Abstract
Acute otitis media (AOM) in children represents a public health concern, being one of the leading causes of health care visits and antibiotic prescriptions worldwide. The overall aim of this paper is to unravel the major current insights into the antibiotic treatment of AOM in children. Our approach is three-fold: 1. a preclinical evaluation of antibiotics in animal models of AOM stressing on the advantages of different species when testing for different schemes of antibiotics; 2. an overview on the new antimicrobial agents whose efficacy has been demonstrated in refractory cases of AOM in children; and 3. an analysis of the different guidelines stressing on the differences and similarities between the various schemes of antibiotic treatment. The preferred therapeutic agents remain amoxicillin and the amoxicillin-clavulanate combination for AOM caused by Streptococcus pneumoniae, whereas oral cephalosporin is preferred in AOM due to Moraxella catarrhalis and Haemophilus influenzae. As for the second and third line antimicrobial treatments, there is a wide variety of suggested antibiotic classes with variations in duration and posology. The decision to prescribe antimicrobial treatment as a first-line choice is based on the severity of the symptoms in 16 of the guidelines included in this review.
1. Background
Acute otitis media (AOM) is a multifactorial disease representing the second most common cause of family physician visits in the pediatric population, following upper respiratory infections [1,2], with a negative economic impact [3]. Although we face nowadays a decrease in the number of otitis cases due to pneumococcal vaccination in infants [4], by 1 year of age about 23% of the children experience ≥1 episode of otitis media (OM), and by 3 years of age 60% experience ≥1 episode of OM and 24% ≥3 episodes [5]. Although the susceptibility to antibiotics among bacteria commonly causing AOM has decreased, the importance of antibiotic therapy cannot be denied [6,7]. In the pre-antibiotic era, 6% of the patients with AOM developed infectious complications [8], although the incidence of suppurated complications has declined to less than 1% after the introduction of antibiotics [9].
Our aim is to unravel the major insights into the antibiotic treatment of AOM in children. We will start by presenting a preclinical evaluation of antibiotics in animal models of AOM stressing on the advantages (characteristics) of different species when testing for different schemes of antibiotics. In the second part of our paper, we will provide an overview on the new antimicrobial agents whose efficacy has been demonstrated in refractory cases of AOM in children. Therapeutic failures in AOM in children are usually due to inadequate antimicrobial treatment, non-identification of the pathogen, or antimicrobial resistance [10,11,12]. To discuss each of these issues is beyond the purpose of our paper. We will refer only to antibiotic resistance because this is nowadays a frequent phenomenon. In the last part of the paper, we will analyze the different guidelines for the treatment of AOM in children, stressing on the differences and similarities between the various schemes of antibiotic treatment.
2. Preclinical Evaluation of Antibiotics in Animal Models of Acute Otitis Media
Animal models have been and will continue to be a powerful way to explore the mechanisms of diseases, with a significant impact on the development of new compounds and optimal therapeutic regimens [13]. Preclinical models of AOM in rodents allow the study of histopathological alterations during inflammation of the middle ear [14,15,16]; potential new therapies, including antibiotics or vaccines and the biocompatibility of implanted biomaterials [17,18]. Each AOM animal model (mice, rats, gerbils, chinchillas, or guinea pigs) studied over time has highlighted a series of drawbacks, but if the proposed limitations or questions are those to which the model can answer, the data acquired could be consistently interpreted [19]. Animal models of AOM revealed several histological and pathological similarities with the human disease, leading to the possibility of extrapolating the findings to new genetic or transgenic models. Moreover, the small size of most of these species facilitates low husbandry costs and easy handling (Table 1). Additionally, in vivo preclinical models utilized in laboratory settings frequently possess predictable pharmacokinetics, pharmacodynamics, and physiology, which have been already well explored [13,15,20,21]. The common disadvantages of using rodent AOM models comprise difficulties in small size tissue manipulation, in generating a multifactorial background of pathogenesis, and in some cases the development of sepsis (Table 1) [13,15,17,19,22,23,24,25].

Table 1.
The most common advantages and disadvantages of rodent species used in acute otitis media models.
AOM represents one of the most often cited reasons for the antibiotic prescription in children under 3 years of age [33]. This condition can be caused by both bacterial (Moraxella catarrhalis, Staphylococcus aureus, Streptococcus pneumoniae and Haemophilus influenzae) and viral pathogens (such as rhinovirus, respiratory syncytial virus, adenovirus, and influenza virus) [33,34,35]. A rigorous evaluation of the studies to verify whether antibiotic treatment impacts AOM outcomes is difficult to interpret, given the great rate of spontaneous recovery in children with this condition [36]. Thus, appropriate animal models that mimic the human infection have been designed to study this disease and to explore the efficacy of some antibiotic agents (Table 2).
Table 2.
Preclinical assessment of antibiotics in animal models of acute otitis media.
A careful assessment of these studies in which these drugs were evaluated together with detailed analysis of pharmacodynamics and pharmacokinetic aspects of each of them could differentiate the various compounds and recognize those with best tolerability, cost/efficacy ratio, and safety.
3. Treatment Options, Antibiotic Resistance, and New Antibiotics/Antibiotics’ Schemes in AOM in Children
3.1. Classic Therapeutic Options in AOM in Children
The preferred therapeutic agents remain amoxicillin and the amoxicillin-clavulanate combination for AOM caused by S. pneumoniae, whereas oral cephalosporin’s (cefixime) is preferred in AOM due to M. catarrhalis, and H. influenzae [11]. The efficacy of amoxicillin-clavulanate versus azithromycin in 180 children with OMA aged 6 months to 12 years has been prospectively studied by Guven et al. [11]. The 10-day amoxicillin-clavulanate therapy (45 mg amoxicillin/kg) regimen was as effective as the azithromycin 3-day therapy (10 mk/kg/day, once). Both were well tolerated and had an equal incidence of side effects [11]. Kono et al. [12] have compared two “classic” antibiotic schemes in a sample of 146 pediatric patients with AOM (age 1 month to 5 years old) from eight private Japanese clinics: amoxicillin (70 mg/kg) for five days and amoxicillin in the same dose + clarithromycin (15 mg/kg) only for the first 3 days. M. catarrhalis, S. pneumoniae and H. influenzae were identified in the secretions from the middle ear. The curing of AOM was confirmed 14 days after the start of treatment for both groups. Therapeutic failure was recorded in 25 children, 16 of 58 being under 2 years of age. In the group treated with amoxicillin + clarithromycin, a smaller number of therapeutic failures were registered. Despite the proven efficacy of the conventional treatment, antibiotic resistance is an increasing phenomenon nowadays. A meta-analysis of the studies on the antimicrobial resistance in AOM in children performed during 1980–2017 [39], detected resistance of Gram-positive bacteria (S. pneumoniae) to penicillin but not to amoxicillin, the recommendation being to continue using this antibiotic as a first choice in treating children with otitis media [39,40]. The bacteriology of AOM was dominated by S. pneumoniae and H. influenzae, both of which were insensitive to first-line therapy. M. catarrhalis has demonstrated beta-lactamase production and amoxicillin resistance. In cases of penicillin allergy, erythromycin was used, for which S. pneumoniae showed high resistance. However, all three pathogens were susceptible to the amoxicillin-clavulanate combination, a combination that is normally recommended as second-line therapy [39]. Brook et al. [41] have reported beta-lactamase activity in 79% of the ear samples from children with otitis media. This might be explained by the fact that 70% of the patients had been treated with beta-lactam antibiotics [42].
