
Impact of an Antibiotic Stewardship Program on the Incidence of Resistant Escherichia coli: A Quasi-Experimental Study

 ,
, 
Abstract
1. Introduction
2. Results
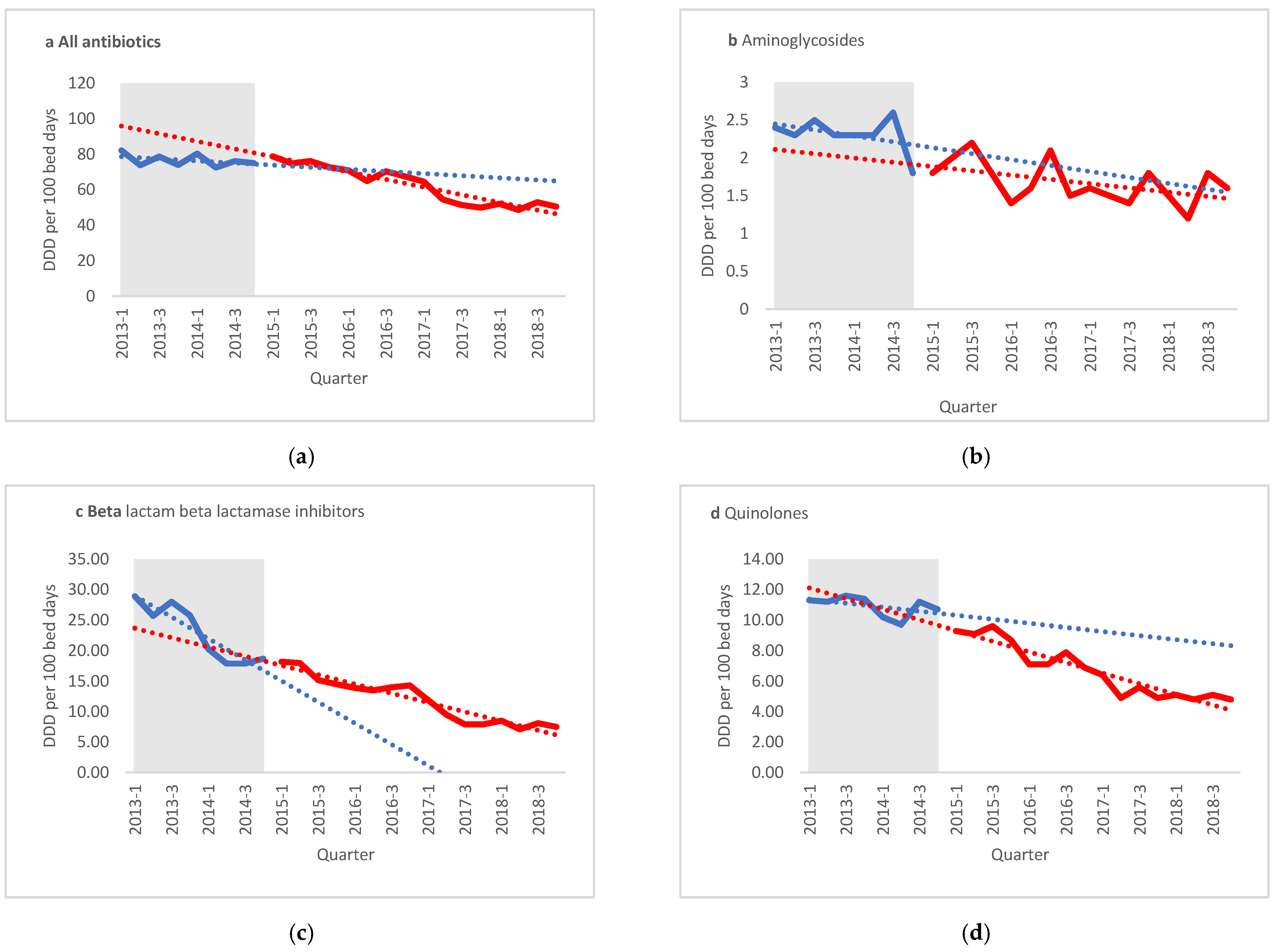
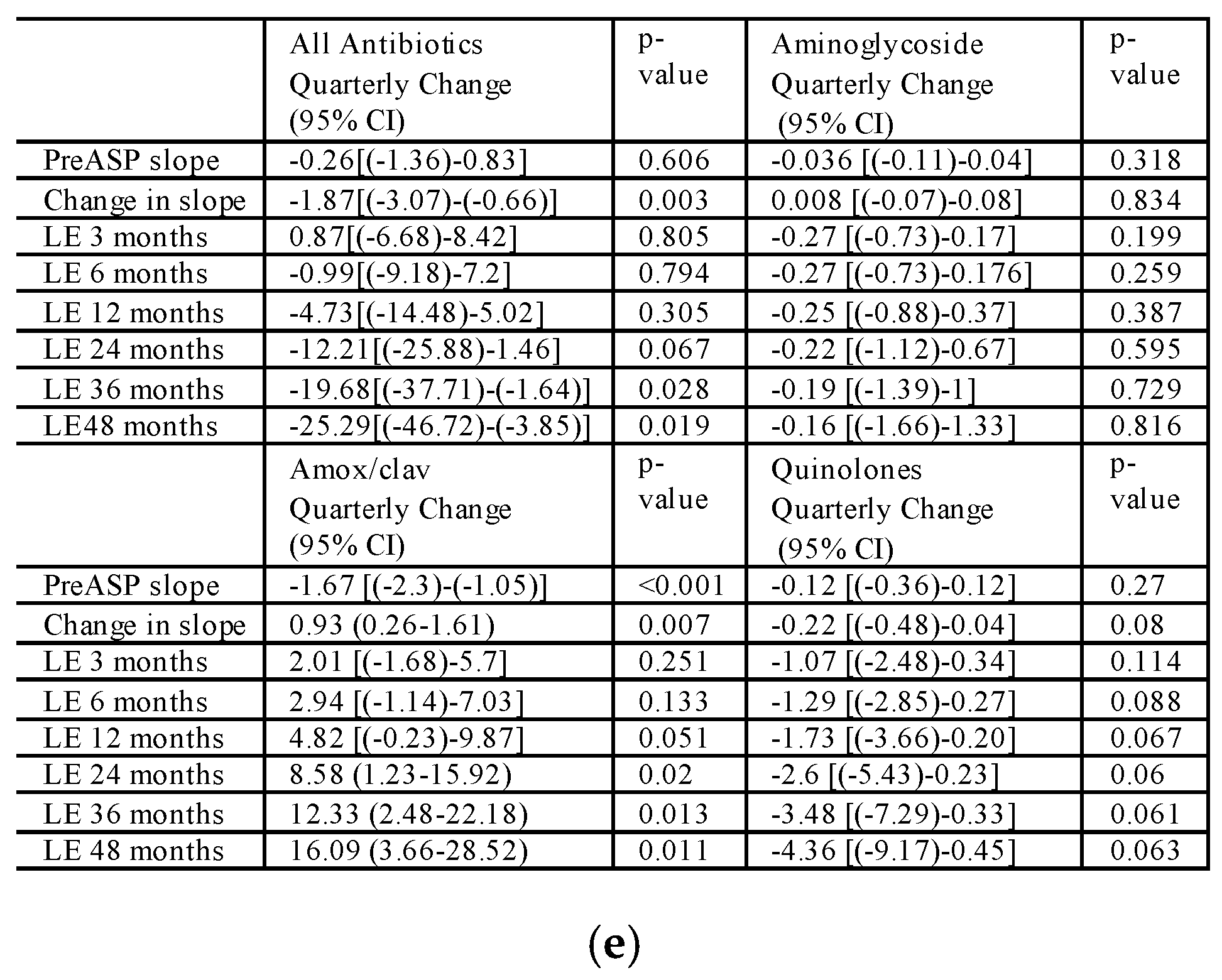
