Non-Invasive Diagnosis of Diabetes by Volatile Organic Compounds in Urine Using FAIMS and Fox4000 Electronic Nose

 , , and
, , and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Sample Preparation
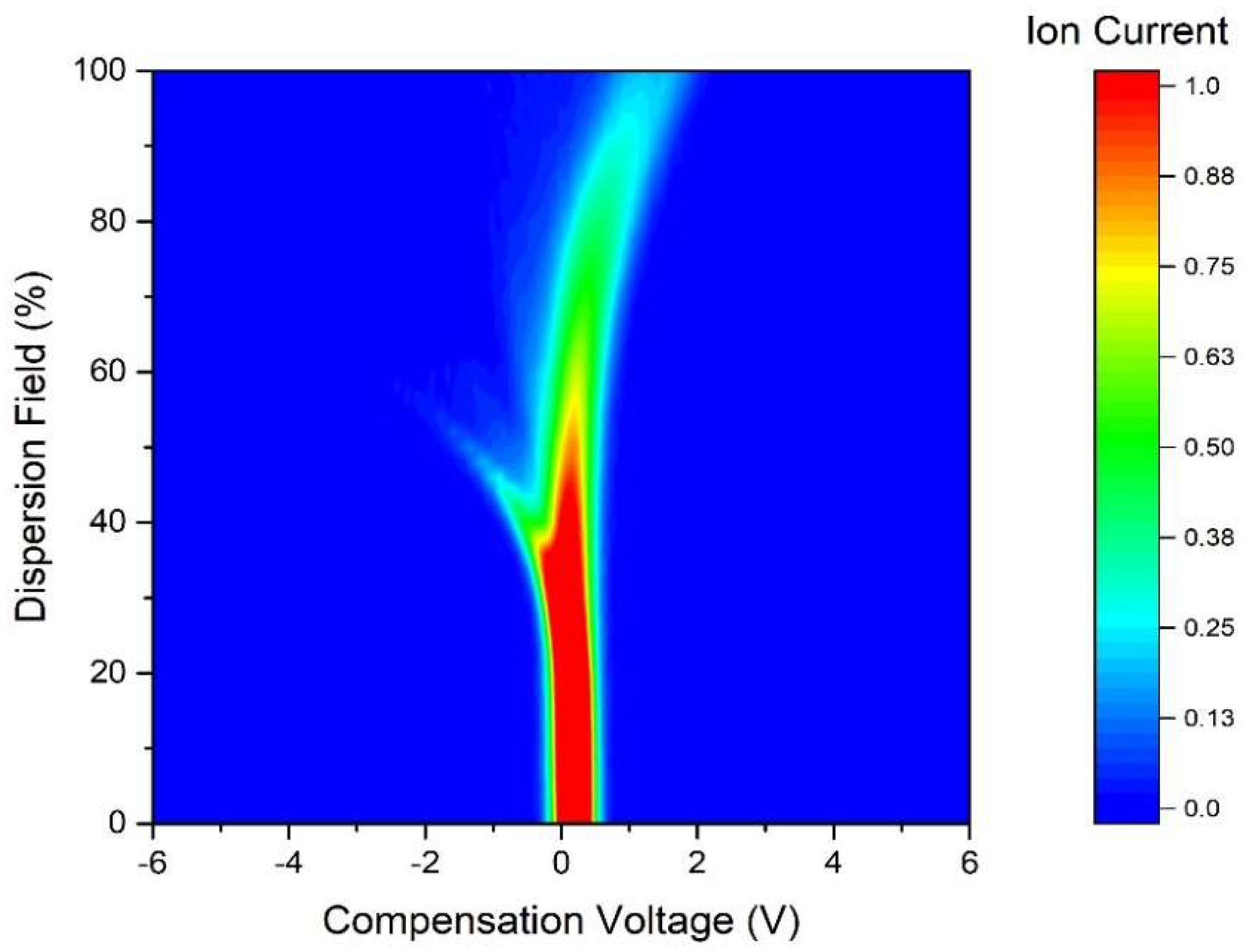
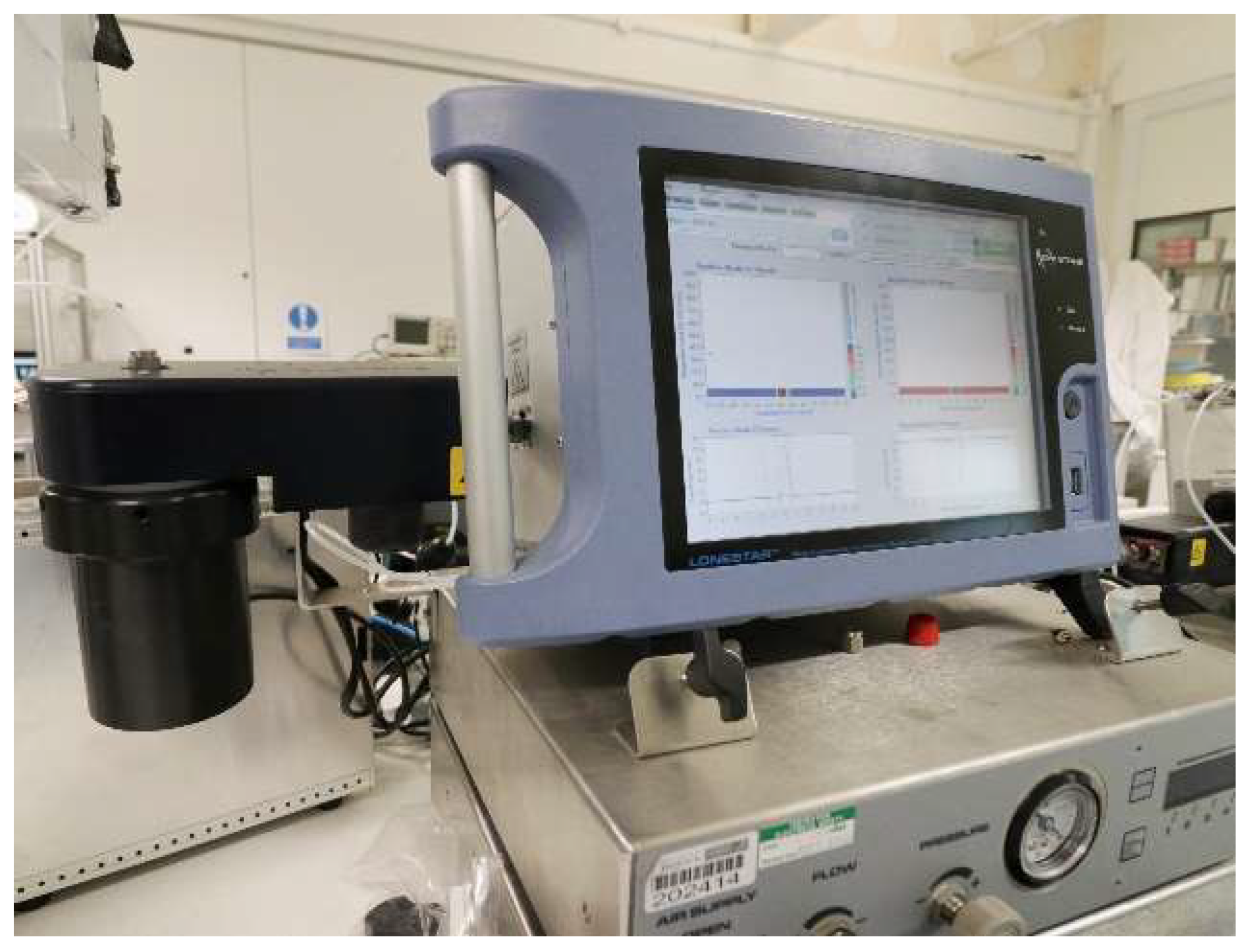
2.2. FAIMS Chemical Analyser
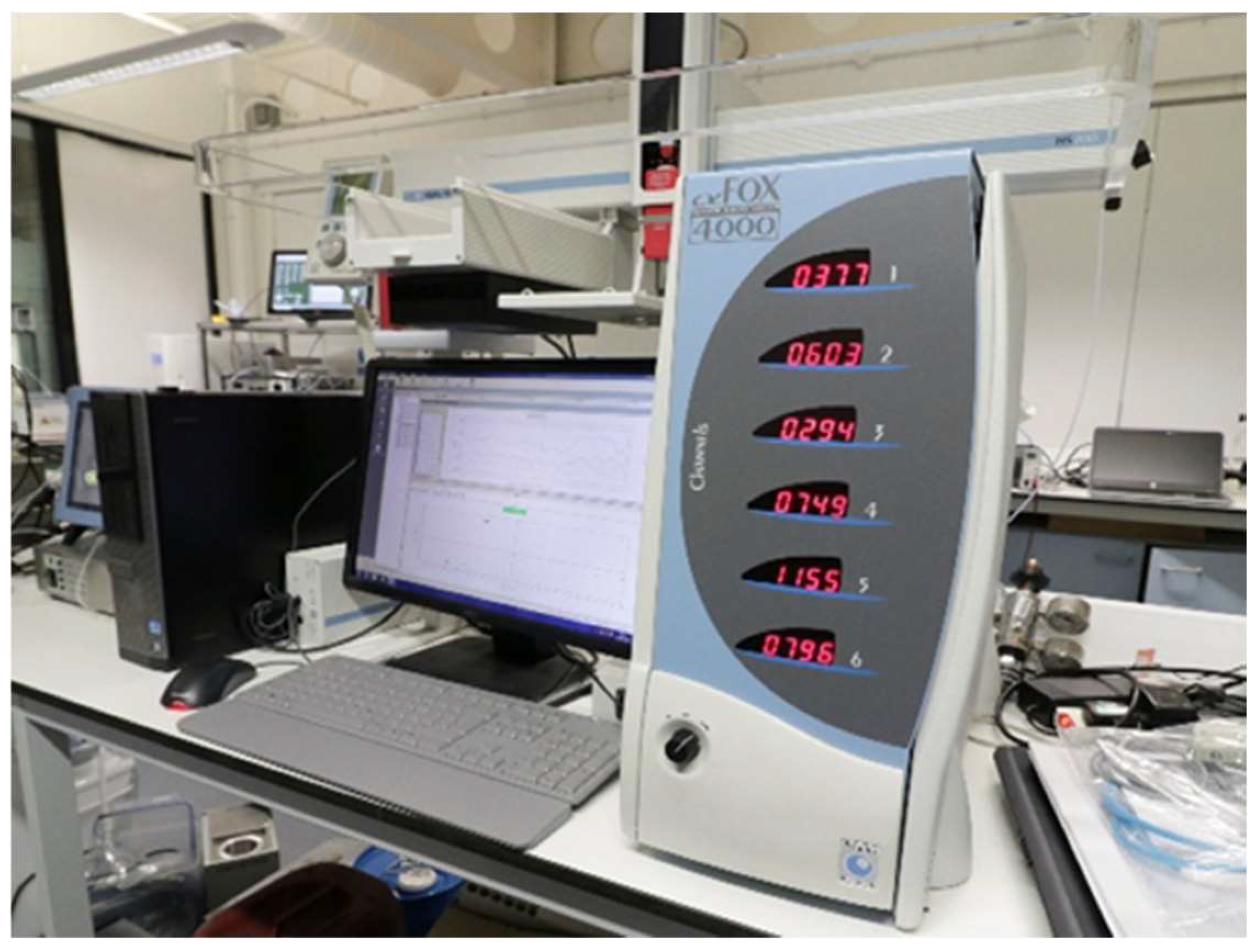
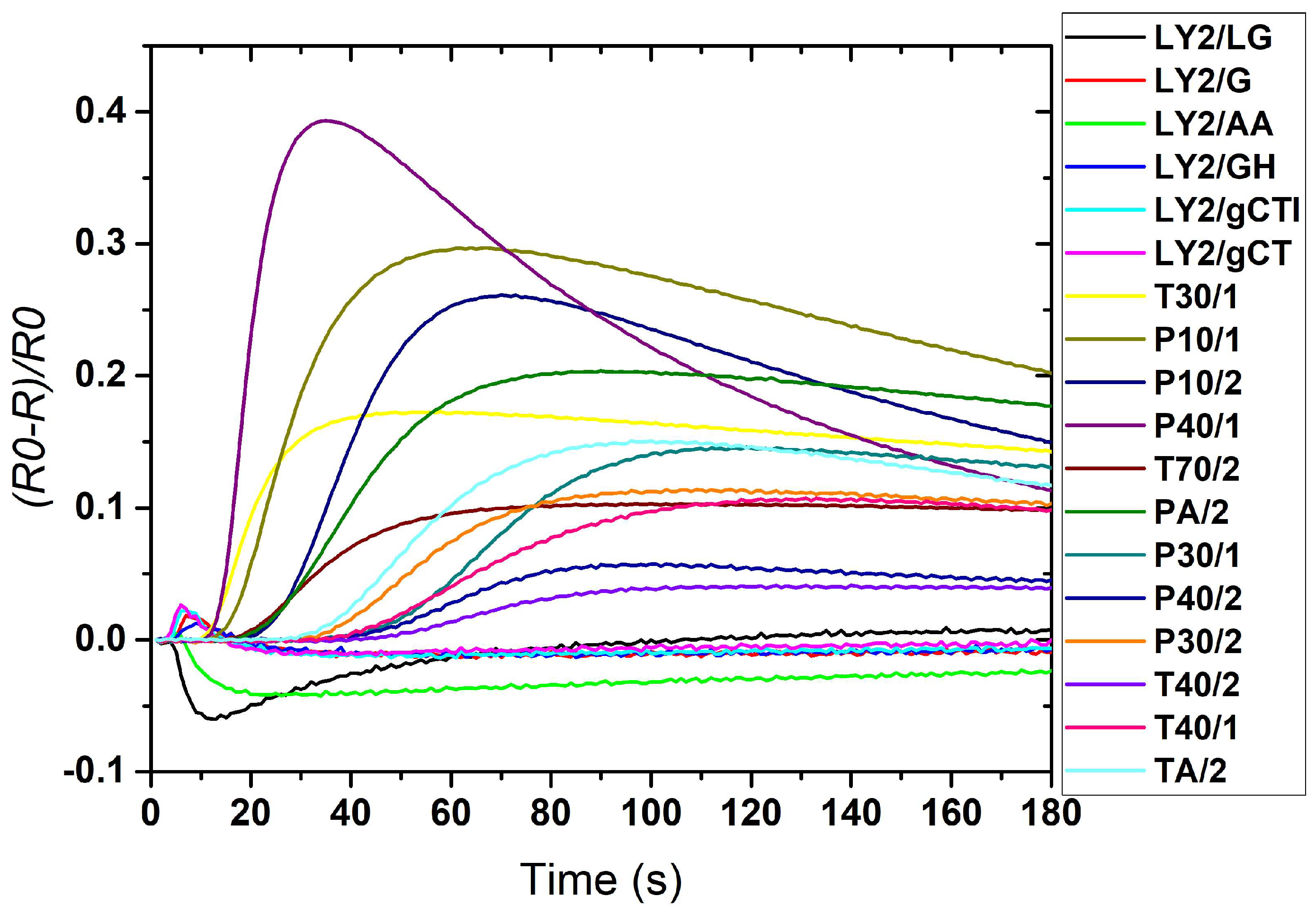
2.3. Electronic Nose
3. Results
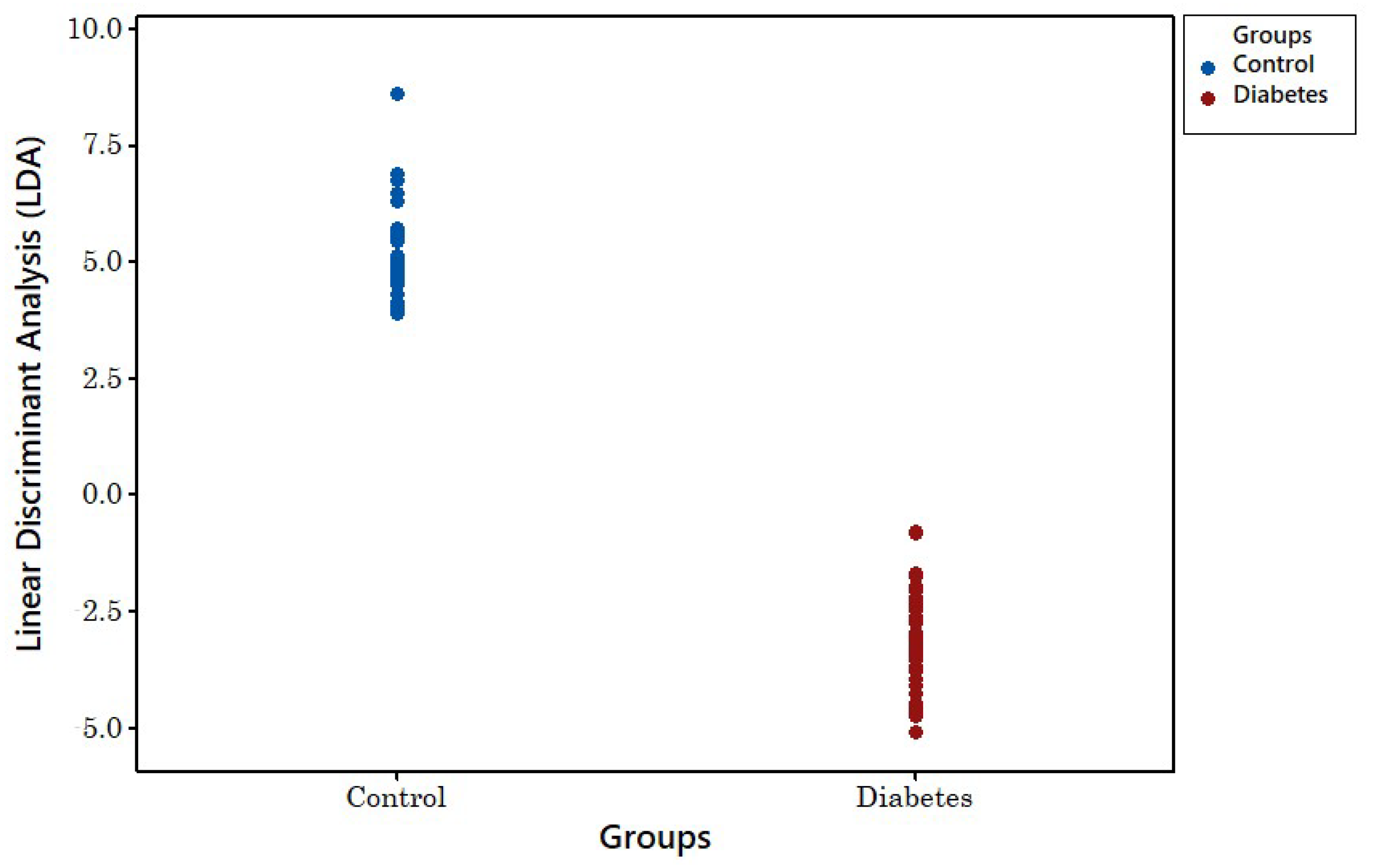
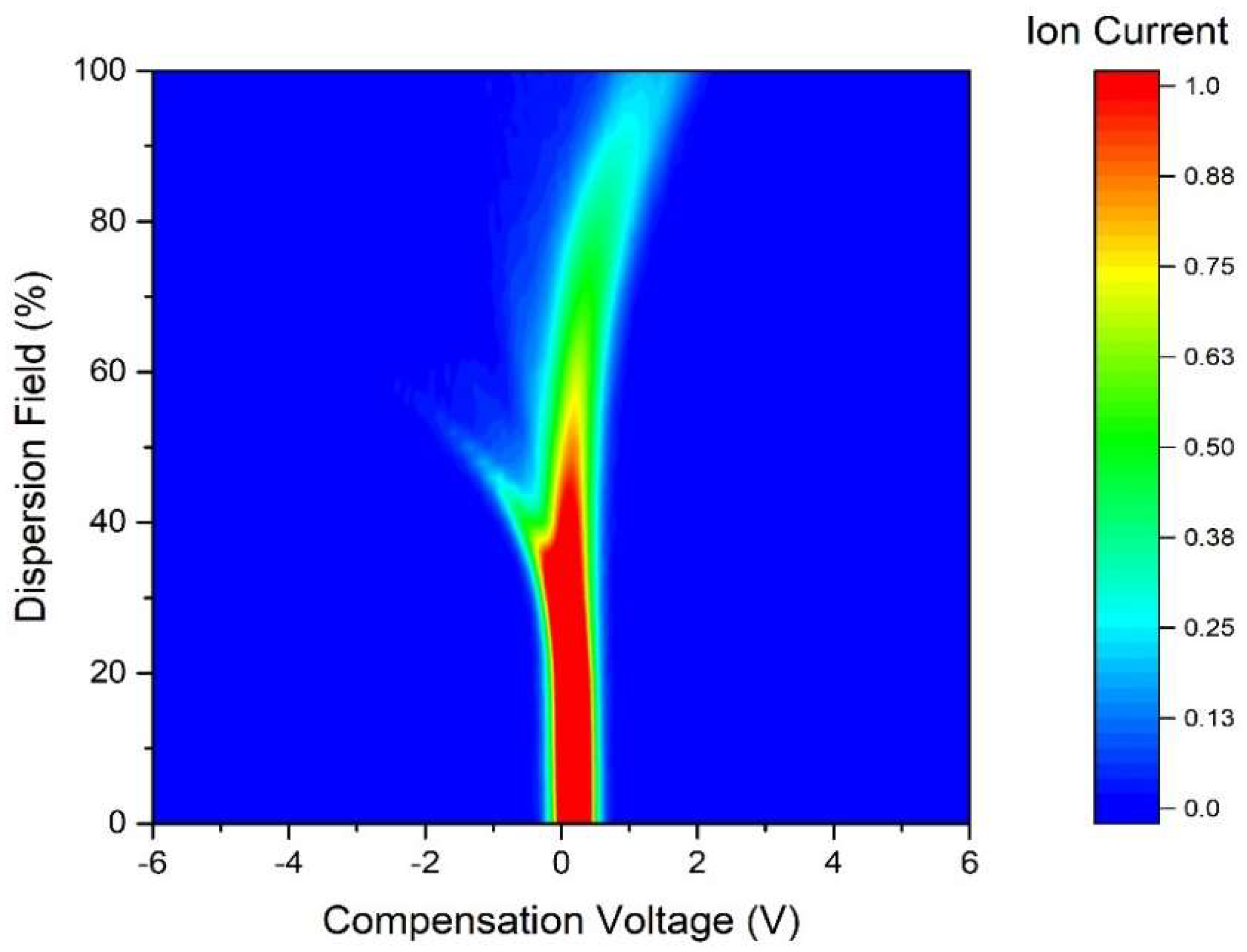
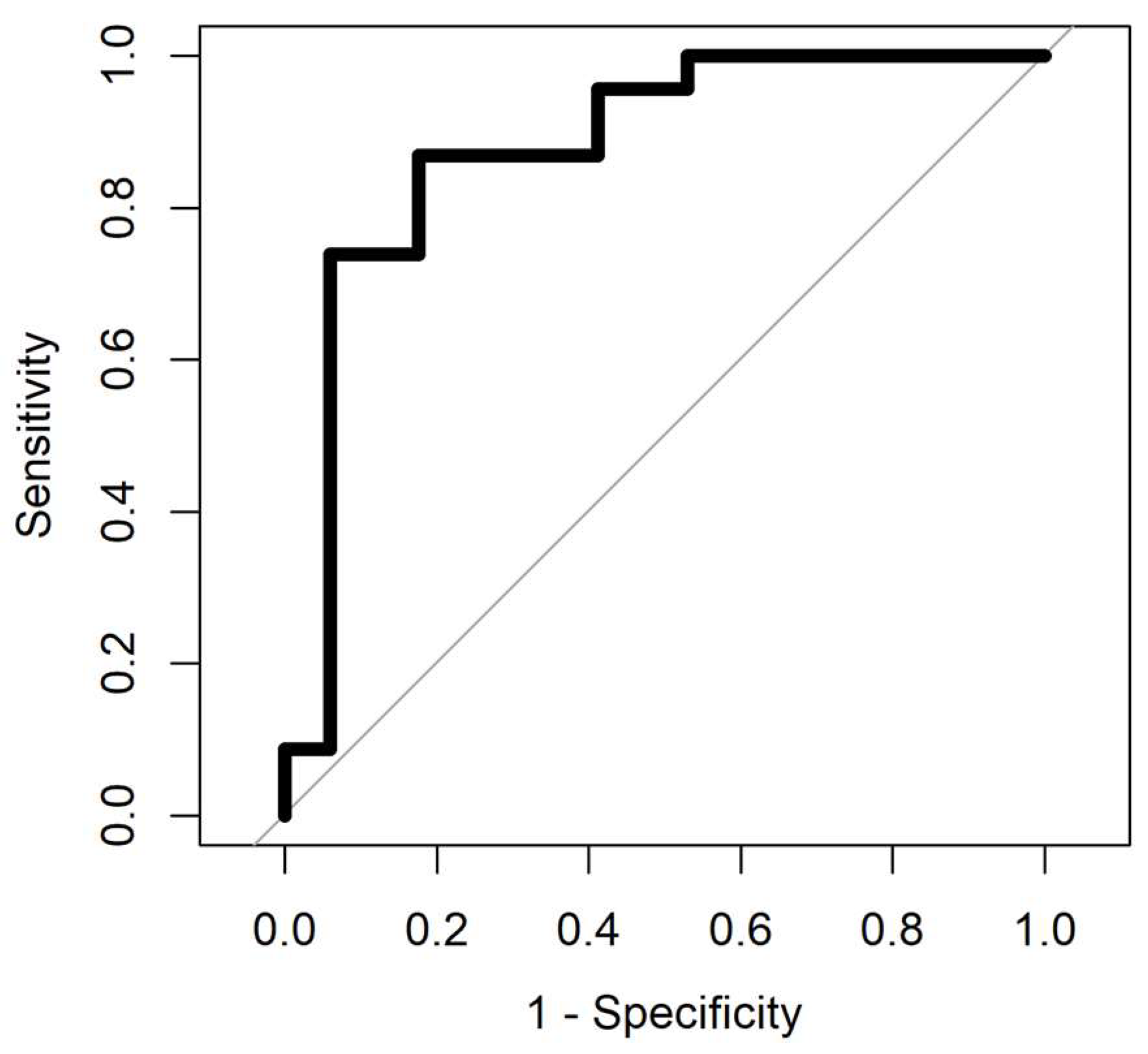
3.1. FAIMS Analysis
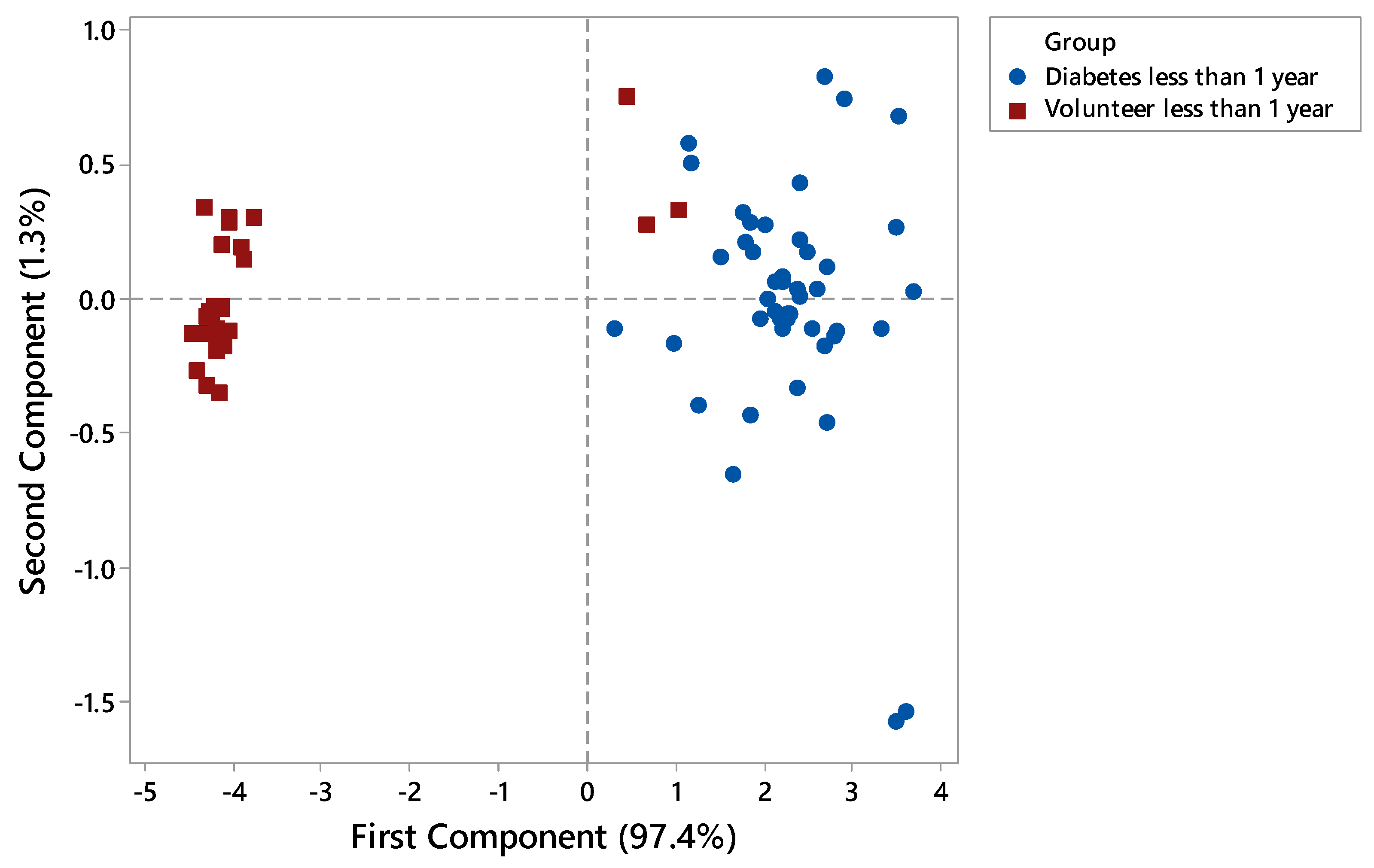
