
Local/Topical Antibiotics for Peri-Implantitis Treatment: A Systematic Review

 ,
,  ,
,
Abstract
:1. Introduction
2. Methods
2.1. Study Selection
2.2. Inclusion/Exclusion Criteria
2.3. Data Extraction
- Study characteristics: name of the first author, year, country, disease (peri-implantitis or peri-implant mucositis), study design, blinding, type of intervention (surgical vs. non-surgical), follow-up;
- Participant characteristics: implant numbers/subjects, inclusion criteria;
- Treatment and control groups characteristics;
- Primary and secondary outcomes;
- Results
2.4. Risk of Bias
3. Results
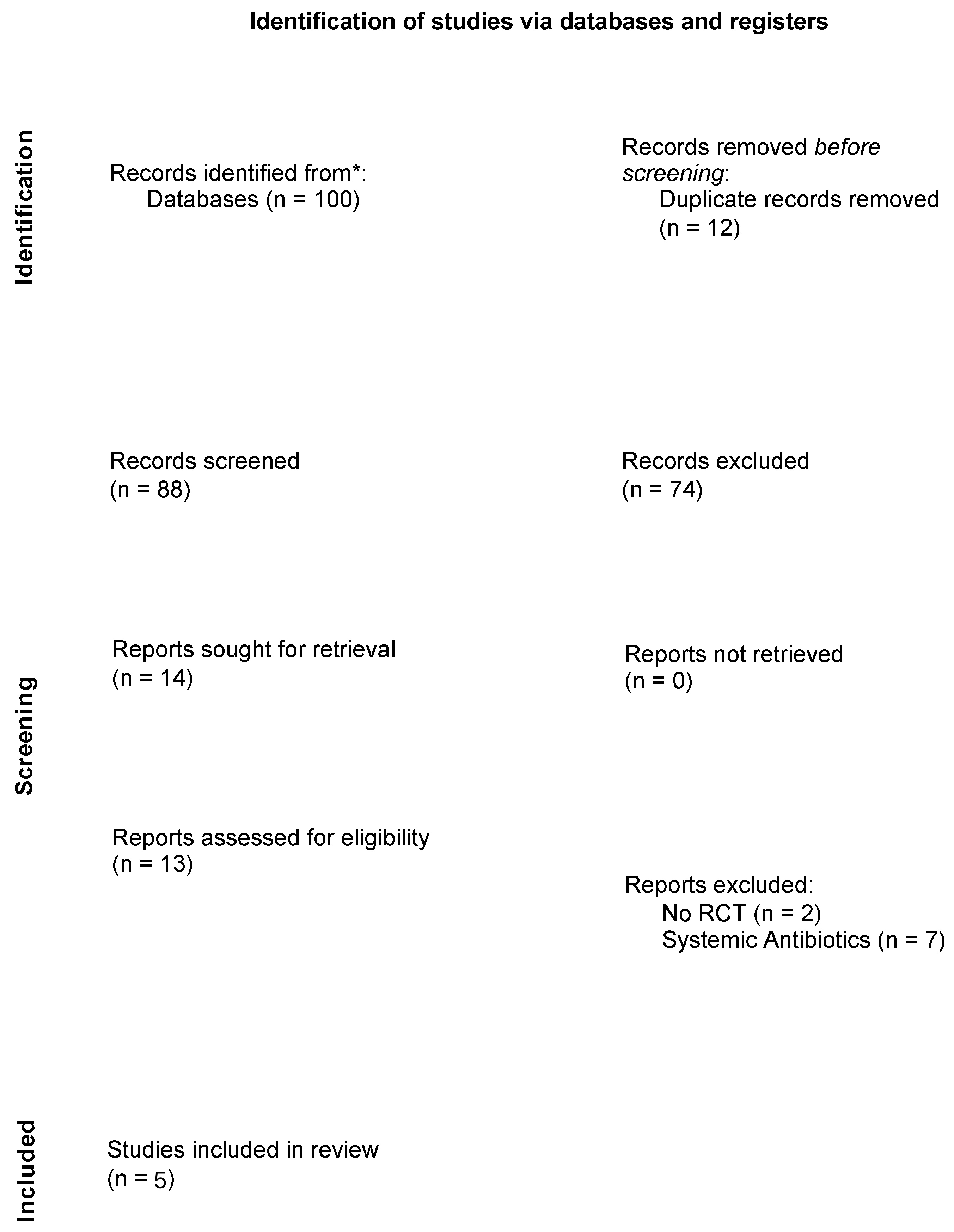
3.1. Study Selection
3.2. Risk of Bias
3.3. Study Characteristics
3.4. Doxycycline Efficacy
3.5. Minocycline Efficacy
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Pjetursson, B.E.; Tan, K.; Lang, N.P.; Bragger, U.; Egger, M.; Zwahlen, M. A systematic review of the survival and complication rates of fixed partial dentures (FPDs) after an observation period of at least 5 years. Clin. Oral Implants Res. 2004, 15, 625–642. [Google Scholar] [CrossRef]
- Lee, C.T.; Huang, Y.W.; Zhu, L.; Weltman, R. Prevalences of peri-implantitis and peri-implant mucositis: Systematic review and meta-analysis. J. Dent. 2017, 62, 1–12. [Google Scholar] [CrossRef]
- Smeets, R.; Henningsen, A.; Jung, O.; Heiland, M.; Hammacher, C.; Stein, J.M. Definition, etiology, prevention and treatment of peri-implantitis—A review. Head Face Med. 2014, 10, 34. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Berglundh, T.; Persson, L.; Klinge, B. A systematic review of the incidence of biological and technical complications in implant dentistry reported in prospective longitudinal studies of at least 5 years. J. Clin. Periodontol. 2002, 29 (Suppl. 3), 197–212; [Google Scholar] [CrossRef]
- Schwarz, F.; Derks, J.; Monje, A.; Wang, H.L. Peri-implantitis. J. Periodontol. 2018, 89 (Suppl. 1), S267–S290. [Google Scholar] [CrossRef]
- Berglundh, T.; Armitage, G.; Araujo, M.G.; Avila-Ortiz, G.; Blanco, J.; Camargo, P.M.; Chen, S.; Cochran, D.; Derks, J.; Figuero, E.; et al. Peri-implant diseases and conditions: Consensus report of workgroup 4 of the 2017 World Workshop on the Classification of Periodontal and Peri-Implant Diseases and Conditions. J. Clin. Periodontol. 2018, 45 (Suppl. 20), S286–S291. [Google Scholar] [CrossRef] [Green Version]
- Heitz-Mayfield, L.J.; Lang, N.P. Comparative biology of chronic and aggressive periodontitis vs. peri-implantitis. Periodontol. 2000 2010, 53, 167–181. [Google Scholar] [CrossRef]
- Heitz-Mayfield, L.J.; Mombelli, A. The therapy of peri-implantitis: A systematic review. Int. J. Oral Maxillofac. Implant. 2014, 29, 325–345. [Google Scholar] [CrossRef] [Green Version]
- Teughels, W.; van Assche, N.; Sliepen, I.; Quirynen, M. Effect of material characteristics and/or surface topography on biofilm development. Clin. Oral Implant. Res. 2006, 17 (Suppl. 2), 68–81. [Google Scholar] [CrossRef] [PubMed]