2.1. Change in Antibiotics Use during the Study
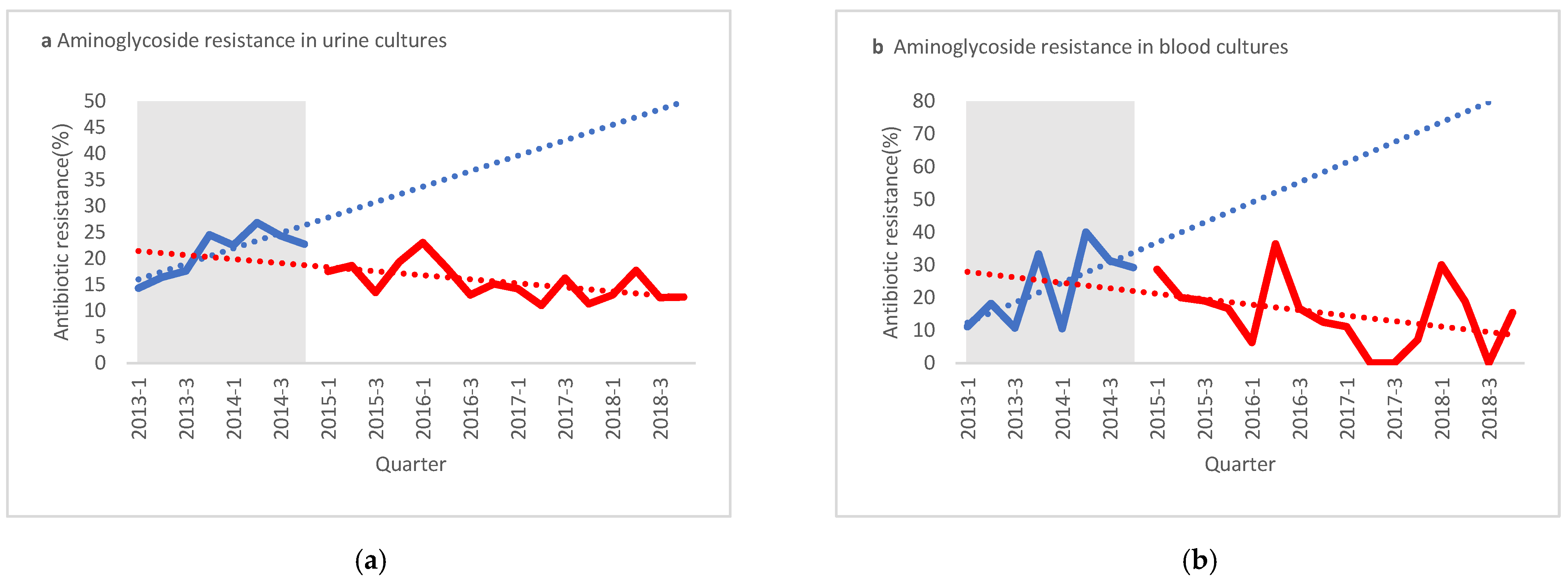
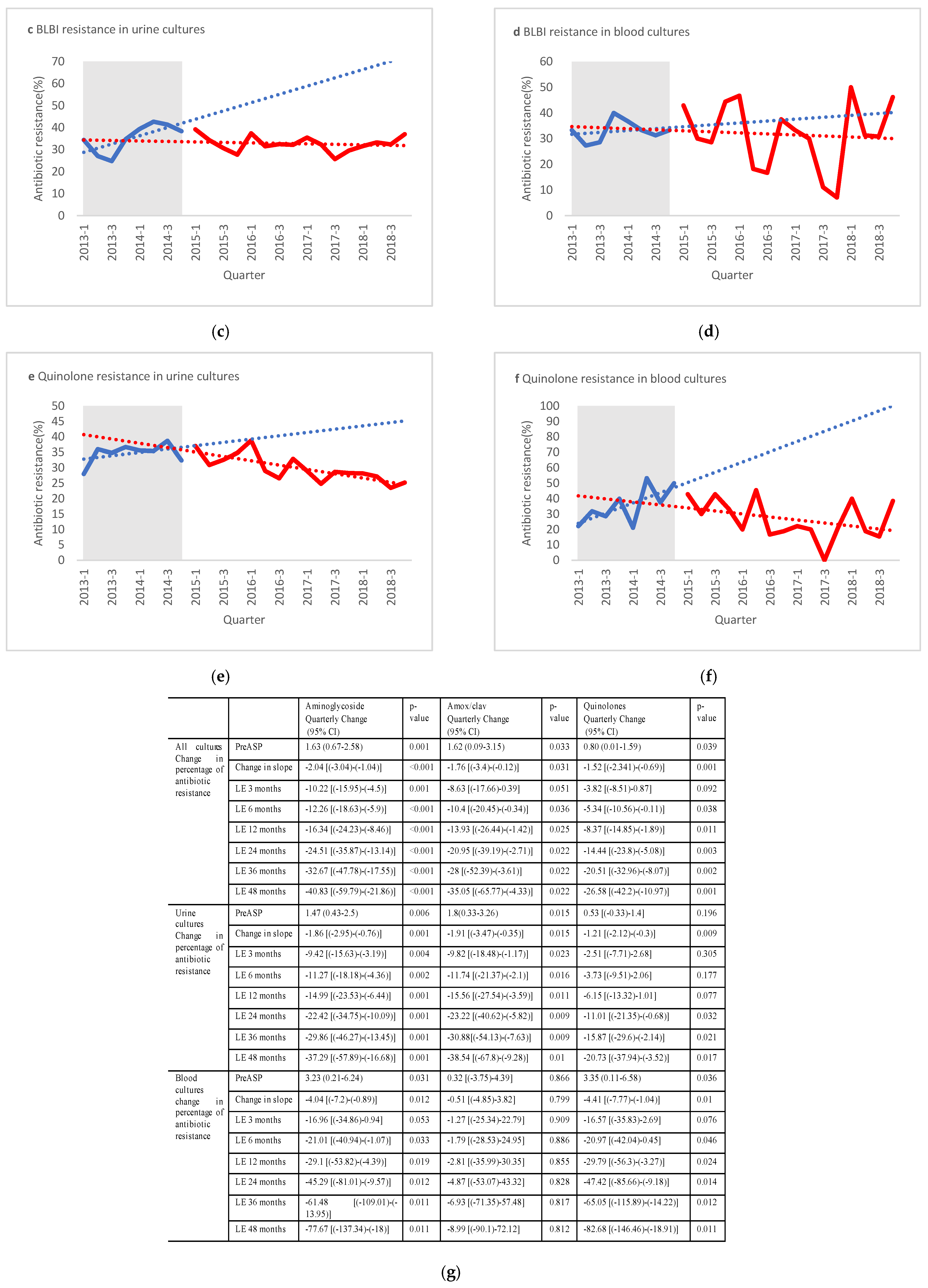
2.2. Change in E. coli Resistance Rates to Antibiotics during the Study
3. Discussion
4. Materials and Methods
4.1. Intervention
4.2. Study Design and Patients
4.3. Data Sources and Collection
4.4. Outcome Measures
4.5. Statistical Analysis
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Centers for Disease Control and Prevention. Antibiotic Resistance Threats in the United States 2019; Centers for Disease Control and Prevention: Atlanta, GA, USA, 2019. Available online: https://www.cdc.gov/drugresistance/pdf/threats-report/2019-ar-threats-report-508.pdf (accessed on 8 August 2020).
