
Evaluation of Multidrug-Resistant P. aeruginosa in Healthcare Facility Water Systems


 ,
,  and
and
Abstract
:1. Introduction
2. Results
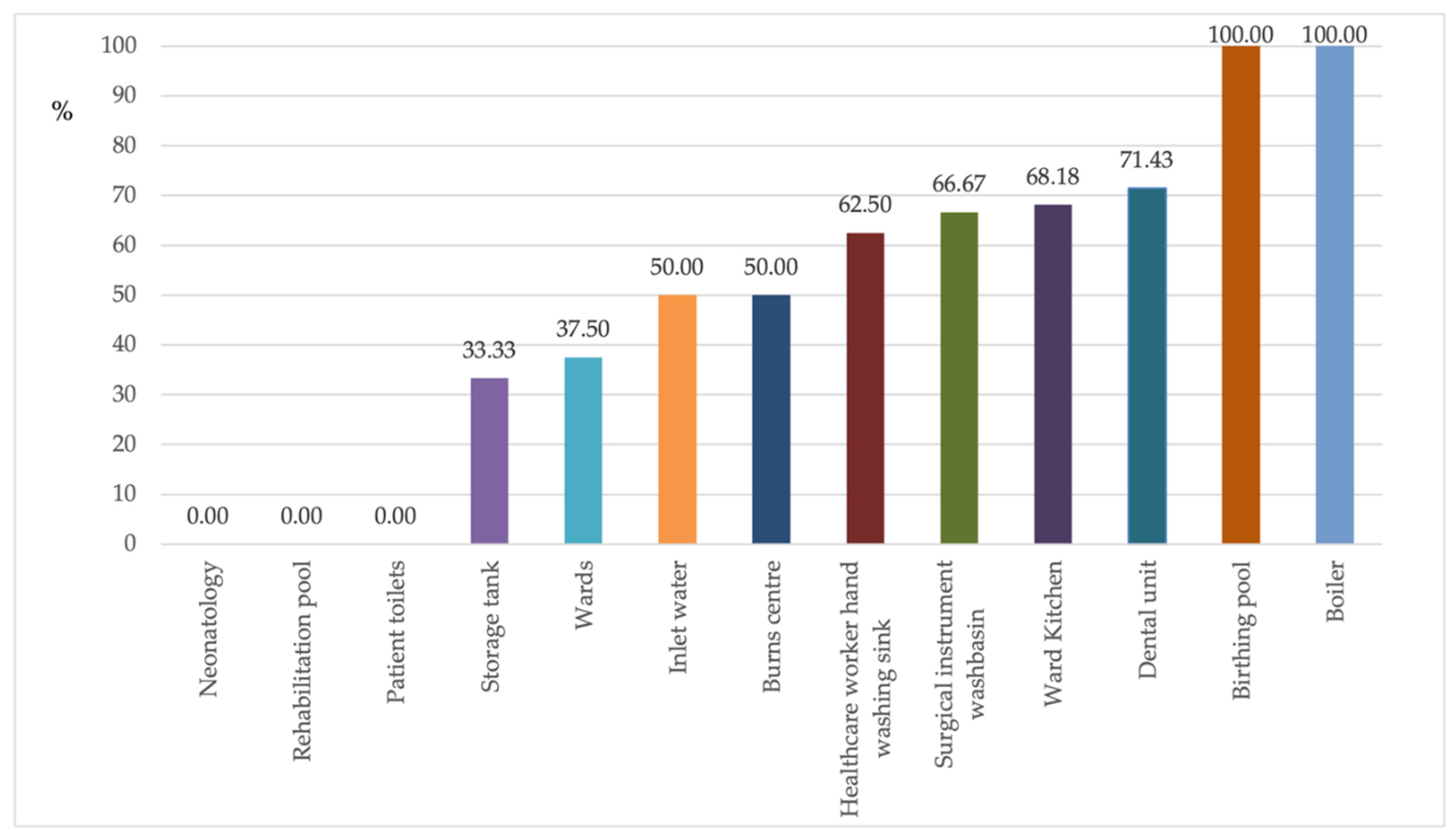
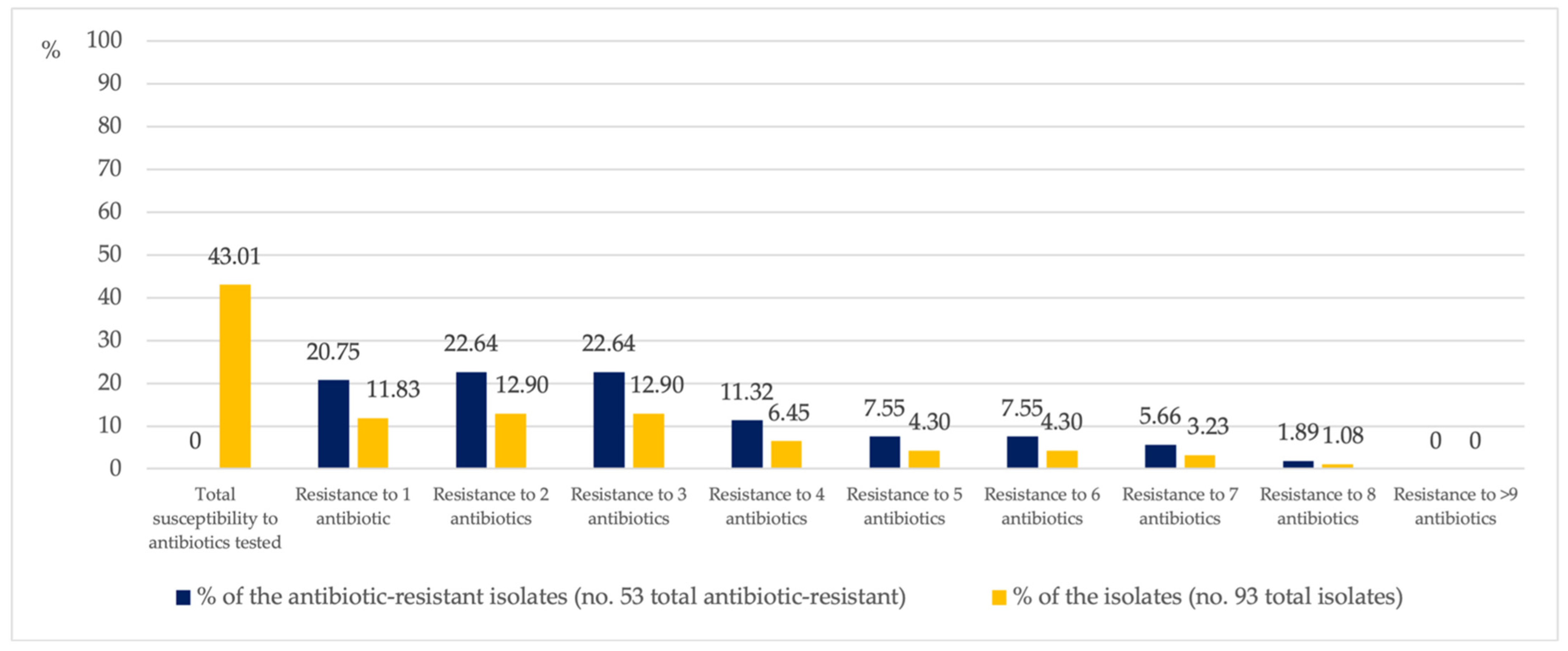
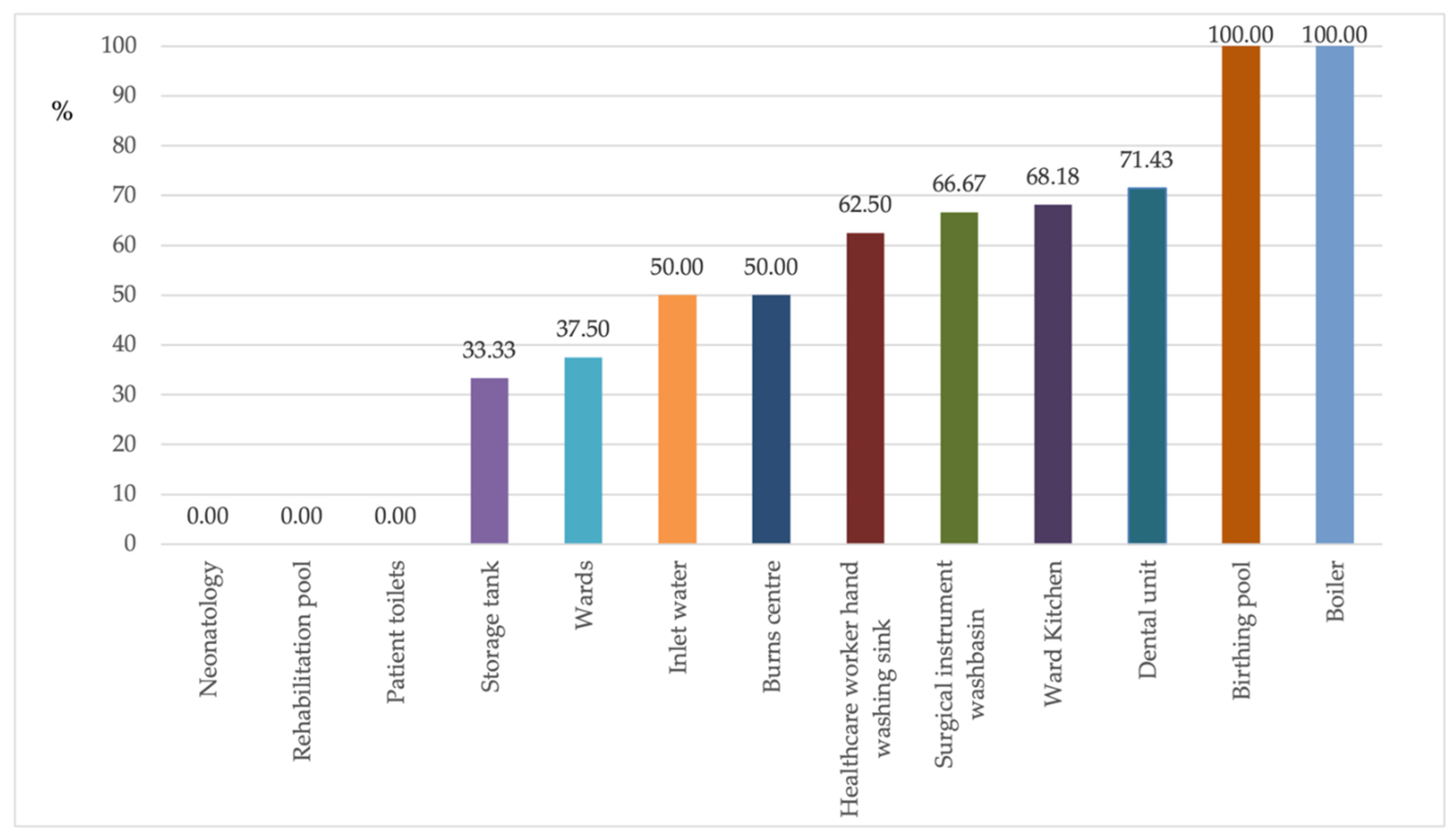
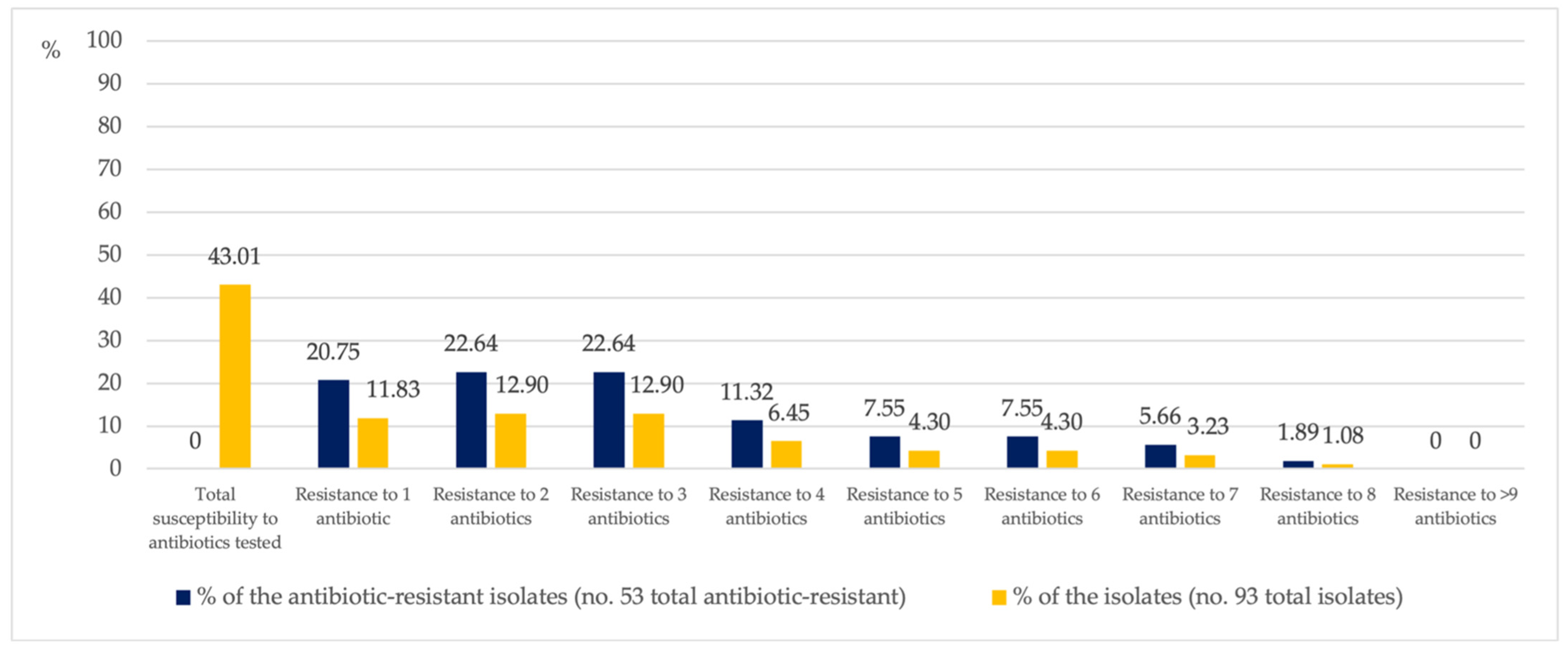
2.1. Multiresistant P. aeruginosa
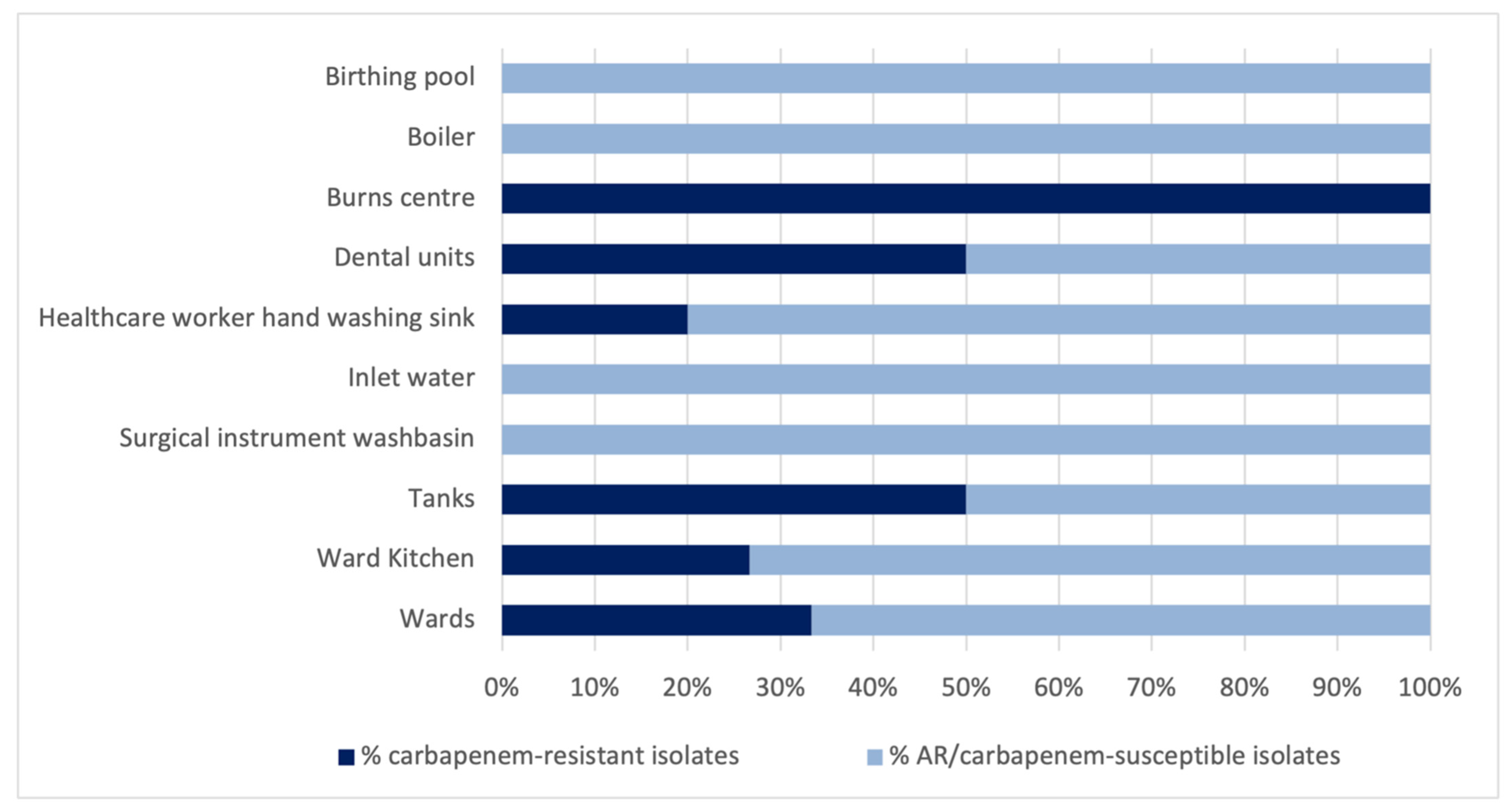
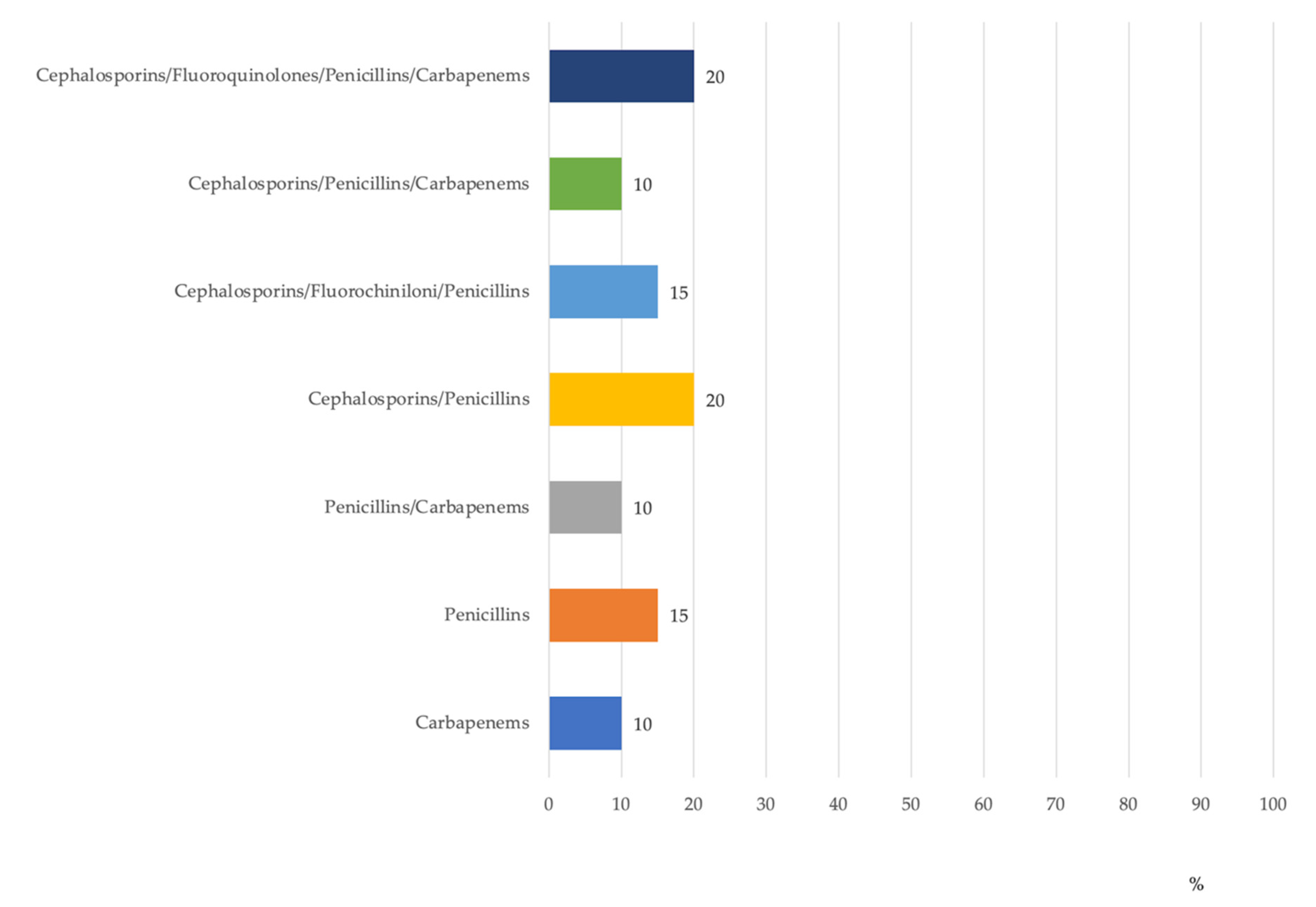
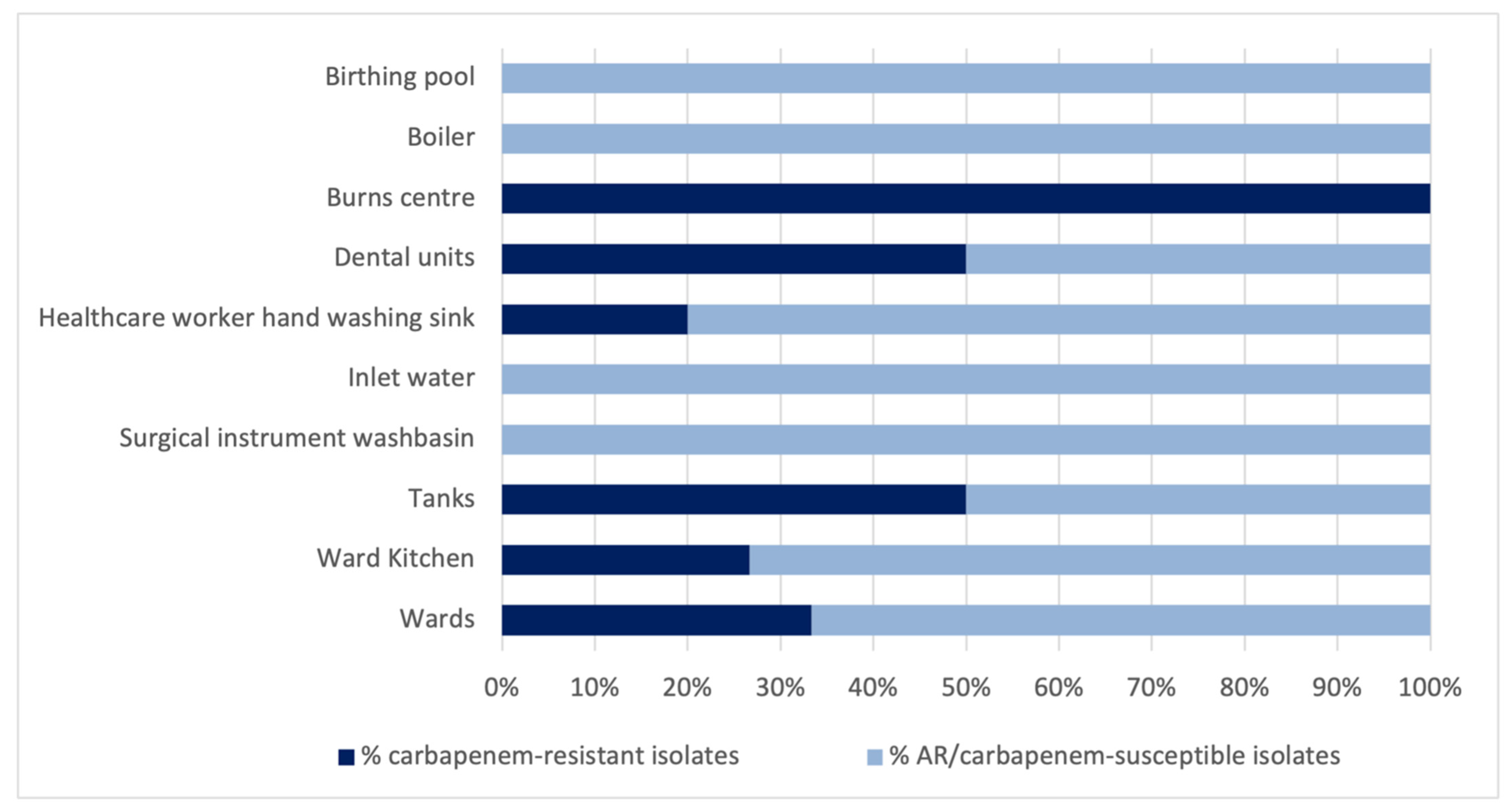
2.2. Carbapenem Resistance
3. Discussion
4. Materials and Methods
4.1. Setting
4.2. Water Sampling and Microbiological Analysis
