
Retrospective Radiographic Evaluation of Ridge Dimensional Changes After Vertical Augmentation Using the Novel Wide-Head Tent Pole Screw Technique


Abstract
1. Introduction
2. Materials and Methods
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Gerritsen, A.E.; Allen, P.F.; Witter, D.J.; Bronkhorst, E.M.; Creugers, N.H. Tooth loss and oral health-related quality of life: A systematic review and meta-analysis. Health Qual. Life Outcomes 2010, 8, 126. [Google Scholar] [CrossRef] [PubMed]
- Ali, Z.; Baker, S.R.; Shahrbaf, S.; Martin, N.; Vettore, M.V. Oral health-related quality of life after prosthodontic treatment for patients with partial edentulism: A systematic review and meta-analysis. J. Prosthet. Dent. 2019, 121, 59–68.e3. [Google Scholar] [CrossRef] [PubMed]
- Aghaloo, T.L.; Moy, P.K. Which hard tissue augmentation techniques are the most successful in furnishing bony support for implant placement? Int. J. Oral Maxillofac. Implants 2007, 22, 49–70. [Google Scholar] [PubMed]
- Aloy-Prósper, A.; Peñarrocha-Oltra, D.; Peñarrocha-Diago, M.; Peñarrocha-Diago, M. The outcome of intraoral onlay block bone grafts on alveolar ridge augmentations: A systematic review. Med. Oral Patol. Oral Cir Bucal 2015, 20, e251–e258. [Google Scholar] [CrossRef]
- Sakkas, A.; Wilde, F.; Heufelder, M.; Winter, K.; Schramm, A. Autogenous bone grafts in oral implantology-is it still a “gold standard”? A consecutive review of 279 patients with 456 clinical procedures. Int. J. Implant. Dent. 2017, 3, 23. [Google Scholar]
- Jensen, O.T. Alveolar segmental “Sandwich” osteotomies for posterior edentulous mandibular sites for dental implants. J. Oral. Maxillofac. Surg. 2006, 64, 471–475. [Google Scholar] [CrossRef]
- Khoury, F.; Hanser, T. Three-Dimensional Vertical Alveolar Ridge Augmentation in the Posterior Maxilla: A 10-year Clinical Study. Int. J. Oral. Maxillofac. Implants. 2019, 34, 471–480. [Google Scholar] [CrossRef]
- Esenlik, E.; DeMitchell-Rodriguez, E.M. Alveolar Distraction. Clin. Plast. Surg. 2021, 48, 419–429. [Google Scholar] [CrossRef]
- Hameed, M.H.; Gul, M.; Ghafoor, R.; Khan, F.R. Vertical Ridge Gain with Various Bone Augmentation Techniques: A Systematic Review and Meta-Analysis. J. Prosthodont. 2019, 28, 421–427. [Google Scholar] [CrossRef]