3.2. Antibiotic Resistance
A ten-year retrospective analysis revealed that the rate of antibiotic-resistant ear infections has doubled over the last decade. Ampicillin had the highest overall resistance rate (88.5%), followed by ceftriaxone (84.5%), amoxicillin (81.9%), and tetracycline (74.5%) [43]. Although important advances have been made in the development of pneumococcal conjugate vaccines, multidrug resistance was found in 84% of the S. pneumoniae strains isolated in 62 children, aged between 1 and 16 years, during the episodes of AOM (including recurrent/treatment failure AOM and post-treatment visits) [44]. Bacterial resistance to antibiotics occurs frequently and is the ability of pathogens (bacteria, parasites, viruses, etc.) to develop in the presence of active substances that would normally destroy or inactivate them. Antibiotics identify bacteria and then exert their bactericidal or bacteriostatic effect [4,10]. The phenomenon of bacterial resistance occurs most often in the case of long-term, repetitive therapies, otitis media being the condition that often requires such therapy. Beta-lactamases are enzymes produced by many bacteria resistant to beta-lactam antibiotics (penicillins, cephalosporins, cefamycins, and carbapenems), when these antibiotics are present in the environment. Penicillinase is a specific type of beta-lactamase [10] released by Gram-negative anaerobic bacteria in the infected area.
In order to understand the mechanism of bacterial resistance to beta-lactam antibiotics, we will shortly discuss the main mechanisms of action of penicillin-type antibiotics. These are antibiotics with a beta-lactam structure that selectively interfere with the synthesis of the bacterial cell wall, a wall made of a polymer called peptidoglycan. More specifically, it acts in the last stage of the synthesis of the bacterial cell wall, as it is a bactericidal process and consists in the irreversible binding of the beta-lactam ring in the antibiotic structure to the penicillin binding proteins (PBPs) located in the membrane, which serve as specific receptors for beta-lactams. All beta-lactam antibiotics, which inhibit glutamine synthetase, bind to PBPs and have been shown to catalyze a number of reactions involved in the process of synthesizing cross-linked peptidoglycan necessary to maintain the integrity of the bacterial cell. This is an irreversible reaction and inactivates the enzyme. These proteins (transpeptidases) are bacterial enzymes that bind penicillin, and their exposure to antibiotics prevents the synthesis of the cell wall and causes structural changes or even cell lysis. Penicillins inhibit this transpeptidase-catalyzed reaction, thus blocking cell wall synthesis and the accumulation of “Park nucleotide” or uridine diphosphate (UDP) -acetylmuramyl-pentapeptide. Transpeptidases or penicillin-binding proteins, in its presence, form the penicilloyl-enzyme complex with impaired deacetylation reaction catalyzed by transpeptidase with lysis and cell death, hence the quality of bactericidal agents [45]. Another mechanism for the establishment of antimicrobial resistance consists in the alteration of membrane receptors by the modification of the affinity of the receptor for bacteria, amplifying bacterial activity and canceling the activity of the drug [46,47]. Presented in Figure 1 is a schematic representation of the passage of antibiotic molecules in a Gram-negative bacterium.
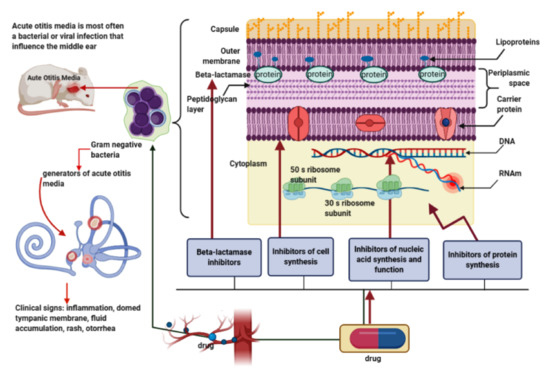
Figure 1.
In the determination of otitis media, pathogens such as Gram-positive and -negative bacteria are causative agents of the acute form; the Gram-negative bacterium is represented in the image because, from a structural and chemical point of view, it is more complex compared with the Gram-positive one. The cell wall contains two outer layers of the cytoplasmic membrane and above the peptidoglycan layer is an outer membrane present only in Gram-negative bacteria. Specific for these bacteria are the “porins” (transmembrane proteins) that allow the passage of antibiotic molecules. Clinically, acute otitis media (AOM) is characterized by inflammation, bulging of the tympanic membrane, accumulation of purulent secretion, otorrhea, and discomfort. The effectiveness of antibiotics in this condition has been proven in both preclinical and clinical studies through various mechanisms of action that affect the middle ear, such as inhibition of cell synthesis, nucleic acids and disruption of their function, inhibition of protein synthesis, and enzymes such as beta-lactamases.
3.3. New Antibiotics/Antibiotic Schemes in the Treatment of AOM in Children
The most effective therapies for beta-lactamase producing pathogens include clindamycin, chloramphenicol and metronidazole in combination with a macrolide, or the combinations of amoxicillin/clavulanate [41] or piperacillin/tazobactam [47]. Clavulanate is a beta-lactamase inhibitor that competes with the antibiotic to bind to the beta-lactamase, prolonging the life of beta-lactamase sensitive antibiotics that could be inactivated by bacteria if beta-lactamase inhibitors were not associated [42,48]. Carbapenem therapy (meropenem, imipenem) can be effective in both aerobic and anaerobic pathogens [49].
Suzuki et al. [4] evaluated six otorhinolaryngology infectious diseases in both adults and children, including chronic OM and AOM, and the antimicrobial susceptibility patterns of the isolated pathogens in 36 hospitals in Japan. Children under 6 years of age with AOM were subjected to antibiotic susceptibility tests for 40 antimicrobial agents from different classes, such as penicillins, cephemes, carbapenems, macrolides, tetracycline, new quinolones (Tosufloxacin and Levofloxacin), glycopeptides, oxazolidinones, aminoglycosides, lipopeptides, lincomycins, imidazoles, and fosfomycin. Among the 149 cases of recurrent AOM in children, H. influenzae was the most prevalent bacteria, followed by S. pneumoniae and M. catarrhalis. The antimicrobial susceptibility testing for the major bacterial strains revealed bacterial resistance for S. pneumoniae and H. influenzae, especially in patients with AOM, with a frequency that was not influenced by gender, age, geographical area, severity of the disease, hospital institution, and previous medication. The authors do not clearly set up in the end a first-line antimicrobial treatment, but they recommend amoxicillin or amoxicillin-clavulanate (in higher than usual dosage: 60–90 mg/kg of amoxicillin), cefditoren, or cefditoren-pivoxil for moderate cases only. Mild cases should receive only symptomatic treatment.
