
Molar Distalization by Clear Aligners with Sequential Distalization Protocol: A Systematic Review and Meta-Analysis


Abstract
1. Introduction
2. Materials and Methods
2.1. Study Selection Criteria
2.2. Search Strategy
2.3. Data Extraction and Analysis
2.4. Risk of Bias/Quality Assessment
2.5. Statistical Analysis
3. Results
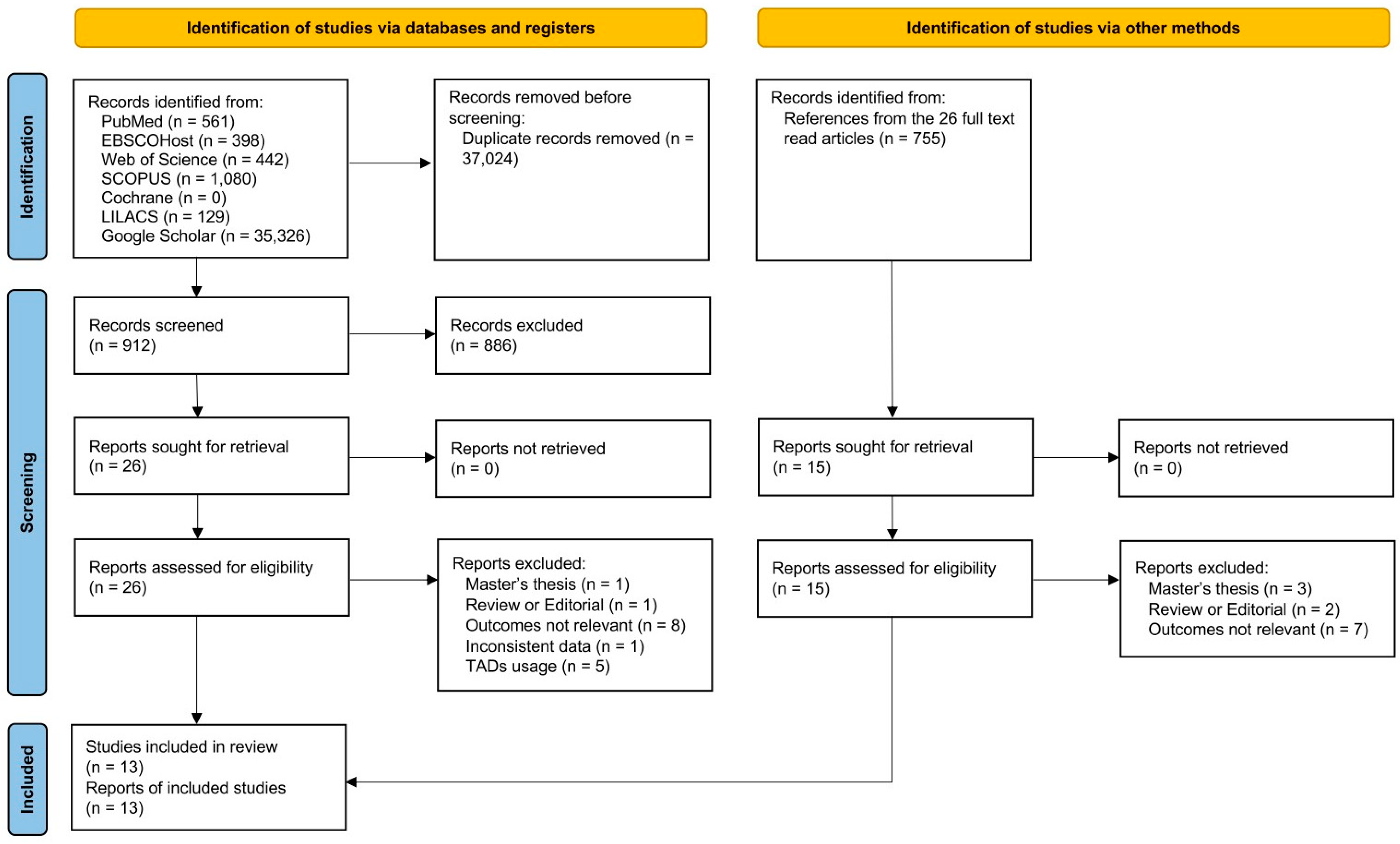
3.1. Literature Searching and Study Selections
3.2. Risk of Bias
3.3. Demographic Data
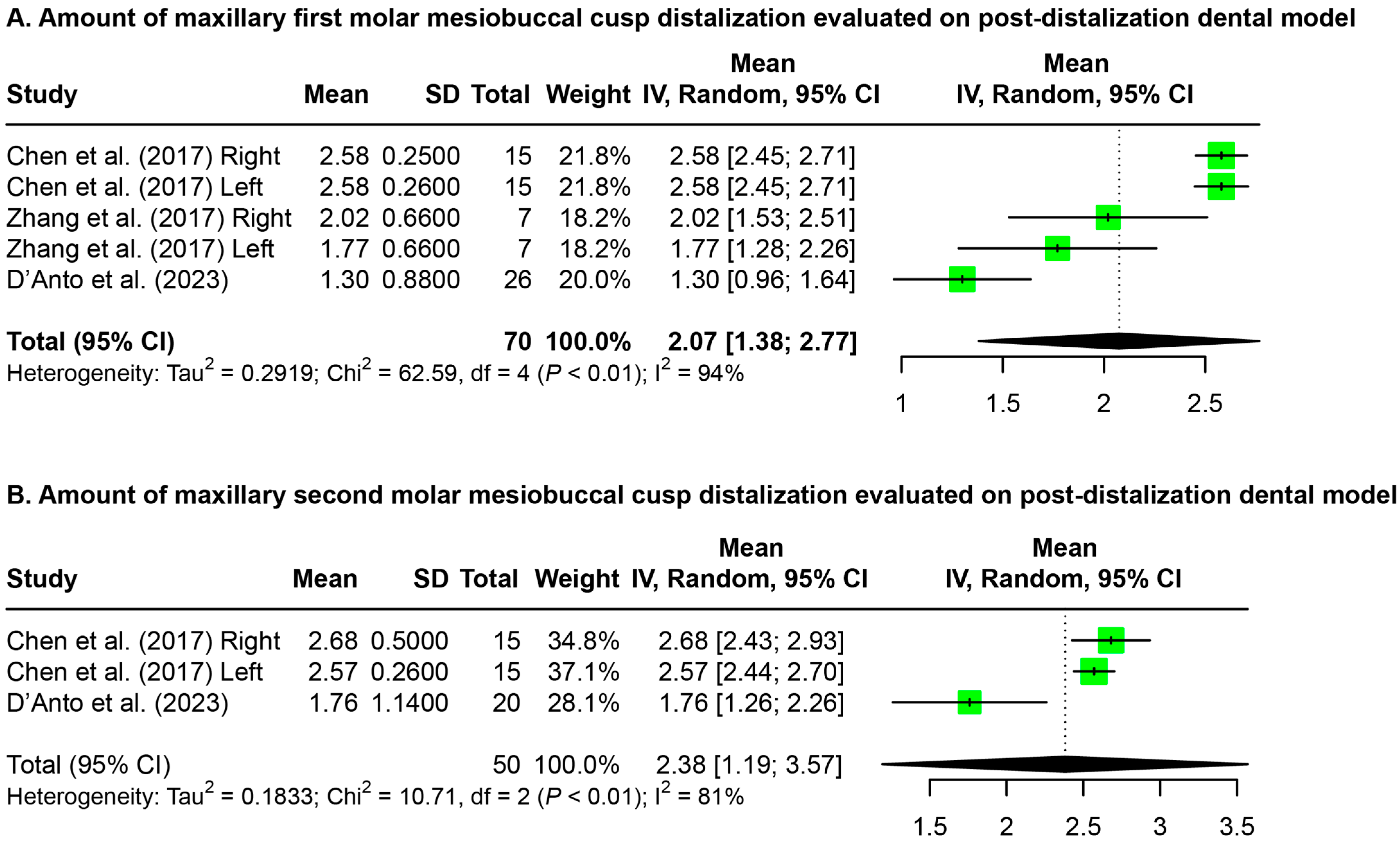
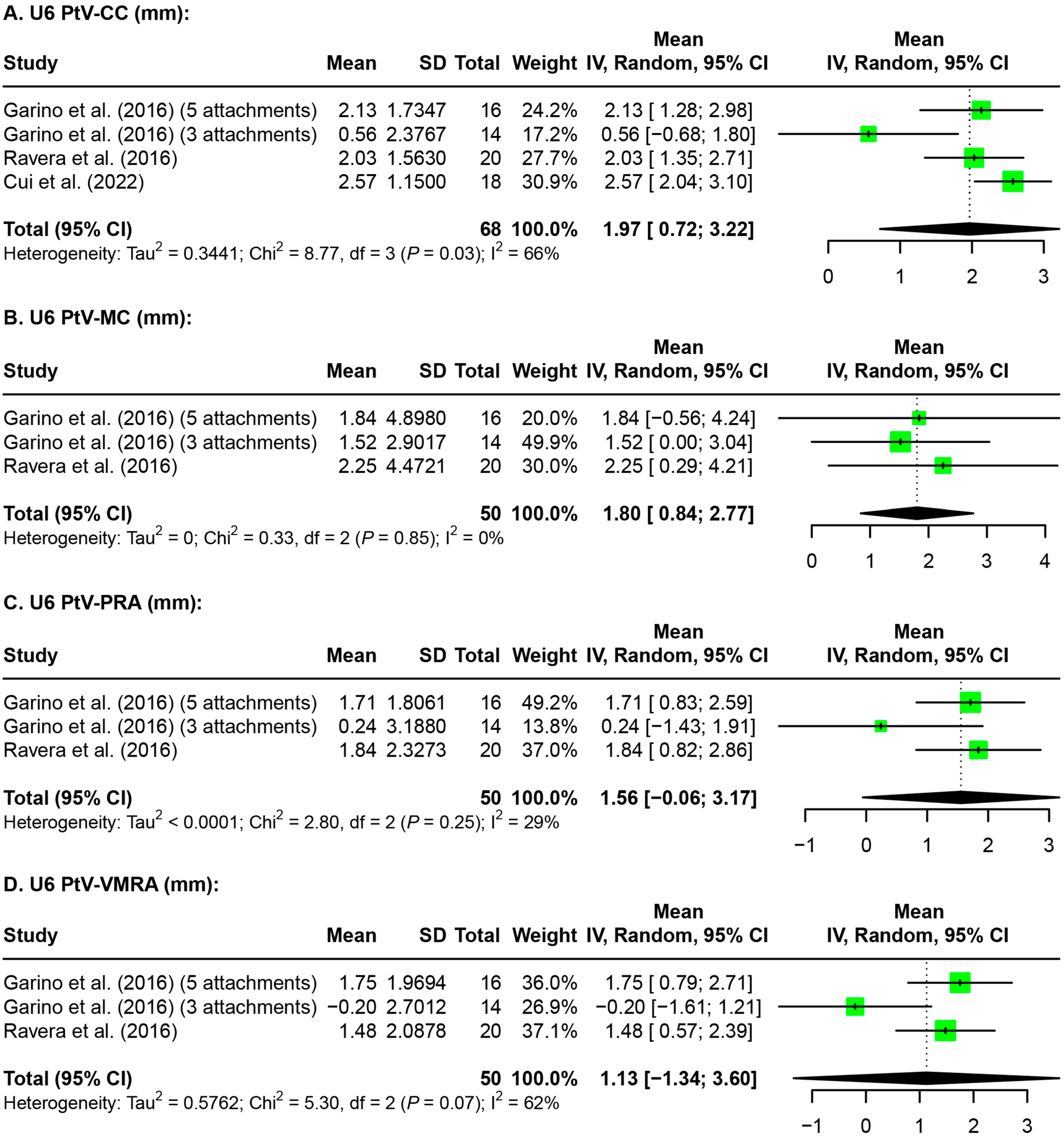
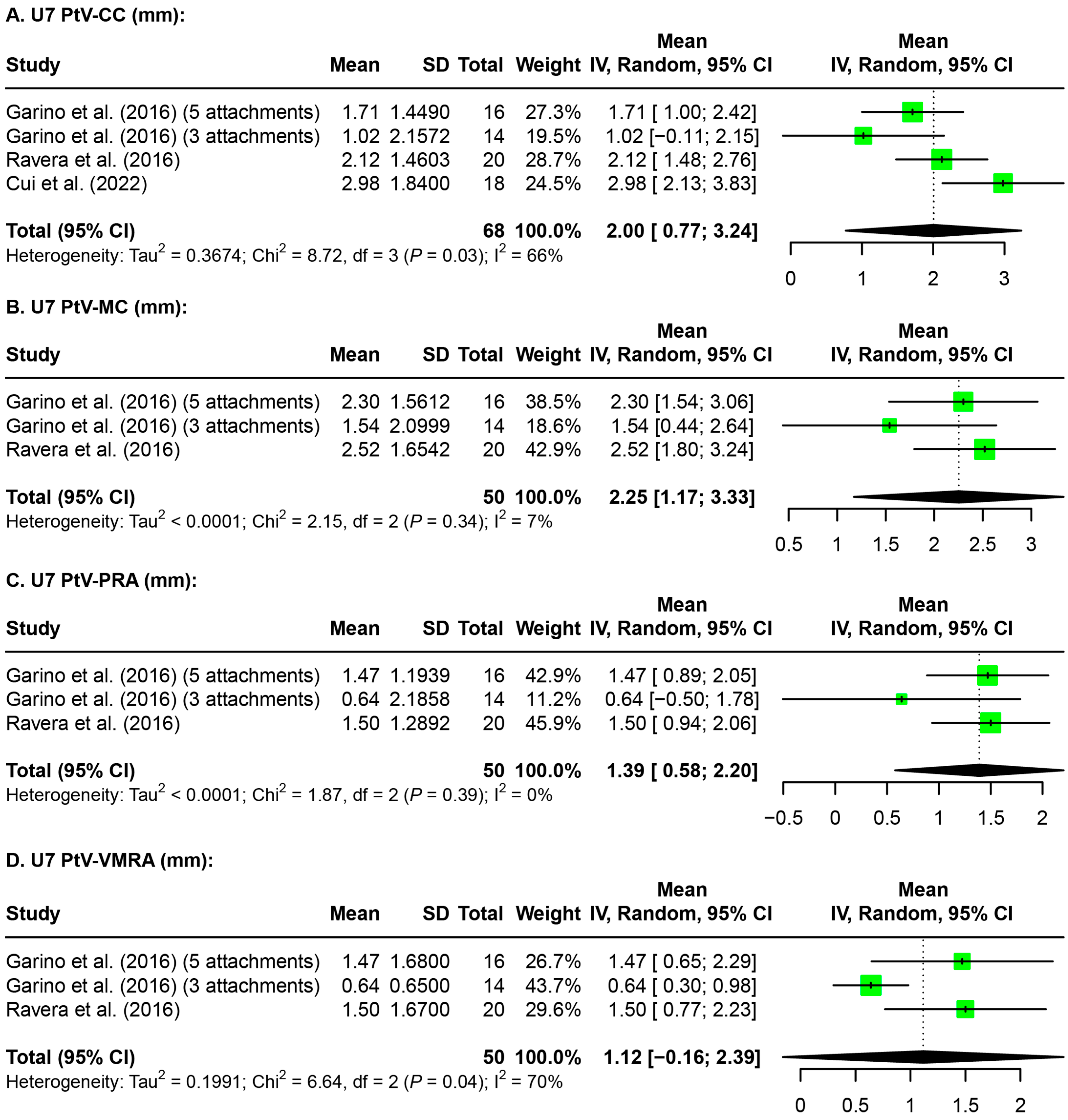
3.4. Maxillary Molar Distalization
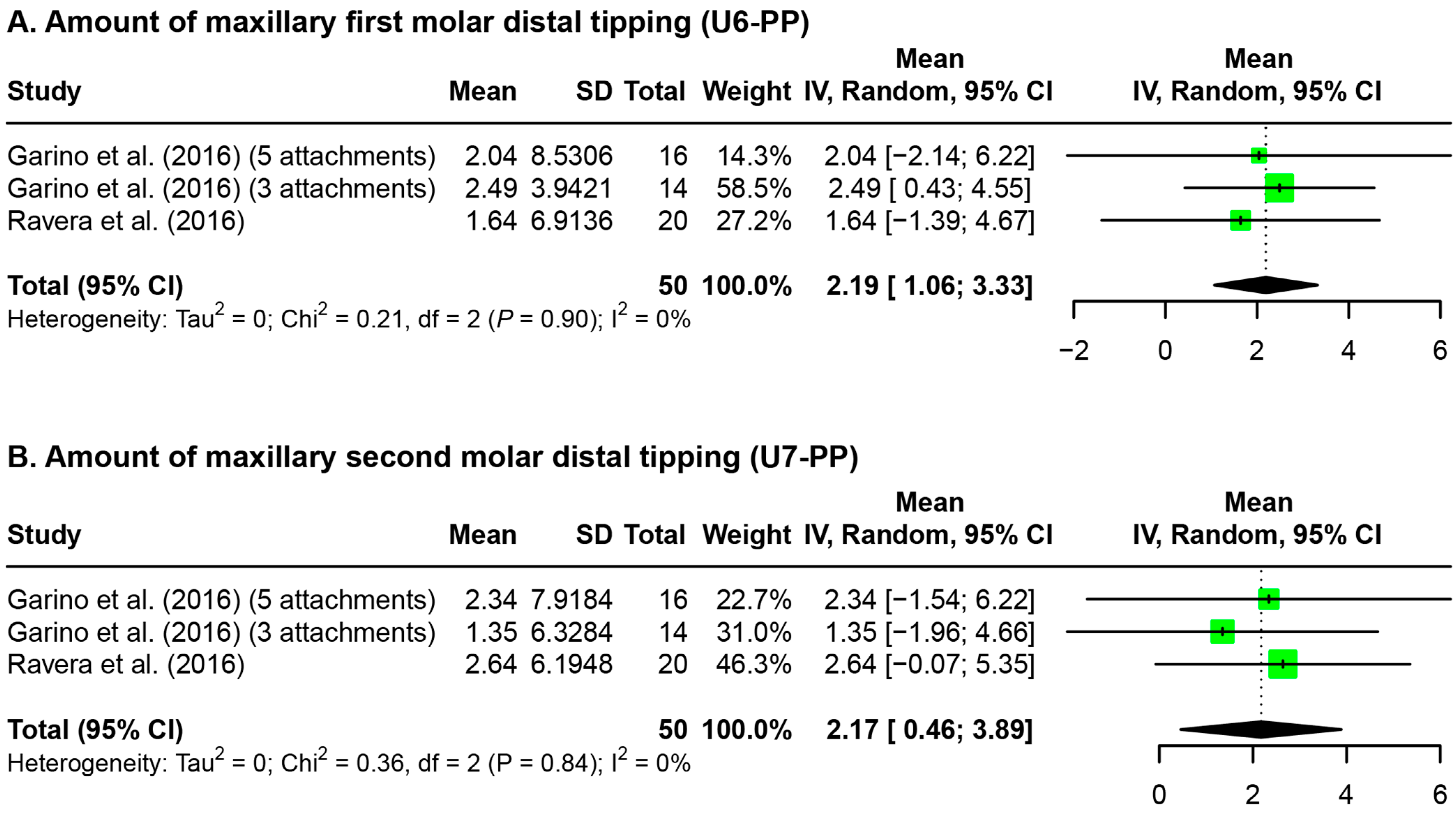
3.5. Maxillary Molar Rotation and Tipping
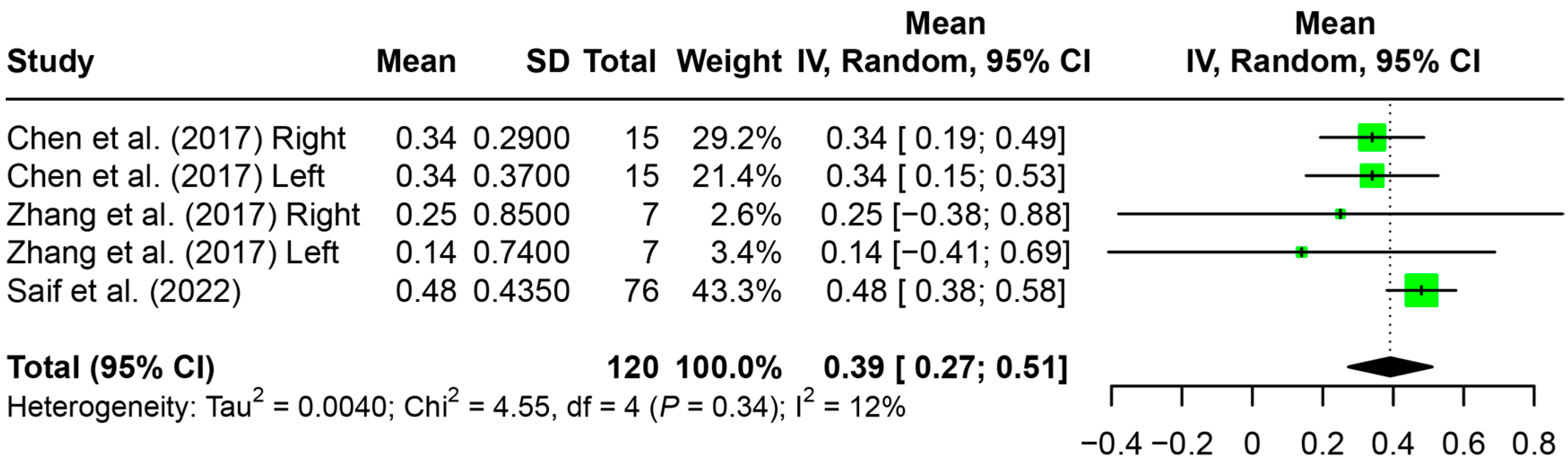
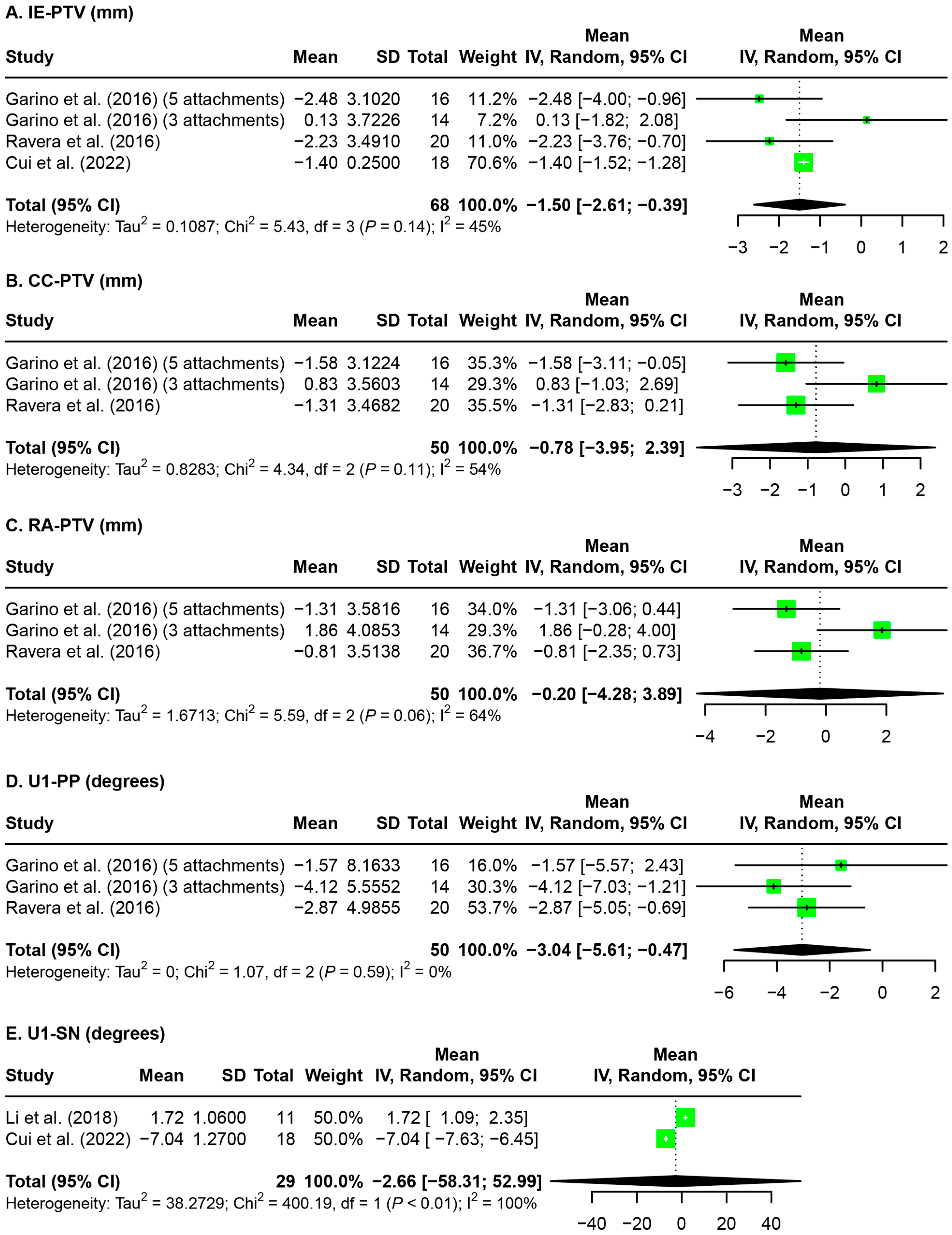
3.6. Anterior Anchorage Loss after Maxillary Molar Distalization
3.7. Mandibular Molar Distalization
4. Discussion
4.1. Summary of Evidence
4.2. Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Janson, G.; Niederberger, A.L.G.; Janson, G.; Valerio, M.V.; Caldas, W.; Valarelli, F.P. Stability of Class II malocclusion treatment with Class II elastics. Am. J. Orthod. Dentofac. Orthop. 2023, 163, 609–617. [Google Scholar] [CrossRef]
- Kim-Berman, H.; McNamara, J.A., Jr.; Lints, J.P.; McMullen, C.; Franchi, L. Treatment effects of the Carriere® Motion 3D appliance for the correction of Class II malocclusion in adolescents. Angle Orthod. 2019, 89, 839–846. [Google Scholar] [CrossRef] [PubMed]
- Aslan, B.I.; Akarslan, Z.Z.; Karadag, O. Effects of Angle class II correction with the Forsus fatigue resistant device on mandibular third molars: A retrospective study. J. Orofac. Orthop. 2021, 82, 403–412. [Google Scholar] [CrossRef] [PubMed]
- Ardeshna, A.; Bogdan, F.; Jiang, S. Class II correction in orthodontic patients utilizing the Mandibular Anterior Repositioning Appliance (MARA). Angle Orthod. 2019, 89, 404–410. [Google Scholar] [CrossRef]
- Taylor, K.L.; Evangelista, K.; Muniz, L.; Ruellas, A.C.O.; Valladares-Neto, J.; McNamara, J., Jr.; Franchi, L.; Kim-Berman, H.; Cevidanes, L.H.S. Three-dimensional comparison of the skeletal and dentoalveolar effects of the Herbst and Pendulum appliances followed by fixed appliances: A CBCT study. Orthod. Craniofac. Res. 2020, 23, 72–81. [Google Scholar] [CrossRef]
- George, S.M.; Campbell, P.M.; Tadlock, L.P.; Schneiderman, E.; Buschang, P.H. Keys to Class II correction: A comparison of 2 extraction protocols. Am. J. Orthod. Dentofac. Orthop. 2021, 159, 333–342. [Google Scholar] [CrossRef] [PubMed]
