
First Case of Bacteraemia Due to Carbapenem-Resistant Bacteroides faecis

 ,
,
Abstract
1. Introduction
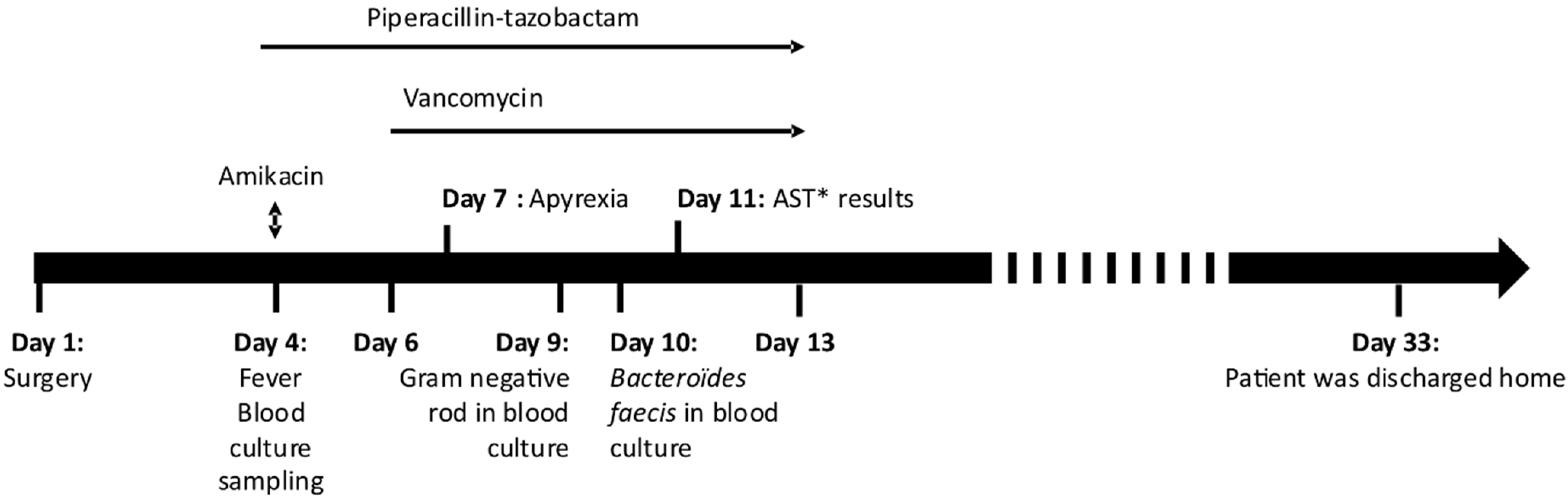
2. Case Report
3. Discussion
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Abadi, A.T.B.; Rizvanov, A.A.; Haertlé, T.; Blatt, N.L. World Health Organization Report: Current Crisis of Antibiotic Resistance. BioNanoScience 2019, 9, 778–788. [Google Scholar] [CrossRef]
- Nagy, E.; Urbán, E.; Nord, C.E. Antimicrobial susceptibility of Bacteroides fragilis group isolates in Europe: 20 years of experience. Clin. Microbiol. Infect. 2011, 17, 371–379. [Google Scholar] [CrossRef] [PubMed]
- Ogane, K.; Tarumoto, N.; Kodana, M.; Onodera, A.; Imai, K.; Sakai, J.; Kawamura, T.; Takeuchi, S.; Murakami, T.; Mitsutake, K.; et al. Antimicrobial susceptibility and prevalence of resistance genes in Bacteroides fragilis isolated from blood culture bottles in two tertiary care hospitals in Japan. Anaerobe 2020, 64, 102215. [Google Scholar] [CrossRef]
- Brook, I. The role of anaerobic bacteria in bacteremia. Anaerobe 2010, 16, 183–189. [Google Scholar] [CrossRef] [PubMed]
- Salonen, J.H.; Eerola, E.; Meurman, O. Clinical Significance and Outcome of Anaerobic Bacteremia. Clin. Infect. Dis. 1998, 26, 1413–1417. [Google Scholar] [CrossRef] [PubMed]
- Kim, M.-S.; Roh, S.W.; Bae, J.-W. Bacteroides faecis sp. nov., isolated from human faeces. Int. J. Syst. Evol. Microbiol. 2010, 60, 2572–2576. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Lee, Y.; Kim, H.S.; Yong, D.; Jeong, S.H.; Lee, K.; Chong, Y. Bacteroides faecisandBacteroides intestinalisRecovered from Clinical Specimens of Human Intestinal Origin. Yonsei Med. J. 2015, 56, 292–294. [Google Scholar] [CrossRef] [PubMed]
- Garcia, M.; Bouvet, P.; Petitpas, F.; Jayle, C.; Legeay, C.; Sautereau, J.; Michaud, A.; Burucoa, C.; Plouzeau, C. First case report of a human sepsis involving a recently identified anaerobic agent: Bacteroides faecis. Anaerobe 2016, 42, 74–77. [Google Scholar] [CrossRef] [PubMed]
- Falagas, M.E.; Siakavellas, E. Bacteroides, Prevotella, and Porphyromonas species: A review of antibiotic resistance and therapeutic options. Int. J. Antimicrob. Agents 2000, 15, 1–9. [Google Scholar] [CrossRef]
- Edwards, R. Expression of the carbapenemase gene (cfiA) in Bacteroides fragilis. J. Antimicrob. Chemother. 2000, 46, 1009–1012. [Google Scholar] [CrossRef] [PubMed]
- Justesen, U.S.; Hansen, F.; Østergaard, C.; Schønheyder, H.C.; Hansen, D.S.; Lemming, L.E.; Schumacher, H.; Heltberg, O.; Knudsen, J.D.; Dzajic, E.; et al. High rates of reduced susceptibility in the Bacteroides fragilis group isolated from blood cultures—The first national survey in Denmark. Int. J. Antimicrob. Agents 2013, 42, 188–190. [Google Scholar] [CrossRef] [PubMed]
- Ayala, J.; Quesada, A.; Vadillo, S.; Criado, J.; Píriz, S. Penicillin-binding proteins of Bacteroides fragilis and their role in the resistance to imipenem of clinical isolates. J. Med. Microbiol. 2005, 54, 1055–1064. [Google Scholar] [CrossRef] [PubMed]