For resistant S. pneumoniae, new compounds such as Tebipenem pivoxil as the first carbapenem with oral administration available for children could be considered [4,50,51].
The efficacy of tebipenem-pivoxil in AOM in children has been demonstrated by Sugita et al. [52] in a clinical trial evaluating the pharmacokinetic–pharmacodynamic parameters at the site of action: the maximum concentration in the ear effusion exceeded the minimum inhibitory concentration for S. pneumoniae and H. influenzae isolates, thus indicating a favorable transfer of tebipenem to the overflow of the ear. The carbapenem efficiency has been proven and confirmed also by the low incidence of relapses and the high rate of the number of cases cured [52].
The therapy with non-beta-lactam compounds (macrolides and quinolones) has been widely used as an alternative to beta-lactams. The use of new quinolones such as tosufloxacin has increased due to macrolide resistance. Tosufloxacin has been used in children with high antimicrobial activity against H. influenzae. Garenoxacin and Moxifloxacin are recommended only in adults [4]. However, the efficacy of tosufloxacinon isolates taken from pediatric patients is still discussed. In the study of Tanaka et al. [53] H. influenzae isolates have been proved resistant and can only survive at the maximum therapeutic concentration of tosufloxacin [53]. Several studies reported a decreased sensitivity to clarithromycin and revealed numerous quinolone-resistant strains [54,55,56].
Cefditoren pivoxil, a third-generation cephalosporin, is administered as an oral prodrug, absorbed and metabolized by hydrolysis reaction in the active compound cefditoren in the intestine, distributed in the blood until the site of action, and then eliminated by the kidneys [57]. It has a broad spectrum of activity, on Gram-positive and Gram-negative bacteria [58], inhibiting the cell wall synthesis by binding the PBP, followed by loss of cell wall integrity and cell death [57]. The studies on pharmacokinetic modeling and pharmacodynamics profile of cefditoren in the presence of human albumin, serum, plasma, and epithelial lining fluid [59] have demonstrated that the bactericidal activity of this compound could be influenced by the ratio between the total serum concentration of the bound form and the free form [60]. Several studies have shown that cefditoren had a very strong effect against H. influenzae, regardless of β-lactamase production [57,61].
4. Guidelines for Antibiotic Treatment in AOM in Children
In order to reduce the potential complications (e.g., mastoiditis, meningitis, and hearing loss) and the economic burden associated with AOM, various professional guidelines and consensus papers have been created. In the United States of America, Sweden, United Kingdom, France, Spain, and Italy, the introduction of guidelines was associated with a reduction of up to 12% of unnecessary prescriptions and an increase of up to 58% in the accuracy of the type and dosage of the prescribed antibiotic [62]. According to a recent Italian study, the implementation of guidelines in a pediatric emergency department led to a reduction from 53.2% to 32.4% in the use of broad-spectrum antibiotics [63]. We proposed to identify and analyze the available guidelines on AOM to detect common aspects, as well as differences, with a focus on antibiotic prescription, recommendations regarding watchful waiting approach, and follow-up strategies.
A systematic review of the literature for guidelines published between January 1989 (first AOM guideline, Netherlands) and September 2020 was conducted. We performed a systematic search on PubMed and EMBASE databases using keywords: “acute otitis media” AND “children” OR “pediatric” AND (“guideline” OR “consensus”). National or international clinical practice guidelines and guidance documents with recommendations for the management of AOM in children were eligible for inclusion. A total of 263 papers have been initially found. The following items were excluded: withdrawn or superseded guidelines, clinical trials or systematic reviews not part of clinical practice guidelines, and types of publications other than guidelines or consensuses (e.g., case reports or case series). Websites of national pediatric associations and bibliographies of all included guidelines were examined in order to identify further relevant resources.
A total of 20 AOM clinical practice guidelines were included in this review. The following guidelines were analyzed and compared regarding antibiotic treatment options: World Health Organization (WHO), Finland, U.S., Australia, Czech Republic, France, Italy, Spain, Denmark, Poland, Portugal, U.K., Belgium, Germany, Ireland, Luxembourg, Netherlands, Norway, Sweden, and Switzerland. All guidelines emphasize the need for accurate diagnosis, which is the main condition in order to establish the adequate treatment.
Two types of approaches towards antibiotic administration have been identified: a watchful waiting approach and immediate antibiotic prescription. WHO guideline recommends antibiotics to all children with confirmed AOM. Immediate antibiotics for any AOM can be considered according to Finland, U.S. and Czech Republic guidelines, whereas the rest of the guidelines mentioned above (16/20) encourage the watchful waiting approach. The indications for immediate antibiotic treatment are also based on the presence of severe symptoms (fever, otalgia, pain, vomiting, diarrhea, tympanic membrane perforation, or otorrhea) and the recurrence of AOM episodes (Table 3). The advantages of the watchful waiting approach are both economic, in terms of cost savings, and also microbiological by preventing the emergence of antibiotic resistance [64]. The decision of whether to immediately recommend antibiotics or to allow the patient an observation period of 48 to 72 h in order to obtain a spontaneous clearing of the OM infections is based on an accurate diagnosis. As there is no available gold standard diagnostic test, the guidelines aim to provide greater precision in the diagnosis and treatment of AOM.
Table 3.
Indications for immediate antibiotic treatment.
Seventy-five percent (15/20) of the guidelines include young age as a criterion for immediate antimicrobial treatment; 57% (8/14) of them recommend antibiotic therapy for children younger than 24 months old. Only 20% (4/20) of the guidelines recommend antibiotics as a first-choice treatment in children with unilateral AOM, whereas 75% (14/20) of guidelines support immediate antibiotic treatment in cases of bilateral AOM in children aged less than 2 years. The decision to prescribe antimicrobial treatment as a first-line choice is based on the presence of severe symptoms (fever, otalgia, pain, vomiting, and diarrhea) in 85% (17/20) of the guidelines included in this review.
