Point-of-Care Diagnostic Test for Beta-Thalassemia


 ,
, 
Abstract
1. Introduction
2. Methods
2.1. Study Design and Oversight
2.2. Study Populations and Procedures
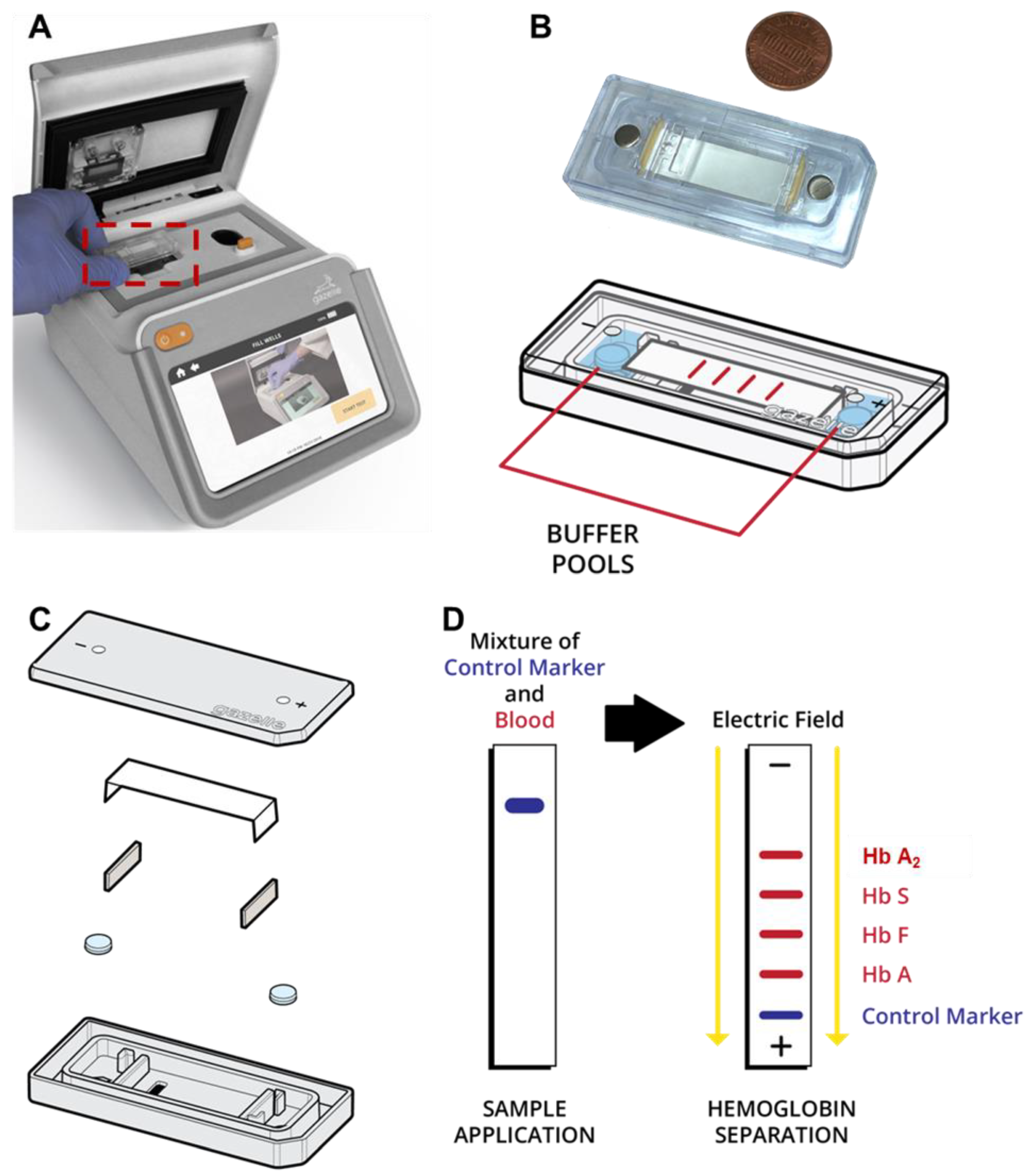
2.3. Gazelle Test Procedure
2.4. Confirmatory Laboratory Procedures
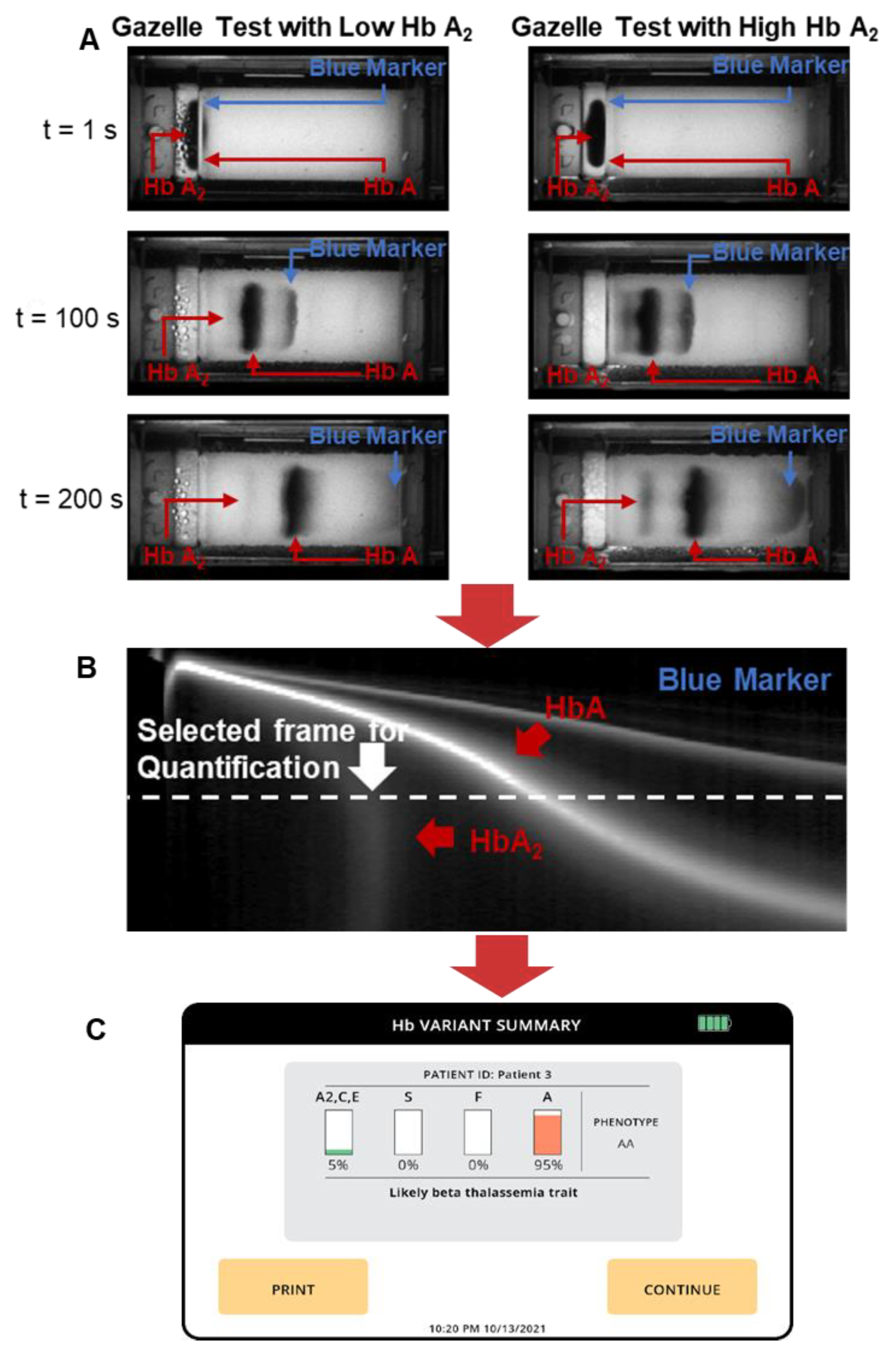
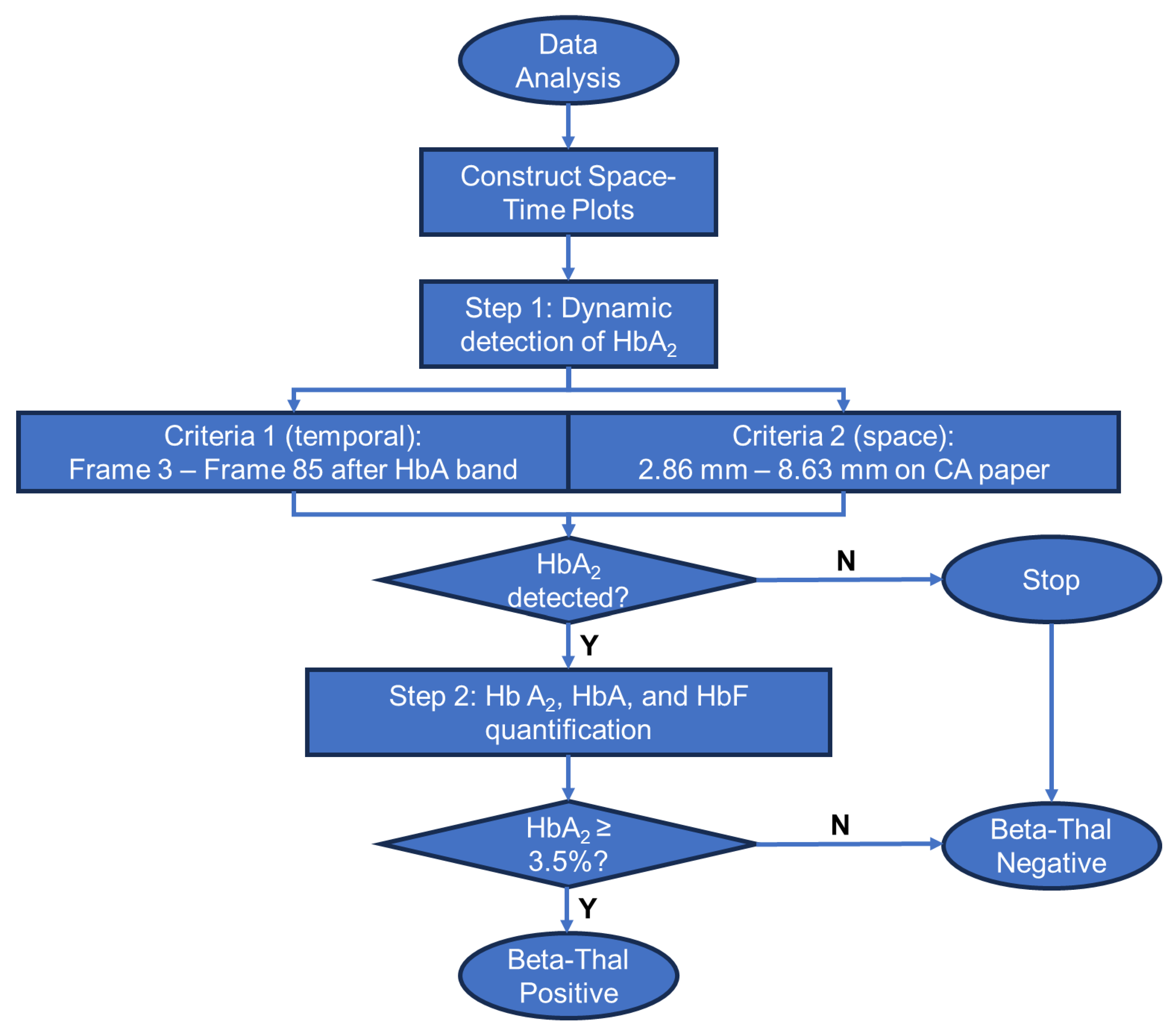
2.5. Gazelle-Multispectral Image Acquisition and Data Analysis
3. Results
3.1. Test Population and Result Reporting
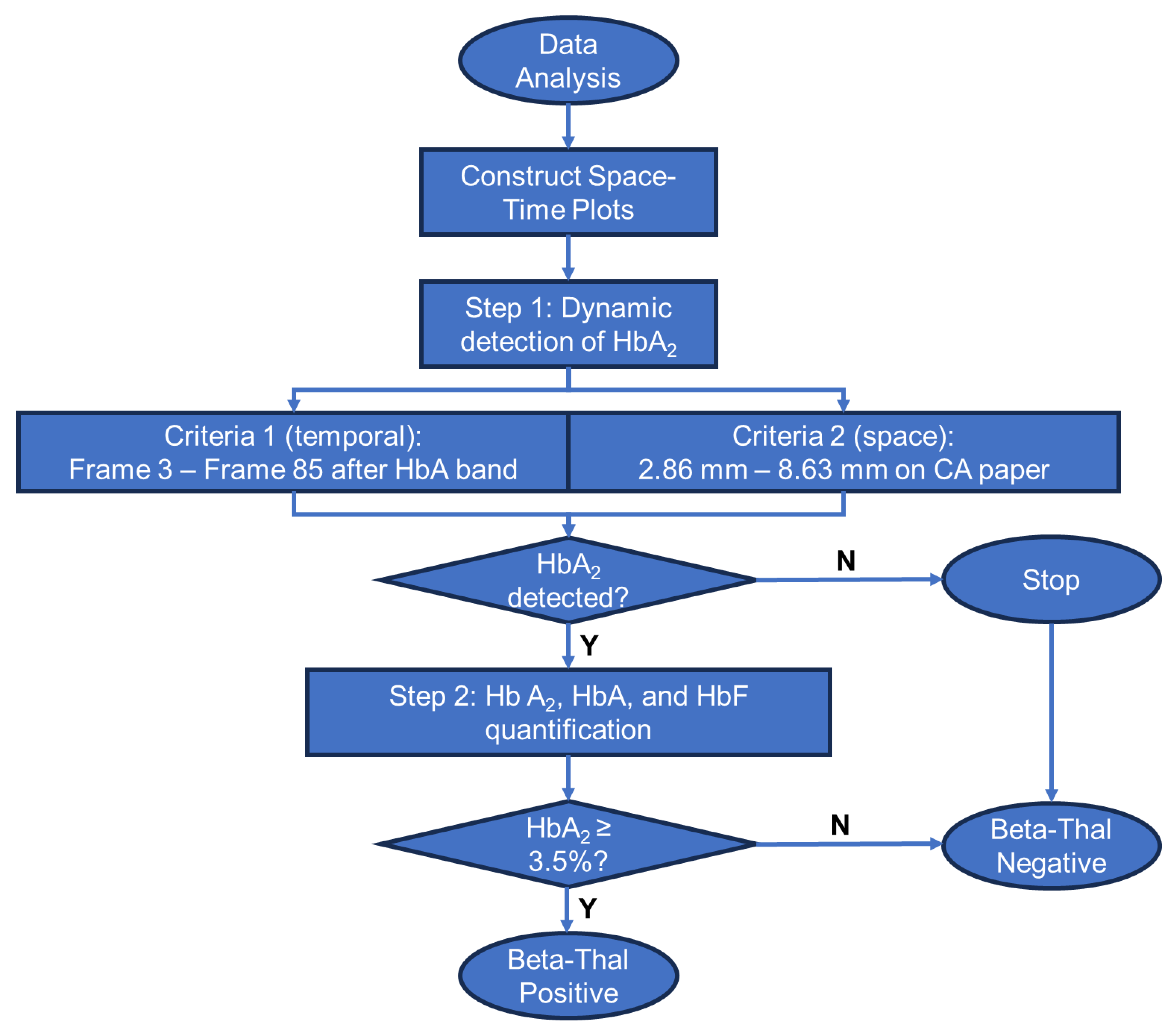
3.2. Gazelle Result Interpretation Criteria
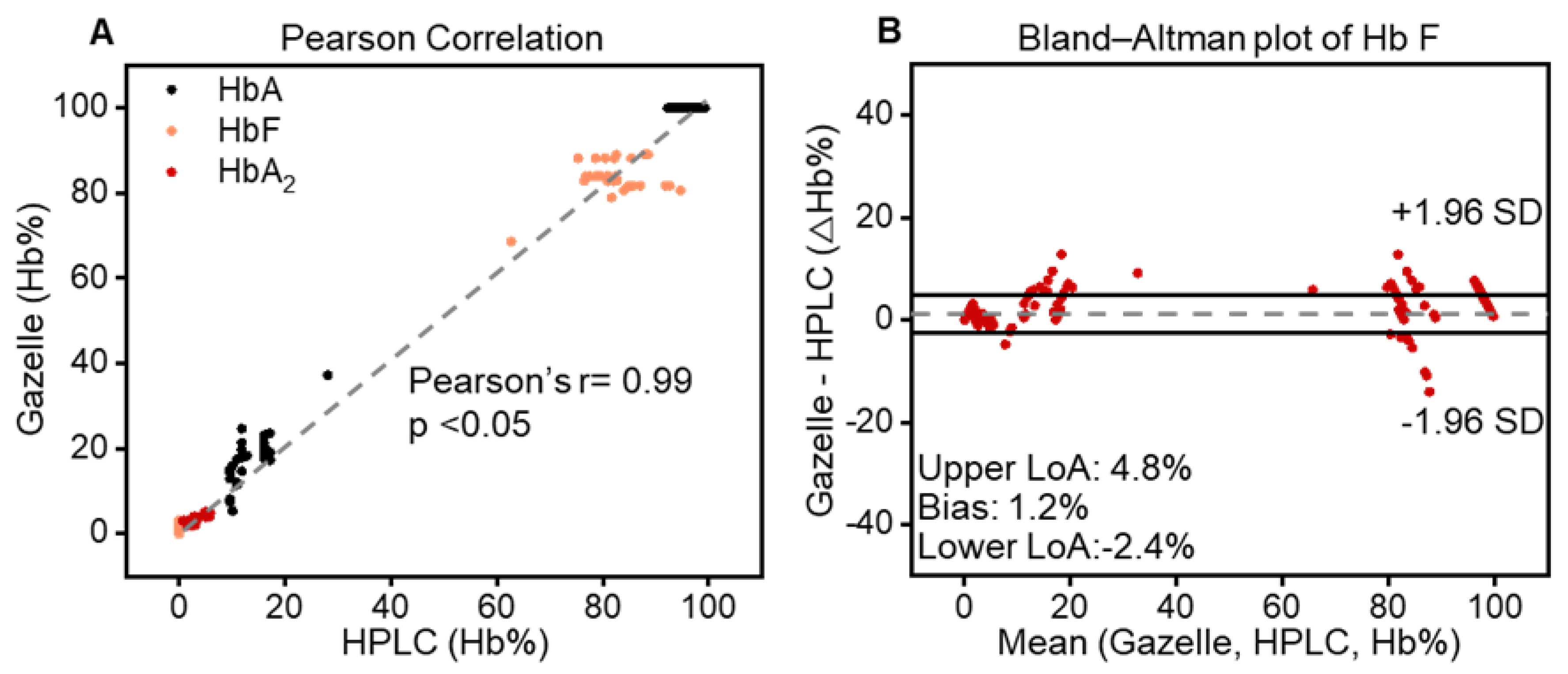
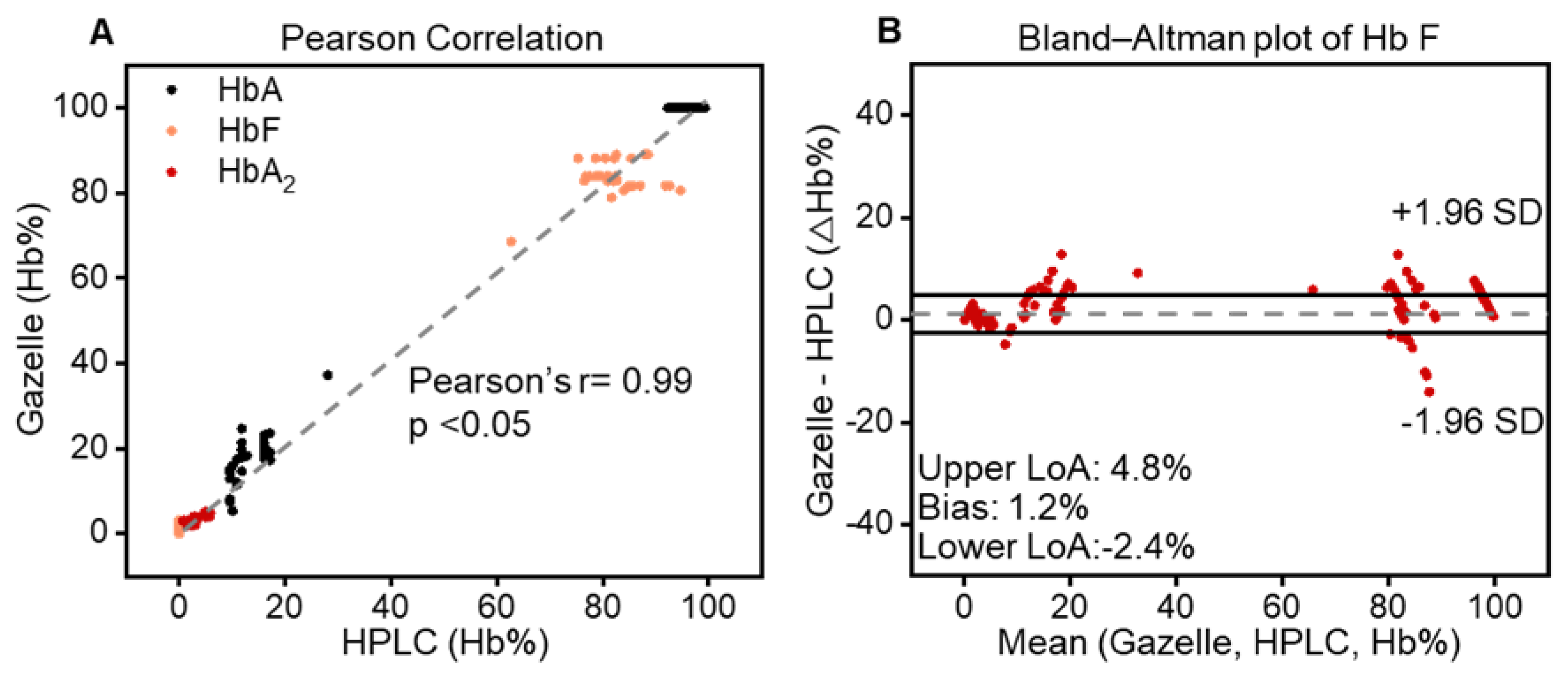
3.3. Gazelle-Multispectral Hb Variant Quantification Demonstrated a High Correlation with HPLC
3.4. Sensitivity and Specificity of Gazelle β-Thalassemia Testing
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- WHO. Newborn Health in the Western Pacific. 2022. Available online: https://www.who.int/westernpacific/health-topics/newborn-health (accessed on 11 January 2022).
- Taher, A.T.; Musallam, K.M.; Cappellini, M.D. β-Thalassemias. N. Engl. J. Med. 2021, 384, 727–743. [Google Scholar] [CrossRef]