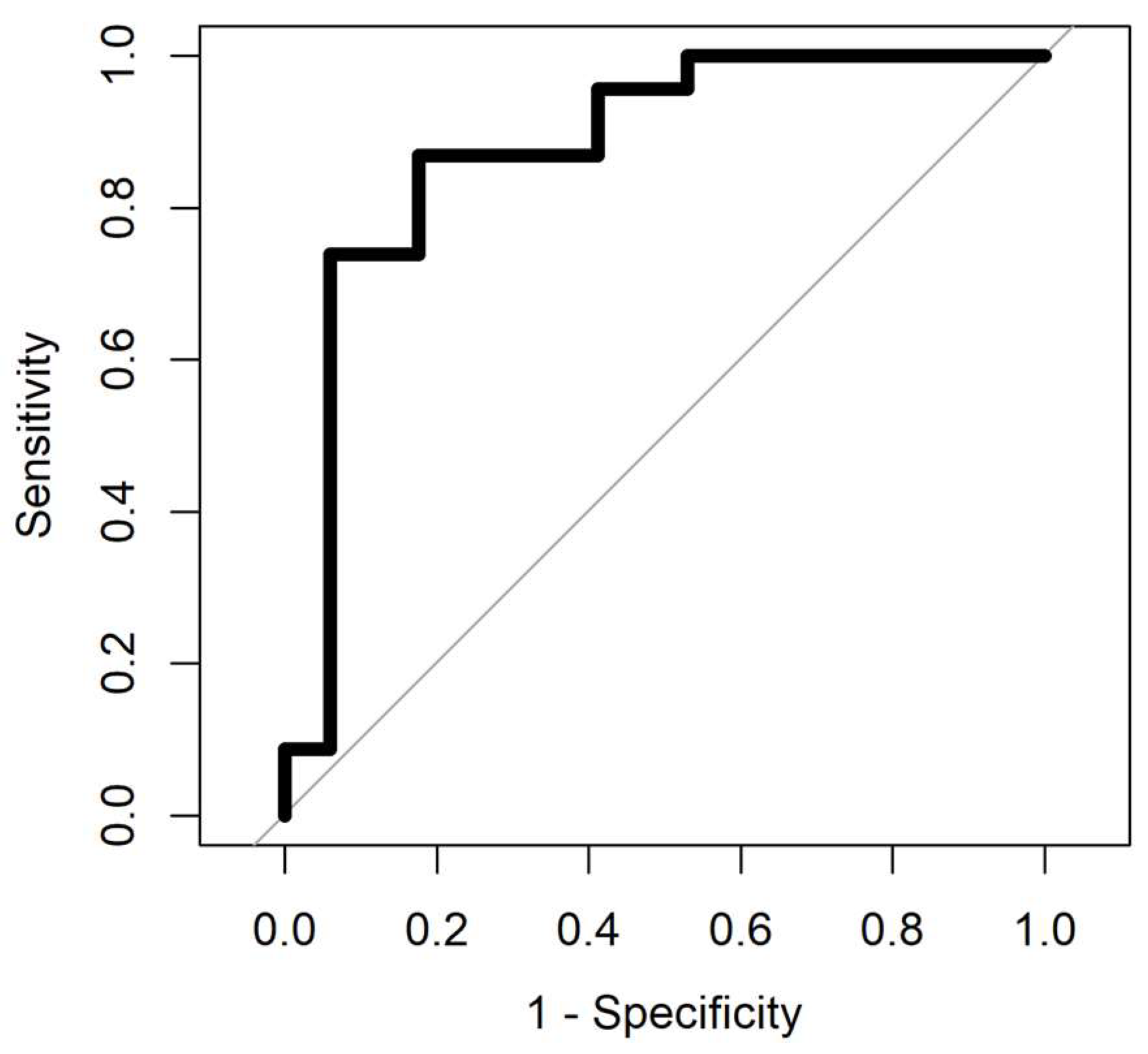
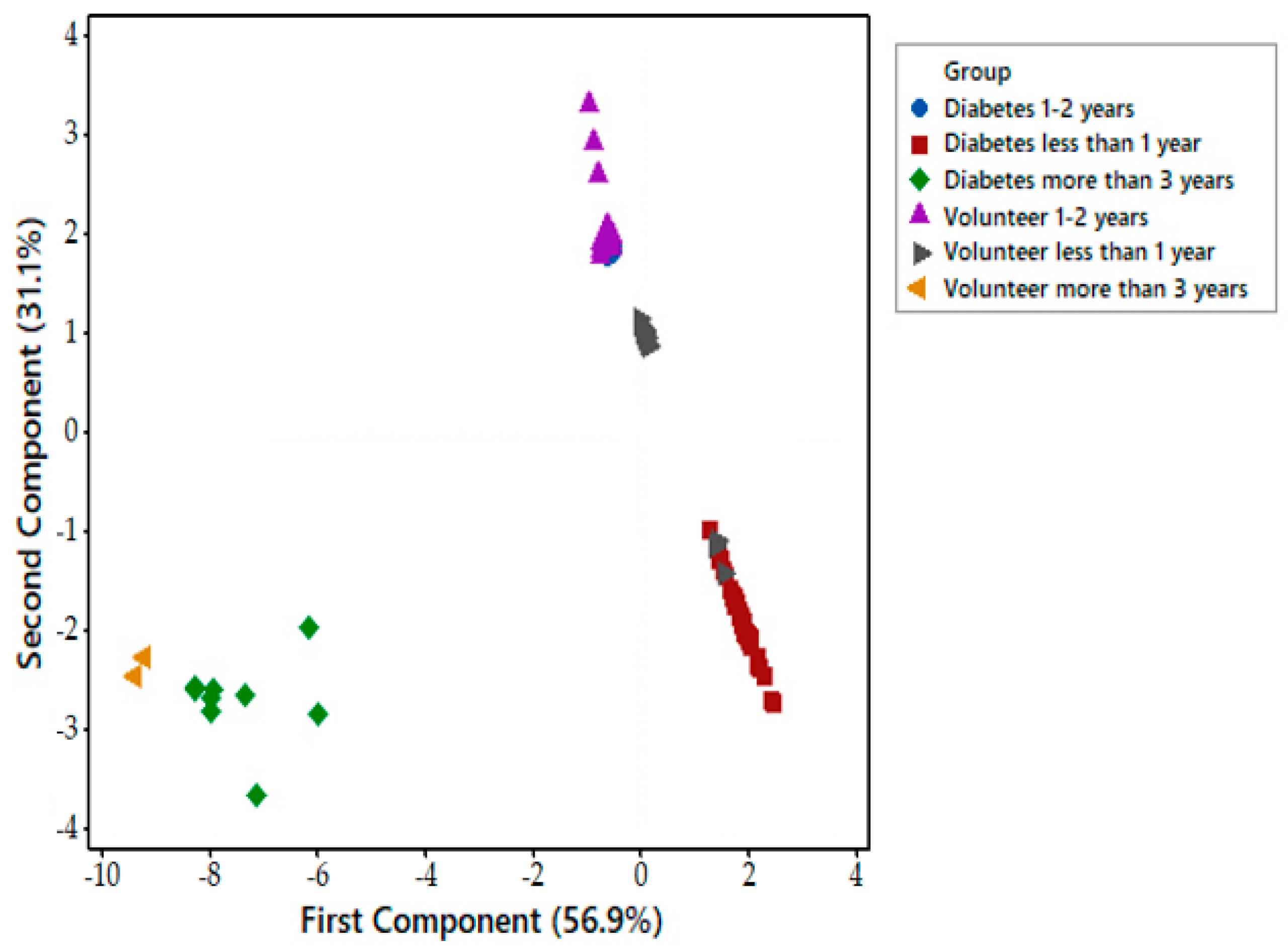
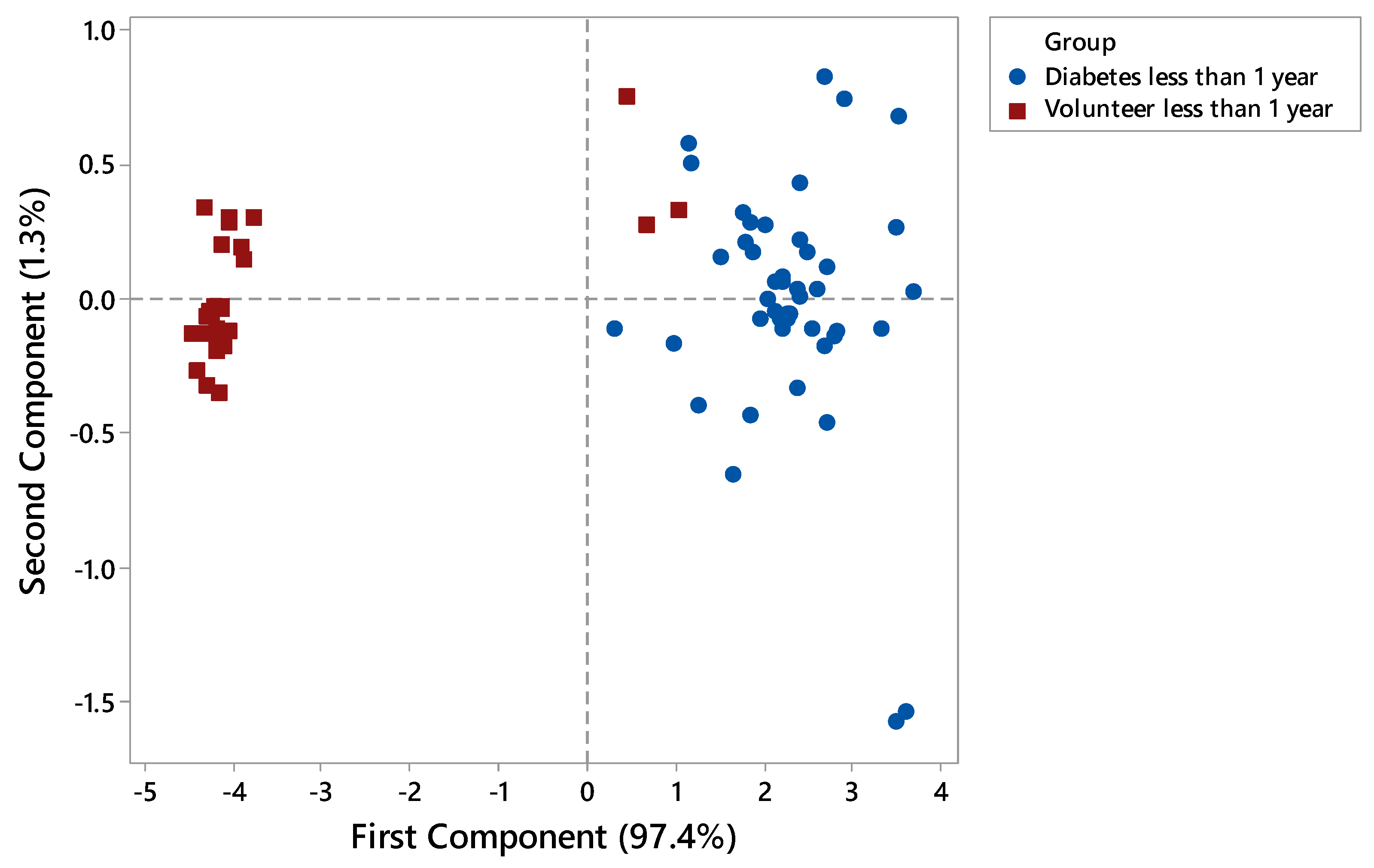
3.2. Electronic Nose Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Persaud, K.; Dodd, G. Analysis of discrimination mechanisms in the mammalian olfactory system using a model nose. Nature 1982, 299, 352–355. [Google Scholar] [CrossRef] [PubMed]
- Westenbrink, E.; Arasaradnam, R.P.; O’Connell, N.; Bailey, C.; Nwokolo, C.; Bardhan, K.D.; Covington, J.A. Development and application of a new electronic nose instrument for the detection of colorectal Cancer. Biosens. Bioelectron. 2014, 67, 733–738. [Google Scholar] [CrossRef] [PubMed]