- Urban, I.A.; Lozada, J.L.; Wessing, B.; Suárez-López del Amo, F.; Wang, H.L. Vertical Bone Grafting and Periosteal Vertical Mattress Suture for the Fixation of Resorbable Membranes and Stabilization of Particulate Grafts in Horizontal Guided Bone Regeneration to Achieve More Predictable Results: A Technical Report. Int. J. Periodontics Restor. Dent. 2016, 36, 153–159. [Google Scholar] [CrossRef]
- Marx, R.E.; Shellenberger, T.; Wimsatt, J.; Correa, P. Severely resorbed mandible: Predictable reconstruction with soft tissue matrix expansion (tent pole) grafts. J. Oral. Maxillofac. Surg. 2002, 60, 878–888, discussion 888–889. [Google Scholar] [CrossRef] [PubMed]
- Fenton, C.C.; Nish, I.A.; Carmichael, R.P.; Sàndor, G.K. Metastatic mandibular retinoblastoma in a child reconstructed with soft tissue matrix expansion grafting: A preliminary report. J. Oral. Maxillofac. Surg. 2007, 65, 2329–2335. [Google Scholar] [CrossRef] [PubMed]
- Manfro, R.; Batassini, F.; Bortoluzzi, M.C. Severely resorbed mandible treated by soft tissue matrix expansion (tent pole) grafts: Case report. Implant. Dent. 2008, 17, 408–413. [Google Scholar] [CrossRef]
- Guillen, G.A.; Araújo, A.L.D.; Macêdo, F.G.C.; Groppo, F.C.; Vargas, P.A.; Nóia, C.F. Evaluation of the screw tent-pole technique for the repair of anterior maxilla width defects: A prospective, randomized, split-mouth study. Int. J. Oral. Maxillofac. Surg. 2021, 50, 801–807. [Google Scholar] [CrossRef]
- Deeb, G.R.; Tran, D.; Carrico, C.K.; Block, E.; Laskin, D.M.; Deeb, J.G. How effective is the tent screw pole technique compared to other forms of horizontal ridge augmentation? J. Oral. Maxillofac. Surg. 2017, 75, 2093–2098. [Google Scholar] [CrossRef]
- Sohn, D.S.; Huang, B.; Kim, J.; Park, W.E.; Park, C.C. Utilization of autologous concentrated growth factors (CGF) enriched bone graft matrix (Sticky Bone) and CGF-enriched fibrin membrane in implant dentistry. J. Implant. Adv. Clin. Dent. 2015, 7, 11–29. [Google Scholar]
- Park, Y.H.; Choi, S.H.; Cho, K.S.; Lee, J.S. Dimensional alterations following vertical ridge augmentation using collagen membrane and three types of bone grafting materials: A retrospective observational study. Clin. Implant. Dent. Relat. Res. 2017, 19, 742–749. [Google Scholar] [CrossRef]
- Chavda, S.; Levin, L. Human studies of vertical and horizontal alveolar ridge augmentation comparing different types of bone graft materials: A systematic review. J. Oral. Implantol. 2018, 44, 74–84. [Google Scholar] [CrossRef]