- Ghosh, J.; Nanda, R.S. Evaluation of an intraoral maxillary molar distalization technique. Am. J. Orthod. Dentofac. Orthop. 1996, 110, 639–646. [Google Scholar] [CrossRef]
- Jones, R.D.; White, J.M. Rapid Class II molar correction with an open-coil jig. J. Clin. Orthod. 1992, 26, 661–664. [Google Scholar]
- Papadopoulos, M.A.; Melkos, A.B.; Athanasiou, A.E. Noncompliance maxillary molar distalization with the first class appliance: A randomized controlled trial. Am. J. Orthod. Dentofac. Orthop. 2010, 137, 586.e1–586.e13; discussion 586–587. [Google Scholar] [CrossRef]
- Bolla, E.; Muratore, F.; Carano, A.; Bowman, S.J. Evaluation of maxillary molar distalization with the distal jet: A comparison with other contemporary methods. Angle Orthod. 2002, 72, 481–494. [Google Scholar] [CrossRef]
- Li, C.; Sfogliano, L.; Jiang, W.; Lee, H.; Zheng, Z.; Chung, C.H.; Jones, J. Total maxillary arch distalization by using headgear in an adult patient. Angle Orthod. 2021, 91, 267–278. [Google Scholar] [CrossRef]
- Quinzi, V.; Marchetti, E.; Guerriero, L.; Bosco, F.; Marzo, G.; Mummolo, S. Dentoskeletal Class II Malocclusion: Maxillary Molar Distalization with No-Compliance Fixed Orthodontic Equipment. Dent. J. 2020, 8, 26. [Google Scholar] [CrossRef] [PubMed]
- Bowman, A.C.; Saltaji, H.; Flores-Mir, C.; Preston, B.; Tabbaa, S. Patient experiences with the Forsus Fatigue Resistant Device. Angle Orthod. 2013, 83, 437–446. [Google Scholar] [CrossRef]
- Hamilton, C.F.; Saltaji, H.; Preston, C.B.; Flores-Mir, C.; Tabbaa, S. Adolescent patients’ experience with the Carriere distalizer appliance. Eur. J. Paediatr. Dent. 2013, 14, 219–224. [Google Scholar]
- Melkos, A.B. Advances in digital technology and orthodontics: A reference to the Invisalign method. Med. Sci. Monit. 2005, 11, PI39–PI42. [Google Scholar]
- Daher, S. Sam Daher’s Techniques for Class II Correction with Invisalign and Elastics; Align Technology: Santa Clara, CA, USA, 2011. [Google Scholar]
- Upadhyay, M.; Arqub, S.A. Biomechanics of clear aligners: Hidden truths & first principles. J. World Fed. Orthod. 2022, 11, 12–21. [Google Scholar]
- D’Anto, V.; Bucci, R.; De Simone, V.; Huanca Ghislanzoni, L.; Michelotti, A.; Rongo, R. Evaluation of Tooth Movement Accuracy with Aligners: A Prospective Study. Materials 2022, 15, 2646. [Google Scholar] [CrossRef] [PubMed]