- Modell, B.; Darlison, M. Global epidemiology of haemoglobin disorders and derived service indicators. Bull. World Health Organ. 2008, 86, 480–487. [Google Scholar] [CrossRef]
- Somervaille, T. Disorders of Hemoglobin: Genetics, Pathophysiology, and Clinical Management. J. R. Soc. Med. 2001, 94, 602–603. [Google Scholar] [CrossRef]
- Bender, M.A.; Hulihan, M.; Dorley, M.C.; del Pilar Aguinaga, M.; Ojodu, J.; Yusuf, C. Newborn Screening Practices for Beta-Thalassemia in the United States. Int. J. Neonatal Screen. 2021, 7, 83. [Google Scholar] [CrossRef]
- Cao, A. Carrier screening and genetic counselling in beta-thalassemia. Int. J. Hematol. 2002, 76 (Suppl. S2), 105–113. [Google Scholar] [CrossRef] [PubMed]
- Bhattacharya, S.; Thiyagarajan, A.; Sharma, N.; Srivastava, A.; Dhar, D.K. Need for a universal thalassemia screening programme in India? A public health perspective. J. Fam. Med. Prim. Care 2019, 8, 1528–1532. [Google Scholar]
- Taher, A.T.; Bou-Fakhredin, R.; Kattamis, A.; Viprakasit, V.; Cappellini, M.D. Improving outcomes and quality of life for patients with transfusion-dependent β-thalassemia: Recommendations for best clinical practice and the use of novel treatment strategies. Expert Rev. Hematol. 2021, 14, 897–909. [Google Scholar] [CrossRef] [PubMed]