- Covington, J.A.; Wedlake, L.; Andreyev, J.; Ouaret, N.; Thomas, M.G.; Nwokolo, C.U.; Bardhan, K.D.; Arasaradnam, R.P. The detection of patients at risk of gastrointestinal toxicity during pelvic radiotherapy by electronic nose and FAIMS: A pilot study. Sensors 2012, 12, 13002–13018. [Google Scholar] [CrossRef] [PubMed]
- Van de Goor, R.; van Hooren, M.; Dingemans, A.-M.; Kremer, B.; Kross, K. Training and validating a portable electronic nose for lung cancer screening. J. Thoracic Oncol. 2018, 13, 676–681. [Google Scholar] [CrossRef] [PubMed]
- Herman-Saffar, O.; Boger, Z.; Libson, S.; Lieberman, D.; Gonen, R.; Zeiri, Y. Early non-invasive detection of breast cancer using exhaled breath and urine analysis. Comput. Biol. Med. 2018, 96, 227–232. [Google Scholar] [CrossRef] [PubMed]
- Kateb, B.; Ryan, M.A.; Homer, M.L.; Lara, L.M.; Yin, Y.; Higa, K.; Chen, M.Y. Sniffing out cancer using the JPL electronic nose: A pilot study of a novel approach to detection and differentiation of brain cancer. NeuroImage 2009, 47, T5–T9. [Google Scholar] [CrossRef] [PubMed]