- D’Anto, V.; Valletta, R.; Ferretti, R.; Bucci, R.; Kirlis, R.; Rongo, R. Predictability of Maxillary Molar Distalization and Derotation with Clear Aligners: A Prospective Study. Int. J. Environ. Res. Public Health 2023, 20, 2941. [Google Scholar] [CrossRef] [PubMed]
- Chen, L.; Wu, J.; Lin, J.; Huang, W.; Xia, Z.; Tan, J. Evaluation of the invisible bracketless appliance on maxillary molar distalization. J. Pract. Stomatol. 2017, 6, 203–207. [Google Scholar]
- Loberto, S.; Paoloni, V.; Pavoni, C.; Cozza, P.; Lione, R. Anchorage Loss Evaluation during Maxillary Molars Distalization Performed by Clear Aligners: A Retrospective Study on 3D Digital Casts. Appl. Sci. 2023, 13, 3646. [Google Scholar] [CrossRef]
- Saif, B.S.; Pan, F.; Mou, Q.; Han, M.; Bu, W.; Zhao, J.; Guan, L.; Wang, F.; Zou, R.; Zhou, H.; et al. Efficiency evaluation of maxillary molar distalization using Invisalign based on palatal rugae registration. Am. J. Orthod. Dentofac. Orthop. 2022, 161, e372–e379. [Google Scholar] [CrossRef] [PubMed]
- Zhang, J.; Zhang, Y.; Liu, Y. Three dimensional evaluation of maxillary molar distal movement using invisible aligners. Chin. J. Orthod. 2017, 24, 70–78. [Google Scholar]
- Patterson, B.D.; Foley, P.F.; Ueno, H.; Mason, S.A.; Schneider, P.P.; Kim, K.B. Class II malocclusion correction with Invisalign: Is it possible? Am. J. Orthod. Dentofac. Orthop. 2021, 159, e41–e48. [Google Scholar] [CrossRef] [PubMed]
- Taffarel, I.A.; Gasparello, G.G.; Mota-Junior, S.L.; Pithon, M.M.; Taffarel, I.P.; Meira, T.M.; Tanaka, O.M. Distalization of maxillary molars with Invisalign aligners in nonextraction patients with Class II malocclusion. Am. J. Orthod. Dentofac. Orthop. 2022, 162, e176–e182. [Google Scholar] [CrossRef] [PubMed]
- Reitan, K. Tissue Rearrangement During Retention of Orthodontically Rotated Teeth. Angle Orthod. 1959, 29, 105–113. [Google Scholar]
- Grunheid, T.; Loh, C.; Larson, B.E. How accurate is Invisalign in nonextraction cases? Are predicted tooth positions achieved? Angle Orthod. 2017, 87, 809–815. [Google Scholar] [CrossRef] [PubMed]
- Liu, X.; Cheng, Y.; Qin, W.; Fang, S.; Wang, W.; Ma, Y.; Jin, Z. Effects of upper-molar distalization using clear aligners in combination with Class II elastics: A three-dimensional finite element analysis. BMC Oral Health 2022, 22, 546. [Google Scholar] [CrossRef]
