
Synergistic Antibacterial Effects of Meropenem in Combination with Aminoglycosides against Carbapenem-Resistant Escherichia coli Harboring blaNDM-1 and blaNDM-5

 , ,
, ,
Abstract
1. Introduction
2. Results and Discussion
2.1. Bacterial Isolates
2.2. The Antibiogram of Carbapenem-Resistant E. coli Isolates
2.3. Antimicrobial Susceptibility to Carbapenem and Aminoglycosides
2.4. Genotypic Resistance Mechanism in Carbapenem-Resistant E. coli Isolates
2.5. The Combined Effect of Meropenem and Aminoglycosides
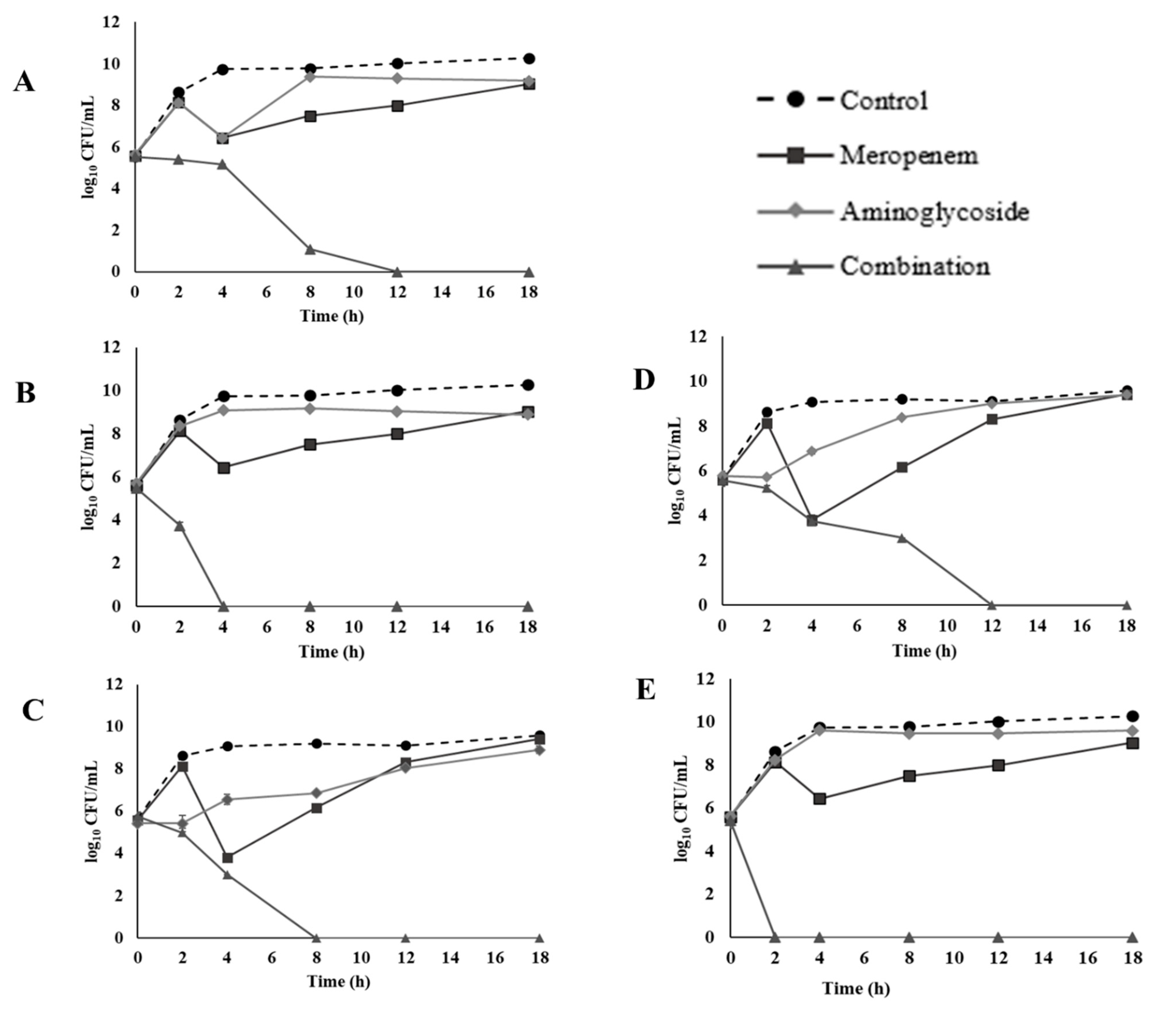
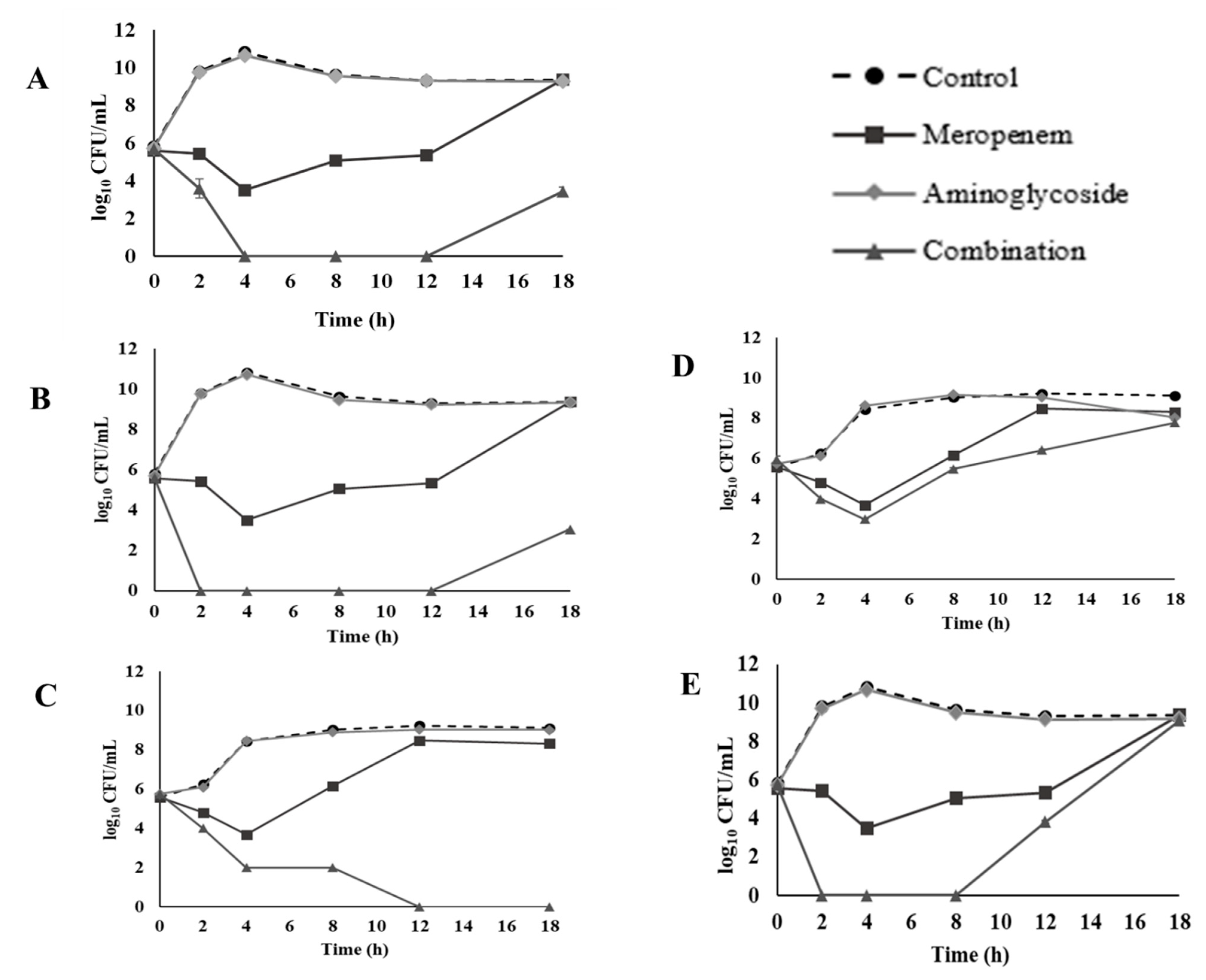
2.6. Time-Kill Assay
3. Materials and Methods
3.1. Chemical and Media
3.2. Bacterial Collection and Identification
3.3. Screening for Carbapenem Resistance
3.4. Antibiogram of Carbapenem-Resistant Isolates
3.5. Genotypic Determination of Carbapenemase and ESBL
3.6. Checkerboard Technique
3.7. Time-Kill Assay
4. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- van Duin, D.; Doi, Y. The global epidemiology of carbapenemase-producing Enterobacteriaceae. Virulence 2017, 8, 460–469. [Google Scholar] [CrossRef]
- Adams, D.J.; Susi, A.; Nylund, C.M. Clinical characteristics, risk factors, and outcomes of patients hospitalized in the US military health system with carbapenem-resistant Enterobacteriaceae infection. Am. J. Infect. Control 2020, 48, 644–649. [Google Scholar] [CrossRef]
- Paveenkittiporn, W.; Lyman, M.; Biedron, C.; Chea, N.; Bunthi, C.; Kolwaite, A.; Janejai, N. Molecular epidemiology of carbapenem-resistant Enterobacterales in Thailand, 2016–2018. Antimicrob. Resist. Infect. Control 2021, 10, 1–8. [Google Scholar] [CrossRef]
- Sheu, C.C.; Lin, S.Y.; Chang, Y.T.; Lee, C.Y.; Chen, Y.H.; Hsueh, P.R. Management of infections caused by extended-spectrum β-lactamase-producing Enterobacteriaceae: Current evidence and future prospects. Expert Rev. Anti Infect. Ther. 2018, 16, 205–218. [Google Scholar] [CrossRef]
- Gutiérrez-Gutiérrez, B.; Rodríguez-Baño, J. Current options for the treatment of infections due to extended-spectrum beta-lactamase-producing Enterobacteriaceae in different groups of patients. Clin. Microbiol. Infect. 2019, 25, 932–942. [Google Scholar] [CrossRef] [PubMed]
- Nordmann, P.; Naas, T.; Poirel, L. Global spread of Carbapenemase-producing Enterobacteriaceae. Emerg. Infect. Dis. 2011, 17, 1791–1798. [Google Scholar] [CrossRef] [PubMed]
- Patel, G.; Bonomo, R. “Stormy waters ahead”: Global emergence of carbapenemases. Front. Microbiol. 2013, 4, 48. [Google Scholar] [CrossRef] [PubMed]
- Hayakawa, K.; Nakano, R.; Hase, R.; Shimatani, M.; Kato, H.; Hasumi, J.; Doi, A.; Sekiya, N.; Nei, T.; Okinaka, K.; et al. Comparison between IMP carbapenemase-producing Enterobacteriaceae and non-carbapenemase-producing Enterobacteriaceae: A multicentre prospective study of the clinical and molecular epidemiology of carbapenem-resistant Enterobacteriaceae. J. Antimicrob. Chemother. 2019, 75, 697–708. [Google Scholar] [CrossRef] [PubMed]
- Logan, L.K.; Weinstein, R.A. The Epidemiology of Carbapenem-Resistant Enterobacteriaceae: The Impact and Evolution of a Global Menace. J. Infect. Dis. 2017, 215, S28–S36. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Wang, Q.; Yin, Y.; Chen, H.; Jin, L.; Gu, B.; Xie, L.; Yang, C.; Ma, X.; Li, H.; et al. Epidemiology of Carbapenem-Resistant Enterobacteriaceae Infections: Report from the China CRE Network. Antimicrob. Agents Chemother. 2018, 62, e01882-17. [Google Scholar] [CrossRef]