- Pumbwe, L.; Ueda, O.; Yoshimura, F.; Chang, A.; Smith, R.L.; Wexler, H.M. Bacteroides fragilis BmeABC efflux systems additively confer intrinsic antimicrobial resistance. J. Antimicrob. Chemother. 2006, 58, 37–46. [Google Scholar] [CrossRef] [PubMed]
- Vogel, M.; Schmitz, R.P.; Hagel, S.; Pletz, M.W.; Gagelmann, N.; Scherag, A.; Schlattmann, P.; Brunkhorst, F.M. Infectious disease consultation for Staphylococcus aureus bacteremia—A systematic review and meta-analysis. J. Infect. 2016, 72, 19–28. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Antibiotic | EUCAST Breakpoints | CASFM Breakpoints | MIC (mg/L) | Interpretation |
|---|---|---|---|---|
| Penicillin | 0.25–0.5 | - | >8 | Resistant |
| Amoxicillin | 0.5–2 | - | >32 | Resistant |
| Amoxicillin/clavulanic acid | 4–8 | 4–8 | >32 | Resistant |
| Piperacillin/tazobactam | 8–16 | 8–16 | >128 | Resistant |
| Piperacillin | 16 | - | >128 | Resistant |
| Cefoxitin | - | - | >64 | Resistant |
| Imipenem | 2–4 | 2–4 | >128 | Resistant |
| Meropenem | 2–8 | 2–8 | >8 | Resistant |
| Chloramphenicol | 8 | 8 | 8 | Susceptible-standard dosing regimen |
| Erythromycin | - | - | >128 | Resistant |
| Clindamycin | 4 | 4 | >64 | Resistant |
| Metronidazole | 4 | 4 | 2 | Susceptible-standard dosing regimen |
| Moxifloxacin | - | 1–2 | 2 | Susceptible-increased exposure |
| Tetracycline | - | - | >16 | Resistant |
| Vancomycin | - | - | 4 | Resistant |
| Reference | Type of Infection | Risk Factors | Resistance | Treatment | Outcome |
|---|---|---|---|---|---|
| Lee et al. 2015 [7] | Post-operative peritonitis | Sigmoid colon cancer | Piperacillin (SIE), cefoxitin, cefotetan | Piperacillin-tazobactam | Favorable |
| Lee et al. 2015 [7] | Bacteremia secondary to post-operative peritonitis | Rectal cancer | Piperacillin (SIE), cefoxitin, cefotetan | Piperacillin-tazobactam | Favorable |
| Garcia et al. 2016 [8] | Bacteremia secondary to colonic ischemia | Epicardic electrodes | Amoxicillin, piperacillin, clindamycin | Metronidazole | Death |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kaeuffer, C.; Ruge, T.; Diancourt, L.; Romain, B.; Ruch, Y.; Jaulhac, B.; Boyer, P.H. First Case of Bacteraemia Due to Carbapenem-Resistant Bacteroides faecis. Antibiotics 2021, 10, 319. https://doi.org/10.3390/antibiotics10030319
Kaeuffer C, Ruge T, Diancourt L, Romain B, Ruch Y, Jaulhac B, Boyer PH. First Case of Bacteraemia Due to Carbapenem-Resistant Bacteroides faecis. Antibiotics. 2021; 10(3):319. https://doi.org/10.3390/antibiotics10030319
Chicago/Turabian StyleKaeuffer, Charlotte, Tiffany Ruge, Laure Diancourt, Benoît Romain, Yvon Ruch, Benoît Jaulhac, and Pierre H. Boyer. 2021. "First Case of Bacteraemia Due to Carbapenem-Resistant Bacteroides faecis" Antibiotics 10, no. 3: 319. https://doi.org/10.3390/antibiotics10030319
APA StyleKaeuffer, C., Ruge, T., Diancourt, L., Romain, B., Ruch, Y., Jaulhac, B., & Boyer, P. H. (2021). First Case of Bacteraemia Due to Carbapenem-Resistant Bacteroides faecis. Antibiotics, 10(3), 319. https://doi.org/10.3390/antibiotics10030319