- Matsumoto, K.; Sherrill-Mix, S.; Boucher, N.; Tanna, N. A cone-beam computed tomographic evaluation of alveolar bone dimensional changes and the periodontal limits of mandibular incisor advancement in skeletal Class II patients. Angle Orthod. 2020, 90, 330–338. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- Ehsani, S.; Nebbe, B.; Normando, D.; Lagravere, M.O.; Flores-Mir, C. Short-term treatment effects produced by the Twin-block appliance: A systematic review and meta-analysis. Eur. J. Orthod. 2015, 37, 170–176. [Google Scholar] [CrossRef]
- Garino, F.; Castroflorio, T.; Daher, S.; Ravera, S.; Rossini, G.; Cugliari, G.; Deregibus, A. Effectiveness of Composite Attachments in Controlling Upper-Molar Movement with Aligners. J. Clin. Orthod. 2016, 50, 341–347. [Google Scholar]
- Ravera, S.; Castroflorio, T.; Garino, F.; Daher, S.; Cugliari, G.; Deregibus, A. Maxillary molar distalization with aligners in adult patients: A multicenter retrospective study. Prog. Orthod. 2016, 17, 12. [Google Scholar] [CrossRef] [PubMed]
- Li, Z.; Wang, W.; Mai, L. The clinical effects of Invisalign-aided molar distalization in the treatment of mild or moderate crowding in anterior teeth. J. Prev. Treat. Stomatol. Dis. 2018, 12, 314–319. [Google Scholar]
- Caruso, S.; Nota, A.; Ehsani, S.; Maddalone, E.; Ojima, K.; Tecco, S. Impact of molar teeth distalization with clear aligners on occlusal vertical dimension: A retrospective study. BMC Oral Health 2019, 19, 182. [Google Scholar] [CrossRef] [PubMed]
- Cui, J.Y.; Ting, L.; Cao, Y.X.; Sun, D.X.; Bing, L.; Wu, X.P. Morphology Changes of Maxillary Molar Distalization by Clear Aligner Therapy. Int. J. Morphol. 2022, 40, 920–926. [Google Scholar] [CrossRef]
- Lin, S.Y.; Hung, M.C.; Lu, L.H.; Sun, J.S.; Tsai, S.J.; Zwei-Chieng Chang, J. Treatment of class II malocclusion with Invisalign(R): A pilot study using digital model-integrated maxillofacial cone beam computed tomography. J. Dent. Sci. 2023, 18, 353–366. [Google Scholar] [CrossRef]
- Wu, D.; Zhao, Y.; Ma, M.; Zhang, Q.; Lei, H.; Wang, Y.; Li, Y.; Chen, X. Efficacy of mandibular molar distalization by clear aligner treatment. Zhong Nan Da Xue Xue Bao Yi Xue Ban 2021, 46, 1114–1121. [Google Scholar] [CrossRef]
- Rota, E.; Parrini, S.; Malekian, K.; Cugliari, G.; Mampieri, G.; Deregibus, A.; Castroflorio, T. Lower Molar Distalization Using Clear Aligners: Bodily Movement or Uprighting? A Preliminary Study. Appl. Sci. 2022, 12, 7123. [Google Scholar] [CrossRef]
- Harrer, M.; Cuijpers, P.; Furukawa, T.A.; Ebert, D.D. Doing Meta-Analysis with R: A Hands-On Guide. Available online: https://dmetar.protectlab.org/ (accessed on 12 February 2024).