- WHO. Global Antimicrobial Resistance and Use Surveillance System (GLASS) Report. 2020. Available online: https://apps.who.int/iris/bitstream/handle/10665/332081/9789240005587-eng.pdf?ua=1 (accessed on 8 August 2020).
- Melzer, M.; Petersen, I. Mortality following bacteraemic infection caused by extended spectrum beta-lactamase (ESBL) producing E. coli compared to non-ESBL producing E. coli. J. Infect. 2007, 55, 254–259. [Google Scholar] [CrossRef]
- Schwaber, M.J.; Carmeli, Y. Mortality and delay in effective therapy associated with extended-spectrum β-lactamase production in Enterobacteriaceae bacteraemia: A systematic review and meta-analysis. J. Antimicrob. Chemother. 2007, 60, 913–920. [Google Scholar] [CrossRef] [PubMed]
- Dellit, T.H.; Owens, R.C.; McGowan, J.E.; Gerding, D.N.; Weinstein, R.A.; Burke, J.P.; Huskins, W.C.; Paterson, D.L.; Fishman, N.O.; Carpenter, C.F.; et al. Infectious Diseases Society of America and the Society for Healthcare Epidemiology of America guidelines for developing an institutional program to enhance antimicrobial stewardship. Clin. Infect. Dis. 2007, 44, 159–177. [Google Scholar] [CrossRef]
- Blaser, M.J. Antibiotic use and its consequences for the normal microbiome. Science 2016, 352, 544–545. [Google Scholar] [CrossRef] [PubMed]
- Talbot, G.H.; Jezek, A.; Murray, B.E.; Jones, R.N.; Ebright, R.H.; Nau, G.J.; Rodvold, K.A.; Newland, J.G.; Boucher, H.W. The Infectious Diseases Society of America’s 10 × ’20 Initiative (Ten New Systemic Antibacterial Agents FDA-approved by 2020): Is 20 × ’20 a Possibility? Clin. Infect. Dis. 2019, 69, 1–11. [Google Scholar] [CrossRef]
- Pollack, L.A.; Srinivasan, A. Core Elements of Hospital Antibiotic Stewardship Programs from the Centers for Disease Control and Prevention. Clin. Infect. Dis. 2014, 59, S97–S100. [Google Scholar] [CrossRef]
- Barlam, T.F.; Cosgrove, S.E.; Abbo, L.M.; Macdougall, C.; Schuetz, A.N.; Septimus, E.J.; Srinivasan, A.; Dellit, T.H.; Falck-Ytter, Y.T.; Fishman, N.O.; et al. Implementing an antibiotic stewardship program: Guidelines by the Infectious Diseases Society of America and the Society for Healthcare Epidemiology of America. Clin. Infect. Dis. 2016, 62, e51–e77. [Google Scholar] [CrossRef] [PubMed]
- Gerding, D.N. The search for good antimicrobial stewardship. Jt. Comm. J. Qual. Improv. 2001, 27, 403–404. [Google Scholar] [CrossRef]
- Standiford, H.C.; Chan, S.; Tripoli, M.; Weekes, E.; Forrest, G.N. Antimicrobial Stewardship at a Large Tertiary Care Academic Medical Center: Cost Analysis Before, During, and After a 7-Year Program. Infect. Control Hosp. Epidemiol. 2012, 33, 338–345. [Google Scholar] [CrossRef] [PubMed]
- Schuts, E.C.; Hulscher, M.E.J.L.; Mouton, J.W.; Verduin, C.M.; Stuart, J.W.T.C.; Overdiek, H.W.P.M.; van der Linden, P.D.; Natsch, S.; Hertogh, C.M.P.M.; Wolfs, T.F.W.; et al. Current evidence on hospital antimicrobial stewardship objectives: A systematic review and meta-analysis. Lancet Infect. Dis. 2016, 16, 847–856. [Google Scholar] [CrossRef]
- Baur, D.; Gladstone, B.P.; Burkert, F.; Carrara, E.; Foschi, F.; Döbele, S.; Tacconelli, E. Effect of antibiotic stewardship on the incidence of infection and colonisation with antibiotic-resistant bacteria and Clostridium difficile infection: A systematic review and meta-analysis. Lancet Infect. Dis. 2017, 17, 990–1001. [Google Scholar] [CrossRef]
- Johnson, L.S.; MacDougall, C.; Trivedi, K.K. The Legislative Momentum of Antimicrobial Stewardship: The US Perspective. Curr. Treat. Options Infect. Dis. 2016, 8, 93–101. [Google Scholar] [CrossRef]