Recommendations regarding the management of recurrent AOM (three or more episodes of AOM in the previous 6 months or four or more episodes in the last 12 months) are included in 40% (8/20) of the guidelines included in this review. Long-term antibiotics are not recommended routinely. The Australian guidelines encourage treatment with long-term antibiotics (e.g., amoxicillin 25–50 mg/kg 1–2 times daily) for 3–6 months in children <2 years of age who are at risk of developing chronic suppurative otitis media. Antibiotic stewardship is promoted by providing clear diagnostic criteria (18/20 guidelines, except Ireland and Switzerland) and by clearly specifying the moment when to initiate antimicrobial treatment (20/20). Almost all the guidelines (19/20, except Ireland’s guideline) clearly specify the duration of antibiotic regimens. Amoxicillin is universally accepted as first-line antibiotic therapy in all included guidelines (Table 4). There is a wide variety of suggested antibiotics as second- and third-line treatments, as well as for the duration and dosage of therapy. The choice of amoxicillin is based on consideration of etiological spectrum of AOM and data on antibiotic resistance. The benefits of antibiotic treatment for AOM consist of the management of pain and the reduction in the risk of serious, acute complications as well as the risk of the long-term sequelae, including chronic suppurate otitis media and mastoiditis.
Table 4.
Antimicrobial treatment recommendations.
After the introduction of national AOM clinical practice guidelines the antibiotic prescription rates decreased by 12% with an increase of up to 58% for the recommended first choice antibiotic [62]. Since the introduction of the first AOM management guideline in 1989 [85], various professional guidelines for AOM diagnosis and treatment have been published. The first review that attempted to compare the current guidelines in AOM management revealed that most guidelines recommend amoxicillin as first-line antibiotic, whereas options for second-line and third-line therapies varied. The authors analyzed the guidelines from selected developed and developing countries, explaining that the differences occur due to differences in local epidemiology, healthcare policy, accessibility to health facilities, and health expenditure [86]. The most recent and compressive review on clinical practice guidelines for AOM in children reveal that there are major similarities in AOM management recommendations in the included papers. In addition to the approach to antibiotic administration (immediate antibiotic treatment, options for first- or second-line antibiotics), the review also compares the methodological quality of the included guidelines, the diagnosis criteria, and whether or not these papers include country-specific resistance patterns for antibiotic administrations [87]. To discuss each of these aspects was beyond the purpose of our paper. However, we noticed some similarities between our results and the conclusions of this article regarding the common aspects discussed in both papers. Oral amoxicillin was the first-line treatment option. Almost the same criteria for immediate antibiotic recommendations were analyzed: age, unilateral AOM, bilateral AOM in children <2 years old, tympanic membrane (TM) perforation/otorrhea, and recurrent AOM. In addition to these criteria, Suzuki et al. included the comorbidities and the parental input. In contrast to this review, we attempted to offer detailed comparison of antimicrobial treatment recommendations, including not only the first-line options but also the suggested alternatives (second-line/treatment failure, third-line/allergy to first-line), in order to provide an orientation tool for clinicians.
5. Concluding Remarks
S. pneumoniae and H. influenzae remain the most important pathogens in the determination of AOM, being the bacteria against which antimicrobial treatment should be targeted. The rat, mouse, gerbil, guinea pig, and chinchilla are the preferred animals for experimental AOM models with individual advantages and disadvantages. Antibiotic resistance is rising in all parts of the world due to the misuse and overuse of the antimicrobial treatment. In response of this worrying phenomenon, new antibiotics have been proven efficient in AOM in children: Tebipenem-pivoxil, Tosufloxacin, and Cefditoren pivoxil. Overall evidence suggests that guideline adherence is effective in reducing antibiotic prescriptions. A total of 20 AOM clinical practice guidelines were included in this review: World Health Organization (WHO), Finland, U.S., Australia, Czech Republic, France, Italy, Spain, Denmark, Poland, Portugal, U.K., Belgium, Germany, Ireland, Luxembourg, Netherlands, Norway, Sweden, and Switzerland. The current guidelines on AOM management include two types of approaches towards antibiotic administration: watchful waiting approach and immediate antibiotic prescription. Amoxicillin is proposed as first-line antimicrobial therapy in all included guidelines, whereas cephalosporin, amoxicillin-clavulanic acid, or Trimethoprim-sulfamethoxazole are among the second-line antibiotics. Recommended treatment duration varied from 5 to 10 days. A higher dosage than usual is recommended for amoxicillin and amoxicillin-clavulanic acid in order to overcome resistant strains. Sixteen of the guidelines recommend immediate antibiotic treatment in case of severe symptoms (fever, otalgia, pain, vomiting, and diarrhea). Fifteen of the 20 included guidelines include age as a criterion for immediate antimicrobial treatment, eight of them recommending immediate antibiotic therapy for children younger than 24 months old. Judicious use of antibiotics is a priority, as antimicrobial resistance represents a serious threat to global public health and the adherence to guideline may reduce the treatment failures, which are usually related to antibiotic resistant strains.
Author Contributions
Conceptualization, C.G., E.L.S., G.D.S., V.B., and D.C.A.; methodology, C.G., E.L.S., G.D.S., V.B., and D.C.A.; writing—original draft preparation, G.D.S., D.C.A., and E.L.S.; visualization, G.D.S., D.C.A., and E.L.S.; supervision and critically reviewing the manuscript, V.B. and C.G.; writing—review and editing, C.G., V.B., G.D.S., D.C.A., and E.L.S. All the authors critically reviewed the manuscript. All authors have read and agreed to the published version of the manuscript.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Data Availability Statement
No new data were created or analyzed in this study. Data sharing is not applicable to this article.
Conflicts of Interest
The authors declare no conflict of interest.
