A Flexible Ultrasound Array for Local Pulse Wave Velocity Monitoring

 ,
,  ,
, 
Abstract
:1. Introduction
2. Materials and Methods
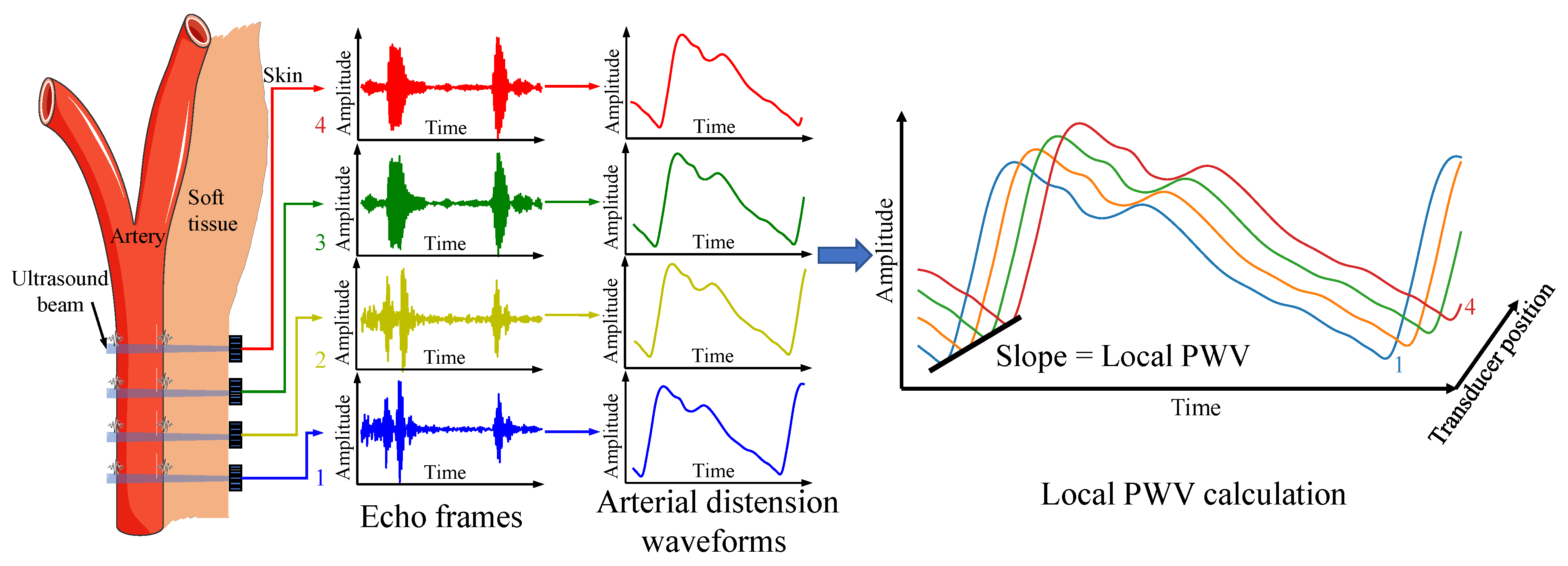
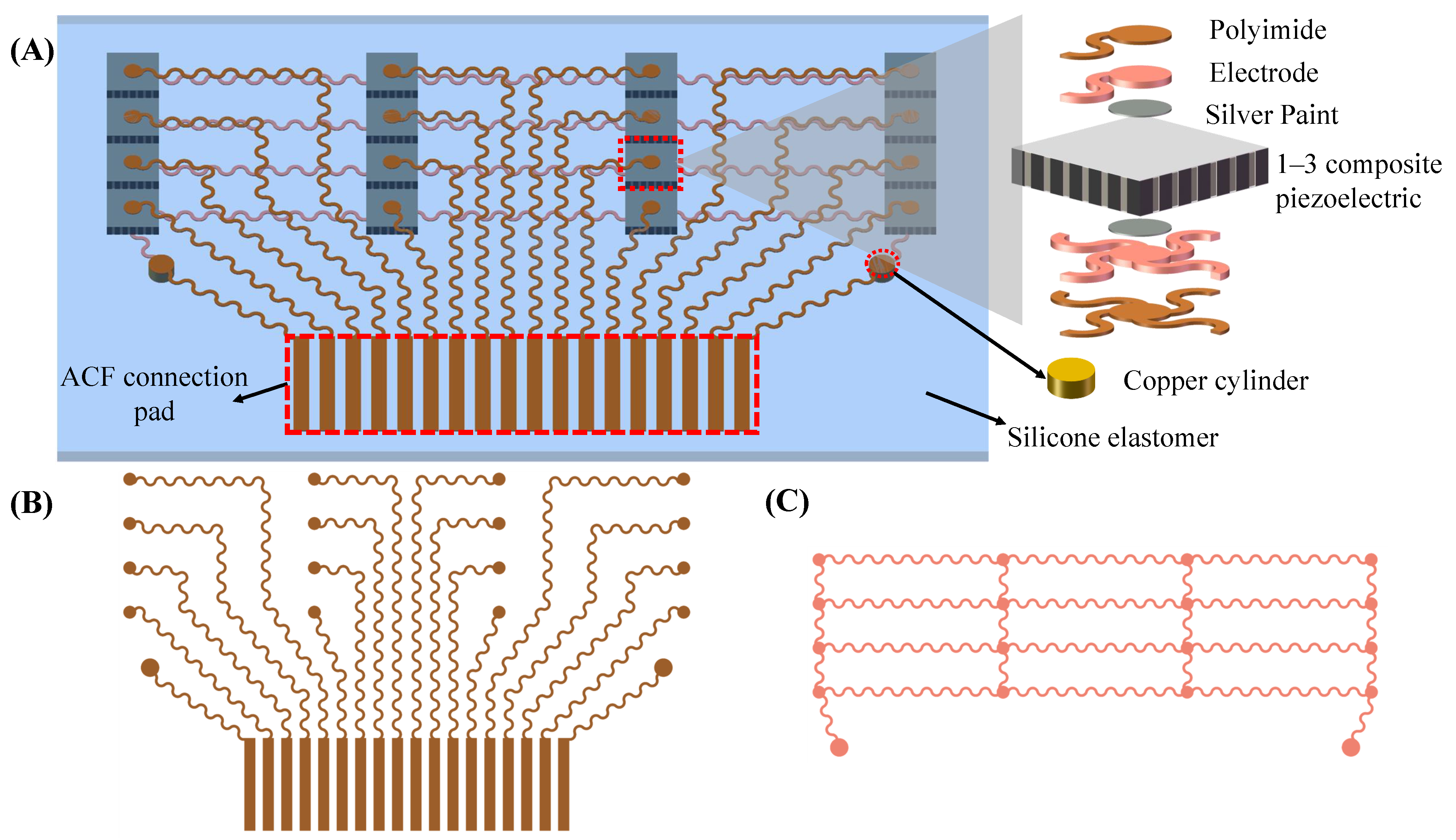
2.1. Measurement Principle and Device Design
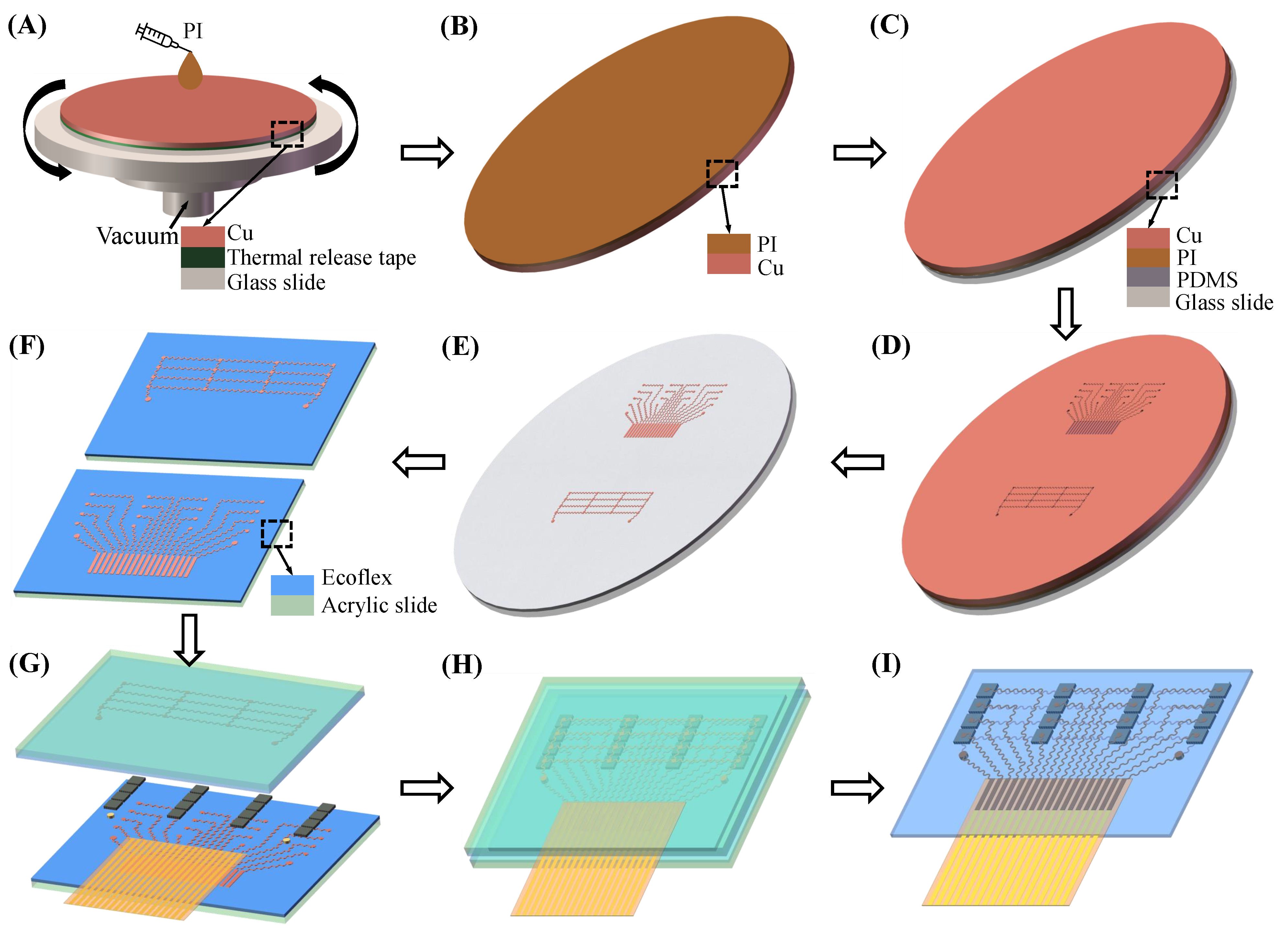
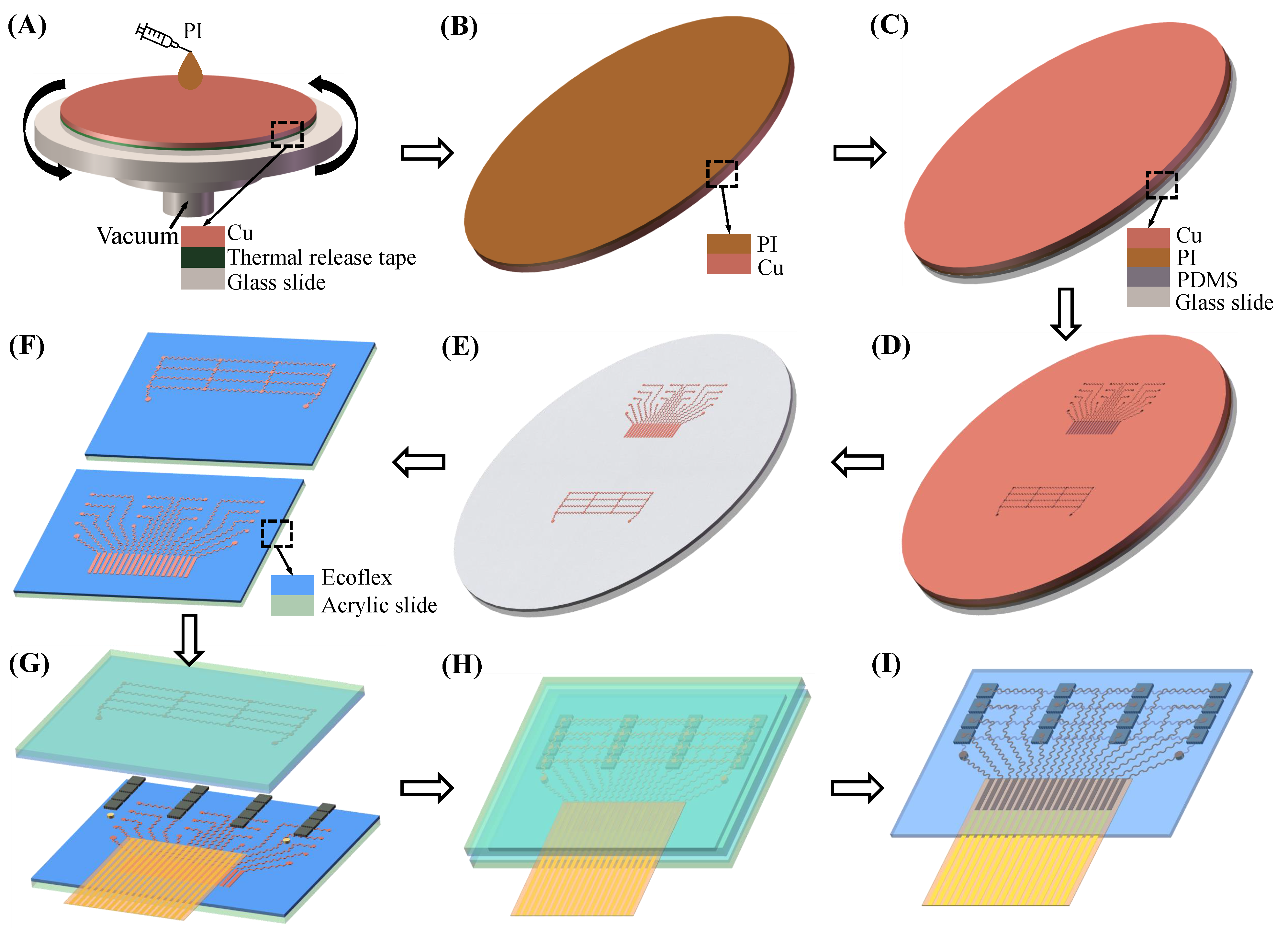
2.2. Fabrication of Flexible Ultrasound Array
2.2.1. Flexible and Stretchable Electrode Patterning
2.2.2. Integration and Packaging
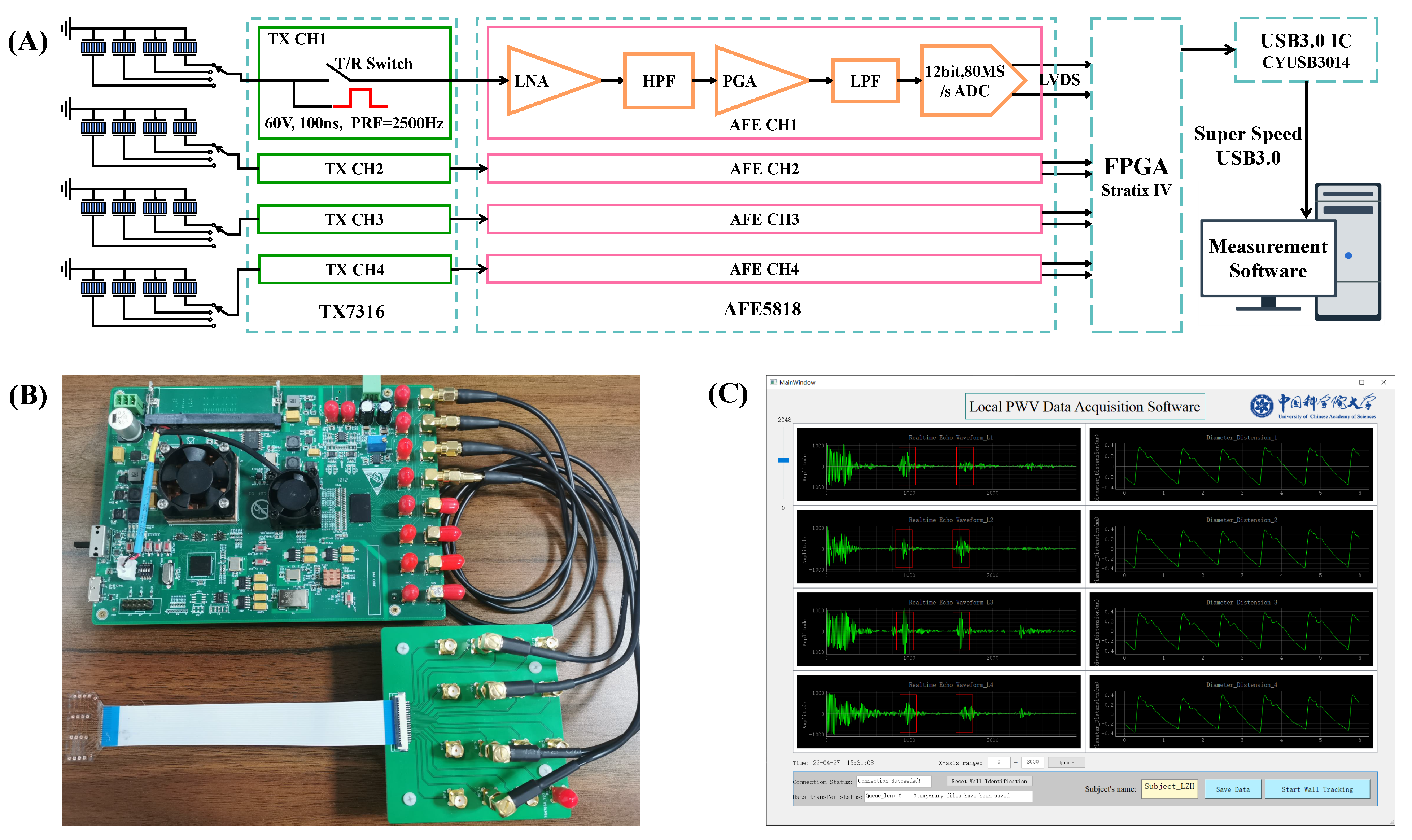
2.3. Data Acquisition Hardware
2.4. Measurement Software
2.5. In Vivo Experiments
3. Results and Discussions
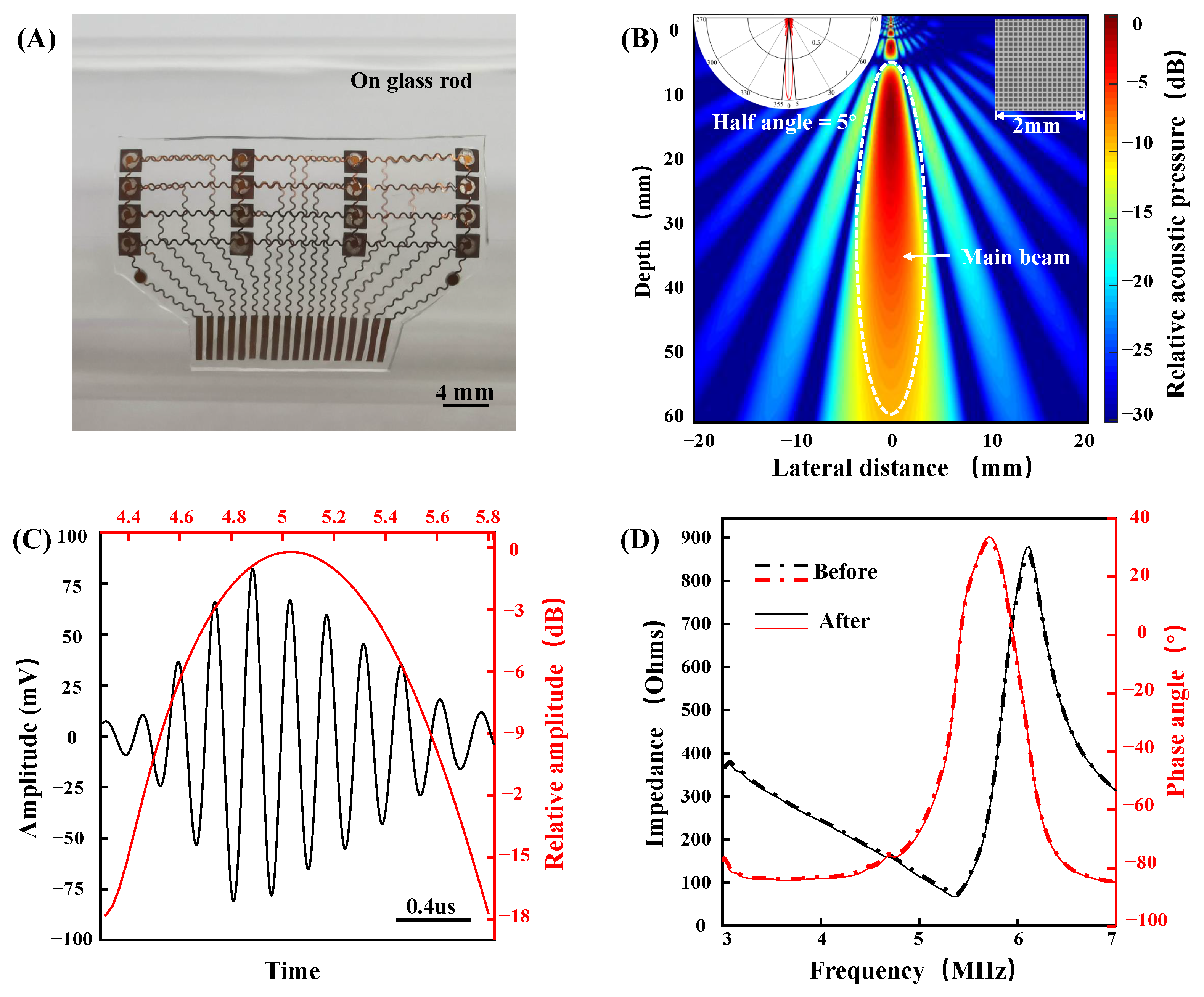
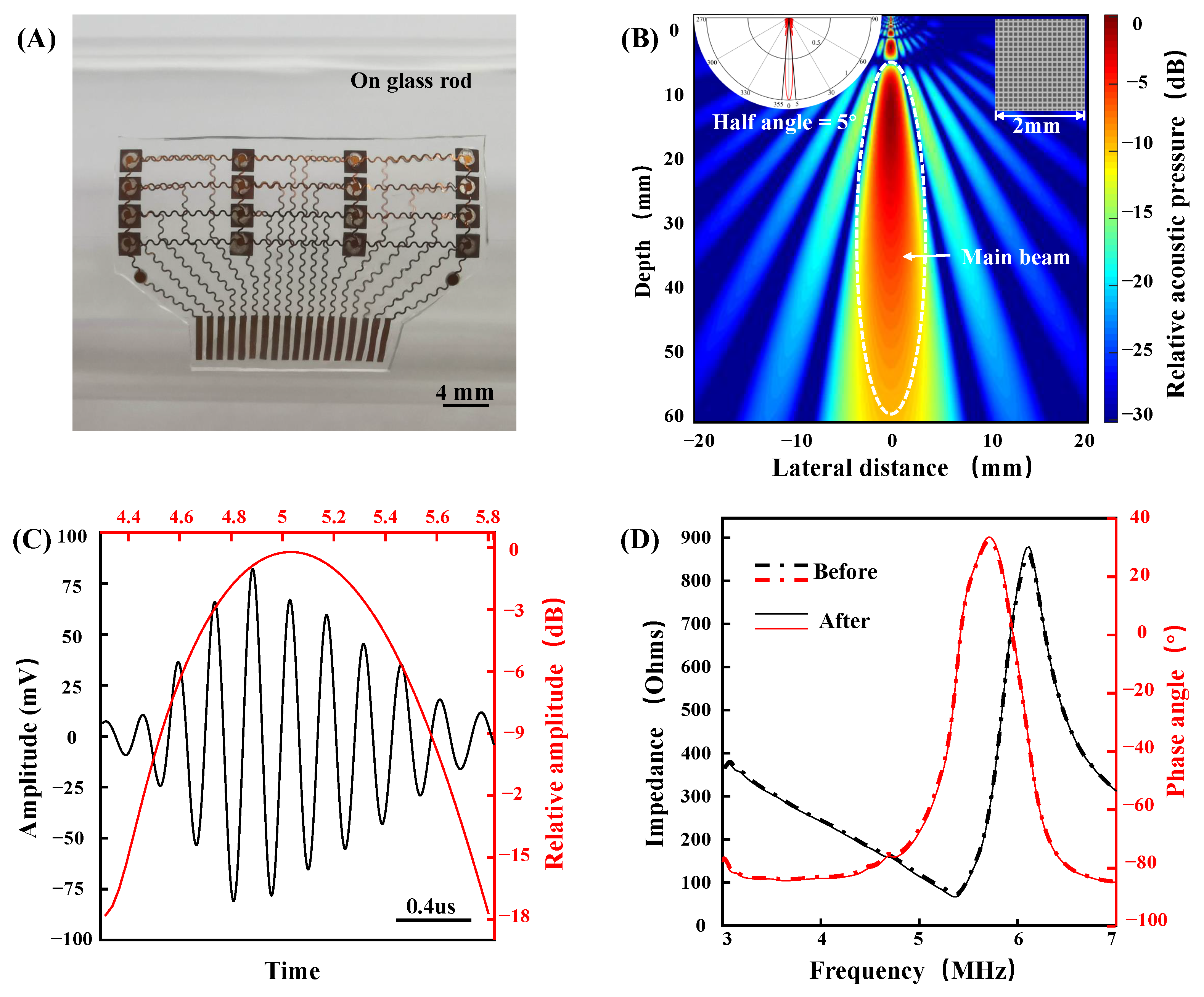
3.1. Device Characterization
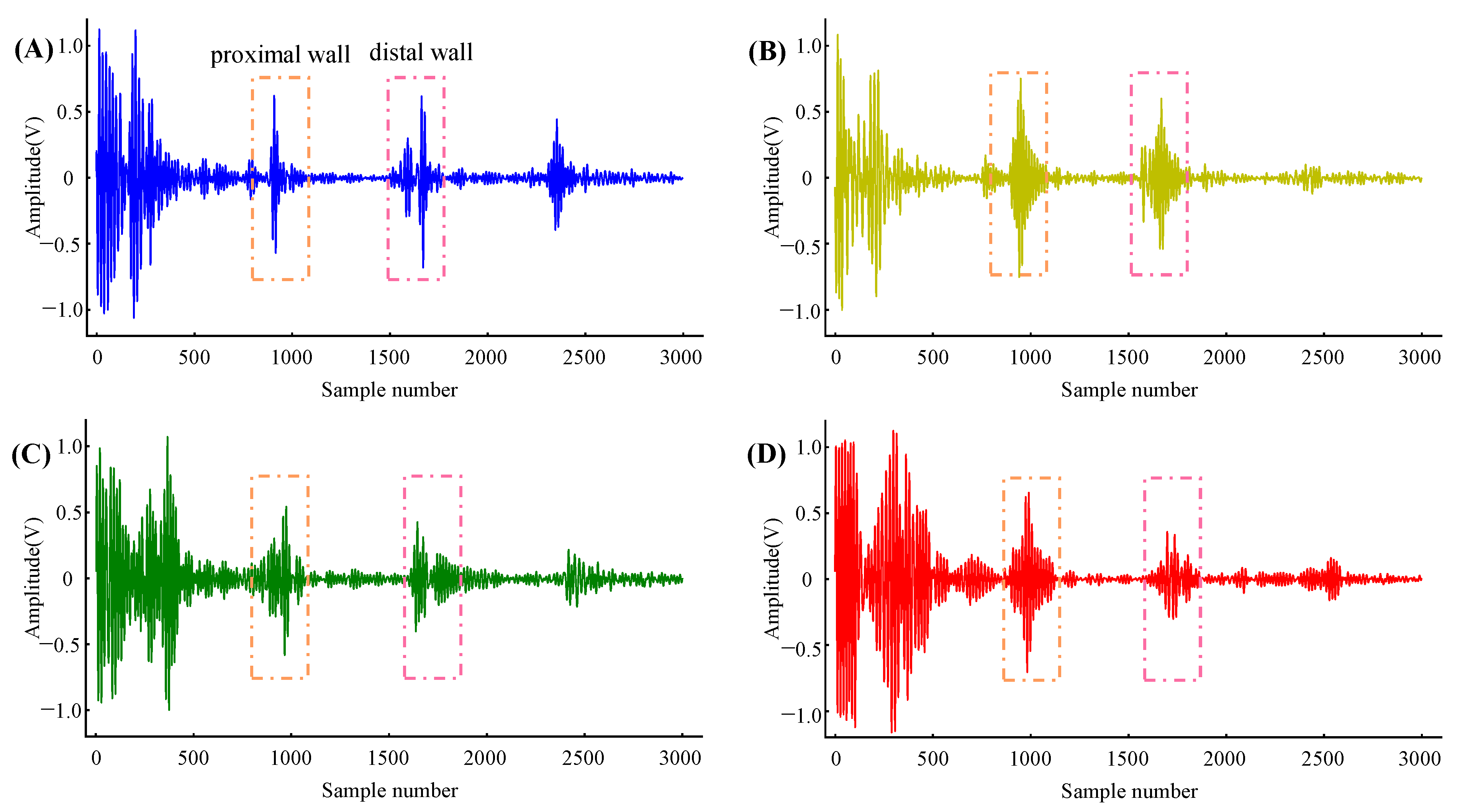
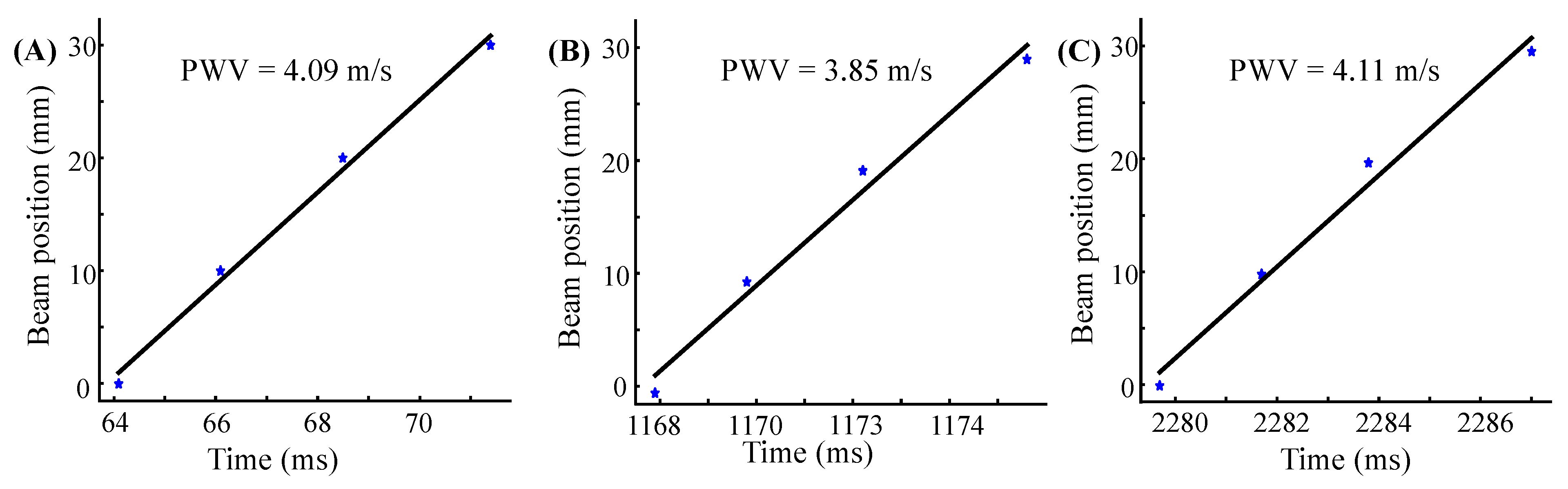
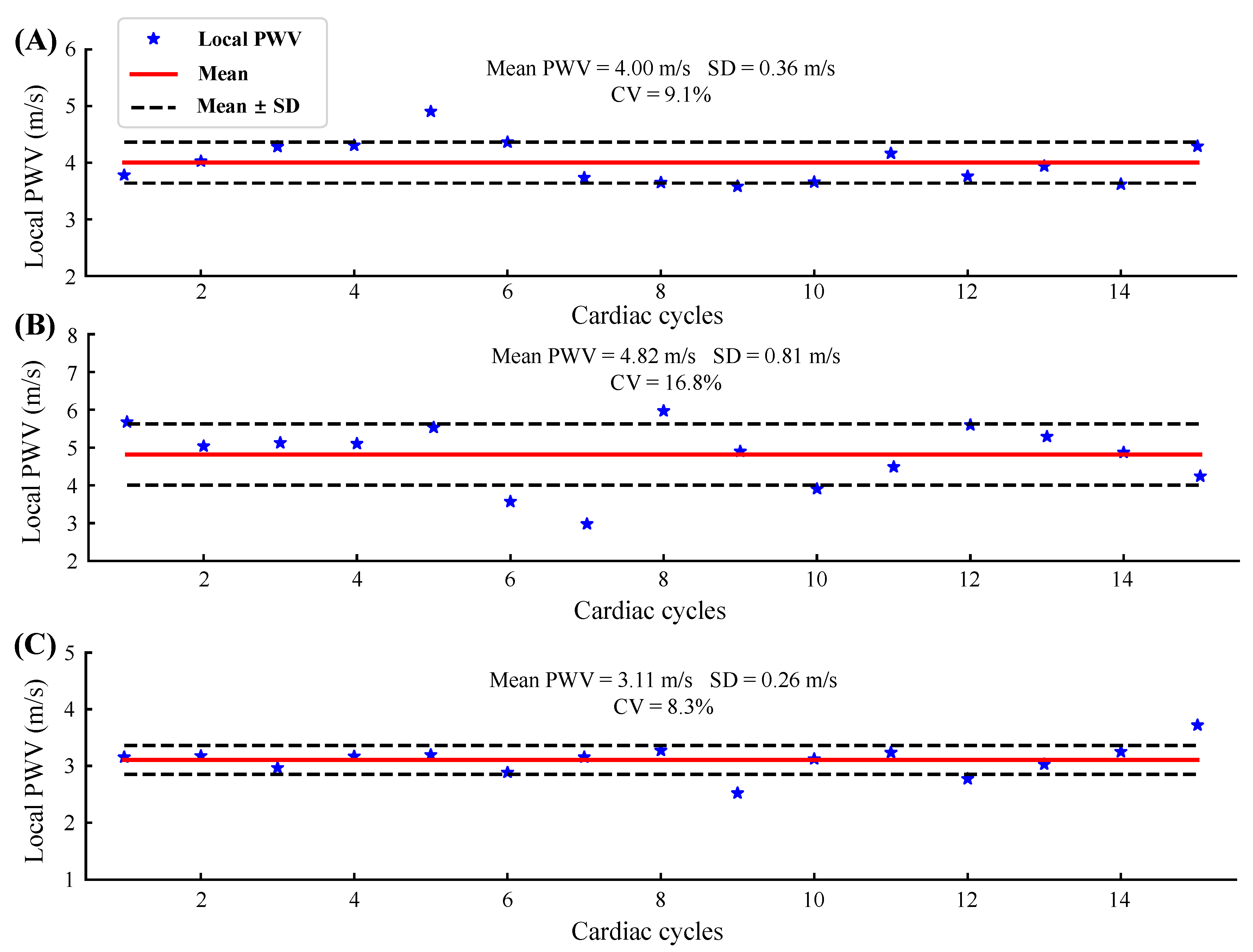
3.2. Device Performance of In Vivo Experiments
3.3. Study Limitations and Future Research Directions
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Nichols, W.W. Clinical measurement of arterial stiffness obtained from noninvasive pressure waveforms. Am. J. Hypertens. 2005, 18, 3s–10s. [Google Scholar] [CrossRef] [PubMed]
- Ben-Shlomo, Y.; Spears, M.; Boustred, C.; May, M.; Anderson, S.G.; Benjamin, E.J.; Boutouyrie, P.; Cameron, J.; Chen, C.-H.; Cruickshank, J.K.; et al. Aortic pulse wave velocity improves cardiovascular event prediction: An individual participant meta-analysis of prospective observational data from 17,635 subjects. J. Am. Coll. Cardiol. 2014, 63, 636–646. [Google Scholar] [CrossRef] [PubMed]
