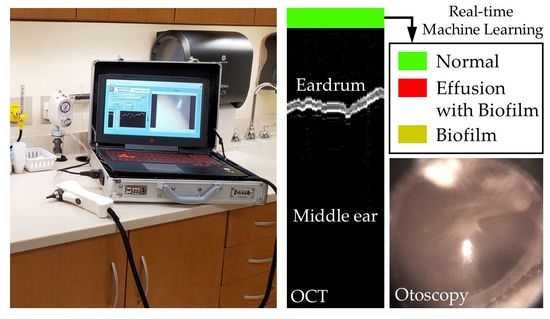
Handheld Briefcase Optical Coherence Tomography with Real-Time Machine Learning Classifier for Middle Ear Infections

 , , ,
, , ,
Abstract
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
1. Introduction
2. Materials and Methods
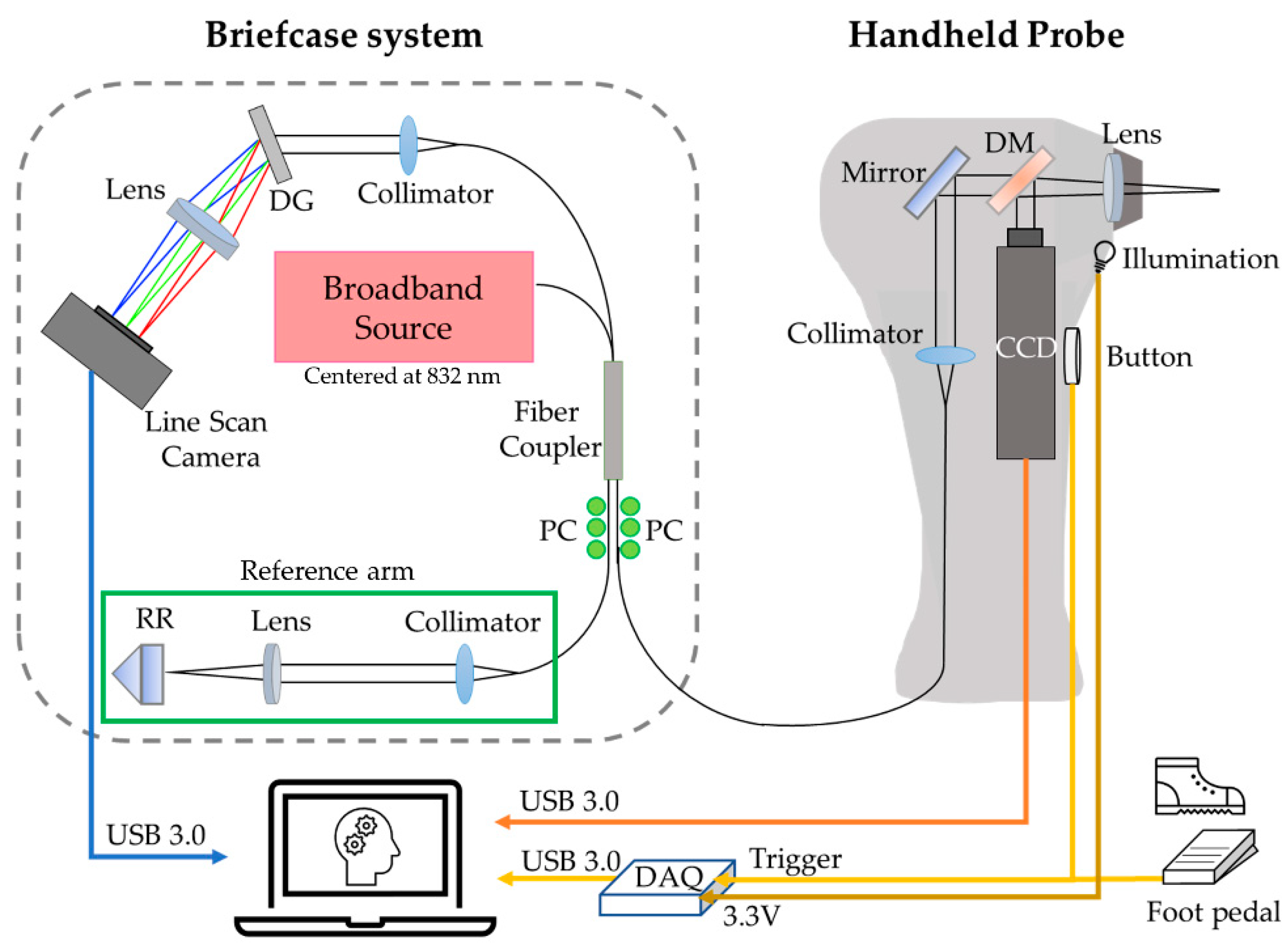
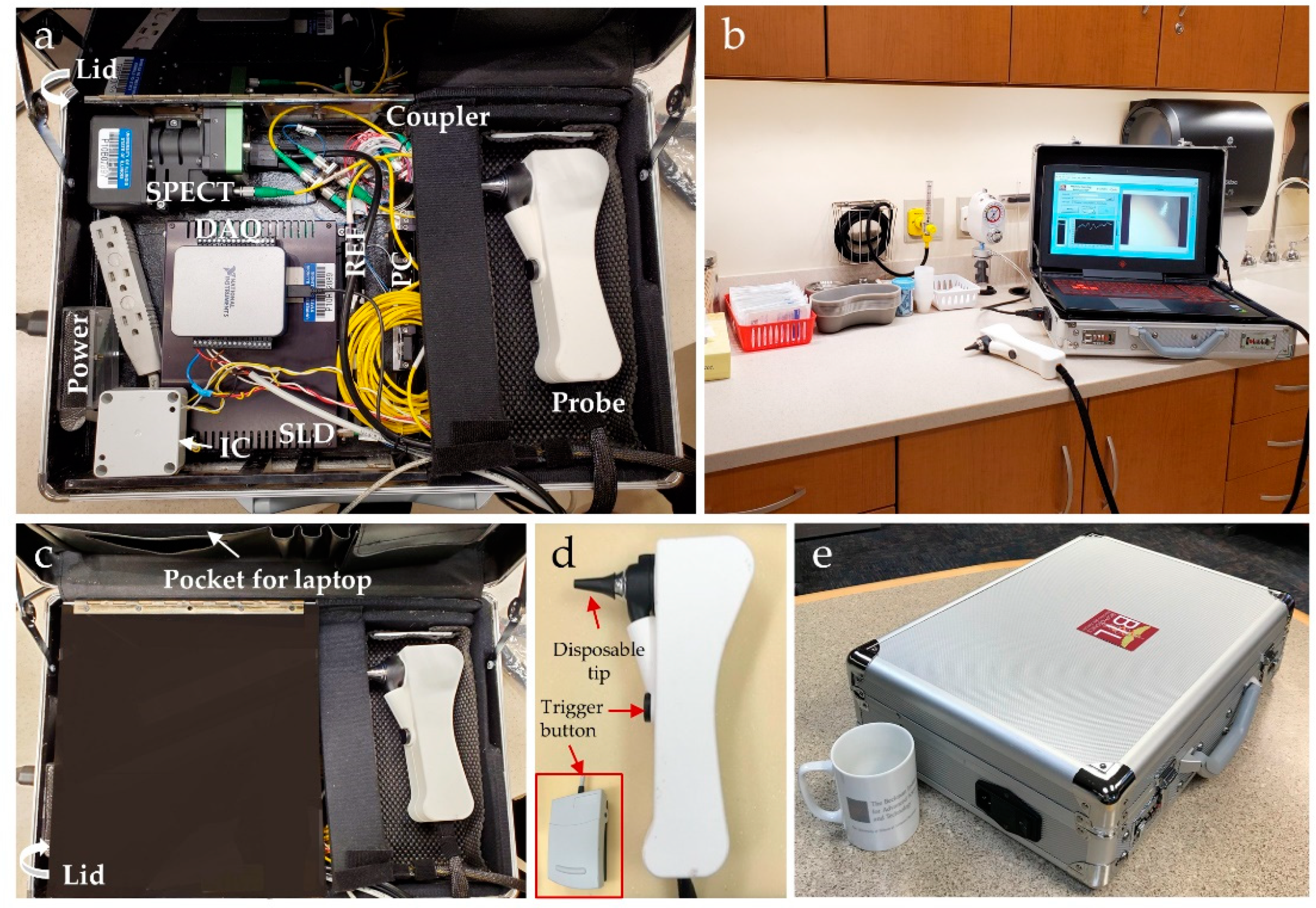
2.1. Development of Compact Briefcase System for Middle Ear Imaging
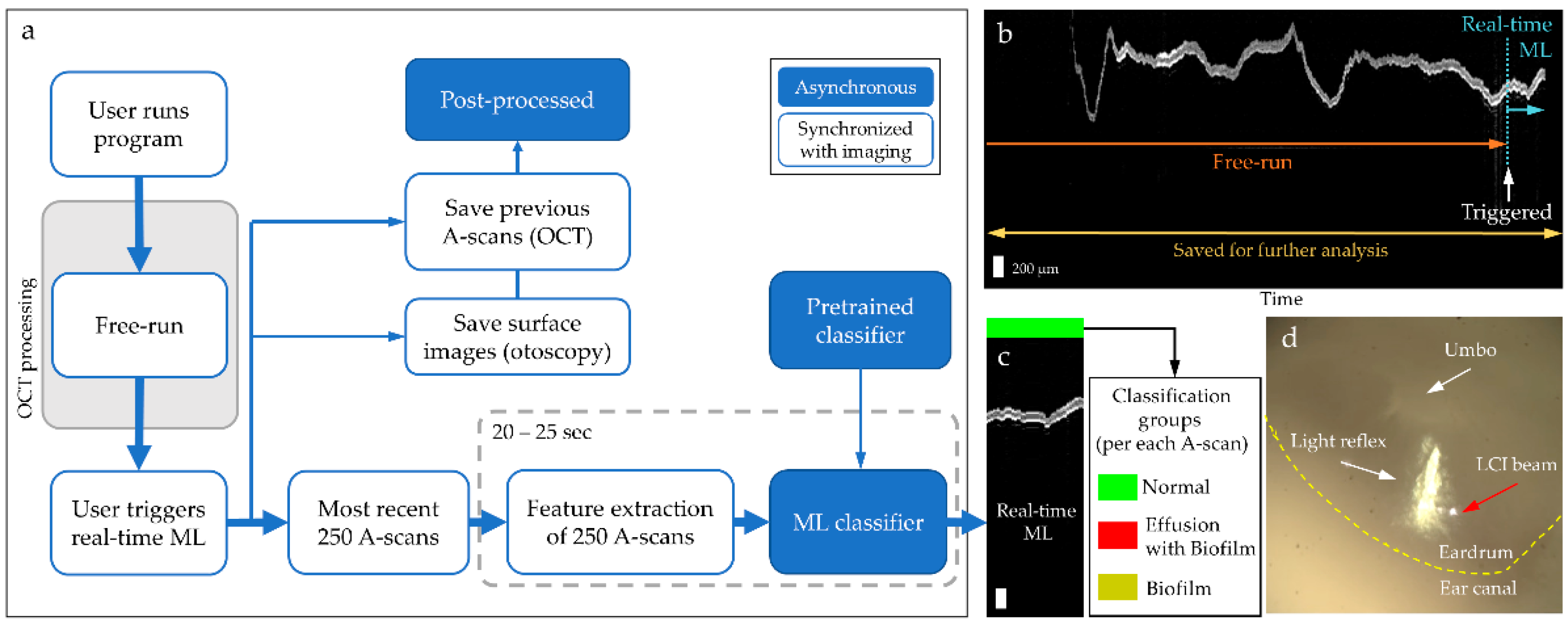
2.2. Integration of Real-Time Machine Learning Classifier in the Briefcase System
2.3. Imaging Human Subjects
2.4. Analytical Methods
3. Results
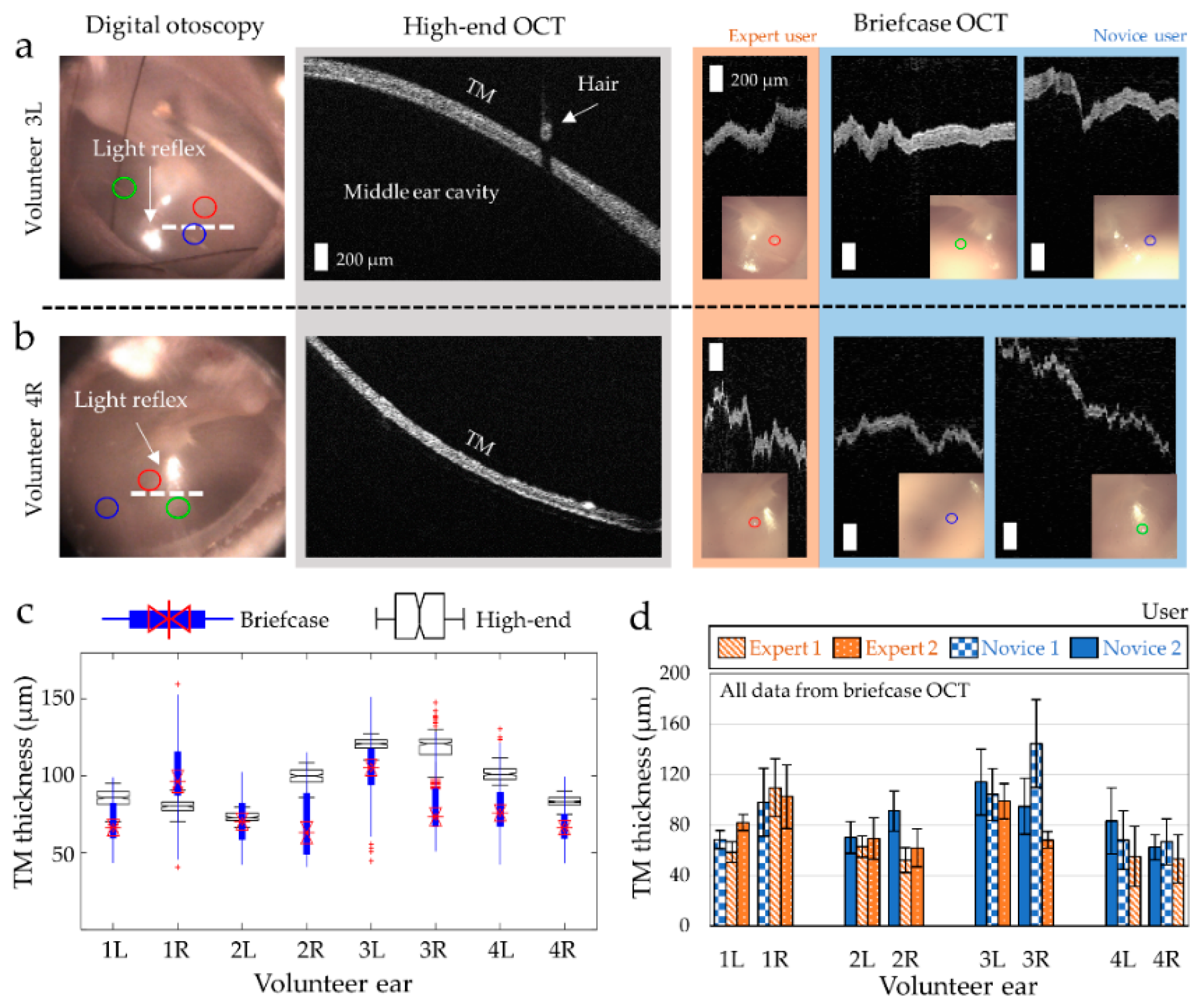
3.1. Middle Ear Imaging of Healthy Volunteers
3.2. User-Invariant Classifications of Healthy Middle Ear
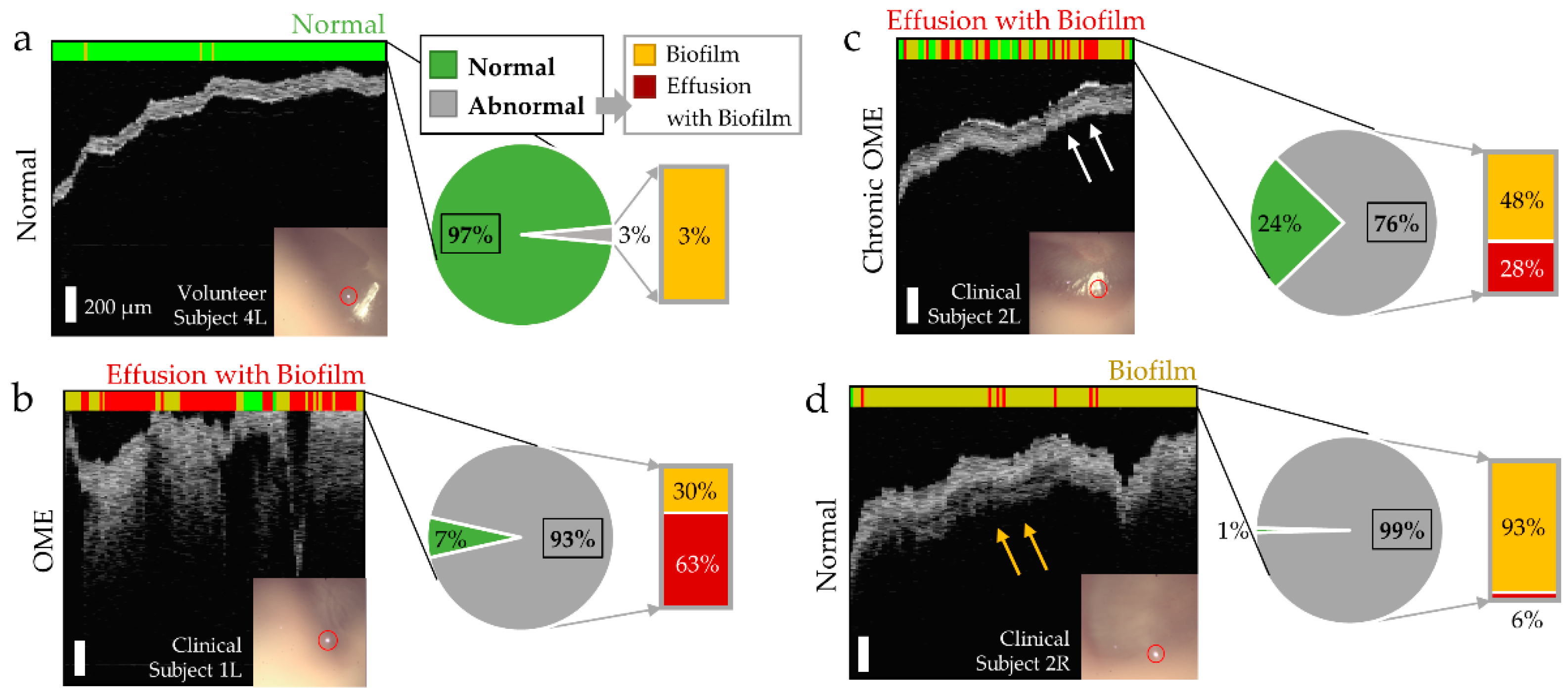
3.3. Machine Learning Classification of Middle Ear Conditions during OM
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Schilder, A.G.M.; Chonmaitree, T.; Cripps, A.W.; Rosenfeld, R.M.; Casselbrant, M.L.; Haggard, M.P.; Venekamp, R.P. Otitis media. Nat. Rev. Dis. Prim. 2016, 2, 1–18. [Google Scholar] [CrossRef]
- Coker, T.R.; Chan, L.S.; Newberry, S.J.; Limbos, M.A.; Suttorp, M.J.; Shekelle, P.G.; Takata, G.S. Diagnosis, microbial epidemiology, and antibiotic treatment of acute otitis media in children: A systematic review. J. Am. Med. Assoc. 2010, 304, 2161–2169. [Google Scholar] [CrossRef]
- Teele, D.W.; Klein, J.O.; Rosner, B. Epidemiology of otitis media during the first seven years of life in children in greater Boston: A prospective, cohort study. J. Infect. Dis. 1989, 160, 83–94. [Google Scholar] [CrossRef]
- Tong, S.; Amand, C.; Kieffer, A.; Kyaw, M.H. Trends in healthcare utilization and costs associated with acute otitis media in the United States during 2008–2014. BMC Health Serv. Res. 2018, 18, 1–10. [Google Scholar] [CrossRef]