Abbreviations
| AOM | acute otitis media |
| BLPB | bacterial beta-lactamase enzyme |
| IFN-γ | interferon-γ |
| IL-10 | interleukin-10 |
| IL-1β | interleukin-1β |
| IL-6 | interleukin-6 |
| IL-8 | interleukin-8 |
| IM | intramuscularly |
| IV | intravenous |
| MCP1 | monocyte chemoattractant protein-1 |
| MIC | the minimum inhibitory concentration |
| MIP-2 protein | macrophage inflammatory protein-2 |
| OME; OM | otitis media with effusion; otitis media |
| PBP | penicillin binding proteins |
| PO | per os |
| TGF-β1 | transforming growth factor-β1 |
| TM | trauma severity score |
| TNF-α | tumor necrosis factor- alpha |
| UDP | uridine diphosphate |
| WHO | World Health Organization |
References
- Schilder, A.G.M.; Chonmaitree, T.; Cripps, A.W.; Rosenfeld, R.M.; Casselbrant, M.L.; Haggard, M.P.; Venekamp, R.P. Otitis media. Nat. Rev. Dis. Prim. 2016, 2, 16063. [Google Scholar] [CrossRef]
- Leung, A.K.; Wong, A.H.C. Acute Otitis Media in Children. Recent Pat. Inflamm. Allergy Drug Discov. 2017, 11, 32–40. [Google Scholar] [CrossRef]
- Vernacchio, L.; Vezina, R.M.; Mitchell, A.A. Management of acute otitis media by primary care physicians: Trends since the release of the 2004 American Academy of Pediatrics/American Academy of Family Physicians clinical practice guideline. Pediatrics 2007, 120, 281–287. [Google Scholar] [CrossRef]
- Suzuki, K.; Kurono, Y.; Ikeda, K.; Hotomi, M.; Yano, H.; Watanabe, A.; Matsumoto, T.; Takahashi, Y.; Hanaki, H. The seventh nationwide surveillance of six otorhinolaryngological infectious diseases and the antimicrobial susceptibility patterns of the isolated pathogens in Japan. J. Infect. Chemother. 2020, 26, 890–899. [Google Scholar] [CrossRef]
- Kaur, R.; Morris, M.; Pichichero, M.E. Epidemiology of acute otitis media in the postpneumococcal conjugate vaccine era. Pediatrics 2017, 140, 20170181. [Google Scholar] [CrossRef]
- Taylor, S.; Marchisio, P.; Vergison, A.; Harriague, J.; Hausdorff, W.P.; Haggard, M. Impact of pneumococcal conjugate vaccination on otitis media: A systematic review. Clin. Infect. Dis. 2012, 54, 1765–1773. [Google Scholar] [CrossRef]
- Pumarola, F.; Marès, J.; Losada, I.; Minguella, I.; Moraga, F.; Tarragó, D.; Aguilera, U.; Casanovas, J.M.; Gadea, G.; Trías, E.; et al. Microbiology of bacteria causing recurrent acute otitis media (AOM) and AOM treatment failure in young children in Spain: Shifting pathogens in the post-pneumococcal conjugate vaccination era. Int. J. Pediatr. Otorhinolaryngol. 2013, 77, 1231–1236. [Google Scholar] [CrossRef]
- Gower, D.; McGuirt, W.F. Intracranial complications of acute and chronic infectious ear disease. Laryngoscope 1983, 93, 1028–1033. [Google Scholar] [CrossRef]
- Rosenfeld, R.M.; Kay, D. Natural history of untreated otitis media. Laryngoscope 2003, 113, 1645–1657. [Google Scholar] [CrossRef]
- Yamanaka, N.; Hotomi, M.; Billal, D.S. Clinical bacteriology and immunology in acute otitis media in children. J. Infect. Chemother. 2008, 14, 180–187. [Google Scholar] [CrossRef]
- Guven, M.; Bulut, Y.; Sezer, T.; Aladag, I.; Eyibilen, A.; Etikan, I. Bacterial etiology of acute otitis media and clinical efficacy of amoxicillin-clavulanate versus azithromycin. Int. J. Pediatr. Otorhinolaryngol. 2006, 70, 915–923. [Google Scholar] [CrossRef]
- Kono, M.; Fukushima, K.; Kamide, Y.; Kunimoto, M.; Matsubara, S.; Sawada, S.; Shintani, T.; Togawa, A.; Uchizono, A.; Uno, Y.; et al. Features predicting treatment failure in pediatric acute otitis media. J. Infect. Chemother. 2020, 27, 19–25. [Google Scholar] [CrossRef]
- Bruk, L.A.; Dunkelberger, K.E.; Khampang, P.; Hong, W.; Sadagopan, S.; Alper, C.M.; Fedorchak, M.V. Controlled release of ciprofloxacin and ceftriaxone from a single ototopical administration of antibiotic-loaded polymer microspheres and thermoresponsive gel. PLoS ONE 2020, 15, e0240535. [Google Scholar] [CrossRef]
- Melhus, Å.; Ryan, A.F. A mouse model for acute otitis media. APMIS 2003, 111, 989–994. [Google Scholar] [CrossRef]
- Tonnaer, E.L.G.M.; Sanders, E.A.M.; Curfs, J.H.A.J. Bacterial otitis media: A new non-invasive rat model. Vaccine 2003, 21, 4539–4544. [Google Scholar] [CrossRef]
- Sato, K.; Liebeler, C.L.; Quartey, M.K.; Le, C.T.; Giebink, G.S. Middle ear fluid cytokine and inflammatory cell kinetics in the chinchilla otitis media model. Infect. Immun. 1999, 67, 1943–1946. [Google Scholar] [CrossRef]
- Hardisty, R.E.; Erven, A.; Logan, K.; Morse, S.; Guionaud, S.; Sancho-Oliver, S.; Hunter, A.J.; Brown, S.D.M.; Steel, K.P. The deaf mouse mutant Jeff (Jf) is a single gene model of otitis media. J. Assoc. Res. Otolaryngol. 2003, 4, 130–138. [Google Scholar] [CrossRef][Green Version]
- Westman, E.; Lundin, S.; Hermansson, A.; Melhus, Å. β-Lactamase-Producing nontypeable Haemophilus influenzae fails to protect Streptococcus pneumoniae from amoxicillin during experimental acute otitis media. Antimicrob. Agents Chemother. 2004, 48, 3536–3542. [Google Scholar] [CrossRef]
- Tyrer, H.E.; Crompton, M.; Bhutta, M.F. What have we learned from murine models of otitis media? Curr. Allergy Asthma Rep. 2013, 13, 501–511. [Google Scholar] [CrossRef]
- Rye, M.S.; Bhutta, M.F.; Cheeseman, M.T.; Burgner, D.; Blackwell, J.M.; Brown, S.D.M.; Jamieson, S.E. Unraveling the genetics of otitis media: From mouse to human and back again. Mamm. Genome 2011, 22, 66–82. [Google Scholar] [CrossRef]
- Post, J.C. Direct evidence of bacterial biofilms in otitis media. Laryngoscope 2001, 111, 2083–2094. [Google Scholar] [CrossRef]
- Hebda, P.A.; Burckart, G.J.; Alper, C.M.; Diven, W.F.; Doyle, W.J.; Zeevi, A. Upregulation of messenger RNA for inflammatory cytokines in middle ear mucosa in a rat model of acute otitis media. Ann. Otol. Rhinol. Laryngol. 1998, 107, 501–507. [Google Scholar] [CrossRef]