- Arif, F.; Fayyaz, J.; Hamid, A. Awareness among parents of children with thalassemia major. J. Pak. Med. Assoc. 2008, 58, 621–624. [Google Scholar] [PubMed]
- Kattamis, A.; Forni, G.L.; Aydinok, Y.; Viprakasit, V. Changing patterns in the epidemiology of β-thalassemia. Eur. J. Haematol. 2020, 105, 692–703. [Google Scholar] [CrossRef] [PubMed]
- Danjou, F.; Anni, F.; Galanello, R. Beta-thalassemia: From genotype to phenotype. Haematologica 2011, 96, 1573–1575. [Google Scholar] [CrossRef] [PubMed]
- Origa, R. Beta-Thalassemia; University of Washington: Seattle, WA, USA, 1993. [Google Scholar]
- Origa, R. β-Thalassemia. Genet. Med. 2017, 19, 609–619. [Google Scholar] [CrossRef]
- Rund, D.; Rachmilewitz, E. Beta-thalassemia. N. Engl. J. Med. 2005, 353, 1135–1146. [Google Scholar] [CrossRef] [PubMed]
- Kawooya, I.; Kayongo, E.; Munube, D.; Mijumbi-Deve, R.; Elliott, S.; Vandermeer, B.; Sewankambo, N. Point-of-care diagnostic tests for sickle cell disease. Cochrane Database Syst. Rev. 2022, 2022, CD014584. [Google Scholar] [CrossRef]
- Clemente, F.; Antonacci, A.; Giardi, M.T.; Frisulli, V.; Tambaro, F.P.; Scognamiglio, V. Last Trends in Point-of-Care (POC) Diagnostics for the Management of Hematological Indices in Home Care Patients. Biosensors 2023, 13, 345. [Google Scholar] [CrossRef] [PubMed]