- Rosenfeld, R.M.; Shin, J.J.; Schwartz, S.R.; Coggins, R.; Gagnon, L.; Hackell, J.M.; Hoelting, D.; Hunter, L.L.; Kummer, A.W.; Payne, S.C.; et al. Clinical practice guidelines: Otitis media with effusion (update). Otolaryngol. Head Neck Surg. 2016, 154, S1–S41. [Google Scholar] [CrossRef]
- Lieberthal, A.S.; Carroll, A.E.; Chonmaitree, T.; Ganiats, T.G.; Hoberman, A.; Jackson, M.A.; Joffe, M.D.; Miller, D.T.; Rosenfield, R.M.; Sevilla, X.D.; et al. The diagnosis and management of acute otitis media. Pediatr 2013, 131, e964–e999. [Google Scholar] [CrossRef] [PubMed]
- Harmes, K.M.; Blackwood, R.A.; Burrows, H.L.; Cooke, J.M.; Van Harrison, R.; Passamani, P.P. Otitis media: Diagnosis and treatment. Am. Fam. Physician 2013, 88, 435–440. [Google Scholar] [PubMed]
- Vergison, A.; Dagan, R.; Arguedas, A.; Bonhoeffer, J.; Cohen, R.; DHooge, I.; Hoberman, A.; Liese, J.; Marchisio, P.; Palmu, A.A.; et al. Otitis media and its consequences: Beyond the earache. Lancet Infect. Dis. 2010, 10, 195–203. [Google Scholar] [CrossRef]
- Pichichero, M.E.; Poole, M.D. Comparison of performance by otolaryngologists, pediatricians, and general practioners on an otoendoscopic diagnostic video examination. Int. J. Pediatr. Otorhinolaryngol. 2005, 69, 361–366. [Google Scholar] [CrossRef]
- Hubler, Z.; Shemonski, N.D.; Shelton, R.L.; Monroy, G.L.; Nolan, R.M.; Boppart, S.A. Real-time automated thickness measurement of the in vivo human tymspanic membrane using optical coherence tomography. Quant. Imaging Med. Surg. 2015, 5, 69–77. [Google Scholar] [PubMed]