- Harrer, M.; Cuijpers, P.; Furukawa, T.; Ebert, D.D. dmetar: Companion R Package for the Guide ‘Doing Meta-Analysis in R’. R Package Version 0.1.0. 2019. Available online: http://dmetar.protectlab.org/ (accessed on 12 February 2024).
- Higgins, J.P.T.; Li, T.; Deeks, J.J. Chapter 6: Choosing effect measures and computing estimates of effect. In Cochrane Handbook for Systematic Reviews of Interventions Version 6.4; Updated August 2023; Higgins, J.P.T., Thomas, J., Chandler, J., Cumpston, M., Li, T., Page, M.J., Welch, V.A., Eds.; Cochrane: Chichester, UK, 2023. [Google Scholar]
- Yang, S. Efficacy of Invisalign on Upper Molar Distalization via CBCT Evaluation; Shanghai Jiaotong University: Shanghai, China, 2015. [Google Scholar]
- Chen, X. The Efficiency of Upper Molar Totally Distalization in Clear System; Shandong University: Jinan, China, 2017. [Google Scholar]
- Jiang, Y. Clinical Study on Stability of Maxillary Molar Distalization with Clear Aligner; Dalian Medical University: Dalian, China, 2018. [Google Scholar]
- Nguyen, M.P. Evaluation of Dental and Skeletal Changes with Sequential Distalization of Maxillary Molars Using Clear Aligners: A Preliminary Study. Master’s Thesis, West Virginia University, Morgantown, WV, USA, 2021. [Google Scholar]
- Society of Orthodontics, Chinese Stomatological Association. Guidelines for clear aligner orthodontic treatment. Zhonghua Kou Qiang Yi Xue Za Zhi 2021, 56, 983–988. [Google Scholar] [CrossRef]
- Gu, Z.X. Clear aligner therapy: Anchorage management and clinical strategies. Zhonghua Kou Qiang Yi Xue Za Zhi 2020, 55, 531–535. [Google Scholar]
- Shi, X.; Mao, J.; Liu, Y. Clinical efficacy and influencing factors of molar distalization with clear aligner. Zhonghua Kou Qiang Yi Xue Za Zhi 2022, 57, 762–768. [Google Scholar] [PubMed]
- Rongo, R.; Dianiskova, S.; Spiezia, A.; Bucci, R.; Michelotti, A.; D’Anto, V. Class II Malocclusion in Adult Patients: What Are the Effects of the Intermaxillary Elastics with Clear Aligners? A Retrospective Single Center One-Group Longitudinal Study. J. Clin. Med. 2022, 11, 7333. [Google Scholar] [CrossRef] [PubMed]
- Cheng, X.Y.; Sang, T.; Wu, J. Cone-beam CT evaluation of the effect of indirect anchorage of mini-screw assisted clear aligner on molar distalization. Zhonghua Kou Qiang Yi Xue Za Zhi 2022, 57, 724–732. [Google Scholar] [CrossRef] [PubMed]
- Li, L.; Guo, R.; Zhang, L.; Huang, Y.; Jia, Y.; Li, W. Maxillary molar distalization with a 2-week clear aligner protocol in patients with Class II malocclusion: A retrospective study. Am. J. Orthod. Dentofac. Orthop. 2023, 164, 123–130. [Google Scholar] [CrossRef] [PubMed]
- Miao, Z.; Zhang, H.; Yang, Y.; Han, Y.; Leng, J.; Wang, S. Influence of maxillary molar distalization with clear aligners on three-dimensional direction: Molar distal movement, intrusion, distal tip and crown buccal torque. Prog. Orthod. 2023, 24, 48. [Google Scholar] [CrossRef] [PubMed]
- Chen, X.; Shi, Y.; Yuan, J.; Li, Y.; Chen, W. Factors influencing the efficacy of invisalign in molar distalization and tooth movement. Front. Bioeng. Biotechnol. 2023, 11, 1215169. [Google Scholar] [CrossRef] [PubMed]
- Han, J.; Ning, N.; Du, H.; Zhou, M.; Cai, C.; Hong, Y.; Zhou, Y.; Chen, X. Efficacy of clear aligners on mandibular molar distalization: A retrospective study. Digit. Med. 2021, 7, 1–11. [Google Scholar] [CrossRef]
- Abdelhady, N.A.; Tawfik, M.A.; Hammad, S.M. Maxillary molar distalization in treatment of angle class II malocclusion growing patients: Uncontrolled clinical trial. Int. Orthod. 2020, 18, 96–104. [Google Scholar] [CrossRef] [PubMed]
- Lombardo, L.; Arreghini, A.; Ramina, F.; Huanca Ghislanzoni, L.T.; Siciliani, G. Predictability of orthodontic movement with orthodontic aligners: A retrospective study. Prog. Orthod. 2017, 18, 35. [Google Scholar] [CrossRef]
- Ren, Y.; Song, B.; Feng, Y.; Pu, P.; Gu, Z. Three-dimensional model superimposition study on efficiency of molar distalization by using removable clear appliance combined with micro-implant anchorage. Chin. J. Orthod. 2018, 25, 92–97. [Google Scholar]
- Zhou, J.M.; Bai, Y.X.; Hao, W.S. Three dimensional evaluation of maxillary molar distal movement using invisible bracketless appliance. Beijing J. Stomatol. 2011, 19, 157–159. [Google Scholar]
- Charalampakis, O.; Iliadi, A.; Ueno, H.; Oliver, D.R.; Kim, K.B. Accuracy of clear aligners: A retrospective study of patients who needed refinement. Am. J. Orthod. Dentofac. Orthop. 2018, 154, 47–54. [Google Scholar] [CrossRef] [PubMed]
- Haouili, N.; Kravitz, N.D.; Vaid, N.R.; Ferguson, D.J.; Makki, L. Has Invisalign improved? A prospective follow-up study on the efficacy of tooth movement with Invisalign. Am. J. Orthod. Dentofac. Orthop. 2020, 158, 420–425. [Google Scholar] [CrossRef]
- Al-Nadawi, M.; Kravitz, N.D.; Hansa, I.; Makki, L.; Ferguson, D.J.; Vaid, N.R. Effect of clear aligner wear protocol on the efficacy of tooth movement. Angle Orthod. 2021, 91, 157–163. [Google Scholar] [CrossRef]
- Bowman, E.; Bowman, P.; Weir, T.; Dreyer, C.W.; Meade, M.J. Evaluation of the predicted vs. achieved occlusal outcomes with the Invisalign(R) appliance: A retrospective investigation of adult patients. Int. Orthod. 2023, 21, 100746. [Google Scholar] [CrossRef] [PubMed]
- Lione, R.; Paoloni, V.; De Razza, F.C.; Pavoni, C.; Cozza, P. The Efficacy and Predictability of Maxillary First Molar Derotation with Invisalign: A Prospective Clinical Study in Growing Subjects. Appl. Sci. 2022, 12, 2670. [Google Scholar] [CrossRef]
- Balboni, A.; Cretella Lombardo, E.; Balboni, G.; Gazzani, F. Vertical effects of distalization protocol with Clear aligners in Class II patients: A prospective study. Minerva Dent. Oral Sci. 2023, 72, 291–297. [Google Scholar] [CrossRef] [PubMed]