- Rajzer, M.W.; Wojciechowska, W.; Klocek, M.; Palka, I.; Brzozowska-Kiszka, M.; Kawecka-Jaszcz, K. Comparison of aortic pulse wave velocity measured by three techniques: Complior, SphygmoCor and Arteriograph. J. Hypertens. 2008, 26, 2001–2007. [Google Scholar] [CrossRef] [PubMed]
- Hirata, K.; Kawakami, M.; O’Rourke, M.F. Pulse Wave Analysis and Pulse Wave Velocity. Circ. J. 2006, 70, 1231–1239. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Boutouyrie, P.; Briet, M.; Collin, C.; Vermeersch, S.; Pannier, B. Assessment of pulse wave velocity. Artery Res. 2009, 3, 3–8. [Google Scholar] [CrossRef]
- Luo, J.; Fujikura, K.; Tyrie, L.S.; Tilson, M.D.; Konofagou, E.E. Pulse wave imaging of normal and aneurysmal abdominal aortas in vivo. IEEE Trans. Med. Imaging 2009, 28, 477–486. [Google Scholar] [CrossRef]
- Baguet, J.P.; Kingwell, B.A.; Dart, A.L.; Shaw, J.; Ferrier, K.E.; Jennings, G.L. Analysis of the regional pulse wave velocity by Doppler: Methodology and reproducibility. J. Hum. Hypertens. 2003, 17, 407–412. [Google Scholar] [CrossRef] [Green Version]