- Heitz-Mayfield, L.J. Peri-implant diseases: Diagnosis and risk indicators. J. Clin. Periodontol. 2008, 35, 292–304. [Google Scholar] [CrossRef] [PubMed]
- Sahrmann, P.; Gilli, F.; Wiedemeier, D.B.; Attin, T.; Schmidlin, P.R.; Karygianni, L. The Microbiome of Peri-Implantitis: A Systematic Review and Meta-Analysis. Microorganisms 2020, 8, 661. [Google Scholar] [CrossRef]
- Hultin, M.; Gustafsson, A.; Hallstrom, H.; Johansson, L.A.; Ekfeldt, A.; Klinge, B. Microbiological findings and host response in patients with peri-implantitis. Clin. Oral Implant. Res. 2002, 13, 349–358. [Google Scholar] [CrossRef]
- Renvert, S.; Polyzois, I. Treatment of pathologic peri-implant pockets. Periodontol. 2000 2018, 76, 180–190. [Google Scholar] [CrossRef] [PubMed]
- Hajishengallis, G. Immunomicrobial pathogenesis of periodontitis: Keystones, pathobionts, and host response. Trends Immunol. 2014, 35, 3–11. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Valderrama, P.; Blansett, J.A.; Gonzalez, M.G.; Cantu, M.G.; Wilson, T.G. Detoxification of Implant Surfaces Affected by Peri-Implant Disease: An Overview of Non-surgical Methods. Open Dent. J. 2014, 8, 77–84. [Google Scholar] [CrossRef] [PubMed]
- Casado, P.L.; Otazu, I.B.; Balduino, A.; de Mello, W.; Barboza, E.P.; Duarte, M.E. Identification of periodontal pathogens in healthy periimplant sites. Implant. Dent. 2011, 20, 226–235. [Google Scholar] [CrossRef] [PubMed]
- Ebadian, A.R.; Kadkhodazadeh, M.; Zarnegarnia, P.; Dahlen, G. Bacterial analysis of peri-implantitis and chronic periodontitis in Iranian subjects. Acta Med. Iran. 2012, 50, 486–492. [Google Scholar]
- Lang, N.P.; Mombelli, A.; Tonetti, M.S.; Bragger, U.; Hammerle, C.H. Clinical trials on therapies for peri-implant infections. Ann. Periodontol. 1997, 2, 343–356. [Google Scholar] [CrossRef]
- Lang, N.P.; Berglundh, T.; Heitz-Mayfield, L.J.; Pjetursson, B.E.; Salvi, G.E.; Sanz, M. Consensus statements and recommended clinical procedures regarding implant survival and complications. Int. J. Oral Maxillofac. Implant. 2004, 19, 150–154. [Google Scholar]
- Zhao, Y.; Pu, R.; Qian, Y.; Shi, J.; Si, M. Antimicrobial photodynamic therapy versus antibiotics as an adjunct in the treatment of periodontitis and peri-implantitis: A systematic review and meta-analysis. Photodiagn. Photodyn. Ther. 2021, 34, 102231. [Google Scholar] [CrossRef]
- Natto, Z.S.; Aladmawy, M.; Levi, P.A., Jr.; Wang, H.L. Comparison of the efficacy of different types of lasers for the treatment of peri-implantitis: A systematic review. Int. J. Oral Maxillofac. Implant. 2015, 30, 338–345. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Filoche, S.; Wong, L.; Sissons, C.H. Oral biofilms: Emerging concepts in microbial ecology. J. Dent. Res. 2010, 89, 8–18. [Google Scholar] [CrossRef] [PubMed]