- Bond, M.; Hunt, B.; Flynn, B.; Huhtinen, P.; Ware, R.; Richards-Kortum, R. Towards a point-of-care strip test to diagnose sickle cell anemia. PLoS ONE 2017, 12, e0177732. [Google Scholar] [CrossRef] [PubMed]
- McGann, P.T.; Hoppe, C. The pressing need for point-of-care diagnostics for sickle cell disease: A review of current and future technologies. Blood Cells Mol. Dis. 2017, 67, 104–113. [Google Scholar] [CrossRef] [PubMed]
- Arishi, W.A.; Alhadrami, H.A.; Zourob, M. Techniques for the Detection of Sickle Cell Disease: A Review. Micromachines 2021, 12, 519. [Google Scholar] [CrossRef]
- Ilyas, S.; Simonson, A.E.; Asghar, W. Emerging point-of-care technologies for sickle cell disease diagnostics. Clin. Chim. Acta 2020, 501, 85–91. [Google Scholar] [CrossRef] [PubMed]
- Jaja, C.; Edem-Hotah, J.; Shepherd, J.; Patel, N.; Xu, H.; Gibson, R.W. Analytic Characteristics and Performance of Novel Immunoassay Point-of-Care Tests for Early Diagnosis of Sickle Cell Disease a Systematic Review. Point Care 2020, 19, 84–94. [Google Scholar] [CrossRef]
- Canning, D.M.; Huntsman, R.G. An assessment of Sickledex as an alternative to the sickling test. J. Clin. Pathol. 1970, 23, 736–737. [Google Scholar] [CrossRef]