- Pennazza, G.; Santonico, M.; Bartolazzi, A.; Martinelli; Paolesse, R.; Di Natale, C.; Bono, R.; Tamburrelli, V.; Cristin, S.; D’Amico, A. Melanoma volatile fingerprint with a gas sensor array: In vivo and in vitro study. Procedia Chem. 2009, 1, 995–998. [Google Scholar] [CrossRef]
- Bax, C.; Taverna, G.; Eusebio, L.; Sironi, S.; Grizzi, F.; Guazzoni, G.; Capelli, L. Innovative diagnostic methods for early prostate cancer detection through urine analysis: A review. Cancers 2018, 10. [Google Scholar] [CrossRef] [PubMed]
- Sujono, H.A.; Rivai, M.; Amin, M. Asthma identification using gas sensors and support vector machine. Telecommun. Comput. Electron. Control 2018, 16, 1468–1480. [Google Scholar] [CrossRef]
- Siyang, S.; Wongchoosuk, C.; Kerdcharoen, T. Diabetes diagnosis by direct measurement from urine odor using electronic nose. In Proceedings of the 5th 2012 Biomedical Engineering International Conference (BMEiCON), Ubon Ratchathani, Thailand, 5–7 December 2012. [Google Scholar] [CrossRef]
- Mohamed, E.I.; Linder, R.; Perri, G.; Di Daniele, N.; Pöppl, S.J.; De Aorenzo, L. Predicting type 2 diabetes using an electronic nose-based artificial neural network analysis. Diabetes Nutr. Metab. 2002, 15, 215–221. [Google Scholar] [PubMed]
- The International Diabetes Federation, Facts and Figures 2017. Available online: https://www.idf.org/aboutdiabetes/what-is-diabetes/facts-figures.html (accessed on 10 February 2018).
- Diabetes, UK. Diabetes Prevalence 2017 (November 2017). Available online: https://www.diabetes.org.uk/professionals/position-statements-reports/statistics/diabetes-prevalence-2017 (accessed on 24 January 2018).
- N.D.A. (NDA). National Diabetes Audit Complications and Mortality 2015–2016. 2017. Available online: https://digital.nhs.uk/catalogue/PUB30030 (accessed on 24 January 2018).