- Simon, M.; Keilig, L.; Schwarze, J.; Jung, B.A.; Bourauel, C. Treatment outcome and efficacy of an aligner technique--regarding incisor torque, premolar derotation and molar distalization. BMC Oral Health 2014, 14, 68. [Google Scholar] [CrossRef] [PubMed]
- Peng, Y.; Li, X. Effect of molar distalization with clear aligners on occlusal vertical dimension in different vertical craniofacial patterns. Chin. J. Tissue Eng. Res. 2024, 28, 4559–4564. [Google Scholar]
- Lin, L.; Li, C.; Chen, S.H.; Boucher, N.S.; Chung, C.H. Transverse growth of the mandibular body in untreated children: A longitudinal CBCT study. Clin. Oral Investig. 2023, 27, 2097–2107. [Google Scholar] [CrossRef]
- Fontana, M.; Cozzani, M.; Mutinelli, S.; Spena, R.; Caprioglio, A. Maxillary molar distalization therapy in adult patients: A multicentre study. Orthod. Craniofac. Res. 2015, 18, 221–231. [Google Scholar] [CrossRef] [PubMed]
- Fontana, M.; Cozzani, M.; Caprioglio, A. Soft tissue, skeletal and dentoalveolar changes following conventional anchorage molar distalization therapy in class II non-growing subjects: A multicentric retrospective study. Prog. Orthod. 2012, 13, 30–41. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Criteria | Description |
|---|---|
| Population | Patients undergoing orthodontic treatment with clear aligners requiring molar distalization |
| Intervention | Molar distalization with sequential distalization protocol of clear aligner therapy |
| Comparisons | The control is pre-treatment models and radiographs |
| Outcome | The amount of molar distalization, molar rotation, molar tipping, and anterior anchorage loss achieved during molar distalization with clear aligners |
| Maxillary | Mandibular | |||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Garino et al. (2016) [32] | Ravera et al. (2016) [33] | Chen et al. (2017) [20] | Zhang et al. (2017) [23] | Li et al. (2018) [34] | Caruso et al. (2019) [35] | Cui et al. (2022) [36] | Saif et al. (2022) [22] | D’Anto et al. (2023) [19] | Lin et al. (2023) [37] | Loberto et al. (2023) [21] | Wu et al. (2021) [38] | Rota et al. (2022) [39] | ||
| 1. Study Design (6) | A. Objective: objective clearly formulated | ⊕ | ⊕ | ⊕ | ⊕ | ⊕ | ⊕ | ⊕ | ⊕ | ⊕ | ⊕ | ⊕ | ⊕ | ⊕ |
| B. Sample size: considered adequate and estimated before collection of data | ⊕ | ⊕ | ? | ⊖ | ? | ? | ? | ⊕ | ? | ⊖ | ⊕ | ? | ⊕ | |
| C. Baseline characteristics: similar baseline characteristics | ⊕ | ⊕ | ? | ? | ⊕ | ? | ⊕ | ⊕ | ⊕ | ⊕ | ⊕ | ⊕ | ⊕ | |
| D. Co-interventions | ⊕ | ⊕ | ⊕ | ⊕ | ⊕ | ⊕ | ⊕ | ? | ⊕ | ⊕ | ⊕ | ⊕ | ⊕ | |
| E. Randomization | ||||||||||||||
| Random sampling | ⊕ | ⊖ | ⊖ | ⊖ | ⊖ | ⊖ | ⊖ | ⊖ | ⊖ | ⊖ | ⊖ | ⊖ | ⊖ | |
| Random allocation of treatment | ⊕ | ⊖ | ⊖ | ⊖ | ⊖ | ⊖ | ⊖ | ⊖ | ⊖ | ⊖ | ⊖ | ⊖ | ⊖ | |
| 2. Study Measurements (5) | F. Measurement method: appropriate to the objective | ⊕ | ⊕ | ⊕ | ⊕ | ? | ⊕ | ⊕ | ⊕ | ⊕ | ⊕ | ⊕ | ⊕ | ⊕ |
| G. Blind measurement: blinding | ||||||||||||||
| Blinding (examiner) | ⊕ | ⊕ | ⊖ | ⊖ | ⊖ | ⊕ | ⊖ | ⊖ | ⊖ | ⊖ | ⊖ | ⊖ | ⊕ | |
| Blinding (statistician) | ⊕ | ⊖ | ⊖ | ⊖ | ⊖ | ⊖ | ⊖ | ⊖ | ⊖ | ⊖ | ⊖ | ⊖ | ⊖ | |
| H. Reliability | ||||||||||||||
| Reliability described? (intra-rater reliability) | ⊕ | ⊕ | ⊖ | ? | ⊖ | ⊕ | ⊖ | ⊕ | ⊕ | ⊕ | ⊕ | ⊖ | ⊖ | |
| Adequate level of agreement? (inter-rater reliability) | ⊖ | ⊕ | ⊖ | ⊖ | ⊖ | ⊖ | ⊖ | ⊕ | ⊕ | ⊖ | ⊖ | ⊖ | ⊖ | |
| 3. Statistical Analysis (5) | I. Statistical analysis | |||||||||||||
| Appropriate for data | ⊕ | ⊕ | ⊕ | ⊖ | ⊖ | ⊕ | ⊕ | ⊕ | ⊕ | ⊕ | ⊕ | ⊖ | ⊕ | |
| Combined subgroup analysis | ⊕ | ⊕ | ⊕ | ⊖ | ⊖ | ⊕ | ⊕ | ⊕ | ⊕ | ⊕ | ⊕ | ⊖ | ⊕ | |
| J. Cofounders (co-interventions): confounders included in the analysis | ⊕ | ⊕ | ⊖ | ⊖ | ⊖ | ⊕ | ⊕ | ? | ⊕ | ⊕ | ⊕ | ⊖ | ⊕ | |
| K. Statistical significance level | ||||||||||||||
| p-value stated? | ⊕ | ⊕ | ⊕ | ⊖ | ⊕ | ⊕ | ⊕ | ⊕ | ⊕ | ⊕ | ⊕ | ⊕ | ⊕ | |
| Confidence intervals stated? | ⊖ | ⊕ | ⊖ | ⊖ | ⊖ | ⊖ | ⊖ | ⊖ | ⊕ | ⊖ | ⊕ | ⊖ | ⊕ | |
| 4. Other | L. Clinical significance | ⊕ | ⊕ | ⊕ | ? | ⊕ | ⊕ | ⊕ | ⊕ | ⊕ | ⊕ | ⊕ | ⊕ | ⊕ |
| Total score | 15 | 14 | 7 | 3 | 5 | 10 | 9 | 10 | 12 | 10 | 12 | 6 | 12 | |
| Percentage of the total | 88.24 | 82.35 | 41.18 | 17.65 | 29.41 | 58.82 | 52.94 | 58.82 | 70.59 | 58.82 | 70.59 | 35.29 | 70.59 | |
| Risk of bias | MED | MED | MED | HIGH | HIGH | HIGH | HIGH | MED | MED | HIGH | HIGH | HIGH | HIGH | |
| Study | Study Type | Maxillary or Mandibular | Patient Age (Years) | Sample Size (F/M) | Clear Aligner Brand | Post-Distalization Records | Post-Treatment Records | ||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Digital Model | Lateral Ceph | CBCT | Digital Model | Lateral Ceph | CBCT | ||||||
| Garino et al. (2016) [32] | Prospective | Maxillary | 30.5 | 30 (18F/12M) | Invisalign | - | - | - | N | Y | N |
| Ravera et al. (2016) [33] | Retrospective | Maxillary | 29.73 ± 6.89 | 20 (11F/8M) | Invisalign | - | - | - | N | Y | N |
| Chen et al. (2017) [20] | Unclear | Maxillary | 25.3 (14–43) | 15 | Invisalign | Y | N | N | - | - | - |
| Zhang et al. (2017) [23] | Unclear | Maxillary | 14.0 ± 3.1 | 7 (5F/2M) | Angel Aligner | Y | N | N | - | - | - |
| Li et al. (2018) [34] | Unclear | Maxillary | 25.3 (21–34) | 11 (7F/4M) | Unclear | - | - | - | Y | Y | N |
| Caruso et al. (2019) [35] | Retrospective | Maxillary | 22.7 ± 5.3 | 10 (8F/2M) | Invisalign | - | - | - | N | Y | N |
| Cui et al. (2022) [36] | Retrospective | Maxillary | 27.8 ± 5.38 (18–38) | 18 | Unclear | - | - | - | N | N | Y |
| Saif et al. (2022) [22] | Prospective | Maxillary | 25.4 (17–39) | 38 (34F/4M) | Invisalign | Y | N | N | - | - | - |