- Doi, Y. Treatment Options for Carbapenem-resistant Gram-negative Bacterial Infections. Clin. Infect. Dis. 2019, 69, S565–S575. [Google Scholar] [CrossRef]
- Falcone, M.; Paterson, D. Spotlight on ceftazidime/avibactam: A new option for MDR Gram-negative infections. J. Antimicrob. Chemother. 2016, 71, 2713–2722. [Google Scholar] [CrossRef] [PubMed]
- Shields, R.K.; Potoski, B.A.; Haidar, G.; Hao, B.; Doi, Y.; Chen, L.; Press, E.G.; Kreiswirth, B.N.; Clancy, C.J.; Nguyen, M.H. Clinical Outcomes, Drug Toxicity, and Emergence of Ceftazidime-Avibactam Resistance Among Patients Treated for Carbapenem-Resistant Enterobacteriaceae Infections. Clin. Infect. Dis. 2016, 63, 1615–1618. [Google Scholar] [CrossRef]
- Livermore, D.M.; Mushtaq, S. Activity of biapenem (RPX2003) combined with the boronate β-lactamase inhibitor RPX7009 against carbapenem-resistant Enterobacteriaceae. J. Antimicrob. Chemother. 2013, 68, 1825–1831. [Google Scholar] [CrossRef]
- Livermore, D.M.; Warner, M.; Mushtaq, S. Activity of MK-7655 combined with imipenem against Enterobacteriaceae and Pseudomonas aeruginosa. J. Antimicrob. Chemother. 2013, 68, 2286–2290. [Google Scholar] [CrossRef]
- Wu, W.; Feng, Y.; Tang, G.; Qiao, F.; McNally, A.; Zong, Z. NDM Metallo-β-Lactamases and Their Bacterial Producers in Health Care Settings. Clin. Microbiol. Rev. 2019, 32, e00115-18. [Google Scholar] [CrossRef]
- Sun, P.; Xia, W.; Liu, G.; Huang, X.; Tang, C.; Liu, C.; Xu, Y.; Ni, F.; Mei, Y.; Pan, S. Characterization Of bla (NDM-5)-Positive Escherichia coli Prevalent In A University Hospital In Eastern China. Infect. Drug Resist. 2019, 12, 3029–3038. [Google Scholar] [CrossRef] [PubMed]
- Yang, P.; Xie, Y.; Feng, P.; Zong, Z. blaNDM-5 carried by an IncX3 plasmid in Escherichia coli sequence type 167. Antimicrob. Agents Chemother. 2014, 58, 7548–7552. [Google Scholar] [CrossRef]
- Li, X.; Fu, Y.; Shen, M.; Huang, D.; Du, X.; Hu, Q.; Zhou, Y.; Wang, D.; Yu, Y. Dissemination of bla(NDM-5) gene via an IncX3-type plasmid among non-clonal Escherichia coli in China. Antimicrob. Resist. Infect. Control 2018, 7, 59. [Google Scholar] [CrossRef] [PubMed]
- Sheu, C.C.; Chang, Y.T.; Lin, S.Y.; Chen, Y.H.; Hsueh, P.R. Infections Caused by Carbapenem-Resistant Enterobacteriaceae: An Update on Therapeutic Options. Front. Microbiol. 2019, 10, 80. [Google Scholar] [CrossRef] [PubMed]
- Pacios, O.; Blasco, L.; Bleriot, I.; Fernandez-Garcia, L.; González Bardanca, M.; Ambroa, A.; López, M.; Bou, G.; Tomás, M. Strategies to Combat Multidrug-Resistant and Persistent Infectious Diseases. Antibiotics 2020, 9, 65. [Google Scholar] [CrossRef]
- Nwabor, O.F.; Terbtothakun, P.; Voravuthikunchai, S.P.; Chusri, S. Evaluation of the Synergistic Antibacterial Effects of Fosfomycin in Combination with Selected Antibiotics against Carbapenem-Resistant Acinetobacter baumannii. Pharmaceuticals 2021, 14, 185. [Google Scholar] [CrossRef] [PubMed]