- Monroy, G.L.; Pande, P.; Nolan, R.M.; Shelton, R.L.; Porter, R.G.; Novak, M.A.; Spillman, D.R.; Chaney, E.J.; McCormick, D.T.; Boppart, S.A. Noninvasive in vivo optical coherence tomography tracking of chronic otitis media in pediatric subjects after surgical intervention. J. Biomed. Opt. 2017, 22, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Monroy, G.L.; Won, J.; Spillman, D.R.; Dsouza, R.; Boppart, S.A. Clinical translation of handheld optical coherence tomography: Practical considerations and recent advancements. J. Biomed. Opt. 2017, 22, 1–30. [Google Scholar] [CrossRef]
- Shelton, R.L.; Jung, W.; Sayegh, S.I.; McCormick, D.T.; Kim, J.; Boppart, S.A. Optical coherence tomography for advanced screening in the primary care office. J. Biophotonics 2014, 7, 525–533. [Google Scholar] [CrossRef]
- Preciado, D.; Nolan, R.M.; Joshi, R.; Krakovsky, G.M.; Zhang, A.; Pudik, N.A.; Kumar, N.K.; Shelton, R.L.; Boppart, S.A.; Bauman, N.M. Otitis media middle ear effusion identification and characterization using an optical coherence tomography otoscope. Otolaryngol. Neck Surg. 2020, 162, 367–374. [Google Scholar] [CrossRef] [PubMed]
- Kirsten, L.; Schindler, M.; Morgenstern, J.; Erkkilä, M.T.; Golde, J.; Walther, J.; Rottmann, P.; Kemper, M.; Bornitz, M.; Neudert, M.; et al. Endoscopic optical coherence tomography with wide field-of-view for the morphological and functional assessment of the human tympanic membrane. J. Biomed. Opt. 2018, 24, 1–11. [Google Scholar] [CrossRef]
- Kim, W.; Kim, S.; Huang, S.; Oghalai, J.S.; Applegate, B.E. Picometer scale vibrometry in the human middle ear using a surgical microscope based optical coherence tomography and vibrometry system. Biomed. Opt. Express 2019, 10, 4395–4410. [Google Scholar] [CrossRef]