- Piltcher, O.B.; Swarts, J.D.; Magnuson, K.; Alper, C.M.; Doyle, W.J.; Hebda, P.A. A rat model of otitis media with effusion caused by eustachian tube obstruction with and without Streptococcus pneumoniae infection: Methods and course. Otolaryngol. Head Neck Surg. 2002, 126, 490–498. [Google Scholar] [CrossRef]
- Yang, R.; Sabharwal, V.; Shlykova, N.; Okonkwo, O.S.; Pelton, S.I.; Kohane, D.S. Treatment of Streptococcus pneumoniae otitis media in a chinchilla model by transtympanic delivery of antibiotics. JCI Insight 2018, 3, e123415. [Google Scholar] [CrossRef]
- Genc, G.; Koyuncu, M.; Kutlar, G.; Guvenc, T.; Gacar, A.; Aksoy, A.; Arslan, S.; Kurnaz, S.C. Does systemic clarithromycin therapy have an inhibitory effect on tympanosclerosis? An experimental animal study. J. Laryngol. Otol. 2015, 129, 136–141. [Google Scholar] [CrossRef]
- Bhutta, M.F. Mouse models of otitis media: Strengths and limitations. Otolaryngol. Head Neck Surg. 2012, 147, 611–614. [Google Scholar] [CrossRef]
- MacArthur, C.J.; Hefeneider, S.H.; Kempton, J.B.; Parrish, S.K.; McCoy, S.L.; Trune, D.R. Evaluation of the mouse model for acute otitis media. Hear. Res. 2006, 219, 12–23. [Google Scholar] [CrossRef]
- Hebda, P.A.; Piltcher, O.B.; Swarts, J.D.; Alper, C.M.; Zeevi, A.; Doyle, W.J. Cytokine profiles in a rat model of otitis media with effusion caused by eustachian tube obstruction with and without Streptococcus pneumoniae infection. Laryngoscope 2002, 112, 1657–1662. [Google Scholar] [CrossRef]
- Von Unge, M.; Decraemer, W.F.; Bagger-Sjöbäck, D.; Van Den Berghe, D. Tympanic membrane changes in experimental purulent otitis media. Hear. Res. 1997, 106, 123–136. [Google Scholar] [CrossRef]
- Von Unge, M.; Decraemer, W.F.; Buytaert, J.A.N.; Dirckx, J.J.J. Evaluation of a model for studies on sequelae after acute otitis media in the Mongolian gerbil. Acta Otolaryngol. 2009, 129, 261–267. [Google Scholar] [CrossRef]
- Larsson, C.; Dirckx, J.J.J.; Decraemer, W.F.; Bagger-Sjöbäck, D.; Von Unge, M. Pars flaccida displacement pattern in purulent otitis media in the gerbil. Otol. Neurotol. 2003, 24, 358–364. [Google Scholar] [CrossRef][Green Version]
- Wang, X.; Fernandez, R.; Tsivkovskaia, N.; Harrop-Jones, A.; Hou, H.J.; Dellamary, L.; Dolan, D.F.; Altschuler, R.A.; Lebel, C.; Piu, F. OTO-201: Nonclinical assessment of a sustained-release ciprofloxacin hydrogel for the treatment of otitis media. Otol. Neurotol. 2014, 35, 459–469. [Google Scholar] [CrossRef]
- Chen, Y.J.; Hsieh, Y.C.; Huang, Y.C.; Chiu, C.H. Clinical manifestations and microbiology of acute otitis media with spontaneous otorrhea in children. J. Microbiol. Immunol. Infect. 2013, 46, 382–388. [Google Scholar] [CrossRef]
- Van Dongen, T.M.A.; Venekamp, R.P.; Wensing, A.M.J.; Bogaert, D.; Sanders, E.A.M.; Schilder, A.G.M. Acute otorrhea in children with tympanostomy tubes: Prevalence of bacteria and viruses in the post-pneumococcal conjugate vaccine era. Pediatr. Infect. Dis. J. 2015, 34, 355–360. [Google Scholar] [CrossRef]
- Minovi, A.; Dazert, S. Erkrankungen des Mittelohres im Kindesalter. Laryngorhinootologie 2014, 93, S1–S23. [Google Scholar] [CrossRef]
- Rosenfeld, R.M.; Vertrees, J.E.; Carr, J.; Cipolle, R.J.; Uden, D.L.; Giebink, G.S.; Canafax, D.M. Clinical efficacy of antimicrobial drugs for acute otitis media: Metaanalysis of 5400 children from thirty-three randomized trials. J. Pediatr. 1994, 124, 355–367. [Google Scholar] [CrossRef]
- Uçar, S.; Huseynov, T.; Çoban, M.; Sarıoğlu, S.; Serbetçioğlu, B.; Yalcin, A.D. Montelukast is as effective as penicillin in treatment of acute otitis media: An experimental rat study. Med. Sci. Monit. Basic Res. 2013, 19, 246–252. [Google Scholar] [CrossRef]
- Yang, R.; Sabharwal, V.; Okonkwo, O.S.; Shlykova, N.; Tong, R.; Lin, L.Y.; Wang, W.; Guo, S.; Rosowski, J.J.; Pelton, S.I.; et al. Treatment of otitis media by transtympanic delivery of antibiotics. Sci. Transl. Med. 2016, 8. [Google Scholar] [CrossRef]
- Mather, M.W.; Drinnan, M.; Perry, J.D.; Powell, S.; Wilson, J.A.; Powell, J. A systematic review and meta-analysis of antimicrobial resistance in paediatric acute otitis media. Int. J. Pediatr. Otorhinolaryngol. 2019, 123, 102–109. [Google Scholar] [CrossRef]
- Rosenblüt, A.; Santolaya, M.E.; Gonzalez, P.; Borel, C.; Cofré, J. Penicillin resistance is not extrapolable to amoxicillin resistance in Streptococcus pneumoniae isolated from middle ear fluid in children with acute otitis media. Ann. Otol. Rhinol. Laryngol. 2006, 115, 186–190. [Google Scholar] [CrossRef]
- Brook, I. The role of anaerobic bacteria in chronic suppurative otitis media in children: Implications for medical therapy. Anaerobe 2008, 14, 297–300. [Google Scholar] [CrossRef] [PubMed]
- Argaw-Denboba, A.; Abejew, A.A.; Mekonnen, A.G. Antibiotic-Resistant Bacteria are Major Threats of Otitis Media in Wollo Area, Northeastern Ethiopia: A Ten-Year Retrospective Analysis. Int. J. Microbiol. 2016, 2016. [Google Scholar] [CrossRef] [PubMed]
- Korona-Glowniak, I.; Zychowski, P.; Siwiec, R.; Mazur, E.; Niedzielska, G.; Malm, A. Resistant Streptococcus pneumoniae strains in children with acute otitis media- high risk of persistent colonization after treatment. BMC Infect. Dis. 2018, 18, 478. [Google Scholar] [CrossRef] [PubMed]
- Kumar, A.; Asthana, M.; Gupta, A.; Nigam, D.; Mahajan, S. Secondary metabolism and antimicrobial metabolites of penicillium. In New and Future Developments in Microbial Biotechnology and Bioengineering: Penicillium System Properties and Applications; Elsevier: Amsterdam, The Netherlands, 2017; pp. 47–68. ISBN 9780444635013. [Google Scholar]
- Fisher, J.F.; Meroueh, S.O.; Mobashery, S. Bacterial resistance to β-lactam antibiotics: Compelling opportunism, compelling opportunity. Chem. Rev. 2005, 105, 395–424. [Google Scholar] [CrossRef] [PubMed]
- Lima, L.M.; da Silva, B.N.M.; Barbosa, G.; Barreiro, E.J. β-Lactam antibiotics: An overview from a medicinal chemistry perspective. Eur. J. Med. Chem. 2020, 208, 112829. [Google Scholar] [CrossRef]