- Ontong, J.C.; Ozioma, N.F.; Voravuthikunchai, S.P.; Chusri, S. Synergistic antibacterial effects of colistin in combination with aminoglycoside, carbapenems, cephalosporins, fluoroquinolones, tetracyclines, fosfomycin, and piperacillin on multidrug resistant Klebsiella pneumoniae isolates. PLoS ONE 2021, 16, e0244673. [Google Scholar] [CrossRef] [PubMed]
- Chukamnerd, A.; Pomwised, R.; Paing Phoo, M.T.; Terbtothakun, P.; Hortiwakul, T.; Charoenmak, B.; Chusri, S. In vitro synergistic activity of fosfomycin in combination with other antimicrobial agents against carbapenem-resistant Klebsiella pneumoniae isolated from patients in a hospital in Thailand. J. Infect. Chemother. 2021, 27, 507–514. [Google Scholar] [CrossRef]
- Liu, E.; Jia, P.; Li, X.; Zhou, M.; Kudinha, T.; Wu, C.; Xu, Y.; Yang, Q. In vitro and in vivo Effect of Antimicrobial Agent Combinations Against Carbapenem-Resistant Klebsiella pneumoniae with Different Resistance Mechanisms in China. Infect. Drug Resist. 2021, 14, 917–928. [Google Scholar] [CrossRef] [PubMed]
- Poole, K.; Gilmour, C.; Farha, M.A.; Parkins, M.D.; Klinoski, R.; Brown, E.D. Meropenem potentiation of aminoglycoside activity against Pseudomonas aeruginosa: Involvement of the MexXY-OprM multidrug efflux system. J. Antimicrob. Chemother. 2018, 73, 1247–1255. [Google Scholar] [CrossRef] [PubMed]
- Gupta, N.; Limbago, B.M.; Patel, J.B.; Kallen, A.J. Carbapenem-resistant Enterobacteriaceae: Epidemiology and prevention. Clin. Infect. Dis. 2011, 53, 60–67. [Google Scholar] [CrossRef]
- Chotiprasitsakul, D.; Srichatrapimuk, S.; Kirdlarp, S.; Pyden, A.D.; Santanirand, P. Epidemiology of carbapenem-resistant Enterobacteriaceae: A 5-year experience at a tertiary care hospital. Infect. Drug Resist. 2019, 12, 461–468. [Google Scholar] [CrossRef]
- Segagni Lusignani, L.; Presterl, E.; Zatorska, B.; Van den Nest, M.; Diab-Elschahawi, M. Infection control and risk factors for acquisition of carbapenemase-producing enterobacteriaceae. A 5 year (2011–2016) case-control study. Antimicrob. Resist. Infect. Control 2020, 9, 18. [Google Scholar] [CrossRef]
- Rodríguez-Baño, J.; Gutiérrez-Gutiérrez, B.; Machuca, I.; Pascual, A. Treatment of Infections Caused by Extended-Spectrum-Beta-Lactamase-, AmpC-, and Carbapenemase-Producing Enterobacteriaceae. Clin. Microbiol. Rev. 2018, 31, e00079-17. [Google Scholar] [CrossRef]
- Guh, A.Y.; Bulens, S.N.; Mu, Y.; Jacob, J.T.; Reno, J.; Scott, J.; Wilson, L.E.; Vaeth, E.; Lynfield, R.; Shaw, K.M.; et al. Epidemiology of Carbapenem-Resistant Enterobacteriaceae in 7 US Communities, 2012–2013. JAMA 2015, 314, 1479–1487. [Google Scholar] [CrossRef]
- Han, J.H.; Goldstein, E.J.; Wise, J.; Bilker, W.B.; Tolomeo, P.; Lautenbach, E. Epidemiology of Carbapenem-Resistant Klebsiella pneumoniae in a Network of Long-Term Acute Care Hospitals. Clin. Infect. Dis. 2017, 64, 839–844. [Google Scholar] [CrossRef]
- Sun, H.K.; Ong, C.T.; Umer, A.; Harper, D.; Troy, S.; Nightingale, C.H.; Nicolau, D.P. Pharmacokinetic profile of tigecycline in serum and skin blister fluid of healthy subjects after multiple intravenous administrations. Antimicrob. Agents Chemother. 2005, 49, 1629–1632. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Vattimo Mde, F.; Watanabe, M.; da Fonseca, C.D.; Neiva, L.B.; Pessoa, E.A.; Borges, F.T. Polymyxin B Nephrotoxicity: From Organ to Cell Damage. PLoS ONE 2016, 11, e0161057. [Google Scholar] [CrossRef] [PubMed]