- Steele, C.; Sinski, A.; Asibey, J.; Hardy-Dessources, M.D.; Elana, G.; Brennan, C. Point-of-care screening for sickle cell disease in low-resource settings: A multi-center evaluation of HemoTypeSC, a novel rapid test. Am. J. Hematol. 2019, 94, 39–45. [Google Scholar] [CrossRef] [PubMed]
- Kanter, J.; Telen, M.J.; Hoppe, C.; Roberts, C.L.; Kim, J.S.; Yang, X. Validation of a novel point of care testing device for sickle cell disease. BMC Med. 2015, 13, 225. [Google Scholar] [CrossRef] [PubMed]
- WHO World Health Organization. First WHO Model List of Essential In Vitro Diagnostics; WHO Technical Report Series, No. 1017; WHO: Geneva, Switzerland, 2019. [Google Scholar]
- An, R.; Huang, Y.; Man, Y.; Valentine, R.W.; Kucukal, E.; Goreke, U.; Sekyonda, Z.; Piccone, C.; Owusu-Ansah, A.; Ahuja, S.; et al. Emerging point-of-care technologies for anemia detection. Lab A Chip 2021, 21, 1843–1865. [Google Scholar] [CrossRef] [PubMed]
- WHO. Second WHO Model List of Essential In Vitro Diagnostics; WHO/MVP/EMP/2019.05; WHO: Geneva, Switzerland, 2019. [Google Scholar]