- Rüttimann, S.; Keck, B.; Hartmeier, C.; Maetzel, A.; Bucher, H.C. Long-Term Antibiotic Cost Savings from a Comprehensive Intervention Program in a Medical Department of a University-Affiliated Teaching Hospital. Clin. Infect. Dis. 2004, 38, 348–356. [Google Scholar] [CrossRef] [PubMed]
- Peragine, C.; Walker, S.A.N.S.E.; Simor, A.; Walker, S.A.N.S.E.; Kiss, A.; Leis, J.A. Impact of a Comprehensive Antimicrobial Stewardship Program on Institutional Burden of Antimicrobial Resistance: A 14-Year Controlled Interrupted Time-series Study. Clin. Infect. Dis. 2019, 71, 2897–2904. [Google Scholar] [CrossRef]
- Peñalva, G.; Fernández-Urrusuno, R.; Turmo, J.M.; Hernández-Soto, R.; Pajares, I.; Carrión, L.; Vázquez-Cruz, I.; Botello, B.; García-Robredo, B.; Cámara-Mestres, M.; et al. Long-term impact of an educational antimicrobial stewardship programme in primary care on infections caused by extended-spectrum β-lactamase-producing Escherichia coli in the community: An interrupted time-series analysis. Lancet Infect. Dis. 2019, 20, 199–207. [Google Scholar] [CrossRef]
- Elnasasra, A.; Alnsasra, H.; Smolyakov, R.; Riesenberg, K.; Nesher, L. Ethnic diversity and increasing resistance patterns of hospitalized community-acquired urinary tract infections in Southern Israel: A prospective study. Isr. Med. Assoc. J. 2017, 19, 538–542. [Google Scholar]
- Boel, J.; Andreasen, V.; Jarløv, J.O.; Østergaard, C.; Gjørup, I.; Bøggild, N.; Arpi, M. Impact of antibiotic restriction on resistance levels of Escherichia coli: A controlled interrupted time series study of a hospital-wide antibiotic stewardship programme. J. Antimicrob. Chemother. 2016, 71, 2047–2051. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Livermore, D.M.; Hope, R.; Reynolds, R.; Blackburn, R.; Johnson, A.P.; Woodford, N. Declining cephalosporin and fluoroquinolone non-susceptibility among bloodstream Enterobacteriaceae from the UK: Links to prescribing change? J. Antimicrob. Chemother. 2013, 68, 2667–2674. [Google Scholar] [CrossRef]
- Claeys, K.C.; Hopkins, T.L.; Vega, A.D.; Heil, E.L. Fluoroquinolone Restriction as an Effective Antimicrobial Stewardship Intervention. Curr. Infect. Dis. Rep. 2018, 20, 7. [Google Scholar] [CrossRef]
- Jones-Dias, D.; Manageiro, V.; Ferreira, E.; Louro, D.; Caniça, M. Diversity of extended-spectrum and plasmid-mediated AmpC β-lactamases in Enterobacteriaceae isolates from portuguese health care facilities. J. Microbiol. 2014, 52, 496–503. [Google Scholar] [CrossRef] [PubMed]
- Knudsen, J.D.; Andersen, S.E. A Multidisciplinary Intervention to Reduce Infections of ESBL- and AmpC-Producing, Gram-Negative Bacteria at a University Hospital. PLoS ONE 2014, 9, e86457. [Google Scholar] [CrossRef] [PubMed]
- Conterno, L.O.; Shymanski, J.; Ramotar, K.; Toye, B.; Zvonar, R.; Roth, V. Impact and cost of infection control measures to reduce nosocomial transmission of extended-spectrum β-lactamase-producing organisms in a non-outbreak setting. J. Hosp. Infect. 2007, 65, 354–360. [Google Scholar] [CrossRef]
- FDA Drug Safety and Availability. FDA Drug Safety Communication: FDA Updates Warnings for Oral and Injectable Fluoroquinolone Antibiotics Due to Disabling Side Effects. 2018. Available online: https://www.fda.gov/drugs/drug-safety-and-availability/fda-drug-safety-communication-fda-updates-warnings-oral-and-injectable-fluoroquinolone-antibiotics (accessed on 18 August 2020).