- Hashemian, S.M.R.; Farhadi, Z.; Farhadi, T. Fosfomycin: The characteristics, activity, and use in critical care. Ther. Clin. Risk Manag. 2019, 15, 525–530. [Google Scholar] [CrossRef]
- Doi, Y.; Wachino, J.I.; Arakawa, Y. Aminoglycoside Resistance: The Emergence of Acquired 16S Ribosomal RNA Methyltransferases. Infect. Dis. Clin. N. Am. 2016, 30, 523–537. [Google Scholar] [CrossRef] [PubMed]
- Ramirez, M.S.; Tolmasky, M.E. Aminoglycoside modifying enzymes. Drug Resist. Updates 2010, 13, 151–171. [Google Scholar] [CrossRef] [PubMed]
- Bodendoerfer, E.; Marchesi, M.; Imkamp, F.; Courvalin, P.; Böttger, E.C.; Mancini, S. Co-occurrence of aminoglycoside and β-lactam resistance mechanisms in aminoglycoside- non-susceptible Escherichia coli isolated in the Zurich area, Switzerland. Int. J. Antimicrob. Agents 2020, 56, 106019. [Google Scholar] [CrossRef] [PubMed]
- Iredell, J.; Brown, J.; Tagg, K. Antibiotic resistance in Enterobacteriaceae: Mechanisms and clinical implications. BMJ 2016, 352. [Google Scholar] [CrossRef] [PubMed]
- Queenan, A.M.; Bush, K. Carbapenemases: The versatile beta-lactamases. Clin. Microbiol. Rev. 2007, 20, 440–458. [Google Scholar] [CrossRef]
- Okoche, D.; Asiimwe, B.B.; Katabazi, F.A.; Kato, L.; Najjuka, C.F. Prevalence and Characterization of Carbapenem-Resistant Enterobacteriaceae Isolated from Mulago National Referral Hospital, Uganda. PLoS ONE 2015, 10, e0135745. [Google Scholar] [CrossRef]
- Boutal, H.; Vogel, A.; Bernabeu, S.; Devilliers, K.; Creton, E.; Cotellon, G.; Plaisance, M.; Oueslati, S.; Dortet, L.; Jousset, A.; et al. A multiplex lateral flow immunoassay for the rapid identification of NDM-, KPC-, IMP- and VIM-type and OXA-48-like carbapenemase-producing Enterobacteriaceae. J. Antimicrob. Chemother. 2018, 73, 909–915. [Google Scholar] [CrossRef]
- Suay-García, B.; Pérez-Gracia, M.T. Present and Future of Carbapenem-resistant Enterobacteriaceae (CRE) Infections. Antibiotics 2019, 8, 122. [Google Scholar] [CrossRef] [PubMed]
- Dortet, L.; Cuzon, G.; Ponties, V.; Nordmann, P. Trends in carbapenemase-producing Enterobacteriaceae, France, 2012 to 2014. Eurosurveillance 2017, 22, 30461. [Google Scholar] [CrossRef]
- Nordmann, P.; Poirel, L. The difficult-to-control spread of carbapenemase producers among Enterobacteriaceae worldwide. Clin. Microbiol. Infect. 2014, 20, 821–830. [Google Scholar] [CrossRef]
- Chang, Y.T.; Siu, L.K.; Wang, J.T.; Wu, T.L.; Chen, Y.H.; Chuang, Y.C.; Lin, J.C.; Lu, P.L. Resistance mechanisms and molecular epidemiology of carbapenem-nonsusceptible Escherichia coli in Taiwan, 2012–2015. Infect. Drug Resist. 2019, 12, 2113–2123. [Google Scholar] [CrossRef] [PubMed]
- Groundwater, P.W.; Xu, S.; Lai, F.; Váradi, L.; Tan, J.; Perry, J.D.; Hibbs, D.E. New Delhi metallo-β-lactamase-1: Structure, inhibitors and detection of producers. Future Med. Chem. 2016, 8, 993–1012. [Google Scholar] [CrossRef] [PubMed]
- Cheng, Z.; Thomas, P.W.; Ju, L.; Bergstrom, A.; Mason, K.; Clayton, D.; Miller, C.; Bethel, C.R.; VanPelt, J.; Tierney, D.L. Evolution of New Delhi metallo-β-lactamase (NDM) in the clinic: Effects of NDM mutations on stability, zinc affinity, and mono-zinc activity. J. Biol. Chem. 2018, 293, 12606–12618. [Google Scholar] [CrossRef] [PubMed]