- Nabeel, P.M.; Karthik, S.; Joseph, J.; Sivaprakasam, M. Arterial Blood Pressure Estimation From Local Pulse Wave Velocity Using Dual-Element Photoplethysmograph Probe. IEEE Trans. Instrum. Meas. 2018, 67, 1399–1408. [Google Scholar] [CrossRef]
- Pereira, T.; Santos, I.; Oliveira, T. Characterization of Optical System for Hemodynamic Multi-Parameter Assessment. Cardiovasc. Eng. Technol. 2013, 4, 87–97. [Google Scholar] [CrossRef] [Green Version]
- Pereira, H.C.; Pereira, T.; Almeida, V.; Borges, E.; Figueiras, E.; Simões, J.B.; Malaquias, J.L.; Cardoso, J.M.; Correia, C.M. Characterization of a double probe for local pulse wave velocity assessment. Physiol. Meas. 2010, 31, 1449–1465. [Google Scholar] [CrossRef]
- Hsu, Y.; Young, D.J. Skin-Coupled Personal Wearable Ambulatory Pulse Wave Velocity Monitoring System Using Microelectromechanical Sensors. IEEE Sens. J. 2014, 14, 3490–3497. [Google Scholar] [CrossRef]
- Rachim, V.P.; Kang, S.; Baek, J.H.; Park, S.M. Unobtrusive, Cuffless Blood Pressure Monitoring Using a Soft Polymer Sensor Array With Flexible Hybrid Electronics. IEEE Sens. J. 2021, 21, 10132–10142. [Google Scholar] [CrossRef]
- Shu, Y.; Li, C.; Wang, Z.; Mi, W.; Li, Y.; Ren, T.-L. A Pressure Sensing System for Heart Rate Monitoring with Polymer-Based Pressure Sensors and An Anti-Interference Post Processing Circuit. Sensors 2015, 15, 3224–3235. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nabeel, P.M.; Joseph, J.; Sivaprakasam, M. Arterial compliance probe for local blood pulse wave velocity measurement. In Proceedings of the 2015 37th Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBC), Milan, Italy, 25–29 August 2015; pp. 5712–5715. [Google Scholar]