- Qua, K.; Swiatkowski, S.M.; Gurkan, U.A.; Pelfrey, C.M. A retrospective case study of successful translational research: Gazelle Hb variant point-of-care diagnostic device for sickle cell disease. J. Clin. Transl. Sci. 2021, 5, e207. [Google Scholar] [CrossRef] [PubMed]
- An, R.; Hasan, M.N.; Man, Y.; Gurkan, U.A. Integrated Point-of-Care Device for Anemia Detection and Hemoglobin Variant Identification. In Proceedings of the 2019 IEEE Healthcare Innovations and Point of Care Technologies, (HI-POCT), Bethesda, ML, USA, 20–22 November 2019. [Google Scholar]
- Hasan, M.N.; Fraiwan, A.; An, R.; Alapan, Y.; Ung, R.; Akkus, A.; Xu, J.Z.; Rezac, A.J.; Kocmich, N.J.; Creary, M.S.; et al. Paper-based microchip electrophoresis for point-of-care hemoglobin testing. Analyst 2020, 145, 2525–2542. [Google Scholar] [CrossRef]
- Hasan, M.N.; An, R.; Akkus, A.; Akkaynak, D.; Minerick, A.R.; Kharangate, C.R.; Gurkan, U.A. Dynamic pH and Thermal Analysis of Paper-Based Microchip Electrophoresis. Micromachines 2021, 12, 1433. [Google Scholar] [CrossRef]
- An, R.; Huang, Y.; Rocheleau, A.; Avanaki, A.; Thota, P.; Zhang, Q.; Man, Y.; Sekyonda, Z.; Segbefia, C.I.; Dei-Adomakoh, Y.; et al. Multispectral imaging for MicroChip electrophoresis enables point-of-care newborn hemoglobin variant screening. Heliyon 2022, 8, e11778. [Google Scholar] [CrossRef]