- Khan, S.; Ali, A.; Khan, A.U. Structural and functional insight of New Delhi Metallo β-lactamase-1 variants. Future Med. Chem. 2018, 10, 221–229. [Google Scholar] [CrossRef]
- Tian, X.; Zheng, X.; Sun, Y.; Fang, R.; Zhang, S.; Zhang, X.; Lin, J.; Cao, J.; Zhou, T. Molecular Mechanisms and Epidemiology of Carbapenem-Resistant Escherichia coli Isolated from Chinese Patients During 2002–2017. Infect. Drug Resist. 2020, 13, 501–512. [Google Scholar] [CrossRef]
- Netikul, T.; Kiratisin, P. Genetic Characterization of Carbapenem-Resistant Enterobacteriaceae and the Spread of Carbapenem-Resistant Klebsiella pneumonia ST340 at a University Hospital in Thailand. PLoS ONE 2015, 10, e0139116. [Google Scholar] [CrossRef] [PubMed]
- Kerdsin, A.; Deekae, S.; Chayangsu, S.; Hatrongjit, R.; Chopjitt, P.; Takeuchi, D.; Akeda, Y.; Tomono, K.; Hamada, S. Genomic characterization of an emerging bla(KPC-2) carrying Enterobacteriaceae clinical isolates in Thailand. Sci. Rep. 2019, 9, 18521. [Google Scholar] [CrossRef] [PubMed]
- Poirel, L.; Walsh, T.R.; Cuvillier, V.; Nordmann, P. Multiplex PCR for detection of acquired carbapenemase genes. Diagn. Microbiol. Infect. Dis. 2011, 70, 119–123. [Google Scholar] [CrossRef] [PubMed]
- Monstein, H.J.; Ostholm-Balkhed, A.; Nilsson, M.V.; Nilsson, M.; Dornbusch, K.; Nilsson, L.E. Multiplex PCR amplification assay for the detection of blaSHV, blaTEM and blaCTX-M genes in Enterobacteriaceae. APMIS 2007, 115, 1400–1408. [Google Scholar] [CrossRef]
- Yadav, R.; Bulitta, J.B.; Schneider, E.K.; Shin, B.S.; Velkov, T.; Nation, R.L.; Landersdorfer, C.B. Aminoglycoside Concentrations Required for Synergy with Carbapenems against Pseudomonas aeruginosa Determined via Mechanistic Studies and Modeling. Antimicrob. Agents Chemother. 2017, 61, e00722-17. [Google Scholar] [CrossRef]
- Kadurugamuwa, J.L.; Lam, J.S.; Beveridge, T.J. Interaction of gentamicin with the A band and B band lipopolysaccharides of Pseudomonas aeruginosa and its possible lethal effect. Antimicrob. Agents Chemother. 1993, 37, 715–721. [Google Scholar] [CrossRef] [PubMed]
- Papp-Wallace, K.M.; Endimiani, A.; Taracila, M.A.; Bonomo, R.A. Carbapenems: Past, present, and future. Antimicrob. Agents Chemother. 2011, 55, 4943–4960. [Google Scholar] [CrossRef]
- Linden, P. Safety profile of meropenem: An updated review of over 6,000 patients treated with meropenem. Drug Saf. 2007, 30, 657–668. [Google Scholar] [CrossRef]
- Baldwin, C.M.; Lyseng-Williamson, K.A.; Keam, S.J. Meropenem: A review of its use in the treatment of serious bacterial infections. Drugs 2008, 68, 803–838. [Google Scholar] [CrossRef] [PubMed]
- Zavascki, A.P.; Klee, B.O.; Bulitta, J.B. Aminoglycosides against carbapenem-resistant Enterobacteriaceae in the critically ill: The pitfalls of aminoglycoside susceptibility. Expert Rev. Anti Infect. Ther. 2017, 15, 519–526. [Google Scholar] [CrossRef]
- Wargo, K.A.; Edwards, J.D. Aminoglycoside-induced nephrotoxicity. J. Pharm. Pract. 2014, 27, 573–577. [Google Scholar] [CrossRef] [PubMed]
- Baciewicz, A.M.; Sokos, D.R.; Cowan, R.I. Aminoglycoside-associated nephrotoxicity in the elderly. Ann. Pharmacother. 2003, 37, 182–186. [Google Scholar] [CrossRef] [PubMed]