- Fairbanks, D.N.F. Pocket Guide to Otolaryngology-Head and Neck Surgery, 13rd ed.; The American Academy of Otolaryngology-Head and Neck Surgery Foundation: Alexandria, VA, USA, 2007. [Google Scholar]
- Chiappini, E.; Motisi, M.A.; Becherucci, P.; Pierattelli, M.; Galli, L.; Marchisio, P. Italian primary care paediatricians’ adherence to the 2019 National Guideline for the management of acute otitis media in children: A cross-sectional study. Int. J. Pediatr. Otorhinolaryngol. 2020, 138, 110282. [Google Scholar] [CrossRef]
- Brook, I. Microbiology and Principles of Antimicrobial Therapy for Head and Neck Infections. Infect. Dis. Clin. N. Am. 2007, 21, 355–391. [Google Scholar] [CrossRef]
- Yano, H. Analysis of nasopharyngeal flora in children with acute otitis media attending a day care center. Jpn. J. Antibiot. 2003, 56, 87–92. [Google Scholar]
- Kitamura, K.; Iino, Y.; Kamide, Y.; Kudo, F.; Nakayama, T.; Suzuki, K.; Taiji, H.; Takahashi, H.; Yamanaka, N.; Uno, Y. Clinical Practice Guidelines for the diagnosis and management of acute otitis media (AOM) in children in Japan—2013 Update. Auris Nasus Larynx 2015, 42, 99–106. [Google Scholar] [CrossRef]
- Sugita, R. Good transfer of tebipenem into middle ear effusion conduces to the favorable clinical outcomes of tebipenem pivoxil in pediatric patients with acute otitis media. J. Infect. Chemother. 2013, 19, 465–471. [Google Scholar] [CrossRef]
- Tanaka, E.; Hara, N.; Wajima, T.; Ochiai, S.; Seyama, S.; Shirai, A.; Shibata, M.; Shiro, H.; Natsume, Y.; Noguchi, N. Emergence of Haemophilus influenzae with low susceptibility to quinolones and persistence in tosufloxacin treatment. J. Glob. Antimicrob. Resist. 2019, 18, 104–108. [Google Scholar] [CrossRef]
- Seyama, S.; Wajima, T.; Yanagisawa, Y.; Nakaminami, H.; Ushio, M.; Fujii, T.; Noguchi, N. Rise in Haemophilus influenzae with reduced quinolone susceptibility and development of a simple screening method. Pediatr. Infect. Dis. J. 2017, 36, 263–266. [Google Scholar] [CrossRef]
- Seyama, S.; Wajima, T.; Nakaminami, H.; Noguchi, N. Clarithromycin resistance mechanisms of epidemic β-lactamase-nonproducing ampicillin-resistant Haemophilus influenzae strains in Japan. Antimicrob. Agents Chemother. 2016, 60, 3207–3210. [Google Scholar] [CrossRef]
- Wajima, T.; Seyama, S.; Nakamura, Y.; Kashima, C.; Nakaminami, H.; Ushio, M.; Fujii, T.; Noguchi, N. Prevalence of macrolide-non-susceptible isolates among β-lactamase-negative ampicillin-resistant Haemophilus influenzae in a tertiary care hospital in Japan. J. Glob. Antimicrob. Resist. 2016, 6, 22–26. [Google Scholar] [CrossRef]
- Biedenbach, D.J.; Jones, R.N. Update of cefditoren activity tested against community-acquired pathogens associated with infections of the respiratory tract and skin and skin structures, including recent pharmacodynamic considerations. Diagn. Microbiol. Infect. Dis. 2009, 64, 202–212. [Google Scholar] [CrossRef]
- Jones, R.N.; Pfaller, M.A.; Jacobs, M.R.; Appelbaum, P.C.; Fuchs, P.C. Cefditoren in vitro activity and spectrum: A review of international studies using reference methods. Diagn. Microbiol. Infect. Dis. 2001, 41, 1–14. [Google Scholar] [CrossRef]
- Lodise, T.P.; Kinzig-Schippers, M.; Drusano, G.L.; Loos, U.; Vogel, F.; Bulitta, J.; Hinder, M.; Sörgel, F. Use of population pharmacokinetic modeling and Monte Carlo simulation to describe the pharmacodynamic profile of cefditoren in plasma and epithelial lining fluid. Antimicrob. Agents Chemother. 2008, 52, 1945–1951. [Google Scholar] [CrossRef][Green Version]
- Sevillano, D.; Giménez, M.J.; Alou, L.; Aguilar, L.; Cafini, F.; Torrico, M.; González, N.; Echeverría, O.; Coronel, P.; Prieto, J. Effects of human albumin and serum on the in vitro bactericidal activity of cefditoren against penicillin-resistant Streptococcus pneumoniae. J. Antimicrob. Chemother. 2007, 60, 156–158. [Google Scholar] [CrossRef][Green Version]
- Seral, C.; Suárez, L.; Rubio-Calvo, C.; Gómez-Lus, R.; Gimeno, M.; Coronel, P.; Durán, E.; Becerril, R.; Oca, M.; Castillo, F.J. In vitro activity of cefditoren and other antimicrobial agents against 288 Streptococcus pneumoniae and 220 Haemophilus influenzae clinical strains isolated in Zaragoza, Spain. Diagn. Microbiol. Infect. Dis. 2008, 62, 210–215. [Google Scholar] [CrossRef]
- Deniz, Y.; Van Uum, R.T.; De Hoog, M.L.A.; Schilder, A.G.M.; Damoiseaux, R.A.M.J.; Venekamp, R.P. Impact of acute otitis media clinical practice guidelines on antibiotic and analgesic prescriptions: A systematic review. Arch. Dis. Child 2018, 103, 597–602. [Google Scholar] [CrossRef]
- Dona, D.; Baraldi, M.; Brigadoi, G.; Lundin, R.; Perilongo, G.; Hamdy, R.F.; Zaoutis, T.; Da Dalt, L.; Giaquinto, C. The Impact of Clinical Pathways on Antibiotic Prescribing for Acute Otitis Media and Pharyngitis in the Emergency Department. Pediatr. Infect. Dis. J. 2018, 37, 901–907. [Google Scholar] [CrossRef]
- Sun, D.; McCarthy, T.J.; Liberman, D.B. Cost-Effectiveness of watchful waiting in acute Otitis media. Pediatrics 2017, 139, e20163086. [Google Scholar] [CrossRef]
- World Health Organization. Recommendations for Management of Common Childhood Conditions: Evidence for Technical Update of Pocket Book Recommendations; WHO: Geneva, Switzerland, 2010. [Google Scholar]
- Lieberthal, A.S.; Carroll, A.E.; Chonmaitree, T.; Ganiats, T.G.; Hoberman, A.; Jackson, M.A.; Joffe, M.D.; Miller, D.T.; Rosenfeld, R.M.; Sevilla, X.D.; et al. The diagnosis and management of acute otitis media. Pediatrics 2013, 131, e964–e999. [Google Scholar] [CrossRef]
- Australian Government Department of Health. Darwin Otitis Guidelines Group Recommendations for Clinical Care Guidelines on the Management of Otitis Media in Aboriginal and Torres Strait Islander Populations. Available online: https://www1.health.gov.au/internet/publications/publishing.nsf/Content/oatsih-otitis-media-toc~Using-the-Recommendations-for-Clinical-Care-Guidelines-on-Otitis-Media (accessed on 28 November 2020).