- Lee, W.H.; Rho, Y.H. Measurement of Cuffless Blood Pressure by Using a Magnetoplethysmogram Pulsimeter. Insights Blood Press. 2016, 2, 1–8. [Google Scholar]
- Lascio, N.D.; Bruno, R.M.; Stea, F.; Bianchini, E.; Gemignani, V.; Ghiadoni, L.; Faita, F. Non-invasive assessment of carotid PWV via accelerometric sensors: Validation of a new device and comparison with established techniques. Eur. J. Appl. Physiol. 2014, 114, 1503–1512. [Google Scholar] [CrossRef]
- Arathy, R.; Nabeel, P.M.; Joseph, J.; Sivaprakasam, M. Accelerometric patch probe for cuffless blood pressure evaluation from carotid local pulse wave velocity: Design, development, and in vivo experimental study. Biomed. Phys. Eng. Express 2019, 5, 45010. [Google Scholar] [CrossRef]
- Rabben, S.I.; Stergiopulos, N.; Hellevik, L.R.; Smiseth, O.A.; Slørdahl, S.; Urheim, S.; Angelsen, B. An ultrasound-based method for determining pulse wave velocity in superficial arteries. J. Biomech. 2004, 37, 1615–1622. [Google Scholar] [CrossRef]
- Segers, P.; Swillens, A.; Taelman, L.; Vierendeels, J. Wave reflection leads to over- and underestimation of local wave speed by the PU- and QA-loop methods: Theoretical basis and solution to the problem. Physiol. Meas. 2014, 35, 847–861. [Google Scholar] [CrossRef]