- Sáez-Alcaide, L.M.; González Gallego, B.; Fernando Moreno, J.; Moreno Navarro, M.; Cobo-Vázquez, C.; Cortés-Bretón Brinkmann, J.; Meniz-García, C. Complications associated with vertical bone augmentation techniques in implant dentistry: A systematic review of clinical studies published in the last ten years. J. Stomatol. Oral Maxillofac. Surg. 2023, 124, 101574. [Google Scholar] [CrossRef]
- Sakkas, A.; Schramm, A.; Winter, K.; Wilde, F. Risk factors for post-operative complications after procedures for autologous bone augmentation from different donor sites. J. Cranio-Maxillofac. Surg. 2018, 46, 312–322. [Google Scholar] [CrossRef]
- Koo, H.; Hwang, J.; Choi, B.J.; Lee, W.J.; Ohe, J.Y.; Jung, J. Comparison of vertical bone resorption following various types of autologous block bone grafts. Maxillofac. Plast. Reconstr. Surg. 2023, 45, 38. [Google Scholar] [CrossRef] [PubMed]
- Sbordone, L.; Toti, P.; Menchini-Fabris, G.B.; Sbordone, C.; Piombino, P.; Guidetti, F. Volume changes of autogenous bone grafts after alveolar ridge augmentation of atrophic maxillae and mandibles. Int. J. Oral. Maxillofac. Surg. 2009, 38, 1059–1065. [Google Scholar] [CrossRef] [PubMed]
- Sabri, H.; Heck, T.; Manouchehri, N.; Alhachache, S.; Calatrava, J.; Misch, C.M.; Wang, H.L. Bone augmentation using titanium mesh: A systematic review and meta-analysis. Int J Oral Implant. 2024, 17, 251–269. [Google Scholar]
- Uehara, S.; Kurita, H.; Shimane, T.; Sakai, H.; Kamata, T.; Teramoto, Y.; Yamada, S. Predictability of staged localized alveolar ridge augmentation using a micro titanium mesh. Oral. Maxillofac. Surg. 2015, 19, 411–416. [Google Scholar] [CrossRef]
- Aceves-Argemí, R.; Roca-Millan, E.; González-Navarro, B.; Marí-Roig, A.; Velasco-Ortega, E.; López-López, J. Titanium meshes in guided bone regeneration: A systematic review. Coatings 2021, 11, 316. [Google Scholar] [CrossRef]
- Chiapasco, M.; Consolo, U.; Bianchi, A.; Ronchi, P. Alveolar distraction osteogenesis for the correction of vertically deficient edentulous ridges: A multicenter prospective study on humans. Int. J. Oral. Maxillofac. Implant. 2004, 19, 399–407. [Google Scholar] [CrossRef]
- Roccuzzo, A.; Marchese, S.; Worsaae, N.; Jensen, S.S. The sandwich osteotomy technique to treat vertical alveolar bone defects prior to implant placement: A systematic review. Clin. Oral. Investig. 2020, 24, 1073–1089. [Google Scholar] [CrossRef]
- Khoury, F.; Hanser, T. 3D vertical alveolar crest augmentation in the posterior mandible using the tunnel technique: A 10-year clinical study. Int. J. Oral Implantol. 2022, 15, 111–126. [Google Scholar]