- National Institute for Health and Care Excellence. Otitis Media (Acute): Antimicrobial Prescribing NICE Guideline; National Institute for Health and Care Excellence: London, UK, 2018. [Google Scholar]
- Marchisio, P.; Bellussi, L.; Di Mauro, G.; Doria, M.; Felisati, G.; Longhi, R.; Novelli, A.; Speciale, A.; Mansi, N.; Principi, N. Acute otitis media: From diagnosis to prevention. Summary of the Italian guideline. Int. J. Pediatr. Otorhinolaryngol. 2010, 74, 1209–1216. [Google Scholar] [CrossRef]
- Del Castillo Martín, F.; Baquero Artigao, F.; de la Calle Cabrera, T.; López Robles, M.V.; Ruiz-Canela Cáceres, J.; Alfayate Miguélez, S.; Moraga Llop, F.; Cilleruelo Ortega, M.J.; Calvo Rey, C. Consensus document on the aetiology, diagnosis and treatment of acute otitis media. Pediatr. Atension Primaria 2012, 14, 195–205. [Google Scholar] [CrossRef]
- Dansk Selskab for Almen Medicin. Luftvejsinfektioner—DSAM Vejledninger. Respiratory Tract Infections—Diagnosis and Treatment 2014. Available online: https://vejledninger.dsam.dk/luftvejsinfektioner/ (accessed on 28 November 2020).
- Agence Française de Sécurité Sanitaire des Produits de Santé. Antibiothérapie par Voie Générale en Pratique Courante—EM Consulte. Recommendations for Good Practice—Antimicrobials by General Route in Current Practice in Upperrespiratory Tract Infections. Available online: https://www.em-consulte.com/article/143366/antibiotherapie-par-voie-generale-en-pratique-cour (accessed on 28 November 2020).
- Ralston, S.L.; Lieberthal, A.S.; Meissner, H.C.; Alverson, B.K.; Baley, J.E.; Gadomski, A.M.; Johnson, D.W.; Light, M.J.; Maraqa, N.F.; Mendonca, E.A.; et al. Clinical practice guideline: The diagnosis, management, and prevention of bronchiolitis. Pediatrics 2014, 134, e1474–e1502. [Google Scholar] [CrossRef]
- Kingery, J.; Taylor, W.; Braun, D. Acute otitis media. Osteopath. Fam. Physician 2016, 8, 22–25. [Google Scholar]
- Deutsche Gesellschaft für Allegemeinmedizin und Familienmedizin (DEGAM). DEGAM-Leitlinie Nr 7-Ohrenschmerzen [DEGAM Guideline Number 7—Earache]. Available online: https://www.awmf.org/en/clinical-practice-guidelines/search-for-guidelines.html#result-list (accessed on 28 November 2020).
- Health Services Executive and Royal College of Physicians Ireland. Acute Otitis Media. Available online: https://www.hse.ie/eng/services/publications/clinical-strategy-and-programmes/paediatrics-acute-otitis-media.pdf (accessed on 28 November 2020).
- Conseil Scientifique Domaine de la Santé Otite Moyenne Aigue. Acute Otitis Media. Available online: https://conseil-scientifique.public.lu/dam-assets/publications/antibiotherapie/otite-version-longue.pdf (accessed on 28 November 2020).
- Damoiseaux, R.A.M.J.; Venekamp, R.P.; Eekhof, J.A.H.; Bennebroek Gravenhorst, F.M.; Schoch, A.G.; Burgers, J.S.; Bouma, M.W.J. Otitis Media Acuta Bij Kinderen/NHG-Richtlijnen. Available online: https://richtlijnen.nhg.org/standaarden/otitis-media-acuta-bij-kinderen (accessed on 28 November 2020).
- Karma, P.; Palva, T.; Kouvalainen, K.; Kärjä, J.; Mäkelä, P.H.; Prinssi, V.P.; Ruuskanen, O.; Launiala, K. Finnish Approach to the Treatment of Acute Otitis Media Report of the Finnish Consensus Conference. Ann. Otol. Rhinol. Laryngol. 1987, 129, 1–19. [Google Scholar] [CrossRef]
- Tuerlinckx, D. L’usage Rationnel des Antibiotiques Chez L’enfant en Ambulatoire; INAMI: Bruxeles, Belgium, 2016. [Google Scholar]
- Hryniewicz, W.; Piotr Albrecht, P.; Radzikowski, A. Rekomendacje Postępowania w Pozaszpitalnych Zakażeniach Układu Oddechowego; Narodowy Instytut Leków: Warsaw, Poland, 2016; ISBN 978-83-938000-5-6. [Google Scholar]
- Groth, A. Diagnostik, Behandling och Uppföljning av Akut Mediaotit (AOM)—Bakgrundsdokumentation; Information från Läkemedelsverket: Uppsala, Sweden, 2010. [Google Scholar]
- Bernhard, S.; Büttcher, M.; Heininger, U.; Ratnam, S.; Johannes Trück, C.R.; Wagner, N.; Zucol, F.; Berger, C.; Ritz, N. Guidance for Testing and Preventing Infections and Updating Immunisations in Asymptomatic Refugee Children and Adolescents in Switzerland. Pediatrica 2016, 27, 11–18. [Google Scholar]
- Bébrová, E.J.B.; Cizek, H.; Vaclav, D.; Galský, J.; Prakt, L. Doporučený postup pro antibiotickou léčbu komunitních respiračních infekcí v primární péči. Prakt. Lék 2003, 83, 502–515. [Google Scholar]
- Van Buchem, F.L. The treatment of acute otitis media. Ned. Tijdschr. Geneeskd. 1989, 133, 290–292. [Google Scholar] [PubMed]
- Ovnat Tamir, S.; Shemesh, S.; Oron, Y.; Marom, T. Acute otitis media guidelines in selected developed and developing countries: Uniformity and diversity. Arch. Dis. Child. 2017, 102, 450–457. [Google Scholar] [CrossRef] [PubMed]
- Suzuki, H.G.; Dewez, J.E.; Nijman, R.G.; Yeung, S. Clinical practice guidelines for acute otitis media in children: A systematic review and appraisal of European national guidelines. BMJ Open 2020, 10, 35343. [Google Scholar] [CrossRef] [PubMed]

Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).