- Leite, G.C.; Neto, L.V.P.; Gaudereto, J.J.; de Maio Carrilho, C.M.D.; Rossi, F.; Levin, A.S.; Costa, S. Effect of antibiotics combination and comparison of methods for detection of synergism in multiresistant Gram-negative bacteria. J. Infect. Dis. Ther. 2015, 3, 1–9. [Google Scholar] [CrossRef]
- Petersen, P.J.; Labthavikul, P.; Jones, C.H.; Bradford, P.A. In vitro antibacterial activities of tigecycline in combination with other antimicrobial agents determined by chequerboard and time-kill kinetic analysis. J. Antimicrob. Chemother. 2006, 57, 573–576. [Google Scholar] [CrossRef]
- CLSI. Performance Standards for Antimicrobial Susceptibility Testing. In CLSI Supplement M100; Clinical and Laboratory Standards Institute: Wayne, PA, USA, 2018; Volume 28. [Google Scholar]
- Odds, F.C. Synergy, antagonism, and what the chequerboard puts between them. J. Antimicrob. Chemother. 2003, 52, 1. [Google Scholar] [CrossRef]
- Cebrero-Cangueiro, T.; Álvarez-Marín, R.; Labrador-Herrera, G.; Smani, Y.; Cordero-Matía, E.; Pachón, J.; Pachón-Ibáñez, M.E. In vitro Activity of Pentamidine Alone and in Combination With Aminoglycosides, Tigecycline, Rifampicin, and Doripenem Against Clinical Strains of Carbapenemase-Producing and/or Colistin-Resistant Enterobacteriaceae. Front. Cell. Infect. Microbiol. 2018, 8, 363. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Antibiotics | MIC (µg/mL) | Percentage % | ||||
|---|---|---|---|---|---|---|
| Range | MIC50 | MIC90 | Susceptible | Intermediate | Resistant | |
| Aminoglycoside | ||||||
| Amikacin | 2–> 1024 | 4 | >1024 | 73.7 | 0 | 26.3 |
| Gentamicin | 1–> 1024 | 64 | >1024 | 21 | 5.3 | 73.7 |
| Kanamycin | 8–> 1024 | 128 | >1024 | 21 | 0 | 79 |
| Streptomycin | 16–1024 | 512 | 1024 | 0 | 0 | 100 |
| Tobramycin | 1–> 1024 | 32 | >1024 | 5.3 | 10.5 | 84.2 |
| β-lactam + β-lactamase inhibitor | ||||||
| Cefoperazone-sulbactam | 256–> 1024 | 512 | >1024 | 5.3 | 0 | 94.7 |
| Ceftolozane-tazobactam | 1024–> 1024 | >1024 | >1024 | 5.3 | 0 | 94.7 |
| Carbapenem | ||||||
| Imipenem | 16–128 | 64 | 128 | 0 | 0 | 100 |
| Meropenem | 32–128 | 128 | 128 | 0 | 0 | 100 |
| Cephalosporin | ||||||
| Cefotaxime | 256–> 1024 | >1024 | >1024 | 0 | 0 | 100 |
| Ceftazidime | 1024–> 1024 | >1024 | >1024 | 0 | 0 | 100 |
| Fluoroquinolone | ||||||
| Ciprofloxacin | 0.5–512 | 128 | 256 | 5.3 | 10.5 | 84.2 |
| Levofloxacin | <0.5–64 | 16 | 32 | 26.3 | 0 | 73.7 |
| Glycylcycline | ||||||
| Minocycline | <2–16 | <2 | 16 | 68.4 | 15.8 | 15.8 |
| Tigecycline | 0.0625–4 | 2 | 4 | 21 | 0 | 79 |
| Other | ||||||
| Colistin | 0.25–2 | 0.5 | 2 | 100 | 0 | 0 |
| Fosfomycin | 16–1024 | 16 | 1024 | 89.5 | 0 | 10.5 |
| Clinical Isolate | Source | bla Genotype | MIC (µg/mL) | |||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Carbapenem | Aminoglycoside | |||||||||
| Carbapenemase | ESBL | Imipenem | Meropenem | Amikacin | Gentamicin | Kanamycin | Streptomycin | Tobramycin | ||
| CREC 1 | Rectal | blaNDM-1 | blaCTX-M, blaTEM | 64 (R) | 64 (R) | 2 (S) | 64 (R) | 16 (S) | 1024 (R) | 16 (R) |
| CREC 2 | Rectal | blaNDM-1 | blaCTX-M, blaTEM | 64 (R) | 64 (R) | 2 (S) | 64 (R) | 16 (S) | 1024 (R) | 8 (I) |