- Lan, S.F.; Kehinde, T.; Zhang, X.; Khajotia, S.; Schmidtke, D.W.; Starly, B. Controlled release of metronidazole from composite poly-epsilon-caprolactone/alginate (PCL/alginate) rings for dental implants. Dent. Mater. 2013, 29, 656–665. [Google Scholar] [CrossRef]
- Kotsovilis, S.; Karoussis, I.K.; Trianti, M.; Fourmousis, I. Therapy of peri-implantitis: A systematic review. J. Clin. Periodontol. 2008, 35, 621–629. [Google Scholar] [CrossRef] [PubMed]
- Garrett, S.; Adams, D.F.; Bogle, G.; Donly, K.; Drisko, C.H.; Hallmon, W.W.; Hancock, E.B.; Hanes, P.; Hawley, C.E.; Johnson, L.; et al. The effect of locally delivered controlled-release doxycycline or scaling and root planing on periodontal maintenance patients over 9 months. J. Periodontol. 2000, 71, 22–30. [Google Scholar] [CrossRef] [Green Version]
- Schwarz, F.; Schmucker, A.; Becker, J. Efficacy of alternative or adjunctive measures to conventional treatment of peri-implant mucositis and peri-implantitis: A systematic review and meta-analysis. Int. J. Implant. Dent. 2015, 1, 22. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Killoy, W.J. Chemical treatment of periodontitis: Local delivery of antimicrobials. Int. Dent. J. 1998, 48, 305–315. [Google Scholar] [CrossRef]
- Renvert, S.; Lessem, J.; Dahlen, G.; Renvert, H.; Lindahl, C. Mechanical and repeated antimicrobial therapy using a local drug delivery system in the treatment of peri-implantitis: A randomized clinical trial. J. Periodontol. 2008, 79, 836–844. [Google Scholar] [CrossRef]
- Da Rocha, H.A.; Silva, C.F.; Santiago, F.L.; Martins, L.G.; Dias, P.C.; de Magalhães, D. Local Drug Delivery Systems in the Treatment of Periodontitis: A Literature Review. J. Int. Acad. Periodontol. 2015, 17, 82–90. [Google Scholar]
- Mombelli, A.; Feloutzis, A.; Bragger, U.; Lang, N.P. Treatment of peri-implantitis by local delivery of tetracycline. Clinical, microbiological and radiological results. Clin. Oral Implant. Res. 2001, 12, 287–294. [Google Scholar] [CrossRef]
- Sinha, S.; Kumar, S.; Dagli, N.; Dagli, R.J. Effect of tetracycline HCl in the treatment of chronic periodontitis—A clinical study. J. Int. Soc. Prev. Community Dent. 2014, 4, 149–153. [Google Scholar] [CrossRef] [Green Version]
- Boyeena, L.; Koduganti, R.R.; Panthula, V.R.; Jammula, S.P. Comparison of efficacy of probiotics versus tetracycline fibers as adjuvants to scaling and root planing. J. Indian Soc. Periodontol. 2019, 23, 539–544. [Google Scholar] [CrossRef]
- Dang, A.B.; Chaubey, K.K.; Thakur, R.K.; Mohan, R.; Chowdhary, Z.; Tripathi, R. Comparative evaluation of efficacy of three treatment modalities—Tetracycline fibers, scaling and root planing, and combination therapy: A clinical study. J. Indian Soc. Periodontol. 2016, 20, 608–613. [Google Scholar] [CrossRef] [PubMed]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. BMJ 2009, 339, b2535. [Google Scholar] [CrossRef] [Green Version]