- Byun, H.; Kim, Y.H.; Xing, J.; Shin, S.-J.; Lee, S.H.; Yoo, H.; Chung, J.H. Utilization potential of intraluminal optical coherence tomography for the Eustachian tube. Sci. Rep. 2021, 11, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Schuon, R.; Mrevlje, B.; Vollmar, B.; Lenarz, T.; Paasche, G. Intraluminal three-dimensional optical coherence tomography—A tool for imaging of the Eustachian tube? J. Laryngol. Otol. 2019, 133, 87–94. [Google Scholar] [CrossRef]
- Huang, D.; Swanson, E.A.; Lin, C.P.; Schuman, J.S.; Stinson, W.G.; Chang, W.; Hee, M.R.; Flotte, T.; Gregory, K.; Puliafito, C.A.; et al. Optical coherence tomography. Science 1991, 254, 1178–1181. [Google Scholar] [CrossRef]
- Monroy, G.L.; Shelton, R.L.; Nolan, R.M.; Nguyen, C.T.; Novak, M.A.; Hill, M.C.; McCormick, D.T.; Boppart, S.A. Noninvasive depth-resolved optical measurements of the tympanic membrane and middle ear for differentiating otitis media. Laryngoscope 2015, 125, E276–E282. [Google Scholar] [CrossRef]
- Monroy, G.L.; Pande, P.; Shelton, R.L.; Nolan, R.M.; Spillman, D.R., Jr.; Porter, R.G.; Novak, M.A.; Boppart, S.A. Non-invasive optical assessment of viscosity of middle ear effusions in otitis media. J. Biophotonics 2017, 10, 394–403. [Google Scholar] [CrossRef] [PubMed]
- Won, J.; Monroy, G.L.; Huang, P.-C.; Hill, M.C.; Novak, M.A.; Porter, R.G.; Spillman, D.R.; Chaney, E.J.; Barkalifa, R.; Boppart, S.A. Assessing the effect of middle ear effusions on wideband acoustic immittance using optical coherence tomography. Ear Hear. 2020, 41, 811–824. [Google Scholar] [CrossRef] [PubMed]
- Monroy, G.L.; Hong, W.; Khampang, P.; Porter, R.G.; Novak, M.A.; Spillman, D.R.; Barkalifa, R.; Chaney, E.J.; Kerschner, J.E.; Boppart, S.A. Direct analysis of pathogenic structures affixed to the tympanic membrane during chronic otitis media. Otolaryngol. Neck Surg. 2018, 159, 117–126. [Google Scholar] [CrossRef]
