, O.; Becker, P. Determinants, outcomes and costs of ceftriaxone v. amoxicillin-clavulanate in the treatment of community-acquired pneumonia at Witbank hospital. S. Afr. Med. J. 2014, 104, 187–191. [Google Scholar] [PubMed]
- Sanchez, M.E.; Vargas, J.G.; Baños, V.; Gómez, J.R.; Muñoz, L.; Simarro, E.; Soto, M.C.; Canteras, M.; Valdés, M. Prospective and comparative study between cefuroxime, ceftriaxone and amoxicillin-clavulanic acid in the treatment of community-acquired pneumonia. Rev. Esp. Quimioter. 1998, 11, 132–138. [Google Scholar]
- Leishker, A.H.; Kolb, G.F. Aspiration pneumonia: Management in Germany. Eur. Geriatr. Med. 2011, 2, 184–186. [Google Scholar] [CrossRef]
- Kohno, S.; Imamura, Y.; Shindo, Y.; Seki, M.; Ishida, T.; Teramoto, S.; Kadota, J.; Tomono, K.; Watanabe, A. Clinical practice guidelines for nursing- and healthcare-associated pneumonia (NHCAP). Respir. Investig. 2013, 51, 103–126. [Google Scholar] [CrossRef] [PubMed]
- Tokuyasu, H.; Harada, T.; Watanabe, E.; Okazaki, R.; Touge, H.; Kawasaki, Y.; Shimizu, E. Effectiveness of meropenem for the treatment of aspiration pneumonia in elderly patients. Intern. Med. 2009, 48, 129–135. [Google Scholar] [CrossRef]
- Akata, K.; Yatera, K.; Yamasaki, K.; Kawanami, T.; Naito, K.; Noguchi, S.; Fukuda, K.; Ishimoto, H.; Taniguchi, H.; Mukae, H. The significance of oral streptococci in patients with pneumonia with risk factors for aspiration: The bacterial floral analysis of 16S ribosomal RNA gene using bronchoalveolar lavage fluid. BMC. Pulm. Med. 2016, 16, 79. [Google Scholar] [CrossRef]
- Taylor, J.K.; Fleming, G.B.; Singanayagam, A.; Hill, A.T.; Chalmers, J.D. Risk factors for aspiration in community-acquired pneumonia: Analysis of a hospitalized UK cohort. Am. J. Med. 2013, 126, 995–1001. [Google Scholar] [CrossRef]
- Heffelfinger, J.D.; Dowell, S.F.; Jorgensen, J.H.; Klugman, K.P.; Mabry, L.R.; Musher, D.M.; Plouffe, J.F.; Rakowsky, A.; Schuchat, A.; Whitney, C.G. Management of community-acquired pneumonia in the era of pneumococcal resistance: A report from the drug-resistant Streptococcus pneumoniae therapeutic working group. Arch. Intern. Med. 2000, 160, 1399–1408. [Google Scholar] [CrossRef]
- Ohno, A.; Ishii, Y.; Kobayashi, I.; Yamaguchi, K. Antibacterial activity and PK/PD of ceftriaxone against penicillin-resistant Streptococcus pneumoniae and beta-lactamase-negative ampicillin-resistant Haemophilus influenzae isolates from patients with community-acquired pneumonia. J. Infect. Chemother. 2007, 13, 296–301. [Google Scholar] [CrossRef]
- Bartlett, J.G. Anaerobic bacterial infection of the lung. Anaerobe 2012, 18, 235–239. [Google Scholar] [CrossRef] [PubMed]
- Dubreuil, L.; Behra-Miellet, J.; Vouillot, C.; Bland, S.; Sedallian, A.; Mory, F. β-lactamase production in Prevotella and in vitro susceptibilities to selected β-lactam antibiotics. Int. J. Antimicrob. Agents 2003, 21, 267–273. [Google Scholar] [CrossRef]
- Fujita, K.; Takata, I.; Sugiyama, H.; Suematsu, H.; Yamagishi, Y.; Mikamo, H. Antimicrobial susceptibilities of clinical isolates of the anaerobic bacteria which can cause aspiration pneumonia. Anaerobe 2019, 57, 86–89. [Google Scholar] [CrossRef]
- The Guidelines of Preferred Reporting Items for Systematic Review and Meta-Analysis (PRISMA) Statement. Available online: http://prisma-statement.org (accessed on 29 August 2022).
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; PRISMA Group. Preferred reporting items for systematic reviews and me-ta-analyses: The PRISMA statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [PubMed]
- Kato, H.; Hagihara, M.; Asai, N.; Hirai, J.; Yamagishi, Y.; Iwamoto, T.; Mikamo, H. A systematic review and meta-analysis of efficacy and safety of azithromycin versus moxifloxacin for the initial treatment of Mycoplasma genitalium. Antibiotics 2022, 11, 353. [Google Scholar] [CrossRef]
- Kato, H.; Hagihara, M.; Morikawa, Y.; Asai, N.; Mikamo, H.; Iwamoto, T. Retrospective comparison of the effectiveness and safety of ceftriaxone 1 g twice daily versus 2 g once daily for treatment of aspiration pneumonia. Antibiotics 2022, 11, 983. [Google Scholar] [CrossRef]
- Kim, S.Y.; Park, J.E.; Lee, Y.J.; Seo, H.J.; Sheen, S.S.; Hahn, S.; Jang, B.H.; Son, H.J. Testing a tool for assessing the risk of bias for nonrandomized studies showed moderate reliability and promising validity. J. Clin. Epidemiol. 2013, 66, 408–414. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- Available online: http://www.prisma-statement.org/ (accessed on 19 September 2022).