- Higgins, J.P.; Altman, D.G.; Gotzsche, P.C.; Juni, P.; Moher, D.; Oxman, A.D.; Savovic, J.; Schulz, K.F.; Weeks, L.; Sterne, J.A.; et al. The Cochrane Collaboration’s tool for assessing risk of bias in randomised trials. BMJ 2011, 343, d5928. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Renvert, S.; Lessem, J.; Dahlen, G.; Lindahl, C.; Svensson, M. Topical minocycline microspheres versus topical chlorhexidine gel as an adjunct to mechanical debridement of incipient peri-implant infections: A randomized clinical trial. J. Clin. Periodontol. 2006, 33, 362–369. [Google Scholar] [CrossRef] [PubMed]
- Park, S.H.; Song, Y.W.; Cha, J.K.; Lee, J.S.; Kim, Y.T.; Shin, H.S.; Lee, D.W.; Lee, J.H.; Kim, C.S. Adjunctive use of metronidazole-minocycline ointment in the nonsurgical treatment of peri-implantitis: A multicenter randomized controlled trial. Clin. Implant. Dent. Relat. Res. 2021, 23, 543–554. [Google Scholar] [CrossRef]
- Cha, J.K.; Lee, J.S.; Kim, C.S. Surgical Therapy of Peri-Implantitis with Local Minocycline: A 6-Month Randomized Controlled Clinical Trial. J. Dent. Res. 2019, 98, 288–295. [Google Scholar] [CrossRef] [PubMed]
- Buchter, A.; Meyer, U.; Kruse-Losler, B.; Joos, U.; Kleinheinz, J. Sustained release of doxycycline for the treatment of peri-implantitis: Randomised controlled trial. Br. J. Oral Maxillofac. Surg. 2004, 42, 439–444. [Google Scholar] [CrossRef] [PubMed]
- Figuero, E.; Graziani, F.; Sanz, I.; Herrera, D.; Sanz, M. Management of peri-implant mucositis and peri-implantitis. Periodontol. 2000 2014, 66, 255–273. [Google Scholar] [CrossRef]
- Heitz-Mayfield, L.J.A.; Salvi, G.E.; Mombelli, A.; Loup, P.J.; Heitz, F.; Kruger, E.; Lang, N.P. Supportive peri-implant therapy following anti-infective surgical peri-implantitis treatment: 5-year survival and success. Clin. Oral Implant. Res. 2018, 29, 1–6. [Google Scholar] [CrossRef]
- Jepsen, K.; Jepsen, S.; Laine, M.L.; Anssari Moin, D.; Pilloni, A.; Zeza, B.; Sanz, M.; Ortiz-Vigon, A.; Roos-Jansaker, A.M.; Renvert, S. Reconstruction of Peri-implant Osseous Defects: A Multicenter Randomized Trial. J. Dent. Res. 2016, 95, 58–66. [Google Scholar] [CrossRef] [PubMed]
- Strooker, H.; Rohn, S.; van Winkelhoff, A.J. Clinical and microbiologic effects of chemical versus mechanical cleansing in professional supportive implant therapy. Int. J. Oral Maxillofac. Implant. 1998, 13, 845–850. [Google Scholar]
- Paquette, D.W.; Ryan, M.E.; Wilder, R.S. Locally delivered antimicrobials: Clinical evidence and relevance. J. Dent. Hyg. 2008, 82 (Suppl. 3), 10–15. [Google Scholar]
- Bassetti, M.; Schar, D.; Wicki, B.; Eick, S.; Ramseier, C.A.; Arweiler, N.B.; Sculean, A.; Salvi, G.E. Anti-infective therapy of peri-implantitis with adjunctive local drug delivery or photodynamic therapy: 12-month outcomes of a randomized controlled clinical trial. Clin. Oral Implant. Res. 2014, 25, 279–287. [Google Scholar] [CrossRef]