- Esfahani, S.; Sagar, N.M.; Kyrou, I.; Mozdiak, E.; O’Connell, N.; Nwokolo, C.; Bardhan, K.D.; Arasaradnam, R.P.; Covington, J.A. Variation in Gas and Volatile Compound Emissions from Human Urine as It Ages, Measured by an Electronic Nose. Biosensors 2016, 6. [Google Scholar] [CrossRef] [PubMed]
- Covington, J.A.; van der Schee, M.P.; Edge, A.S.L.; Boyle, B.; Savage, R.S.; Arasaradnam, R.P. The application of FAIMS gas analysis in medical diagnostics. Analyst 2015, 140, 6775–6781. [Google Scholar] [CrossRef] [PubMed]
- Covington, J.A.; Westenbrink, E.W.; Ouaret, N.; Harbord, R.; Bailey, C.; O’Connell, N.; Cullis, J.; Williams, N.; Nwokolo, C.U.; Bardhan, K.D.; et al. Application of a novel tool for diagnosing bile acid diarrhea. Sensors 2013, 13, 11899–11912. [Google Scholar] [CrossRef] [PubMed]
- Arasaradnam, R.P.; Ouaret, N.; Thomas, M.G.; Quraishi, N.; Heatherington, E.; Nwokolo, C.U.; Bardhan, K.D.; Covington, J.A. A novel tool for noninvasive diagnosis and tracking of patients with inflammatory bowel disease. Inflamm. Bowel Dis. 2013, 19, 999–1003. [Google Scholar] [CrossRef] [PubMed]
- Lin, H.; Yan, Y.; Zhao, T.; Peng, L.; Zou, H.; Li, J.; Yang, X.; Xiong, Y.; Wang, M.; Wu, H. Rapid discrimination of Apiaceae plants by electronic nose coupled with multivariate statistical analyses. J. Pharm. Biomed. Anal. 2013, 84, 1–4. [Google Scholar] [CrossRef] [PubMed]
- Kursa, M.B.; Rudnicki, W.R. Feature selection with the Boruta package. J. Stat. Softw. 2010, 36, 1–13. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Demographic Data | Diabetes | Control |
|---|---|---|
| Male (%) | 27 (39.1) | 43 (64.2) |
| Female (%) | 42 (60.9) | 24 (35.8) |
| Median age (year) | 57 | 53.5 |
| Mean alcohol (units/week) | 1.8 | 1.09 |
| Median BMI | 39.7 | 26.1 |
| Sensor No. | References | Description |
|---|---|---|
| S1 | LY2/LG | Oxidising gas |
| S2 | LY2/G | Ammonia, carbon monoxide |
| S3 | LY2/AA | Ethanol |
| S4 | LY2/GH | Ammonia/ Organic amines |
| S5 | LY2/gCTL | Hydrogen sulfide |
| S6 | LY2/gCT | Propane/Butane |
| S7 | T30/1 | Organic solvents |
| S8 | P10/1 | Hydrocarbons |
| S9 | P10/2 | Methane |
| S10 | P40/1 | Fluorine |
| S11 | T70/2 | Aromatic compounds |
| S12 | PA/2 | Ethanol, Ammonia/Organic amines |
| S13 | P30/1 | Polar compounds (Ethanol) |
| S14 | P40/2 | Heteroatom/Chloride/Aldehydes |
| S15 | P30/2 | Alcohol |
| S16 | T40/2 | Aldehydes |
| S17 | T40/1 | Chlorinated compounds |
| S18 | TA/2 | Air quality |
| Methods | AUC | Sensitivity | Specificity | PPV | NPV | p-Value |
|---|---|---|---|---|---|---|
| Sparse Logistic Regression | 0.89 (0.79–0.99) | 0.74 (0.51–0.9) | 0.88 (0.63–0.99) | 0.89 | 0.71 | 4.368 × 10−6 |
| Random Forest | 0.86 (0.74–0.98) | 0.78 (0.56–0.92) | 0.82 (0.56–0.96) | 0.86 | 0.74 | 6.690 × 10−5 |
| Gaussian Process | 0.88 (0.76–1) | 0.87 (0.66–0.97) | 0.82 (0.56–0.96) | 0.87 | 0.82 | 7.187 × 10−6 |
| Support Vector Machine | 0.88 (0.77–0.99) | 0.74 (0.51–0.9) | 0.94 (0.71–0.99) | 0.94 | 0.73 | 7.189 × 10−6 |
| Methods | AUC | Sensitivity | Specificity | PPV | NPV | p-Value |
|---|---|---|---|---|---|---|
| Sparse Logistic Regression | 0.9 (0.7–1) | 1 (0.75–1) | 0.9 (0.55–0.99) | 0.93 | 1 | 3.199 × 10−4 |
| Random Forest | 0.93 (0.79–1) | 1 (0.75–1) | 0.9 (0.55–0.98) | 0.93 | 1 | 1.419 × 10−4 |
| Gaussian Process | 0.94 (0.82–1) | 0.92 (0.64–1) | 1 (0.69–1) | 1 | 0.91 | 5.856 × 10−5 |
| Support Vector Machine | 0.9 (0.7–1) | 1 (0.75–1) | 0.9 (0.55–0.99) | 0.93 | 1 | 3.199 × 10−4 |
| Methods | AUC | Sensitivity | Specificity | PPV | NPV | p-Value |
|---|---|---|---|---|---|---|
| Sparse Logistic Regression | 0.89 (0.83–0.95) | 0.65 (0.53–0.76) | 0.98 (0.89–1) | 0.98 | 0.64 | 1.583 × 10−13 |
| Random Forest | 0.89 (0.84–0.95) | 0.69 (0.58–0.79) | 0.9 (0.77–0.97) | 0.91 | 0.65 | 1.088 × 10−13 |
| Gaussian Process | 0.85 (0.78–0.92) | 0.77 (0.66–0.86) | 0.85 (0.72–0.94) | 0.89 | 0.71 | 4.04 × 10−11 |
| Support Vector Machine | 0.78 (0.69–0.88) | 0.88 (0.78–0.94) | 0.69 (0.54–0.81) | 0.81 | 0.79 | 8.529 × 10−8 |
| Methods | AUC | Sensitivity | Specificity | PPV | NPV | p-Value |
|---|---|---|---|---|---|---|
| Sparse Logistic Regression | 0.99 (0.96–1) | 0.98 (0.89–1) | 0.97 (0.86–1) | 0.98 | 0.97 | 3.639 × 10−15 |
| Random Forest | 0.97 (0.94–1) | 0.98 (0.89–1) | 0.87 (0.72–0.96) | 0.91 | 0.97 | 4.317 × 10−14 |
| Gaussian Process | 0.94 (0.89–0.99) | 0.9 (0.78–0.97) | 0.89 (0.75–0.97) | 0.92 | 0.87 | 9.162 × 10−13 |
| Support Vector Machine | 0.94 (0.87–1) | 0.98 (0.89–1) | 0.89 (0.75–0.97) | 0.92 | 0.97 | 9.733 × 10−13 |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Esfahani, S.; Wicaksono, A.; Mozdiak, E.; Arasaradnam, R.P.; Covington, J.A. Non-Invasive Diagnosis of Diabetes by Volatile Organic Compounds in Urine Using FAIMS and Fox4000 Electronic Nose. Biosensors 2018, 8, 121. https://doi.org/10.3390/bios8040121
Esfahani S, Wicaksono A, Mozdiak E, Arasaradnam RP, Covington JA. Non-Invasive Diagnosis of Diabetes by Volatile Organic Compounds in Urine Using FAIMS and Fox4000 Electronic Nose. Biosensors. 2018; 8(4):121. https://doi.org/10.3390/bios8040121
Chicago/Turabian StyleEsfahani, Siavash, Alfian Wicaksono, Ella Mozdiak, Ramesh P. Arasaradnam, and James A. Covington. 2018. "Non-Invasive Diagnosis of Diabetes by Volatile Organic Compounds in Urine Using FAIMS and Fox4000 Electronic Nose" Biosensors 8, no. 4: 121. https://doi.org/10.3390/bios8040121
APA StyleEsfahani, S., Wicaksono, A., Mozdiak, E., Arasaradnam, R. P., & Covington, J. A. (2018). Non-Invasive Diagnosis of Diabetes by Volatile Organic Compounds in Urine Using FAIMS and Fox4000 Electronic Nose. Biosensors, 8(4), 121. https://doi.org/10.3390/bios8040121