- Soldatos, N.K.; Stylianou, P.; Koidou, V.P.; Angelov, N.; Yukna, R.; Romanos, G.E. Limitations and options using resorbable versus nonresorbable membranes for successful guided bone regeneration. Quintessence Int. 2017, 48, 131–147. [Google Scholar]
- Tay, J.R.H.; Ng, E.; Lu, X.J.; Lai, W.M.C. Healing complications and their detrimental effects on bone gain in vertical-guided bone regeneration: A systematic review and meta-analysis. Clin. Implant. Dent. Relat. Res. 2022, 24, 43–71. [Google Scholar] [CrossRef]
- Urban, I.A.; Montero, E.; Monje, A.; Sanz-Sánchez, I. Effectiveness of vertical ridge augmentation interventions: A systematic review and meta-analysis. J. Clin. Periodontol. 2019, 46 (Suppl. 21), 319–339. [Google Scholar] [CrossRef] [PubMed]
- Abdullrahman, F.; Assad, M.; Albash, Z. Tent-pole technique for alveolar ridge width preservation with a compromised buccal plate: A prospective cohort study. Ann. Med. Surg. 2023, 85, 5344–5349. [Google Scholar] [CrossRef] [PubMed]
- Le, B.; Rohrer, M.D.; Prasad, H.S. Screw “tent-pole” grafting technique for reconstruction of large vertical alveolar ridge defects using human mineralized allograft for implant site preparation. J. Oral. Maxillofac. Surg. 2010, 68, 428–435. [Google Scholar] [CrossRef] [PubMed]
- Troeltzsch, M.; Troeltzsch, M.; Kauffmann, P.; Gruber, R.; Brockmeyer, P.; Moser, N.; Rau, A.; Schliephake, H. Clinical efficacy of grafting materials in alveolar ridge augmentation: A systematic review. J. Cranio-Maxillofac. Surg. 2016, 44, 1618–1629. [Google Scholar] [CrossRef]
- Elnayef, B.; Monje, A.; Gargallo-Albiol, J.; Galindo-Moreno, P.; Wang, H.L.; Hernández-Alfaro, F. Vertical ridge augmentation in the atrophic mandible: A systematic review and meta-analysis. Int. J. Oral. Maxillofac. Implant. 2017, 32, 291–312. [Google Scholar] [CrossRef]
- Palkovics, D.; Solyom, E.; Somodi, K.; Pinter, C.; Windisch, P.; Bartha, F.; Molnar, B. Three-dimensional volumetric assessment of hard tissue alterations following horizontal guided bone regeneration using a split-thickness flap design: A case series. BMC Oral. Health 2023, 23, 118. [Google Scholar] [CrossRef]
- Sohn, D.S. Reconstruction of three-dimensional alveolar ridge defects utilizing screws and implant abutments for the tent-pole grafting techniques. In Essential Techniques of Alveolar Bone Augmentation in Implant Dentistry, 2nd ed.; Tolstunov, L., Ed.; Wiley Blackwell: Hoboken, NJ, USA, 2023; pp. 404–418. [Google Scholar]