- Tan, O.L.; Safii, S.H.; Razali, M. Commercial Local Pharmacotherapeutics and Adjunctive Agents for Nonsurgical Treatment of Periodontitis: A Contemporary Review of Clinical Efficacies and Challenges. Antibiotics 2019, 9, 11. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nadig, P.S.; Shah, M.A. Tetracycline as local drug delivery in treatment of chronic periodontitis: A systematic review and meta-analysis. J. Indian Soc. Periodontol. 2016, 20, 576–583. [Google Scholar] [CrossRef]
- Xu, L.; Wang, Y.; Nguyen, V.T.; Chen, J. Effects of Topical Antibiotic Prophylaxis on Wound Healing After Flapless Implant Surgery: A Pilot Study. J. Periodontol. 2016, 87, 275–280. [Google Scholar] [CrossRef] [PubMed]
- Herrera, D.; Matesanz, P.; Martin, C.; Oud, V.; Feres, M.; Teughels, W. Adjunctive effect of locally delivered antimicrobials in periodontitis therapy: A systematic review and meta-analysis. J. Clin. Periodontol. 2020, 47 (Suppl. 22), 239–256. [Google Scholar] [CrossRef] [PubMed]
- Nastri, L.; de Rosa, A.; de Gregorio, V.; Grassia, V.; Donnarumma, G. A New Controlled-Release Material Containing Metronidazole and Doxycycline for the Treatment of Periodontal and Peri-Implant Diseases: Formulation and In Vitro Testing. Int. J. Dent. 2019, 2019, 9374607. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Madi, M.; Pavlic, V.; Samy, W.; Alagl, A. The anti-inflammatory effect of locally delivered nano-doxycycline gel in therapy of chronic periodontitis. Acta Odontol. Scand. 2018, 76, 71–76. [Google Scholar] [CrossRef] [PubMed]
- Schenk, G.; Flemmig, T.F.; Betz, T.; Reuther, J.; Klaiber, B. Controlled local delivery of tetracycline HCl in the treatment of periimplant mucosal hyperplasia and mucositis. A controlled case series. Clin. Oral Implant. Res. 1997, 8, 427–433. [Google Scholar] [CrossRef] [PubMed]
- Hallstrom, H.; Persson, G.R.; Lindgren, S.; Olofsson, M.; Renvert, S. Systemic antibiotics and debridement of peri-implant mucositis. A randomized clinical trial. J. Clin. Periodontol. 2012, 39, 574–581. [Google Scholar] [CrossRef]
- Heo, S.; Kim, H.J.; Joo, J.Y.; Lee, J.; Kim, S.J.; Choi, J. Simplified nonsurgical treatment of peri-implantitis using chlorhexidine and minocycline hydrochloride. J. Periodontal Implant Sci. 2018, 48, 326–333. [Google Scholar] [CrossRef] [PubMed]
- Heitz-Mayfield, L.J.; Lang, N.P. Antimicrobial treatment of peri-implant diseases. Int. J. Oral Maxillofac. Implant. 2004, 19, 128–139. [Google Scholar]
- Mensi, M.; Scotti, E.; Calza, S.; Pilloni, A.; Grusovin, M.G.; Mongardini, C. A new multiple anti-infective non-surgical therapy in the treatment of peri-implantitis: A case series. Minerva Stomatol. 2017, 66, 255–266. [Google Scholar] [CrossRef]
- Moura, L.A.; Oliveira Giorgetti Bossolan, A.P.; de Rezende Duek, E.A.; Sallum, E.A.; Nociti, F.H., Jr.; Casati, M.Z.; Sallum, A.W. Treatment of peri-implantitis using nonsurgical debridement with bioresorbable nanospheres for controlled release of doxycycline: Case report. Compend. Contin. Educ. Dent. 2012, 33, E145–E149. [Google Scholar]