- Seo, J.; Pietrangelo, S.J.; Sodini, C.G.; Lee, H.S. Motion Tolerant Unfocused Imaging of Physiological Waveforms for Blood Pressure Waveform Estimation Using Ultrasound. IEEE Trans. Ultrason. Ferroelectr. Freq. Control. 2018, 65, 766–779. [Google Scholar] [CrossRef]
- Meinders, J.M.; Kornet, L.; Brands, P.J.; Hoeks, A.P. Assessment of local pulse wave velocity in arteries using 2D distension waveforms. Ultrason. Imaging 2001, 23, 199–215. [Google Scholar] [CrossRef]
- Deng, L.; Zhang, Y.; Chen, Z.; Zhao, Z.; Zhang, K.; Wu, J. Regional Upstroke Tracking for Transit Time Detection to Improve the Ultrasound-Based Local PWV Estimation in Carotid Arteries. IEEE Trans. Ultrason. Ferroelectr. Freq. Control 2020, 67, 691–702. [Google Scholar] [CrossRef] [PubMed]
- Eriksson, A.; Greiff, E.; Loupas, T.; Persson, M.; Pesque, P. Arterial pulse wave velocity with tissue doppler imaging. Ultrasound Med. Biol. 2002, 28, 571–580. [Google Scholar] [CrossRef]
- Wang, C.H.; Li, X.S.; Hu, H.J.; Zhang, L.; Huang, Z.L.; Lin, M.Y.; Zhang, Z.R.; Yin, Z.N.; Huang, B.; Gong, H.; et al. Monitoring of the central blood pressure waveform via a conformal ultrasonic device. Nat. Biomed. Eng. 2018, 2, 687–695. [Google Scholar] [CrossRef] [PubMed]