4.3. Antibiotic Susceptibility Testing
4.4. Statistical Analysis
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Feretzakis, G.; Loupelis, E.; Sakagianni, A.; Skarmoutsou, N.; Michelidou, S.; Velentza, A.; Martsoukou, M.; Valakis, K.; Petropoulou, S.; Koutalas, E. A 2-Year Single-Centre Audit on Antibiotic Resistance of Pseudomonas aeruginosa, Acinetobacter baumannii and Klebsiella pneumoniae Strains from an Intensive Care Unit and Other Wards in a General Public Hospital in Greece. Antibiotics 2019, 8, 62. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bogiel, T.; Prażyńska, M.; Kwiecińska-Piróg, J.; Mikucka, A.; Gospodarek-Komkowska, E. Carbapenem-Resistant Pseudomonas aeruginosa Strains-Distribution of the Essential Enzymatic Virulence Factors Genes. Antibiotics 2021, 10, 8. [Google Scholar] [CrossRef]
- Spagnolo, A.M.; Sartini, M.; Cristina, M.L. Pseudomonas aeruginosa in the healthcare facility setting. Rev. Med. Microbiol. 2021, 32, 169–175. [Google Scholar] [CrossRef]
- Behzadi, P.; Baráth, Z.; Gajdács, M. It’s Not Easy Being Green: A Narrative Review on the Microbiology, Virulence and Therapeutic Prospects of