- Tacconelli, E.; Cataldo, M.A.; Paul, M.; Leibovici, L.; Kluytmans, J.; Schröder, W.; Foschi, F.; De Angelis, G.; De Waure, C.; Cadeddu, C.; et al. STROBE-AMS: Recommendations to optimise reporting of epidemiological studies on antimicrobial resistance and informing improvement in antimicrobial stewardship. BMJ Open 2016, 6, e010134. [Google Scholar] [CrossRef] [PubMed]
- Bauer, A.W.; Kirby, W.M.; Sherris, J.C.; Turck, M. Antibiotic susceptibility testing by a standardized single disk method. Am. J. Clin. Pathol. 1966, 45, 493–496. [Google Scholar] [CrossRef] [PubMed]
- CLSI. Clinical and Laboratory Standards Institute Performance Standards for Antimicrobial Susceptibility Testing an informational Supplement for Global Application Developed through the Clinical and Laboratory Standards Institute Consensus Process. 26th Edition. Available online: www.clsi.org (accessed on 14 May 2019).





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | All Cultures | Urine Cultures | Blood Cultures | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Pre-ASP n = 3182 | Post-ASP n = 2819 | p-value | Pre-ASP n = 2897 | Post-ASP n = 2591 | p-value | Pre-ASP n = 284 | Post-ASP n = 221 | p-value | |
| Gender, n (%) | |||||||||
| Male | 689 (21.7) | 533 (19) | 0.009 | 562 (19.4) | 438 (16.9) | 0.017 | 127 (44.7) | 95 (43) | 0.697 |
| Female | 2491 (78.3) | 2279 (81) | 2334 (80.6) | 2153 (83.1) | 157 (55.3) | 126 (57) | |||
| Age, years, median (IQR 25, 75) | 70 (40, 83) | 63 (30, 81) | <0.001 | 69 (39, 82) | 61 (29, 81) | <0.001 | 73.5 (56, 84) | 71 (57, 85) | 0.82 |
| Internal medicine | 976 (30.7) | 773 (27.5) | <0.001 | 910 (31.4) | 727 (28.1) | <0.001 | 66 (23.2) | 46 (20.8) | 0.1 |
| Surgery | 319 (10) | 225 (8) | 296 (10.2) | 208 (8) | 23 (8.1) | 17 (7.7) | |||
| Gynecology | 254 (8) | 214 (7.6) | 243 (8.4) | 212 (8.2) | 11 (3.9) | 2 (0.9) | |||
| Emergency department | 1407 (44.2) | 1429 (50.8) | 1249 (43.1) | 1285 (49.6) | 158 (55.6) | 144 (65.2) | |||
| Intensive care unit | 143 (4.5) | 99 (3.5) | 121 (4.2) | 90 (3.5) | 22 (7.7) | 9 (4.1) | |||
| Other | 82 (2.6) | 72 (2.6) | 78 (2.7) | 69 (2.7) | 4 (1.4) | 3 (1.4) | |||
| Length of hospitalization, Days, median (IQR 25, 85) | 4 (2, 8) | 3 (1, 7) | <0.001 | 4 (1, 8) | 3 (0, 6) | <0.001 | 7 (3, 14) | 6 (3, 11) | 0.265 |