- Yang, Y.; Tian, H.; Yan, B.; Sun, H.; Wu, C.; Shu, Y.; Wang, L.-G.; Ren, T.-L. A flexible piezoelectric micromachined ultrasound transducer. RSC Adv. 2013, 3, 24900–24905. [Google Scholar] [CrossRef]
- Hu, H.J.; Zhu, X.; Wang, C.H.; Zhang, L.; Li, X.S.; Lee, S.; Huang, Z.L.; Chen, R.M.; Chen, Z.Y.; Wang, C.F.; et al. Stretchable ultrasonic transducer arrays for three-dimensional imaging on complex surfaces. Sci. Adv. 2018, 4, eaar3979. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sun, S.; Zhang, M.; Gao, C.; Liu, B.; Pang, W. Flexible piezoelectric micromachined ultrasonic transducers towards new applications. In Proceedings of the 2018 IEEE International Ultrasonics Symposium (IUS), Kobe, Japan, 22–25 October 2018; pp. 1–4. [Google Scholar]
- Wang, C.H.; Qi, B.Y.; Lin, M.Y.; Zhang, Z.R.; Makihata, M.; Liu, B.Y.; Zhou, S.; Huang, Y.H.; Hu, H.J.; Gu, Y.; et al. Continuous monitoring of deep-tissue haemodynamics with stretchable ultrasonic phased arrays. Nat. Biomed. Eng. 2021, 5, 749. [Google Scholar] [CrossRef]
- Wang, F.L.; Jin, P.; Feng, Y.L.; Fu, J.; Wang, P.; Liu, X.; Zhang, Y.C.; Ma, Y.J.; Yang, Y.Y.; Yang, A.M.; et al. Flexible Doppler ultrasound device for the monitoring of blood flow velocity. Sci. Adv. 2021, 7, ebi9283. [Google Scholar] [CrossRef]
- Smith, W.A.; Auld, B.A. Modeling 1–3 composite piezoelectrics: Thickness-mode oscillations. IEEE Trans. Ultrason. Ferroelectr. Freq. Control. 1991, 38, 40–47. [Google Scholar] [CrossRef]