Multidrug-Resistant Pseudomonas aeruginosa. Antibiotics 2021, 10, 42. [Google Scholar] [CrossRef] [PubMed]
- Bédard, E.; Prévost, M.; Déziel, E. Pseudomonas aeruginosa in premise plumbing of large buildings. Microbiologyopen 2016, 5, 937–956. [Google Scholar] [CrossRef] [PubMed]
- Pappa, O.; Apostolos, V.; Galanis, A.; Vantarakis, G.; Mavridou, A. Antibiotic resistance profiles of Pseudomonas aeruginosa isolated from various Greek aquatic environments. FEMS Microbiol. Ecol. 2016, 92, fiw042. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- World Health Organization (WHO). Guidelines for the Prevention and Control of Carbapenem-Resistant Enterobacteriaceae, Acinetobacter Baumannii and Pseudomonas Aeruginosa in Healthcare Facilities. Available online: https://apps.who.int/iris/bitstream/handle/10665/259462/9789241550178-eng.pdf;jsessionid=1D1BF01EC76D852B0261FA36B6A4A582?sequence=1 (accessed on 30 August 2021).
- ECDC. Antimicrobial Resistance in the EU/EEA (EARS-Net). Annual Epidemiological Report for 2019. Available online: https://www.ecdc.europa.eu/en/publications-data/surveillance-antimicrobial-resistance-europe-2019 (accessed on 1 August 2021).