- Nguyen, C.T.; Jung, W.; Kim, J.; Chaney, E.J.; Novak, M.; Stewart, C.N.; Boppart, S.A. Noninvasive in vivo optical detection of biofilm in the human middle ear. Proc. Natl. Acad. Sci. USA 2012, 109, 9529–9534. [Google Scholar] [CrossRef]
- Won, J.; Hong, W.; Khampang, P.; Spillman, D.R., Jr.; Marshall, S.; Yan, K.; Porter, R.G.; Novak, M.A.; Kerschner, J.E.; Boppart, S.A. Longitudinal optical coherence tomography to visualize the in vivo response of middle ear biofilms to antibiotic therapy. Sci. Rep. 2021, 11, 1–13. [Google Scholar] [CrossRef]
- Tawfik, S.A.E.-S.; Ibrahim, A.A.; Talaat, I.M.; El-Alkamy, S.S.A.E.-R.; Youssef, A. Role of bacterial biofilm in development of middle ear effusion. Eur. Arch. Oto-Rhino-Laryngol. 2016, 273, 4003–4009. [Google Scholar] [CrossRef] [PubMed]
- Bakaletz, L.O. Bacterial biofilms in otitis media: Evidence and relevance. Pediatr. Infect. Dis. J. 2007, 26, 17–19. [Google Scholar] [CrossRef]
- Hall-Stoodley, L.; Hu, F.Z.; Gieseke, A.; Nistico, L.; Nguyen, D.; Hayes, J.; Forbes, M.; Greenberg, D.P.; Dice, B.; Burrows, A.; et al. Direct detection of bacterial biofilms on the middle-ear mucosa of children with chronic otitis media. JAMA 2006, 296, 202–211. [Google Scholar] [CrossRef]
- Post, J.C. Direct evidence of bacterial biofilms in otitis media. Laryngoscope 2001, 111, 2083–2094. [Google Scholar] [CrossRef]
- Marom, T.; Kraus, O.; Habashi, N.; Tamir, S.O. Emerging technologies for the diagnosis of otitis media. Otolaryngol. Neck Surg. 2018, 160, 447–456. [Google Scholar] [CrossRef]
- Dsouza, R.; Won, J.; Monroy, G.L.; Spillman, D.R.; Boppart, S.A. Economical and compact briefcase spectral-domain optical coherence tomography system for primary care and point-of-care applications. J. Biomed. Opt. 2018, 23, 096003. [Google Scholar] [CrossRef]