{kind=link}
{kind=link}
{kind=link}
| Study | Study Design | Setting | Period | Country of Study | No of Patients | Agent Used with Dosage | ||
| Shinoda Y, 2016 [19] | Retrospective observational study | Single center | January 2013 to May 2013 | Japan | SAM, 45; CRO, 9 | SAM, NR; CRO, NR | ||
| Terafarad F, 2017 [20] | Retrospective observational study | Single center | January 2014 to December 2015 | Japan | SAM, 20 CRO, 20 | SAM, 3–6 g/day; CRO, 2–4 g/day | ||
| Hasegawa S, 2019 [21] | Retrospective observational study | Multicenter | September 2011 to August 2014 | Japan | SAM, 400; CRO, 237 | SAM, NR; CRO, NR | ||
| Hamao N, 2020 [22] | Open-label, randomized controlled trial | Single center | June 2002 to June 2008 | Japan | SAM, 139; CRO, 124 | SAM, 1.5–6.0 g/day; CRO, 1–2 g/day | ||
| Study | Mean Duration of Therapy, Days | Mean Age, Years | Underlying Disease (%) | Pathogen (%) | ||||
| Shinoda Y, 2016 [19] | SAM, NR; CRO, NR | Overall Over 80, 72.3% | Stroke, 45.5 Alzheimer’s disease, 33.7 Parkinson’s disease, 12.9 | GPB, 9.9 GNB, 55.4 | ||||
| Terahara F, 2017 [20] | SAM, NR; CRO, NR | SAM, 88; CRO, 81 | Dementia, 55.0 Bedridden status, 30.0 Cerebrovascular disease, 27.5 Neuromuscular diseases, 7.5 | NR | ||||
| Hasegawa S, 2019 [21] | SAM, NR; CRO, NR | SAM, 82; CRO, 82 | Dementia, 28.9 Bedridden status, 16.3 Cerebrovascular disease, 4.4 Neuromuscular diseases, 11.9 | Mainly Streptococcus pneumoniae and Haemophilus influenzae | ||||
| Hamao N, 2020 [22] | SAM, 7–14; CRO, 7–14 | SAM, 63; CRO, 61 | NR | S. pneumoniae, 23.2%; H. influenzae, 2.3%; unknown, 47.1% | ||||
| Study | Selection of Participants | Confounding Variables | Measurement of Exposure | Building of Outcome Assessment | Incomplete Outcome Data | Selective Outcome Reporting |
|---|---|---|---|---|---|---|
| Shinoda Y, 2016 [19] | Low risk | High risk | Low risk | High risk | Low risk | Low risk |
| Terahara F, 2017 [20] | Low risk | Low risk | Low risk | High risk | Low risk | Low risk |
| Hasegawa S, 2019 [21] | Low risk | Low risk | Low risk | High risk | Low risk | Low risk |
| Hamao N, 2020 [22] | Low risk | Low risk | Low risk | Low risk | Low risk | Low risk |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kato, H.; Hagihara, M.; Asai, N.; Hirai, J.; Yamagishi, Y.; Iwamoto, T.; Mikamo, H. Comparison between Ceftriaxone and Sulbactam-Ampicillin as Initial Treatment of Community-Acquired Pneumonia: A Systematic Review and Meta-Analysis. Antibiotics 2022, 11, 1291. https://doi.org/10.3390/antibiotics11101291
Kato H, Hagihara M, Asai N, Hirai J, Yamagishi Y, Iwamoto T, Mikamo H. Comparison between Ceftriaxone and Sulbactam-Ampicillin as Initial Treatment of Community-Acquired Pneumonia: A Systematic Review and Meta-Analysis. Antibiotics. 2022; 11(10):1291. https://doi.org/10.3390/antibiotics11101291
Chicago/Turabian StyleKato, Hideo, Mao Hagihara, Nobuhiro Asai, Jun Hirai, Yuka Yamagishi, Takuya Iwamoto, and Hiroshige Mikamo. 2022. "Comparison between Ceftriaxone and Sulbactam-Ampicillin as Initial Treatment of Community-Acquired Pneumonia: A Systematic Review and Meta-Analysis" Antibiotics 11, no. 10: 1291. https://doi.org/10.3390/antibiotics11101291
APA StyleKato, H., Hagihara, M., Asai, N., Hirai, J., Yamagishi, Y., Iwamoto, T., & Mikamo, H. (2022). Comparison between Ceftriaxone and Sulbactam-Ampicillin as Initial Treatment of Community-Acquired Pneumonia: A Systematic Review and Meta-Analysis. Antibiotics, 11(10), 1291. https://doi.org/10.3390/antibiotics11101291