- Pitten, F.A.; Panzig, B.; Schröder, G.; Tietze, K.; Kramer, A. Transmission of a multiresistant Pseudomonas aeruginosa strain at a German University Hospital. J. Hosp. Infect. 2001, 47, 125–130. [Google Scholar] [CrossRef] [PubMed]
- Climo, M.W.; Pastor, A.; Wong, E.S. An outbreak of Pseudomonas aeruginosa related to contaminated urodynamic equipment. Infect. Contr. Hosp. Epidemiol. 1997, 18, 509–510. [Google Scholar] [CrossRef]
- Ferroni, A.; Nguyen, L.; Pron, B.; Quesne, G.; Brusset, M.C.; Berche, P. Outbreak of nosocomial urinary tract infections due to Pseudomonas aeruginosa in a paediatric surgical unit associated with tap-water contamination. J. Hosp. Inf. 1998, 39, 301–307. [Google Scholar] [CrossRef]
- Moolenaar, R.L.; Crutcher, J.M.; San Joaquzin, V.H.; Sewell, L.V.; Hutwagner, L.C.; Carson, L.A.; Robinson, D.A.; Smithee, L.M.; Jarvis, W.R. A prolonged outbreak of Pseudomonas aeruginosa in a neonatal intensive care unit: Did staff fingernails play a role in disease transmission? Infect. Contr. Hosp. Epidemiol. 2000, 21, 80–85. [Google Scholar] [CrossRef] [PubMed]
- Bicking Kinsey, C.; Koirala, S.; Solomon, B.; Rosenberg, J.; Robinson, B.F.; Neri, A.; Laufer Halpin, A.; Arduino, M.J.; Moulton-Meissner, H.; Noble-Wang, J.; et al. Pseudomonas aeruginosa outbreak in a neonatal intensive care unit attributed to hospital tap water. Infect. Contr. Hosp. Epidemiol. 2017, 38, 801–808. [Google Scholar] [CrossRef] [PubMed]
- Döring, G.; Ulrich, M.; Müller, W.; Bitzer, J.; Schmidt-Koenig, L.; Münst, L.; Grupp, H.; Wolz, C.; Stern, M.; Botzenhart, K. Generation of Pseudomonas aeruginosa aerosols during handwashing from contaminated sink drains, transmission to hands of hospital personnel, and its prevention by use of a new heating device. Zentralbl. Hyg. Umweltmed. 1991, 191, 494–505. [Google Scholar] [PubMed]
- Spagnolo, A.M.; Sartini, M.; Cristina, M.L. Microbial contamination of dental unit waterlines and potential risk of infection: A narrative review. Pathogens 2020, 9, 651. [Google Scholar] [CrossRef]
- Tuvo, B.; Totaro, M.; Cristina, M.L.; Spagnolo, A.M.; Di Cave, D.; Profeti, S.; Baggiani, A.; Privitera, G.; Casini, B. Prevention and Control of Legionella and Pseudomonas spp. Colonization in Dental Units. Pathogens 2020, 9, 305. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cristina, M.L.; Spagnolo, A.M.; Orlando, P.; Perdelli, F. The role of the environment in the spread of emerging pathogens in at-risk hospital wards. Rev. Med. Microbiol. 2013, 24, 104–112. [Google Scholar] [CrossRef]
- Cristina, M.L.; Spagnolo, A.M.; Casini, B.; Baggiani, A.; Del Giudice, P.; Brusaferro, S.; Poscia, A.; Moscato, U.; Perdelli, F.; Orlando, P. The impact of aerators on water contamination by emerging gram-negative opportunists in at-risk hospital departments. Infect. Control. Hosp. Epidemiol. 2014, 35, 122–129. [Google Scholar] [CrossRef]
- Montagna, M.T.; Cristina, M.L.; De Giglio, O.; Spagnolo, A.M.; Napoli, C.; Cannova, L.; Deriu, M.G.; Delia, S.A.; Giuliano, A.; Guida, M.; et al. Serological and molecular identification of Legionella spp. isolated from water and surrounding air samples in Italian healthcare facilities. Environ. Res. 2016, 146, 47–50. [Google Scholar] [CrossRef]
- Montagna, M.T.; De Giglio, O.; Napoli, C.; Diella, G.; Rutigliano, S.; Agodi, A.; Auxilia, F.; Baldovin, T.; Bisetto, F.; Arnoldo, L.; et al. Control and prevention measures for legionellosis in hospitals: A cross-sectional survey in Italy. Environ. Res. 2018, 166, 55–60. [Google Scholar] [CrossRef]
- Anaissie, E.J.; Penzak, S.R.; Dignani, M.C. The hospital water supply as a source of nosocomial infections: A plea for action. Arch. Intern. Med. 2002, 162, 1483–1492. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ambrogi, V.; Cavalié, L.; Mantion, B.; Ghiglia, M.J.; Cointault, O.; Dubois, D.; Prère, M.F.; Levitzki, N.; Kamar, N.; Malavaud, S. Transmission of metallo-beta-lactamase-producing Pseudomonas aeruginosa in a nephrology-transplant intensive care unit with potential link to the environment. J. Hosp. Infect. 2016, 92, 27–29. [Google Scholar] [CrossRef] [PubMed]
- Spagnolo, A.M.; Orlando, P.; Perdelli, F.; Cristina, M.L. Hospital water and prevention of waterborne infections. Rev. Med. Microbiol. 2016, 27, 25–32. [Google Scholar] [CrossRef]
- Borges, C.R.M.; Lascowski, K.M.S.; Filho, N.R.; Pelayo, J.S. Microbiological quality of water and dialysate in a haemodialysis unit in Ponta Grossa-PR, Brazil. J. Appl. Microbiol. 2007, 103, 1791–1797. [Google Scholar] [CrossRef]
- Lefebvre, A.; Bertrand, X.; Quantin, C.; Vanhems, P.; Lucet, J.C.; Nuemi, G.; Astruc, K.; Chavanet, P.; Aho-Glélé, L.S. Association between Pseudomonas aeruginosa positive water samples and healthcare-associated cases: Nine-year study at one university hospital. J. Hosp. Infect. 2017, 96, 238–243. [Google Scholar] [CrossRef]
- Schiavano, G.F.; Carloni, E.; Andreoni, F.; Magi, S.; Chironna, M.; Brandi, G.; Amagliani, G. Prevalence and antibiotic resistance of Pseudomonas aeruginosa in water samples in central Italy and molecular characterization of oprD in imipenem resistant isolates. PLoS ONE 2017, 12, e0189172. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ramsay, K.A.; Wardell, S.J.T.; Patrick, W.M.; Brockway, B.; Reid, D.W.; Winstanley, C.; Bell, S.C.; Lamont, I.L. Genomic and phenotypic comparison of environmental and patient-derived isolates of Pseudomonas aeruginosa suggest that antimicrobial resistance is rare within the environment. J. Med. Microbiol. 2019, 68, 1591–1595. [Google Scholar] [CrossRef]
- Hayward, C.; Ross, K.E.; Brown, M.H.; Whiley, H. Water as a Source of Antimicrobial Resistance and Healthcare-Associated Infections. Pathogens 2020, 9, 667. [Google Scholar] [CrossRef] [PubMed]
- Guidelines for Environmental Infection Control in Health-Care Facilities. Recommendations from CDC and the Healthcare Infection Control Practices Advisory Committee (HICPAC). Available online: https://www.cdc.gov/infectioncontrol/guidelines/environmental/index.html (accessed on 30 August 2021).