- Diachkova, E.; Corbella, S.; Taschieri, S.; Tarasenko, S. Nonsurgical Treatment of Peri-Implantitis: Case Series. Dent. J. 2020, 8, 78. [Google Scholar] [CrossRef]
- Thone-Muhling, M.; Swierkot, K.; Nonnenmacher, C.; Mutters, R.; Flores-de-Jacoby, L.; Mengel, R. Comparison of two full-mouth approaches in the treatment of peri-implant mucositis: A pilot study. Clin. Oral Implant. Res. 2010, 21, 504–512. [Google Scholar] [CrossRef]
- Porras, R.; Anderson, G.B.; Caffesse, R.; Narendran, S.; Trejo, P.M. Clinical response to 2 different therapeutic regimens to treat peri-implant mucositis. J. Periodontol. 2002, 73, 1118–1125. [Google Scholar] [CrossRef]
- Schar, D.; Ramseier, C.A.; Eick, S.; Arweiler, N.B.; Sculean, A.; Salvi, G.E. Anti-infective therapy of peri-implantitis with adjunctive local drug delivery or photodynamic therapy: Six-month outcomes of a prospective randomized clinical trial. Clin. Oral Implant. Res. 2013, 24, 104–110. [Google Scholar] [CrossRef]
- Salvi, G.E.; Persson, G.R.; Heitz-Mayfield, L.J.; Frei, M.; Lang, N.P. Adjunctive local antibiotic therapy in the treatment of peri-implantitis II: Clinical and radiographic outcomes. Clin. Oral Implant. Res. 2007, 18, 281–285. [Google Scholar] [CrossRef] [PubMed]
- Tang, Z.; Cao, C.; Sha, Y.; Lin, Y.; Wang, X. Effects of non-surgical treatment modalities on peri-implantitis. Zhonghua Kou Qiang Yi Xue Za Zhi 2002, 37, 173–175. [Google Scholar]
- Paul, T.P.; Emmatty, R.; Pulikkottil, J.J.; Rahman, A.A.; Kumar, S.A.; George, N. Comparative Evaluation of Sustained Release Collagen Device Containing 5% Metronidazole (Metrogene) along With and Without Scaling and Root Planing at Regular Intervals with Treatment of Chronic Periodontitis: A Case Control Study. J. Int. Oral Health 2015, 7, 18–22. [Google Scholar]
- Canullo, L.; Penarrocha-Oltra, D.; Soldini, C.; Mazzocco, F.; Penarrocha, M.; Covani, U. Microbiological assessment of the implant-abutment interface in different connections: Cross-sectional study after 5 years of functional loading. Clin. Oral Implant. Res. 2015, 26, 426–434. [Google Scholar] [CrossRef]
- Canullo, L.; Penarrocha-Oltra, D.; Covani, U.; Rossetti, P.H. Microbiologic and Clinical Findings of Implants in Healthy Condition and with Peri-Implantitis. Int. J. Oral Maxillofac. Implant. 2015, 30, 834–842. [Google Scholar] [CrossRef] [PubMed]
- Toledano, M.; Osorio, M.T.; Vallecillo-Rivas, M.; Toledano-Osorio, M.; Rodriguez-Archilla, A.; Toledano, R.; Osorio, R. Efficacy of local antibiotic therapy in the treatment of peri-implantitis: A systematic review and meta-analysis. J. Dent. 2021, 113, 103790. [Google Scholar] [CrossRef]