- Brands, P.J.; Hoeks, A.P.G.; Ledoux, L.A.F.; Reneman, R.S. A radio frequency domain complex cross-correlation model to estimate blood flow velocity and tissue motion by means of ultrasound. Ultrasound Med. Biol. 1997, 23, 911–920. [Google Scholar] [CrossRef]
- Sahani, A.K.; Joseph, J.; Sivaprakasam, M. Evaluation of the algorithm for automatic identification of the common carotid artery in ARTSENS. Physiol. Meas. 2014, 35, 1299–1317. [Google Scholar] [CrossRef]
- Mukkamala, R.; Hahn, J.O.; Inan, O.T.; Mestha, L.K.; Kim, C.S.; Toreyin, H.; Kyal, S. Toward Ubiquitous Blood Pressure Monitoring via Pulse Transit Time: Theory and Practice. IEEE Trans. Biomed. Eng. 2015, 62, 1879–1901. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Luo, J.; Li, R.X.; Konofagou, E.E. Pulse wave imaging of the human carotid artery: An in vivo feasibility study. IEEE Trans. Ultrason. Ferroelectr. Freq. Control. 2012, 59, 174–181. [Google Scholar] [CrossRef] [PubMed]
- Kiran, V.R.; Nabeel, P.M.; Joseph, J. Image-Free Fast Ultrasound for Measurement of Local Pulse Wave Velocity: In vitro Validation and In vivo Feasibility. IEEE Trans. Ultrason. Ferroelectr. Freq. Control. 2022. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Subject ID | Age (Years) | Trial ID | Elements Used | Mean ± SD ( m/s) | CV | |
|---|---|---|---|---|---|---|