- Erickson, B.J.; Korfiatis, P.; Akkus, Z.; Kline, T.L. Machine learning for medical imaging. Radiographics 2017, 37, 505–515. [Google Scholar] [CrossRef]
- Cao, C.; Liu, F.; Tan, H.; Song, D.; Shu, W.; Li, W.; Zhou, Y.; Bo, X.; Xie, Z. Deep learning and its applications in biomedicine. Genom. Proteom. Bioinform. 2018, 16, 17–32. [Google Scholar] [CrossRef] [PubMed]
- Ran, A.R.; Tham, C.C.; Chan, P.P.; Cheng, C.-Y.; Tham, Y.-C.; Rim, T.H.; Cheung, C.Y. Deep learning in glaucoma with optical coherence tomography: A review. Eye 2021, 35, 188–201. [Google Scholar] [CrossRef] [PubMed]
- Monroy, G.L.; Won, J.; Dsouza, R.; Pande, P.; Hill, M.C.; Porter, R.G.; Novak, M.A.; Spillman, D.R.; Boppart, S.A. Automated classification platform for the identification of otitis media using optical coherence tomography. NPJ Digit. Med. 2019, 2, 1–11. [Google Scholar] [CrossRef]
- Vermeer, K.A.; Mo, J.; Weda, J.J.A.; Lemij, H.G.; De Boer, J.F. Depth-resolved model-based reconstruction of attenuation coefficients in optical coherence tomography. Biomed. Opt. Express 2014, 5, 322–337. [Google Scholar] [CrossRef]
- Van Der Jeught, S.; Dirckx, J.J.J.; Aerts, J.R.M.; Bradu, A.; Podoleanu, A.G.; Buytaert, J.A.N. Full-field thickness distribution of human tympanic membrane obtained with optical coherence tomography. J. Assoc. Res. Otolaryngol. 2013, 14, 483–494. [Google Scholar] [CrossRef]
- Barnett, M.L.; Ray, K.N.; Souza, J.; Mehrotra, A. Trends in telemedicine use in a large commercially insured population, 2005–2017. JAMA 2018, 320, 2147–2149. [Google Scholar] [CrossRef] [PubMed]
