
A Two-Year Comparative Evaluation of Clinical Performance of a Nanohybrid Composite Resin to a Flowable Composite Resin


 ,
,  ,
,  , , and
, , and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Inclusion and Exclusion Criteria
- -
- Age between 20 and 60 years.
- -
- Good dental hygiene.
- -
- Capacity to read and sign the informed consent form.
- -
- Need for replacement of old fillings and deficient restorations or treatment of primary caries (replacement of defective restoration regardless of the depth of the cavity: The flowable composite resin (G-ænial Universal Flo, GC) and the nanohybrid universal composite resin (Tetric Evo Ceram, Ivoclar Vivadent) used in Class I and II direct esthetic restorations in posterior teeth were used to fill each cavity in incremental horizontal 2-mm layers, polymerized with a light-curing unit (Litex 695, Dentamerica, Industry, CA, USA), at a distance of 2 mm for 20 s on a soft start mode to minimize polymerization shrinkage of composite: curing begins at low light intensity followed by full light intensity to permit grater flow and stress release in the composite. A minimum of 800 mW/cm2 of light intensity is provided.
- -
- Confirmed follow-up examinations.
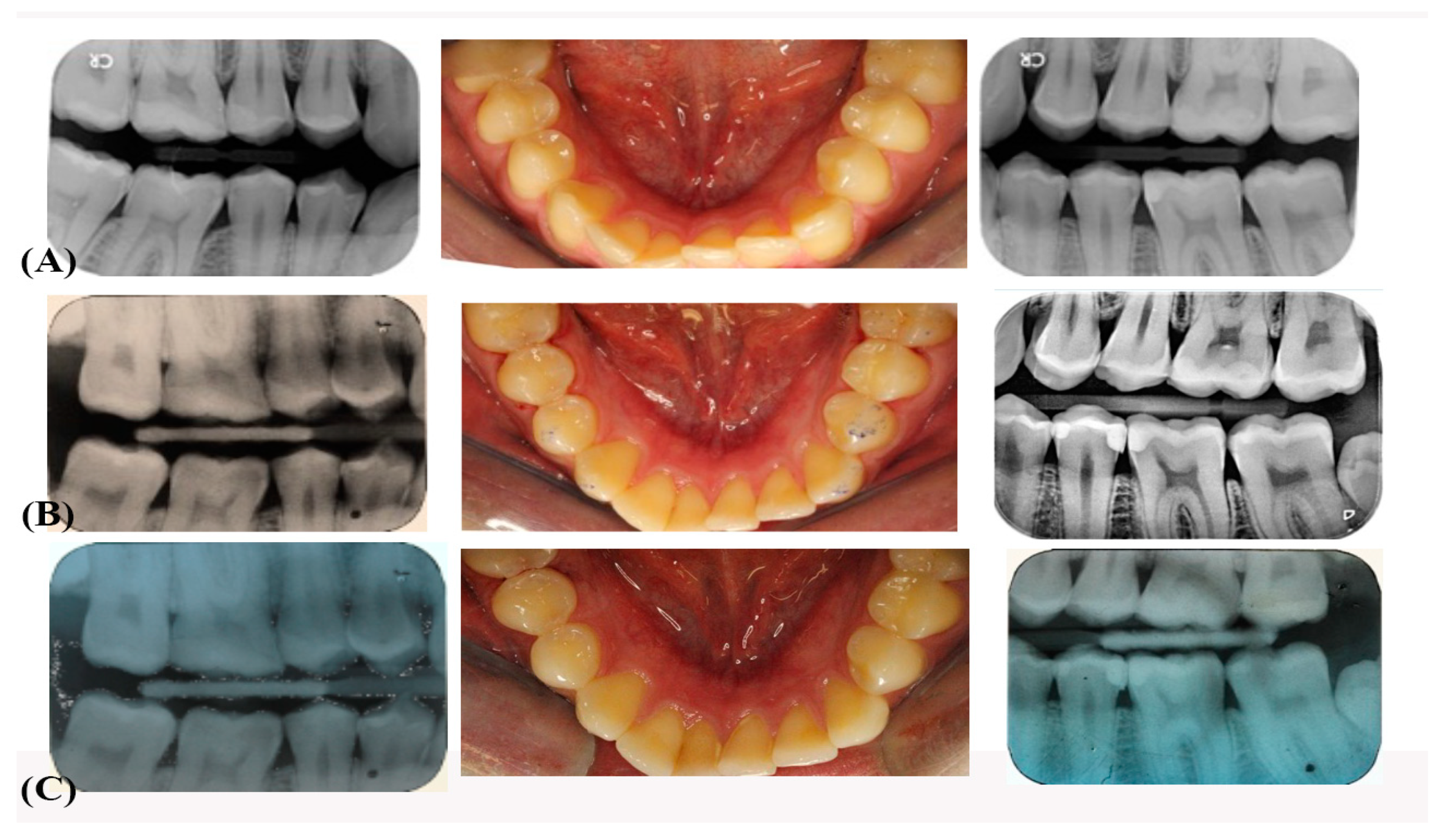
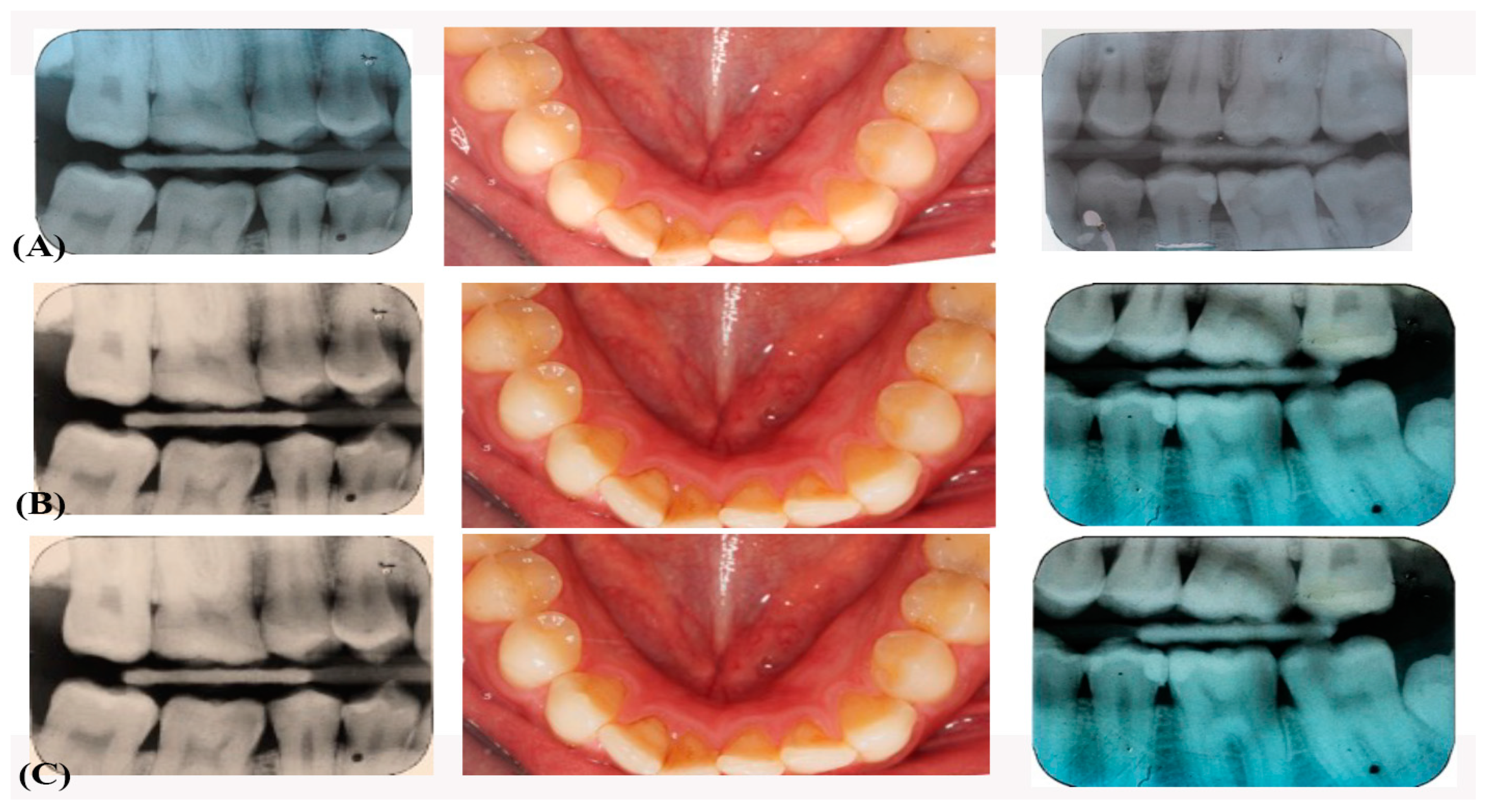