- Smiley, C.J.; Tracy, S.L.; Abt, E.; Michalowicz, B.S.; John, M.T.; Gunsolley, J.; Cobb, C.M.; Rossmann, J.; Harrel, S.K.; Forrest, J.L.; et al. Systematic review and meta-analysis on the nonsurgical treatment of chronic periodontitis by means of scaling and root planing with or without adjuncts. J. Am. Dent. Assoc. 2015, 146, 508–524. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Author | Country | Number Pz and Imp | Setting | Clinical Characteristics | Surgical/Non-Surgical | Treatment | TG | CG | FU (Months) | Main Findings |
|---|---|---|---|---|---|---|---|---|---|---|
| Buchter et al. (2004) [39] | Germany | 28 pz 48 imp TG: 14 pz CG: 14 pz | NR | Chronic peri-implantitis PD > 5 mm; bone defects exceeding 50% of the length of the implant on radiographs | Non-surgical | Removal prosthetic restoration + abutment sterilised + 0.2% CHX irrigation + implant scaling | 8.5% DOX | No additional treatment | 4 | TG: CAL: 5.32 ± 0.33, 4.17 ± 0.30 (p < 0.001); PD: 5.64 ± 0.32, 4.49 ± 0.29 (p < 0.001); BOP: 0.54 ± 0.07, 0.27 ± 0.06 (p = 0.001) CG: CAL: 5.51 ± 0.27, 5.18 ± 0.33 (p < 0.001); PD: 5.68 ± 0.28, 5.4 ± 0.34 (p < 0.001); BOP: 0.63 ± 0.06, 0.50 ± 0.07 (p = 0.001) Difference between groups: CAL: p = 0.024, PD: p = 0.046, BOP: p = 0.01 |
| Renvert et al. (2006) [36] | Sweden | 30 pz 30 imp TG: 16 pz CG: 14 pz | Kristianstad University | BOP or pus + PD ≥ 4 mm + presence of putative pathogenic bacteria + loss of bone ≤ 3 threads on radiographs | Non-surgical | OHI + supra and sub mucosa scaling + rubber cup polish | Submucosal administration of MIN microspheres | Submucosal administration of 0.1 mL CHX gel 1% | 12 | TG: PI (%): 50 ± 25, 27 ± 24; BOP/BOS (%): 88 ± 12, 71 ± 22 PD (mm) 3.9 ± 0.7, 3.6 ± 0.6 CG: PI (%): 60 ± 49, 27 ± 45; BOP/BOS (%): 89.2 ± 17.2, 63.5 ± 19.1; PD (mm) 3.87 ± 1.16, 3.72 ± 1.02. Comparison between groups at six months: PI (p > 0.05), BOP/SOP (p ≤ 0.01 all four sites/implants, p > 0.05 deepest site/implant), PD (p ≤ 0.001). Comparisons between groups at 12 months: PI (p > 0.05), BOP/SOP (p > 0.05 all four sites/implants, p ≤ 0.05 deepest site/implant), PD (p ≤ 0.001 all four site/implants, p ≤ 0.01 deepest site/implant). No statistical significance emerged between the two antimicrobials for any bacteria at any time point. |
| Renvert et al. (2008) [28] | Sweden | 32 pz 95 imp TG: 17 pz/57 imp CG: 15 pz/38 imp | Kristianstad University | PD ≥ 4 mm + BOP and/pr pus + radiographic bone loss ≤ 3 threads + occurrence of anaerobic bacteria + presence of one or more bacteria | Non-surgical | NR | MIN microspheres | 0.1 mL 1% CHX gel | 12 | Treatment group: LPS (%): 50 ± 50, 22 ± 42; BOP/BOS (%): 86.5 ± 20.1, 48.1 ± 20.7; PD (mm) 3.85 ± 1.04, 3.55 ± 0.98; Control group: LPS (%): 60 ± 49, 27 ± 45; BOP/BOS (%): 89.2 ± 17.2, 63.5 ± 19.1; PD (mm) 3.87 ± 1.16, 3.72 ± 1.02. Comparison between groups at six months: LPS (p = 0.003); PD (p > 0.05), BOP/SOP (p < 0.001). Comparisons between groups at 12 months: LPS (p > 0.05); PD (p > 0.05), BOP/SOP (p < 0.001). No statistically significant differences in the mean total numbers of bacteria between and within groups after 12 months. |