- Singh, A.K.; Kasle, D.A.; Jiang, R.; Sukys, J.; Savoca, E.L.; Lerner, M.Z.; Kohli, N. A review of telemedicine applications in otorhinolaryngology: Considerations during the coronavirus disease of 2019 pandemic. Laryngoscope 2021, 131, 744–759. [Google Scholar] [CrossRef]
- Cai, Y.; Zheng, Y.J.; Gulati, A.; Butrymowicz, A.; Krauter, R.; Pletcher, S.D.; Sharon, J.D.; Goldberg, A.N.; Chang, J.L. Patient use of low-cost digital videoscopes and smartphones for remote ear and oropharyngeal examinations. JAMA Otolaryngol. Neck Surg. 2021, 147, 336–342. [Google Scholar] [CrossRef]
- Livingstone, D.; Talai, A.S.; Chau, J.; Forkert, N.D. Building an otoscopic screening prototype tool using deep learning. J. Otolaryngol. Head Neck Surg. 2019, 48, 1–5. [Google Scholar] [CrossRef]
- Pichichero, M.E. Can machine learning and AI replace otoscopy for diagnosis of otitis media? Pediatrics 2021, 147, e2020049584. [Google Scholar] [CrossRef]
- Crowson, M.G.; Hartnick, C.J.; Diercks, G.R.; Gallagher, T.Q.; Fracchia, M.S.; Setlur, J.; Cohen, M.S. Machine learning for accurate intraoperative pediatric middle ear effusion diagnosis. Pediatrics 2021, 147, e2020034546. [Google Scholar] [CrossRef] [PubMed]
- Livingstone, D.; Chau, J. Otoscopic diagnosis using computer vision: An automated machine learning approach. Laryngoscope 2020, 130, 1408–1413. [Google Scholar] [CrossRef]
- Viscaino, M.; Maass, J.C.; Delano, P.H.; Torrente, M.; Stott, C.; Cheein, F.A. Computer-aided diagnosis of external and middle ear conditions: A machine learning approach. PLoS ONE 2020, 15, e0229226. [Google Scholar] [CrossRef]
- Pichichero, M.E.; Poole, M.D. Assessing diagnostic accuracy and tympanocentesis skills in the management of otitis media. Arch. Pediatr. Adolesc. Med. 2001, 155, 1137–1142. [Google Scholar] [CrossRef] [PubMed]