- Ministère de la Santé e des Solidarités. L’eau dans les établissements de santé. Available online: http://www.sante.gouv.fr/IMG/pdf/Guide_technique_de_l_eau_dans_les_etablissements_de_sante_-_edition_2005.pdf (accessed on 3 June 2021).
- Department of Health. Health Technical Memorandum 04-01: Safe water in Healthcare Premises 2016; The Stationery Office: London, UK, 2016.
- Piano Nazionale di Contrasto dell’Antimicrobico-Resistenza (PNCAR) 2017–2020. Available online: https://www.salute.gov.it/imgs/C_17_pubblicazioni_2660_allegato.pdf (accessed on 3 June 2021).
- ECDC. Surveillance of Antimicrobial Resistance in Europe 2018. Available online: https://www.ecdc.europa.eu/en/publications-data/surveillance-antimicrobial-resistance-europe-2018 (accessed on 13 October 2020).
- Davis, R.; Brown, P.D. Multiple antibiotic resistance index, fitness and virulence potential in respiratory Pseudomonas aeruginosa from Jamaica. J. Med. Microbiol. 2016, 65, 261–271. [Google Scholar] [CrossRef]
- Krumperman, P.H. Multiple antibiotic resistance indexing of Escherichia coli to identify high-risk sources of fecal contamination of foods. Appl. Environ. Microbiol. 1983, 46, 165–170. [Google Scholar] [CrossRef] [Green Version]
- Panghal, M.; Singh, K.; Kadyan, S.; Chaudary, U.; Yadav, J.P. The analysis of distribution of multidrug resistant Pseudomonas and Bacillus species from burn patients and burn ward environment. Burns 2015, 41, 812–819. [Google Scholar] [CrossRef] [PubMed]
- Thi, M.T.T.; Wibowo, D.; Rehm, B.H.A. Pseudomonas aeruginosa Biofilms. Int. J. Mol. Sci. 2020, 21, 8671. [Google Scholar] [CrossRef]
- Maurice, N.M.; Bedi, B.; Sadikot, R.T. Pseudomonas aeruginosa biofilms: Host response and clinical implications in lung infections. Am. J. Respir. Cell. Mol. Biol. 2018, 58, 428–439. [Google Scholar] [CrossRef]
- Spagnolo, A.M.; Sartini, M.; Cave, D.D.; Casini, B.; Tuvo, B.; Cristina, M.L. Evaluation of Microbiological and Free-Living Protozoa Contamination in Dental Unit Waterlines. Int. J. Environ. Res. Public Health 2019, 16, 2648. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Costa, D.; Mercier, A.; Gravouil, K.; Lesobre, J.; Delafont, V.; Bousseau, A.; Verdon, J.; Imbert, C. Pyrosequencing analysis of bacterial diversity in dental unit waterlines. Water Res. 2015, 81, 223–231. [Google Scholar] [CrossRef] [PubMed]
- Lizzadro, J.; Mazzotta, M.; Girolamini, L.; Dormi, A.; Pellati, T.; Cristino, S. Comparison between Two Types of Dental Unit Waterlines: How Evaluation of Microbiological Contamination Can Support Risk Containment. Int. J. Environ. Res. Public Health 2019, 16, 328. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- de Oliveira, A.C.; Maluta, R.P.; Stella, A.E.; Rigobelo, E.C.; Marin, J.M.; Ávila, F.A. Isolation of Pseudomonas aeruginosa strains from dental office environments and units in Barretos, state of São Paulo, Brazil, and analysis of their susceptibility to antimicrobial drugs. Braz. J. Microbiol. 2008, 39, 579–584. [Google Scholar] [CrossRef] [PubMed]
- Persoon, M.C.; Voor, A.F.; Wielders, C.C.H.; Gommers, D.; Vos, M.C.; Severin, J.A. Mortality associated with carbapenem-susceptible and Verona Integron-encoded Metallo-β-lactamase-positive Pseudomonas aeruginosa bacteremia. Antimicrob. Resist. Infect. Control 2020, 9, 25. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization (WHO). Water Safety Plan Manual: Step-by-Step Risk Management for Drinking-Water Suppliers. Available online: https://apps.who.int/iris/bitstream/handle/10665/75141/9789241562638_eng.pdf?sequence=1&isAllowed=y (accessed on 30 August 2021).