| CREC 3 | Rectal | - | blaCTX-M, blaSHV, blaTEM | 128 (R) | 128 (R) | 64 (R) | 64 (R) | 64 (R) | 256 (R) | 128 (R) |
| CREC 4 | Throat | blaNDM-5 | blaCTX-M, blaTEM | 64 (R) | 64 (R) | 4 (S) | 32 (R) | 64 (R) | 512 (R) | 32 (R) |
| CREC 5 | Rectal | blaNDM-5 | blaCTX-M, blaTEM | 64 (R) | 64 (R) | 4 (S) | 64 (R) | 64 (R) | 512 (R) | 32 (R) |
| CREC 6 | Rectal | blaNDM-5 | blaCTX-M, blaTEM | 32 (R) | 64 (R) | 4 (S) | 1 (S) | 32 (S) | 64 (R) | 8 (I) |
| CREC 7 | Throat | blaNDM-1 | blaCTX-M, blaTEM | 128 (R) | 128 (R) | 8 (S) | 128 (R) | 256 (R) | 512 (R) | 64 (R) |
| CREC 8 | Rectal | blaNDM-1 | blaCTX-M, blaTEM | 128 (R) | 128 (R) | 8 (S) | 128 (R) | 128 (R) | 16 (R) | 64 (R) |
| CREC 9 | Environment | blaNDM-1 | blaCTX-M, blaTEM | 64 (R) | 128 (R) | 8 (S) | 64 (R) | 512 (R) | 512 (R) | 64 (R) |
| CREC 10 | Rectal | - | blaTEM | 64 (R) | 128 (R) | 4 (S) | 0.5 (S) | 8 (S) | 32 (R) | 1 (S) |
| CREC 11 | Blood | - | blaCTX-M, blaTEM | 32 (R) | 64 (R) | >1024 (R) | >1024 (R) | >1024 (R) | 32 (R) | >1024 (R) |
| CREC 12 | Blood | blaNDM-5 | blaCTX-M, blaTEM | 64 (R) | 128 (R) | >1024 (R) | >1024 (R) | >1024 (R) | 32 (R) | >1024 (R) |
| CREC 13 | Blood | blaNDM-5 | blaCTX-M, blaTEM | 32 (R) | 128 (R) | 8 (S) | 1 (S) | 128 (R) | 32 (R) | 32 (R) |
| CREC 14 | Blood | blaNDM-5 | blaTEM | 16 (R) | 32 (R) | >1024 (R) | >1024 (R) | >1024 (R) | 1024 (R) | 512 (R) |
| CREC 15 | Blood | blaNDM-5 | blaCTX-M, blaTEM | 64 (R) | 64 (R) | 4 (S) | 1 (S) | 128 (R) | 512 (R) | 16 (R) |
| CREC 16 | Blood | blaNDM-5 | blaCTX-M, blaTEM | 64 (R) | 128 (R) | 2 (S) | 128 (R) | 128 (R) | 512 (R) | 16 (R) |
| CREC 17 | Blood | blaNDM-5 | blaTEM | 64 (R) | 128 (R) | 4 (S) | 64 (R) | 64 (R) | 256 (R) | 16 (R) |
| CREC 18 | Blood | blaNDM-1, blaOXA-48 | blaCTX-M, blaTEM | 64 (R) | 128 (R) | 4 (S) | 64 (R) | 128 (R) | 256 (R) | 32 (R) |
| CREC 19 | Blood | blaNDM-1 | blaCTX-M, blaTEM | 128 (R) | 32 (R) | 128 (R) | 8 (I) | 1024 (R) | 512 (R) | 128 (R) |
| Primer Name | Sequence (5′ to 3′) | Amplicon Size (bp) | Reference | |
|---|---|---|---|---|
| Carbapenemase | ||||
| blaIMP | IMP-F | GGAATAGAGTGGCTTAAYTCTC | 232 | [53] |
| IMP-R | GGTTTAAYAAAACAACCACC | |||
| blaKPC | KPC-F | CGTCTAGTTCTGCTGTCTTG | 798 | |
| KPC-R | CTTGTCATCCTTGTTAGGCG | |||
| blaNDM | NDM-F | GGTTTGGCGATCTGGTTTTC | 621 | |
| NDM-R | CGGAATGGCTCATCACGATC | |||
| blaOXA-48 | OXA-F | GCGTGGTTAAGGATGAACAC | 438 | |
| OXA-R | CATCAAGTTCAACCCAACCG | |||
| blaVIM | VIM-F | GATGGTGTTTGGTCGCATA | 390 | |
| VIM-R | CGAATGCGCAGCACCAG | |||
| Extended-spectrum β-lactamase | ||||
| blaCTX-M | CTX-M-U1 | ATGTGCAGYACCAGTAARGTKATGGC | 573 | [54] |
| CTX-M-U2 | TGGGTRAARTARGTSACCAGAAYCAGCGG | |||
| blaSHV | bla-SHV.SE | ATGCGTTATATTCGCCTGTG | 747 | |
| bla-SHV.AS | TGCTTTGTTATTCGGGCCAA | |||
| blaTEM | TEM-164.S | TCGCCGCATACACTATTCTCAGAATGA | 445 | |
| TEM-165.AS | ACGCTCACCGGCTCCAGATTTAT | |||
| Clinical Isolate | Meropenem + Amikacin | Meropenem + Gentamicin | Meropenem + Kanamycin | Meropenem + Streptomycin | Meropenem + Tobramycin | |||||
|---|---|---|---|---|---|---|---|---|---|---|
| MIC a | ΣFICI | MIC a | ΣFICI | MIC a | ΣFICI | MIC a | ΣFICI | MIC a | ΣFICI | |
| CREC 1 | 8/0.5 | 0.38 (S) | 2/8 | 0.16 (S) | 8/4 | 0.38 (S) | 1/256 | 0.27 (S) | 4/2 | 0.19 (S) |