| Antibiotic | All Cultures Resistant/Tested (%) | Urine Cultures Resistant/Tested (%) | Blood Cultures Resistant/Tested (%) | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Pre-ASP n = 3182 | Post-ASP n = 2819 | p value | Pre-ASP n = 2897 | Post-ASP n = 2591 | p value | Pre-ASP n = 284 | Post-ASP n = 221 | p value | |
| Ampicillin | 2256/3174 (71.1) | 1923/2796 (68.8) | 0.053 | 2059/2896 (71.1) | 1775/2577 (68.9) | 0.074 | 197/277 (71.1) | 143/212 (67.4) | 0.383 |
| Cefuroxime | 842/3174 (26.5) | 943/2788 (33.8) | <0.001 | 762/2896 (26.3) | 845/2570 (32.8) | <0.001 | 80/277 (28.8) | 66/211 (31.2) | 0.566 |
| Gentamycin | 603/3175 (19) | 430/2796 (15.4) | <0.001 | 543/2897 (18.7) | 398/2577 (15.4) | 0.001 | 60/277 (21.6) | 32/212 (15.1) | 0.066 |
| Amox/clav | 943/3175 (29.7) | 910/2788 (32.6) | 0.014 | 857/2897 (29.6) | 839/2570 (32.6) | 0.015 | 86/277 (31) | 68/211 (32.2) | 0.781 |
| Ciprofloxacin | 1074/3175 (33.8) | 833/2787 (29.9) | 0.001 | 975/2897 (33.6) | 773/2569 (30.1) | 0.005 | 99/277 (35.7) | 58/211 (27.5) | 0.053 |
| Tmp/Smx | 1199/3175 (37.8) | 993/2787 (35.6) | 0.075 | 1093/2897 (37.7) | 911/2576 (35.4) | 0.07 | 106/277 (38.3) | 81/211 (38.4) | 0.978 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ziv-On, E.; Friger, M.D.; Saidel-Odes, L.; Borer, A.; Shimoni, O.; Nikonov, A.; Nesher, L. Impact of an Antibiotic Stewardship Program on the Incidence of Resistant Escherichia coli: A Quasi-Experimental Study. Antibiotics 2021, 10, 179. https://doi.org/10.3390/antibiotics10020179
Ziv-On E, Friger MD, Saidel-Odes L, Borer A, Shimoni O, Nikonov A, Nesher L. Impact of an Antibiotic Stewardship Program on the Incidence of Resistant Escherichia coli: A Quasi-Experimental Study. Antibiotics. 2021; 10(2):179. https://doi.org/10.3390/antibiotics10020179
Chicago/Turabian StyleZiv-On, Elad, Michael D Friger, Lisa Saidel-Odes, Abraham Borer, Orly Shimoni, Anna Nikonov, and Lior Nesher. 2021. "Impact of an Antibiotic Stewardship Program on the Incidence of Resistant Escherichia coli: A Quasi-Experimental Study" Antibiotics 10, no. 2: 179. https://doi.org/10.3390/antibiotics10020179
APA StyleZiv-On, E., Friger, M. D., Saidel-Odes, L., Borer, A., Shimoni, O., Nikonov, A., & Nesher, L. (2021). Impact of an Antibiotic Stewardship Program on the Incidence of Resistant Escherichia coli: A Quasi-Experimental Study. Antibiotics, 10(2), 179. https://doi.org/10.3390/antibiotics10020179