| D’Anto et al. (2023) [19] | Prospective | Maxillary | 25.7 ± 8.8 (18–45.5) | 16 (12F/4M) | Ordoline aligner | Y | N | N | - | - | - |
| Lin et al. (2023) [37] | Retrospective | Maxillary | 26.64 ± 3.02 (23.1–31.5) | 7 | Invisalign | - | - | - | Y | N | Y |
| Loberto et al. (2023) [21] | Prospective | Maxillary | 14.9 ± 6 | 49 (27F/22M) | Invisalign | Y | N | N | - | - | - |
| Wu et al. (2021) [38] | Prospective | Mandibular | >18 | 20 (12F/8M) | Invisalign | N | N | Y | - | - | - |
| Rota et al. (2022) [39] | Retrospective | Mandibular | 25.6 ± 4.5 | 16 (8F/8M) | Invisalign | - | - | - | N | Y | N |
| Time Points | Tooth | Parameters | References | Amount of Distalization |
|---|---|---|---|---|
| Post-distalization | U6 1 | MB 3 cusp (mm) | Chen et al. (2017) Right [20] | 2.58 ± 0.25 |
| Chen et al. (2017) Left [20] | 2.58 ± 0.26 | |||
| Zhang et al. (2017) Right [23] | 2.02 ± 0.66 * | |||
| Zhang et al. (2017) Left [23] | 1.77 ± 0.66 * | |||
| D’Anto et al. (2023) [19] | 1.30 ± 0.88 | |||
| Loberto et al. (2023) Right [21] | 2.4 | |||
| Loberto et al. (2023) Left [21] | 2.4 | |||
| DB 4 cusp (mm) | D’Anto et al. (2023) [19] | 1.42 ± 0.94 | ||
| Loberto et al. (2023) Right [21] | 3.0 | |||
| Loberto et al. (2023) Left [21] | 2.2 | |||
| CC 5 (mm) | Saif et al. (2022) [22] | 1.81 ± 0.84 | ||
| U7 2 | MB cusp (mm) | Chen et al. (2017) Right [20] | 2.68 ± 0.50 | |
| Chen et al. (2017) Left [20] | 2.57 ± 0.26 | |||
| D’Anto et al. (2023) [19] | 1.76 ± 1.14 | |||
| DB cusp (mm) | D’Anto et al. (2023) [19] | 1.54 ± 1.13 | ||
| CC (mm) | Saif et al. (2022) [22] | 1.85 ± 0.88 | ||
| Post-treatment | U6 | Molar sagittal distance (mm) | Li et al. (2018) [34] | 2.12 ± 1.09 |
| MB cusp (mm) | Lin et al. (2023) [37] | 0.67 ± 0.50 $ | ||
| DB cusp (mm) | Lin et al. (2023) [37] | 0.84 ± 0.60 $ | ||
| MP cusp 6 (mm) | Lin et al. (2023) [37] | 0.36 ± 0.40 $ |
| Time Points | Tooth | Parameters | References | Amount of Distalization |
|---|---|---|---|---|
| Post-treatment | U6 1 | PtV-CC 3 (mm) | Garino et al. (2016) (5 attachments) [32] | 2.13 [1.28, 2.98] |
| Garino et al. (2016) (3 attachments) [32] | 0.56 [−0.68, 1.81] | |||
| Ravera et al. (2016) [33] | 2.03 [1.35, 2.72] | |||
| Cui et al. (2022) [36] | 2.57 ± 1.15 * | |||
| PtV-MC 4 (mm) | Garino et al. (2016) (5 attachments) [32] | 1.84 [−0.56, 4.24] | ||
| Garino et al. (2016) (3 attachments) [32] | 1.52 [−0.07, 2.97] | |||
| Ravera et al. (2016) [33] | 2.25 [0.29, 4.21] | |||
| PtV-PRA 5 (mm) | Garino et al. (2016) (5 attachments) [32] | 1.71 [0.83, 2.60] | ||
| Garino et al. (2016) (3 attachments) [32] | 0.24 [−1.43, 1.91] | |||
| Ravera et al. (2016) [33] | 1.84 [0.82, 2.86] | |||
| PtV-VMRA 6 (mm) | Garino et al. (2016) (5 attachments) [32] | 1.75 [0.78, 2.71] | ||
| Garino et al. (2016) (3 attachments) [32] | −0.20 [−1.62, 1.21] | |||
| Ravera et al. (2016) [33] | 1.48 [0.57, 2.40] | |||
| UMD 7 (mm) | Li et al. (2018) [34] | 2.32 ± 0.84 | ||
| U7 2 | PtV-CC (mm) | Garino et al. (2016) (5 attachments) [32] | 1.71 [1.00, 2.42] | |
| Garino et al. (2016) (3 attachments) [32] | 1.02 [−0.11, 2.15] | |||
| Ravera et al. (2016) [33] | 2.12 [1.48, 2.76] | |||
| Cui et al. (2022) [36] | 2.98 ± 1.84 * | |||
| PtV-MC (mm) | Garino et al. (2016) (5 attachments) [32] | 2.30 [1.53, 3.06] | ||
| Garino et al. (2016) (3 attachments) [32] | 1.54 [0.44, 2.64] | |||
| Ravera et al. (2016) [33] | 2.52 [1.79, 3.24] | |||
| PtV-PRA (mm) | Garino et al. (2016) (5 attachments) [32] | 1.47 [0.89, 2.06] | ||
| Garino et al. (2016) (3 attachments) [32] | 0.64 [−0.51, 1.78] | |||
| Ravera et al. (2016) [33] | 1.50 [0.94, 2.07] | |||
| PtV-VMRA (mm) | Garino et al. (2016) (5 attachments) [32] | 1.68 [1.10, 2.25] | ||
| Garino et al. (2016) (3 attachments) [32] | 0.65 [−0.55, 1.86] | |||
| Ravera et al. (2016) [33] | 1.67 [1.03, 2.31] |
| Time Points | Tooth | Parameters | References | Distal In–Mesial out Rotation |
|---|---|---|---|---|
| Post-distalization | U6 1 | MB-DP 3 (°) | Chen et al. (2017) Right [20] | 0.93 ± 3.51 |
| Chen et al. (2017) Left [20] | 0.75 ± 1.74 | |||
| DB-MP 4 (°) | D’Anto et al. (2023) [19] | 8.09 ± 4.80 | ||
| U7 2 | MB-DP (°) | Chen et al. (2017) Right [20] | 0.85 ± 2.20 | |
| Chen et al. (2017) Left [20] | 0.86 ± 2.16 | |||
| DB-MP (°) | D’Anto et al. (2023) [19] | 6.40 ± 4.14 | ||
| Post-treatment | U6 | Molar rotation (°) | Li et al. (2018) [34] | 3.77 ± 4.88 |
| Time Points | Tooth | Parameters | References | Distal Tipping |
|---|---|---|---|---|
| Post-treatment | U6 1 | UM-SN 3 (°) | Li et al. (2018) [34] | 3.83 ± 1.37 |
| U6-SN 4 (°) | Cui et al. (2022) [36] | 3.43 ± 2.71 * | ||
| U6-PP 5 (°) | Garino et al. (2016) (5 attachments) [32] | 2.04 [−2.14, 6.22] | ||
| Garino et al. (2016) (3 attachments) [32] | 2.49 [0.42, 4.55] | |||
| Ravera et al. (2016) [33] | 1.64 [−1.39, 4.67] | |||
| Caruso et al. (2019) [35] | 1.3 & | |||
| Distal tipping (evaluated on the dental model, °) | Zhang et al. (2017) Right [23] | 5.70 ± 3.03 $ | ||
| Zhang et al. (2017) Left [23] | 4.09 ± 3.30 $ | |||
| U7 2 | U7-SN 6 (°) | Cui et al. (2022) [36] | 4.34 ± 3.28 * | |
| U7-PP 7 (°) | Garino et al. (2016) (5 attachments) [32] | 2.34 [−1.54, 6.22] | ||
| Garino et al. (2016) (3 attachments) [32] | 1.35 [−1.97, 4.66] | |||
| Ravera et al. (2016) [33] | 2.64 [−0.06, 5.37] | |||
| Caruso et al. (2019) [35] | −0.6 & |
| Time Points | Arch | Parameters | References | Amount of Change |
|---|---|---|---|---|
| Post-distalization | Same arch | U1 1 protrusion (mm) | Chen et al. (2017) Right [20] | 0.34 ± 0.29 |
| Chen et al. (2017) Left [20] | 0.34 ± 0.37 | |||
| Zhang et al. (2017) Right [23] | 0.25 ± 0.85 * | |||