- Sohn, D.S.; Lui, A.; Choi, H. Utilization of tenting pole abutments for the reconstruction of severely resorbed alveolar bone: Technical considerations and case series reports. J. Clin. Med. 2024, 13, 1156. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
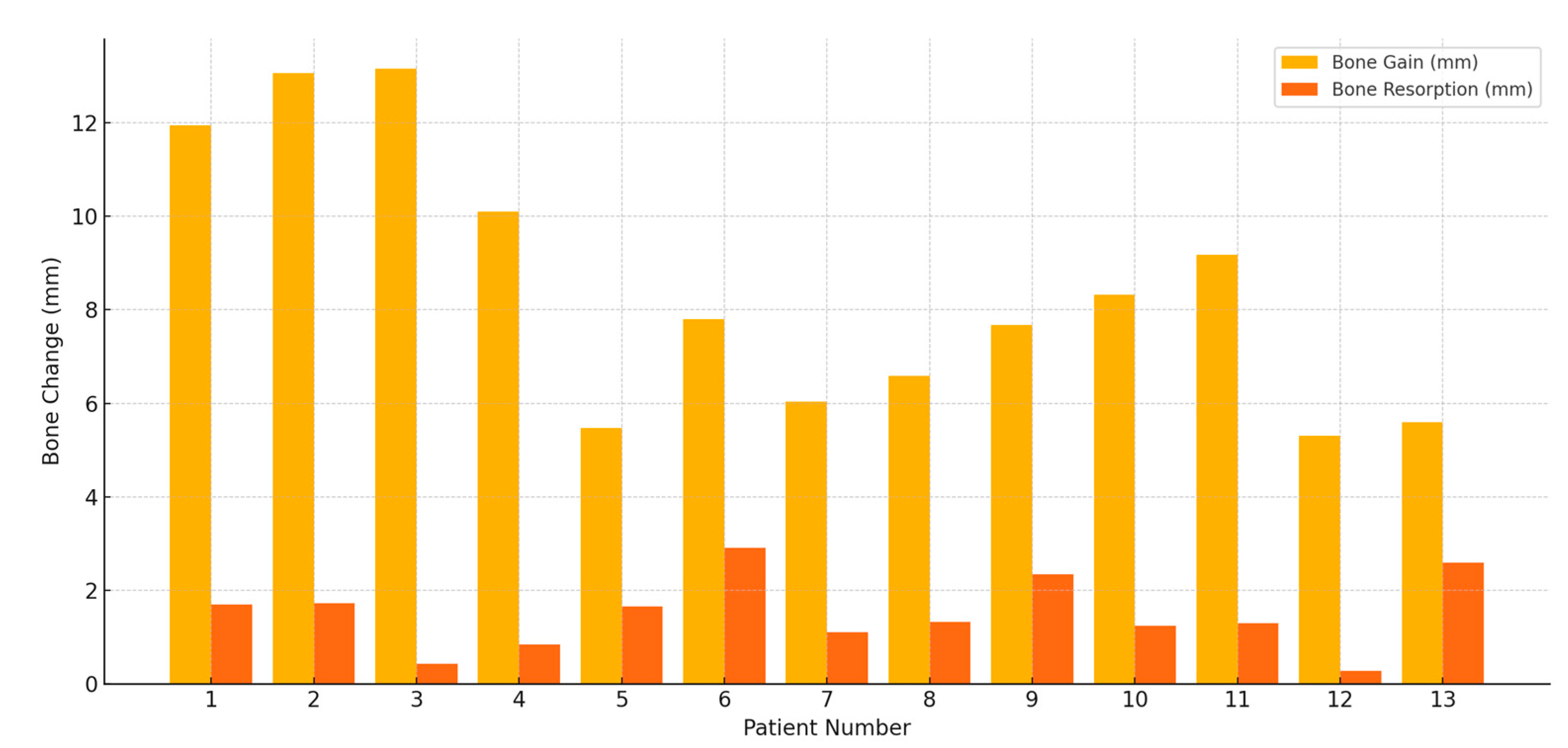
| Patient | Post-Op Height (mm) | Prosthetic Loading (mm, Month) | Functional Loading (mm, Month) | Bone Gain (mm) | Bone Resorption (mm) |
|---|---|---|---|---|---|
| 1 | 29.57 | 28.91 (5 m) | 27.87 (11 m) | 11.95 | 1.7 |
| 2 | 25.82 | 25.3 (4 m) | 24.1 (8 m) | 13.06 | 1.72 |
| 3 | 32.86 | 32.63 (3 m) | 32.43 (8 m) | 13.15 | 0.43 |
| 4 | 16.52 | 15.8 (4 m) | 15.68 (16 m) | 10.10 | 0.84 |
| 5 | 25.33 | 24.06 (3 m) | 23.68 (14 m) | 5.47 | 1.65 |
| 6 | 23.97 | 21.56 (6 m 3 w) | 21.06 (18 m) | 7.8 | 2.91 |
| 7 | 30.20 | 29.13 (6 m) | 29.1 (10 m) | 6.03 | 1.1 |
| 8 | 22.96 | 22.12 (6 m) | 21.64 (20 m) | 6.59 | 1.32 |
| 9 | 28.99 | 27.19 (7 m) | 26.65 (13 m) | 7.67 | 2.34 |
| 10 | 29.37 | 28.19 (7 m) | 28.13 (20 m) | 8.32 | 1.24 |
| 11 | 24.20 | 23.7 (5 m) | 22.9 (8 m) | 9.17 | 1.3 |
| 12 | 25.68 | 25.56 (7 m) | 25.4 (16 m) | 5.3 | 0.28 |
| 13 | 23.78 | 21.69 (7 m) | 21.19 (19 m) | 5.59 | 2.59 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yoon, N.-S.; Choi, H.; Kim, H.-G.; Sohn, D.-S. Retrospective Radiographic Evaluation of Ridge Dimensional Changes After Vertical Augmentation Using the Novel Wide-Head Tent Pole Screw Technique. J. Funct. Biomater. 2025, 16, 215. https://doi.org/10.3390/jfb16060215
Yoon N-S, Choi H, Kim H-G, Sohn D-S. Retrospective Radiographic Evaluation of Ridge Dimensional Changes After Vertical Augmentation Using the Novel Wide-Head Tent Pole Screw Technique. Journal of Functional Biomaterials. 2025; 16(6):215. https://doi.org/10.3390/jfb16060215
Chicago/Turabian StyleYoon, Nam-Suk, Hyunsuk Choi, Hyung-Gyun Kim, and Dong-Seok Sohn. 2025. "Retrospective Radiographic Evaluation of Ridge Dimensional Changes After Vertical Augmentation Using the Novel Wide-Head Tent Pole Screw Technique" Journal of Functional Biomaterials 16, no. 6: 215. https://doi.org/10.3390/jfb16060215
APA StyleYoon, N.-S., Choi, H., Kim, H.-G., & Sohn, D.-S. (2025). Retrospective Radiographic Evaluation of Ridge Dimensional Changes After Vertical Augmentation Using the Novel Wide-Head Tent Pole Screw Technique. Journal of Functional Biomaterials, 16(6), 215. https://doi.org/10.3390/jfb16060215