| Cha et al. (2019) [38] | South Korea | 46 pz 46 imp TG: 24 pz CG: 22 pz | Department of Periodontology | Peri-implant bone loss > 2 mm; PPD > 5 mm; concomitant BOP | Surgical treatment | Surgical treatment | Local MIN (10 mg of minocycline in 0.5 g of OIN) | PBO OIN | 6 | PPD: TG: 3.58 ± 2.32; CG: 2.45 ± 2.13; p = 0.094. BOP: TG: 0.58 ± 0.50; CG: 0.32 ± 0.57; p = 0.102. PI: TG: 0.12 ± 0.90; CG: 0.23 ± 1.07; p = 0.728. GI: TG: 0.96 ± 0.86; CG: 0.41 ± 0.85; p = 0.035. Number of red-complex bacteria decreased in both groups, without statistically significant differences between groups. |
| Park et al. (2021) [37] | Korea | 114 pz 114 imp MM: 38 pz MC: 39 pz NST: 37 pz | Department of Periodontology | Implant inserted at least 1 year previously; PPD ≥ 5 mm; presence of BOP, SoP, and peri-implant bone loss in a periapical radiograph | Non-surgical | OH + non-surgical debridement | MD + MTZ-MIN OIN (MM); MD + MIN OIN (MC) | MD | 4 | MM: PPD −2.71 ± 1.90; BOP: −0.66 ± 0.53; Pus Suppuration: −0.18 ± 0.39; PI: −0.71 ± 0.80. MC: PPD −2.51 ± 1.82; BOP: −0.59 ± 0.50; Pus Suppuration: −0.31 ± 0.46; PI: −0.54 ± 0.76. NTS: PPD −2.03 ± 1.38; BOP: −0.38 ± 0.49; Pus Suppuration: −0.32 ± 0.53; PI: −0.35 ± 0.89. Statistically significant differences were found for PPD and BOP between MM and NTS (p = 0.0023, p = 0.0381). After 12 weeks, significant decreases in the counts of P. gingivalis, T. forsythia, T. denticola, P. intermedia, C. rectus, and F. nucleatum in MM and MC group. In the NST group, decrease only for P. gingivalis |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Passarelli, P.C.; Netti, A.; Lopez, M.A.; Giaquinto, E.F.; De Rosa, G.; Aureli, G.; Bodnarenko, A.; Papi, P.; Starzyńska, A.; Pompa, G.; et al. Local/Topical Antibiotics for Peri-Implantitis Treatment: A Systematic Review. Antibiotics 2021, 10, 1298. https://doi.org/10.3390/antibiotics10111298
Passarelli PC, Netti A, Lopez MA, Giaquinto EF, De Rosa G, Aureli G, Bodnarenko A, Papi P, Starzyńska A, Pompa G, et al. Local/Topical Antibiotics for Peri-Implantitis Treatment: A Systematic Review. Antibiotics. 2021; 10(11):1298. https://doi.org/10.3390/antibiotics10111298
Chicago/Turabian StylePassarelli, Pier Carmine, Andrea Netti, Michele Antonio Lopez, Eleonora Favetti Giaquinto, Giuseppe De Rosa, Gianmarco Aureli, Alina Bodnarenko, Piero Papi, Anna Starzyńska, Giorgio Pompa, and et al. 2021. "Local/Topical Antibiotics for Peri-Implantitis Treatment: A Systematic Review" Antibiotics 10, no. 11: 1298. https://doi.org/10.3390/antibiotics10111298
APA StylePassarelli, P. C., Netti, A., Lopez, M. A., Giaquinto, E. F., De Rosa, G., Aureli, G., Bodnarenko, A., Papi, P., Starzyńska, A., Pompa, G., & D’Addona, A. (2021). Local/Topical Antibiotics for Peri-Implantitis Treatment: A Systematic Review. Antibiotics, 10(11), 1298. https://doi.org/10.3390/antibiotics10111298