| Zhang et al. (2017) Left [23] | 0.14 ± 0.74 * | |||
| Saif et al. (2022) [22] | 0.48 ± 0.435 | |||
| U2 2 protrusion (mm) | Saif et al. (2022) [22] | 0.45 ± 0.384 | ||
| U3 3 mesialization (mm) | Loberto et al. (2023) Right [21] | 1.5 | ||
| Loberto et al. (2023) Left [21] | 1.15 | |||
| Saif et al. (2022) [22] | 0.27 ± 0.250 | |||
| U1 proclination (°) | Zhang et al. (2017) Right [23] | −1.94 ± 2.61 * | ||
| Zhang et al. (2017) Left [23] | −1.02 ± 2.55 * | |||
| Post-treatment | Opposing arch | L1s 4 incisal edge (mm) | Lin et al. (2023) [37] | 1.21 ± 0.86 & |
| Same arch | U1 incisal edge (mm) | Lin et al. (2023) [37] | −0.81 ± 0.89 & |
| Time Points | Arch | Parameters | References | Amount of Change |
|---|---|---|---|---|
| Post-treatment | Same arch | IE-PTV 1 (mm) | Garino et al. (2016) (5 attachments) [32] | −2.48 [−4.00, −0.96] |
| Garino et al. (2016) (3 attachments) [32] | 0.13 [−1.82, 2.08] | |||
| Ravera et al. (2016) [33] | −2.23 [−3.76, −0.70] | |||
| Cui et al. (2022) [36] | −1.40 ± 0.25 & | |||
| CC-PTV 2 (mm) | Garino et al. (2016) (5 attachments) [32] | −1.58 [−3.11, −0.05] | ||
| Garino et al. (2016) (3 attachments) [32] | 0.83 [−1.04, 2.69] | |||
| Ravera et al. (2016) [33] | −1.31 [−2.83, 0.21] | |||
| RA-PTV 3 (mm) | Garino et al. (2016) (5 attachments) [32] | −1.31 [−3.06, 0.45] | ||
| Garino et al. (2016) (3 attachments) [32] | 1.86 [−0.28, 4.00] | |||
| Ravera et al. (2016) [33] | −0.81 [−2.35, 0.73] | |||
| U1D 4 (mm) | Li et al. (2018) [34] | 1.45 ± 0.94 | ||
| U1-PP 5 (°) | Garino et al. (2016) (5 attachments) [32] | −1.57 [−5.57, 2.43] | ||
| Garino et al. (2016) (3 attachments) [32] | −4.12 [−7.03, −1.21] | |||
| Ravera et al. (2016) [33] | −2.87 [−5.06, −0.69] | |||
| Caruso et al. (2019) [35] | −13.5 * | |||
| U1-SN 6 (°) | Li et al. (2018) [34] | 1.72 ± 1.06 | ||
| Cui et al. (2022) [36] | −7.04 ± 1.27 & | |||
| Lin et al. (2023) [37] | −5.03 * | |||
| Opposing arch | L1-MP 7 (°) | Li et al. (2018) [34] | 3.82 ± 2.19 | |
| Lin et al. (2023) [37] | 6.57 * |
| Time Points | Tooth | Parameters | References | Amount of Distalization |
|---|---|---|---|---|
| Post-distalization | L6 1 | MBC 3 (mm) | Wu et al. (2021) [38] | 0.78 ± 0.33 |
| DBC 4 (mm) | Wu et al. (2021) [38] | 0.91 ± 0.31 | ||
| MLC 5 (mm) | Wu et al. (2021) [38] | 0.56 ± 0.89 | ||
| DLC 6 (mm) | Wu et al. (2021) [38] | 0.62 ± 0.84 | ||
| MRA 7 (mm) | Wu et al. (2021) [38] | 0.29 ± 1.08 | ||
| DRA 8 (mm) | Wu et al. (2021) [38] | 0.28 ± 0.66 | ||
| CC 9 (mm) | Wu et al. (2021) [38] | 0.53 ± 1.37 | ||
| RC 10 (mm) | Wu et al. (2021) [38] | 0.41 ± 0.96 | ||
| L7 2 | MBC (mm) | Wu et al. (2021) [38] | 0.81 ± 1.46 | |
| DBC (mm) | Wu et al. (2021) [38] | 1.06 ± 0.65 | ||
| MLC (mm) | Wu et al. (2021) [38] | 0.64 ± 1.19 | ||
| DLC (mm) | Wu et al. (2021) [38] | 0.72 ± 1.07 | ||
| MRA (mm) | Wu et al. (2021) [38] | 0.30 ± 1.01 | ||
| DRA (mm) | Wu et al. (2021) [38] | 0.27 ± 0.82 | ||
| CC (mm) | Wu et al. (2021) [38] | 0.59 ± 0.94 | ||
| RC (mm) | Wu et al. (2021) [38] | 0.56 ± 0.91 | ||
| Post-treatment | L6 | mc-CoGo 11 (mm) | Rota et al. (2022) [39] | 1.07 ± 1.61 (SE) |
| cc-CoGo 12 (mm) | Rota et al. (2022) [39] | 1.16 ± 1.49 (SE) | ||
| mra-CoGo 13 (mm) | Rota et al. (2022) [39] | 0.15 ± 1.71 (SE) | ||
| L7 | mc-CoGo (mm) | Rota et al. (2022) [39] | 1.79 ± 1.57 (SE) | |
| cc-CoGo (mm) | Rota et al. (2022) [39] | 2.47 ± 1.48 (SE) | ||
| mra-CoGo (mm) | Rota et al. (2022) [39] | 0.85 ± 1.63 (SE) |
| Time Points | Tooth | Parameters | References | Distal Tipping |
|---|---|---|---|---|
| Post-distalization | L6 1 | L6 inclination (°) | Wu et al. (2021) [38] | 1.62 ± 1.06 |
| L7 2 | L7 inclination (°) | Wu et al. (2021) [38] | 2.10 ± 1.74 | |
| Post-treatment | L6 | ax-CoGo 3 (°) | Rota et al. (2022) [39] | 4.56 ± 2.03 (SE) |
| ax-GoMe 4 (°) | Rota et al. (2022) [39] | 5.03 ± 1.59 (SE) | ||
| L7 | ax-CoGo (°) | Rota et al. (2022) [39] | 4.56 ± 4.15 (SE) | |
| ax-GoMe (°) | Rota et al. (2022) [39] | 4.47 ± 1.92 (SE) |
| Time Points | Arch | Parameters | References | Amount of Change |
|---|---|---|---|---|
| Post-distalization | Same arch | L1ie 1 (mm) | Wu et al. (2021) [38] | 1.02 ± 0.80 * |
| L1ra 2 (mm) | Wu et al. (2021) [38] | 0.33 ± 1.24 * | ||
| L1cc 3 (mm) | Wu et al. (2021) [38] | 0.56 ± 0.59 * | ||
| L1 4 inclination (°) | Wu et al. (2021) [38] | 1.51 ± 1.51 * | ||
| Post-treatment | Same arch | 31im-CoGo 5 (mm) | Rota et al. (2022) [39] | −1.13 ± 1.52 (SE) |
| 31ax-CoGo 6 (°) | Rota et al. (2022) [39] | −4.18 ± 2.44 (SE) | ||
| 31ax-GoMe 7 (°) | Rota et al. (2022) [39] | −4.78 ± 2.19 (SE) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Shen, C.; Park, T.H.; Chung, C.-H.; Li, C. Molar Distalization by Clear Aligners with Sequential Distalization Protocol: A Systematic Review and Meta-Analysis. J. Funct. Biomater. 2024, 15, 137. https://doi.org/10.3390/jfb15060137
Shen C, Park TH, Chung C-H, Li C. Molar Distalization by Clear Aligners with Sequential Distalization Protocol: A Systematic Review and Meta-Analysis. Journal of Functional Biomaterials. 2024; 15(6):137. https://doi.org/10.3390/jfb15060137
Chicago/Turabian StyleShen, Christie, Tiffany H. Park, Chun-Hsi Chung, and Chenshuang Li. 2024. "Molar Distalization by Clear Aligners with Sequential Distalization Protocol: A Systematic Review and Meta-Analysis" Journal of Functional Biomaterials 15, no. 6: 137. https://doi.org/10.3390/jfb15060137
APA StyleShen, C., Park, T. H., Chung, C.-H., & Li, C. (2024). Molar Distalization by Clear Aligners with Sequential Distalization Protocol: A Systematic Review and Meta-Analysis. Journal of Functional Biomaterials, 15(6), 137. https://doi.org/10.3390/jfb15060137