- Centers for Disease Control and Prevention. Hemoglobinopathies: Current Practices for Screening, Confirmation and Follow-Up; Association of Public Health Laboratories: Silver Spring, MD, USA, 2015.
- An, R.; Man, Y.; Iram, S.; Kucukal, E.; Hasan, M.N.; Huang, Y.; Goreke, U.; Bode, A.; Hill, A.; Cheng, K.; et al. Point-of-care microchip electrophoresis for integrated anemia and hemoglobin variant testing. Lab A Chip 2021, 21, 3863–3875. [Google Scholar] [CrossRef]
- Shinkins, B.; Thompson, M.; Mallett, S.; Perera, R. Diagnostic accuracy studies: How to report and analyse inconclusive test results. BMJ Br. Med. J. 2013, 346, f2778. [Google Scholar] [CrossRef]
- Bossuyt, P.M.; Reitsma, J.B.; E Bruns, D.; A Gatsonis, C.; Glasziou, P.P.; Irwig, L.; Lijmer, J.G.; Moher, D.; Rennie, D.; de Vet, H.C.; et al. STARD 2015: An Updated List of Essential Items for Reporting Diagnostic Accuracy Studies. Clin. Chem. 2015, 61, 1446–1452. [Google Scholar] [CrossRef]
- Ryan, K.; Bain, B.J.; Worthington, D.; James, J.; Plews, D.; Mason, A.; Roper, D.; Rees, D.C.; De La Salle, B.; Streetly, A.; et al. Significant haemoglobinopathies: Guidelines for screening and diagnosis. Br. J. Haematol. 2010, 149, 35–49. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Disease vs. Normal Normal | Disease vs. Trait | Trait vs. Normal | |