- Casini, B.; Buzzigoli, A.; Cristina, M.L.; Spagnolo, A.M.; Del Giudice, P.; Brusaferro, S.; Poscia, A.; Moscato, U.; Valentini, P.; Baggiani, A.; et al. Long-term effects of hospital water network disinfection on Legionella and other waterborne bacteria in an Italian university hospital. Infect. Control Hosp. Epidemiol. 2014, 35, 293–299. [Google Scholar] [CrossRef] [PubMed]
- Vonberg, R.P.; Sohr, D.; Bruderek, J.; Gastmeier, P. Impact of a silver layer on the membrane of tap water filters on the microbiological quality of filtered water. BMC Infect. Dis. 2008, 8, 133. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Reuter, S.; Sigge, A.; Wiedeck, H.; Trautmann, M. Analysis of transmission pathways of Pseudomonas aeruginosa between patients and tap water outlets. Crit. Care Med. 2002, 30, 2222–2228. [Google Scholar] [CrossRef]
- UNI EN ISO 16266: 2008 Water Quality. Detection and Enumeration of Pseudomonas Aeruginosa. Method by Membrane Filtration; Technical committee ISO/TC 147, Subcommittee SC 4; International Organization for Standardization: Geneva, Switzerland, 2008. [Google Scholar]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Sampling Points | % of P. aeruginosa Isolates Tested (No.) | % of Antibiotic-Resistant P. aeruginosa Strains (No.) |
|---|---|---|
| Dental unit | 30.11 (28) | 37.74 (20) |
| Ward kitchen | 23.66 (22) | 28.30 (15) |
| Ward | 8.60 (8) | 5.66 (3) |
| Healthcare worker hand-washing sink | 8.60 (8) | 9.43 (5) |
| Storage tank | 6.45 (6) | 3.77 (2) |
| Neonatology | 4.30 (4) | 0 |
| Rehabilitation pool | 4.30 (4) | 0 |
| Surgical instrument washing sink | 3.23 (3) | 3.77 (2) |
| Birthing pool | 3.23 (3) | 5.66 (3) |
| Inlet water | 2.15 (2) | 1.89 (1) |
| Burns centre | 2.15 (2) | 1.89 (1) |
| Patient toilets | 2.15 (2) | 0 |
| Boiler | 1.08 (1) | 1.89 (1) |
| Total | 100 (93) | 100 (53) |
| Antibiotic Group | Antibiotics Tested | No. Resistant Isolates | % of the Antibiotic-Resistant Isolates (No. 53 Total Antibiotic-Resistant) | % of the Isolates (No. 93 Total Isolates) |
|---|---|---|---|---|
| Aminoglycosides | Amikacin | 0 | 0 | 0 |
| Gentamicin | 1 | 1.89 | 1.08 | |
| Tobramycin | 1 | 1.89 | 1.08 | |
| Cephalosporins | Cefepime | 25 | 47.17 | 26.88 |
| Ceftazidime | 11 | 20.75 | 11.83 | |
| Fluoroquinolones | Ciprofloxacin | 7 | 13.21 | 7.53 |
| Levofloxacin | 24 | 45.28 | 25.81 | |
| Penicillins | Piperacillin | 40 | 75.47 | 43.01 |
| Piperacillin/Tazobactam | 37 | 69.81 | 39.78 | |
| Carbapenems | Imipenem | 18 | 33.96 | 19.35 |
| Meropenem | 4 | 7.55 | 4.30 |
| Resistance Pattern | No. Isolates | % of the Antibiotic-Resistant Isolates (No. 53 Total Antibiotic-Resistant) | % of the Isolates (No. 93 Total Isolates) |
|---|---|---|---|
| Total susceptibility to the antibiotics tested | 40 | - | 43.01 |
| Resistance to 1 group of antibiotics | 20 | 37.74 | 21.51 |
| Resistance to 2 groups of antibiotics | 16 | 30.19 | 17.20 |
| Resistance to 3 groups of antibiotics | 8 | 15.09 | 8.60 |
| Resistance to 4 groups of antibiotics | 9 | 16.98 | 9.68 |
| Resistance to 5 groups of antibiotics | 0 | 0 | 0 |
| Total | 93 |
| Pattern | No. of Isolates Showing Profile | Resistance Phenotype | MAR Index |
|---|---|---|---|
| 1 | 4 | PIP | 0.09 |
| 2 | 5 | LVX | 0.09 |
| 3 | 1 | IPM | 0.09 |
| 4 | 1 | TZP | 0.09 |
| 5 | 1 | CIP, LVX | 0.18 |
| 6 | 7 | PIP, TZP | 0.18 |
| 7 | 1 | TOB, CPM | 0.18 |
| 8 | 1 | LVX, TZP | 0.18 |
| 9 | 1 | IPM, MEM | 0.18 |
| 10 | 3 | PIP, TZP, IPM | 0.27 |
| 11 | 1 | LVX, PIP, TZP | 0.27 |
| 12 | 6 | CPM, PIP, TZP | 0.27 |
| 13 | 2 | CPM, LVX, PIP | 0.27 |
| 14 | 1 | GEN, CIP, LVX | 0.27 |
| 15 | 1 | LVX, PIP, TZP, IPM | 0.36 |
| 16 | 2 | CPM, CAZ, PIP, TZP | 0.36 |
| 17 | 2 | CPM, PIP, TZP, IPM | 0.36 |
| 18 | 1 | PIP, TZP, IPM, MEM | 0.36 |
| 19 | 1 | CPM, CIP, LVX, PIP, TZP | 0.45 |
| 20 | 2 | CPM, CAZ, LVX, PIP, TZP | 0.45 |
| 21 | 1 | CPM, LVX, PIP, TZP, IPM | 0.45 |
| 22 | 4 | CPM, CAZ, LVX, PIP, TZP, IPM | 0.55 |
| 23 | 2 | CPM, CAZ, CIP, LVX, PIP, TZP, IPM | 0.64 |
| 24 | 1 | CPM, CIP, LVX, PIP, TZP, IPM, MEM | 0.64 |
| 25 | 1 | CPM, CAZ, CIP, LVX, PIP, TZP, IPM, MEM | 0.73 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cristina, M.L.; Sartini, M.; Schinca, E.; Ottria, G.; Casini, B.; Spagnolo, A.M. Evaluation of Multidrug-Resistant P. aeruginosa in Healthcare Facility Water Systems. Antibiotics 2021, 10, 1500. https://doi.org/10.3390/antibiotics10121500
Cristina ML, Sartini M, Schinca E, Ottria G, Casini B, Spagnolo AM. Evaluation of Multidrug-Resistant P. aeruginosa in Healthcare Facility Water Systems. Antibiotics. 2021; 10(12):1500. https://doi.org/10.3390/antibiotics10121500
Chicago/Turabian StyleCristina, Maria Luisa, Marina Sartini, Elisa Schinca, Gianluca Ottria, Beatrice Casini, and Anna Maria Spagnolo. 2021. "Evaluation of Multidrug-Resistant P. aeruginosa in Healthcare Facility Water Systems" Antibiotics 10, no. 12: 1500. https://doi.org/10.3390/antibiotics10121500
APA StyleCristina, M. L., Sartini, M., Schinca, E., Ottria, G., Casini, B., & Spagnolo, A. M. (2021). Evaluation of Multidrug-Resistant P. aeruginosa in Healthcare Facility Water Systems. Antibiotics, 10(12), 1500. https://doi.org/10.3390/antibiotics10121500