| Column Numbers | Row Numbers | |||||
| S1 | 26 | 1 | 1, 2, 3, 4 | 2 | 4.00 ± 0.36 | 9.1% |
| S2 | 24 | 1 | 2, 3, 4 | 2 | 3.07 ± 0.49 | 16.1% |
| S3 | 26 | 1 | 1, 2, 3, 4 | 2 | 4.43 ± 0.68 | 15.5% |
| 2 | 1, 2, 3, 4 | 3 | 4.11 ± 0.37 | 9.0% | ||
| S4 | 28 | 1 | 2, 3, 4 | 1 | 4.60 ± 0.60 | 13.0% |
| 2 | 1, 2, 3 | 2 | 4.82 ± 0.81 | 16.8% | ||
| S5 | 26 | 1 | 1, 2, 3, 4 | 3 | 3.23 ± 0.28 | 8.6% |
| 2 | 1, 2, 3, 4 | 3 | 3.11 ± 0.26 | 8.3% | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Xu, L.; Wang, P.; Xia, P.; Wu, P.; Chen, X.; Du, L.; Liu, J.; Xue, N.; Fang, Z. A Flexible Ultrasound Array for Local Pulse Wave Velocity Monitoring. Biosensors 2022, 12, 479. https://doi.org/10.3390/bios12070479
Xu L, Wang P, Xia P, Wu P, Chen X, Du L, Liu J, Xue N, Fang Z. A Flexible Ultrasound Array for Local Pulse Wave Velocity Monitoring. Biosensors. 2022; 12(7):479. https://doi.org/10.3390/bios12070479
Chicago/Turabian StyleXu, Lirui, Peng Wang, Pan Xia, Pang Wu, Xianxiang Chen, Lidong Du, Jiexin Liu, Ning Xue, and Zhen Fang. 2022. "A Flexible Ultrasound Array for Local Pulse Wave Velocity Monitoring" Biosensors 12, no. 7: 479. https://doi.org/10.3390/bios12070479
APA StyleXu, L., Wang, P., Xia, P., Wu, P., Chen, X., Du, L., Liu, J., Xue, N., & Fang, Z. (2022). A Flexible Ultrasound Array for Local Pulse Wave Velocity Monitoring. Biosensors, 12(7), 479. https://doi.org/10.3390/bios12070479