|---|---|---|---|
| True positive, TP | 32 | 32 | 18 |
| True negative, TN | 344 | 18 | 338 |
| False Positive, FP | 0 | 0 | 6 b |
| False negative, FN | 0 | 0 | 0 |
| Sensitivity, TP/(TP + FN) | 100.0% | 100.0% | 100% |
| Specificity, TN/(TN + FP) | 100.0% | 100.0% | 98.3% |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
An, R.; Avanaki, A.; Thota, P.; Nemade, S.; Mehta, A.; Gurkan, U.A. Point-of-Care Diagnostic Test for Beta-Thalassemia. Biosensors 2024, 14, 83. https://doi.org/10.3390/bios14020083
An R, Avanaki A, Thota P, Nemade S, Mehta A, Gurkan UA. Point-of-Care Diagnostic Test for Beta-Thalassemia. Biosensors. 2024; 14(2):83. https://doi.org/10.3390/bios14020083
Chicago/Turabian StyleAn, Ran, Alireza Avanaki, Priyaleela Thota, Sai Nemade, Amrish Mehta, and Umut A. Gurkan. 2024. "Point-of-Care Diagnostic Test for Beta-Thalassemia" Biosensors 14, no. 2: 83. https://doi.org/10.3390/bios14020083
APA StyleAn, R., Avanaki, A., Thota, P., Nemade, S., Mehta, A., & Gurkan, U. A. (2024). Point-of-Care Diagnostic Test for Beta-Thalassemia. Biosensors, 14(2), 83. https://doi.org/10.3390/bios14020083