| CREC 2 | 16/0.125 | 0.31 (S) | 2/8 | 0.16 (S) | 16/4 | 0.50 (S) | 1/256 | 0.27 (S) | 4/2 | 0.31 (S) |
| CREC 3 | 8/16 | 0.31 (S) | 2/16 | 0.27 (S) | 32/8 | 0.38 (S) | 32/32 | 0.38 (S) | 4/8 | 0.09 (S) |
| CREC 4 | 4/1 | 0.31 (S) | 8/8 | 0.38 (S) | 8/16 | 0.38 (S) | 8/64 | 0.25 (S) | 8/4 | 0.25 (S) |
| CREC 5 | 16/0.25 | 0.31 (S) | 2/8 | 0.16 (S) | 4/16 | 0.31 (S) | 8/64 | 0.25 (S) | 8/4 | 0.25 (S) |
| CREC 6 | 8/2 | 0.63 (I) | 8/0.125 | 0.25 (S) | 4/8 | 0.31 (S) | 8/8 | 0.25 (S) | 2/2 | 0.28 (S) |
| CREC 7 | 8/2 | 0.31 (S) | 8/8 | 0.13 (S) | 8/32 | 0.19 (S) | 4/128 | 0.28 (S) | 8/8 | 0.19 (S) |
| CREC 8 | 2/2 | 0.27 (S) | 2/16 | 0.14 (S) | 32/32 | 0.50 (S) | 128/1 | 1.02 (S) | 8/8 | 0.19 (S) |
| CREC 9 | 4/2 | 0.28 (S) | 16/8 | 0.25 (S) | 8/32 | 0.19 (S) | 8/128 | 0.31 (S) | 16/8 | 0.25 (S) |
| CREC 10 | 4/2 | 0.53 (I) | 4/0.125 | 0.28 (S) | 16/2 | 0.38 (S) | 16/8 | 0.38 (S) | 32/0.5 | 0.75 (I) |
| CREC 11 | 32/32 | 0.53 (I) | 16/512 | 0.75 (I) | 64/8 | 1.01 (I) | 64/8 | 1.25 (I) | 64/1024 | 2.00 (I) |
| CREC 12 | 32/256 | 0.50 (S) | 8/128 | 0.19 (S) | 64/8 | 0.51 (I) | 32/8 | 0.50 (S) | 64/8 | 0.51 (I) |
| CREC 13 | 2/2 | 0.27 (S) | 1/0.5 | 0.51 (I) | 2/32 | 0.27 (S) | 4/16 | 0.53 (S) | 2/8 | 0.27 (S) |
| CREC 14 | 16/32 | 0.53 (I) | 0.5/128 | 0.14 (S) | 16/512 | 1.00 (I) | 1/128 | 0.16 (I) | 4/64 | 0.25 (S) |
| CREC 15 | 16/1 | 0.38 (S) | 8/0.25 | 0.31 (S) | 2/32 | 0.27 (S) | 32/1 | 0.25 (S) | 8/4 | 0.31 (S) |
| CREC 16 | 64/0.25 | 0.63 (I) | 4/16 | 0.16 (S) | 4/32 | 0.28 (S) | 8/128 | 0.31 (I) | 16/2 | 0.25 (S) |
| CREC 17 | 32/2 | 0.75 (I) | 4/8 | 0.16 (S) | 16/16 | 0.38 (S) | 8/64 | 0.31 (S) | 8/8 | 0.56 (I) |
| CREC 18 | 32/1 | 0.50 (S) | 2/16 | 0.27 (S) | 16/32 | 0.38 (S) | 8/64 | 0.31 (S) | 4/8 | 0.28 (S) |
| CREC 19 | 2/32 | 0.31 (S) | 16/2 | 0.75 (I) | 4/512 | 0.63 (I) | 4/128 | 0.38 (S) | 8/32 | 0.50 (S) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Terbtothakun, P.; Nwabor, O.F.; Siriyong, T.; Voravuthikunchai, S.P.; Chusri, S. Synergistic Antibacterial Effects of Meropenem in Combination with Aminoglycosides against Carbapenem-Resistant Escherichia coli Harboring blaNDM-1 and blaNDM-5. Antibiotics 2021, 10, 1023. https://doi.org/10.3390/antibiotics10081023
Terbtothakun P, Nwabor OF, Siriyong T, Voravuthikunchai SP, Chusri S. Synergistic Antibacterial Effects of Meropenem in Combination with Aminoglycosides against Carbapenem-Resistant Escherichia coli Harboring blaNDM-1 and blaNDM-5. Antibiotics. 2021; 10(8):1023. https://doi.org/10.3390/antibiotics10081023
Chicago/Turabian StyleTerbtothakun, Pawarisa, Ozioma Forstinus Nwabor, Thanyaluck Siriyong, Supayang P. Voravuthikunchai, and Sarunyou Chusri. 2021. "Synergistic Antibacterial Effects of Meropenem in Combination with Aminoglycosides against Carbapenem-Resistant Escherichia coli Harboring blaNDM-1 and blaNDM-5" Antibiotics 10, no. 8: 1023. https://doi.org/10.3390/antibiotics10081023
APA StyleTerbtothakun, P., Nwabor, O. F., Siriyong, T., Voravuthikunchai, S. P., & Chusri, S. (2021). Synergistic Antibacterial Effects of Meropenem in Combination with Aminoglycosides against Carbapenem-Resistant Escherichia coli Harboring blaNDM-1 and blaNDM-5. Antibiotics, 10(8), 1023. https://doi.org/10.3390/antibiotics10081023