- Hillmann, D. OCT on a chip aims at high-quality retinal imaging. Light. Sci. Appl. 2021, 10. [Google Scholar] [CrossRef]
- Yurtsever, G.; Weiss, N.; Kalkman, J.; Van Leeuwen, T.G.; Baets, R. Ultra-compact silicon photonic integrated interferometer for swept-source optical coherence tomography. Opt. Lett. 2014, 39, 5228–5231. [Google Scholar] [CrossRef] [PubMed]






Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Won, J.; Monroy, G.L.; Dsouza, R.I.; Spillman, D.R., Jr.; McJunkin, J.; Porter, R.G.; Shi, J.; Aksamitiene, E.; Sherwood, M.; Stiger, L.; et al. Handheld Briefcase Optical Coherence Tomography with Real-Time Machine Learning Classifier for Middle Ear Infections. Biosensors 2021, 11, 143. https://doi.org/10.3390/bios11050143
Won J, Monroy GL, Dsouza RI, Spillman DR Jr., McJunkin J, Porter RG, Shi J, Aksamitiene E, Sherwood M, Stiger L, et al. Handheld Briefcase Optical Coherence Tomography with Real-Time Machine Learning Classifier for Middle Ear Infections. Biosensors. 2021; 11(5):143. https://doi.org/10.3390/bios11050143
Chicago/Turabian StyleWon, Jungeun, Guillermo L. Monroy, Roshan I. Dsouza, Darold R. Spillman, Jr., Jonathan McJunkin, Ryan G. Porter, Jindou Shi, Edita Aksamitiene, MaryEllen Sherwood, Lindsay Stiger, and et al. 2021. "Handheld Briefcase Optical Coherence Tomography with Real-Time Machine Learning Classifier for Middle Ear Infections" Biosensors 11, no. 5: 143. https://doi.org/10.3390/bios11050143
APA StyleWon, J., Monroy, G. L., Dsouza, R. I., Spillman, D. R., Jr., McJunkin, J., Porter, R. G., Shi, J., Aksamitiene, E., Sherwood, M., Stiger, L., & Boppart, S. A. (2021). Handheld Briefcase Optical Coherence Tomography with Real-Time Machine Learning Classifier for Middle Ear Infections. Biosensors, 11(5), 143. https://doi.org/10.3390/bios11050143