2.3. Application of Resin Fillings
2.4. Evaluation Criteria
2.5. Data Analysis
3. Results
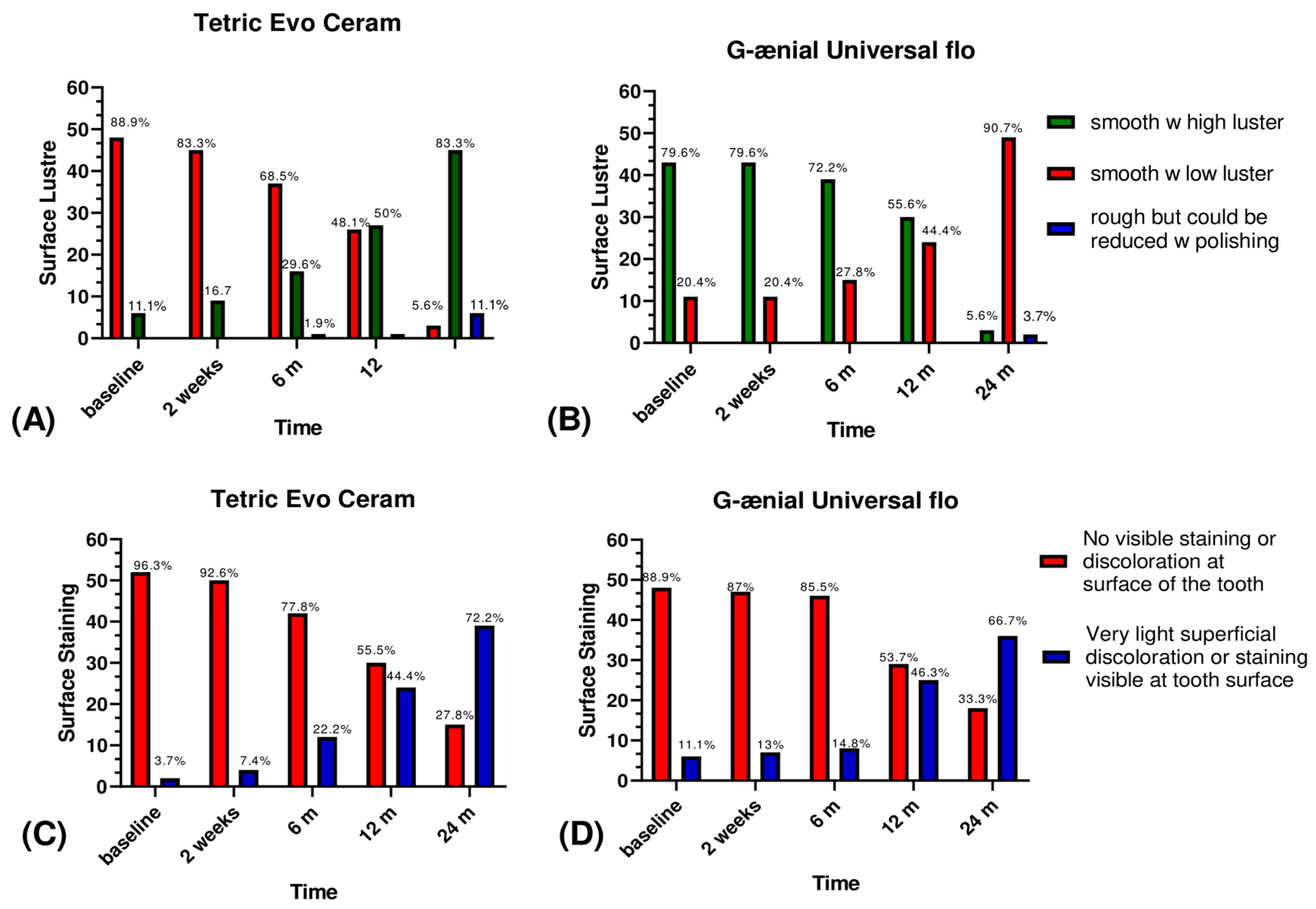
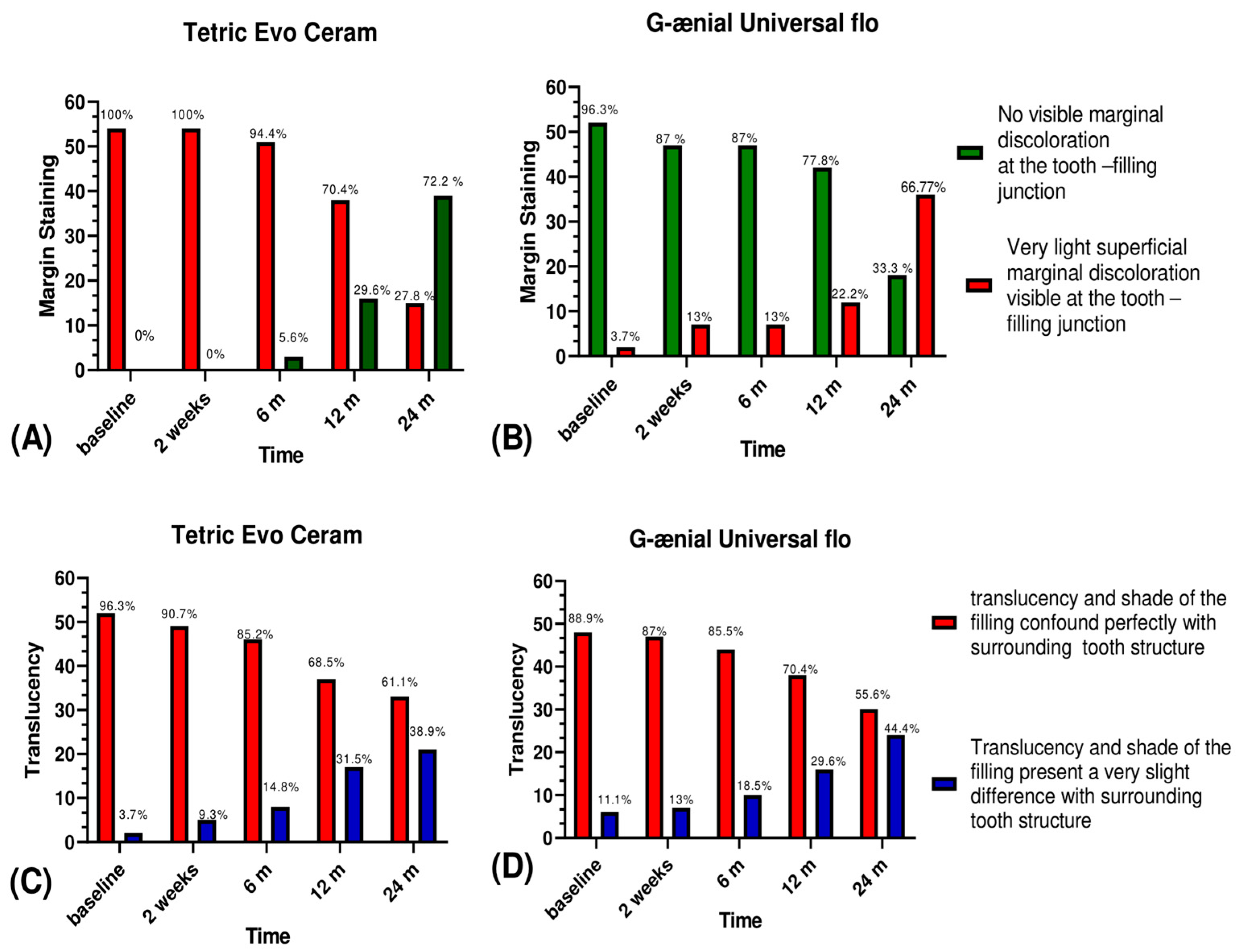
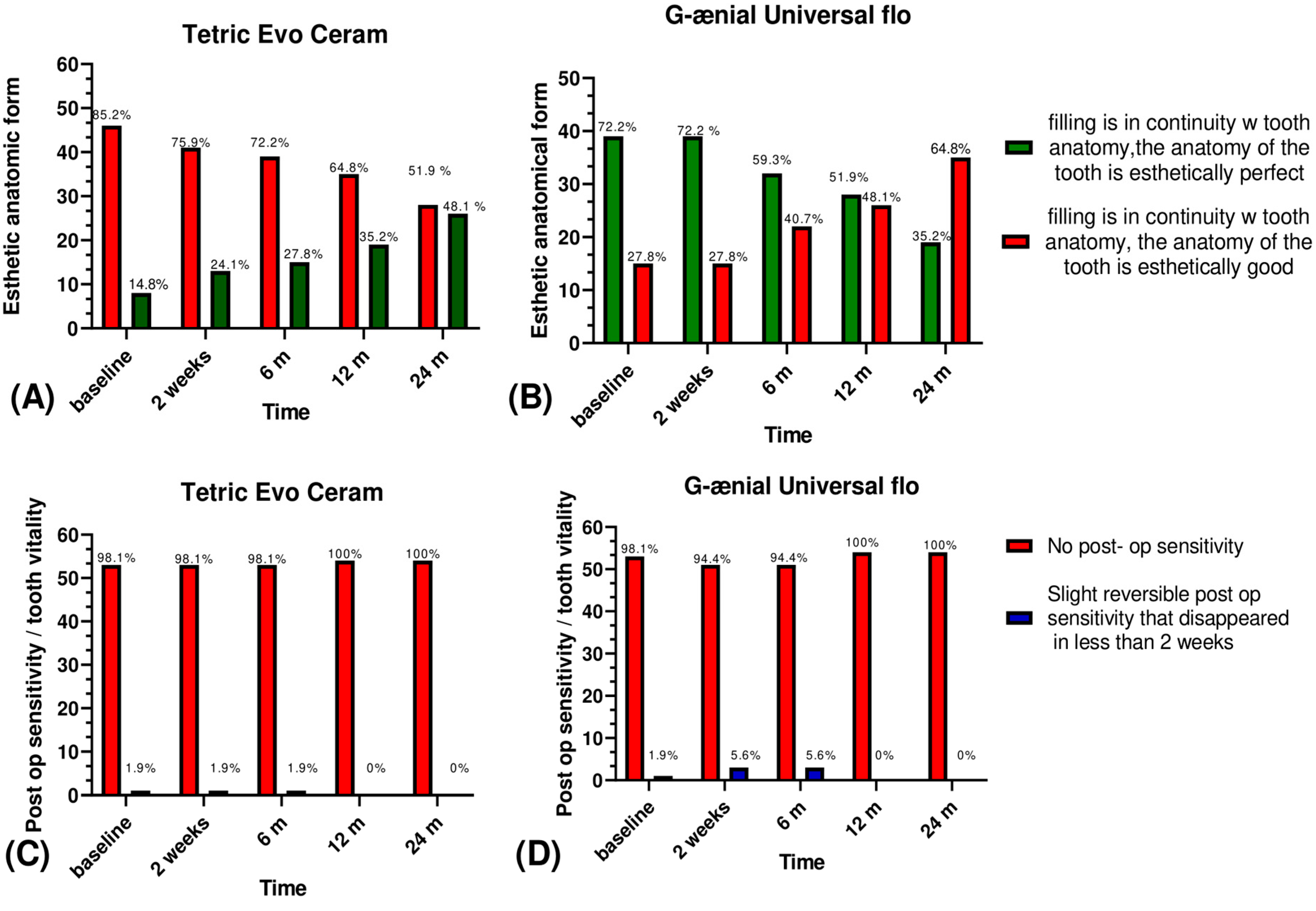
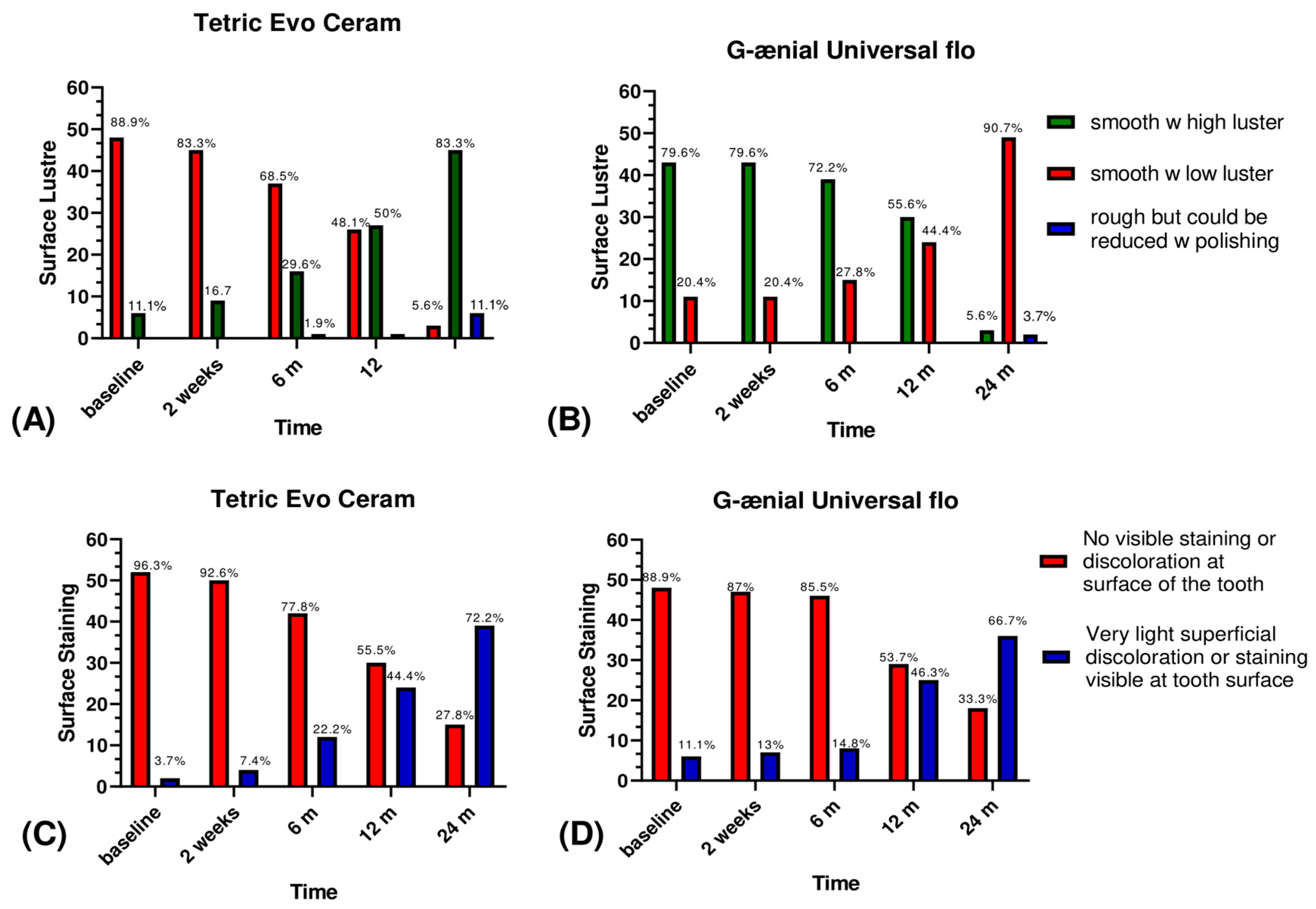
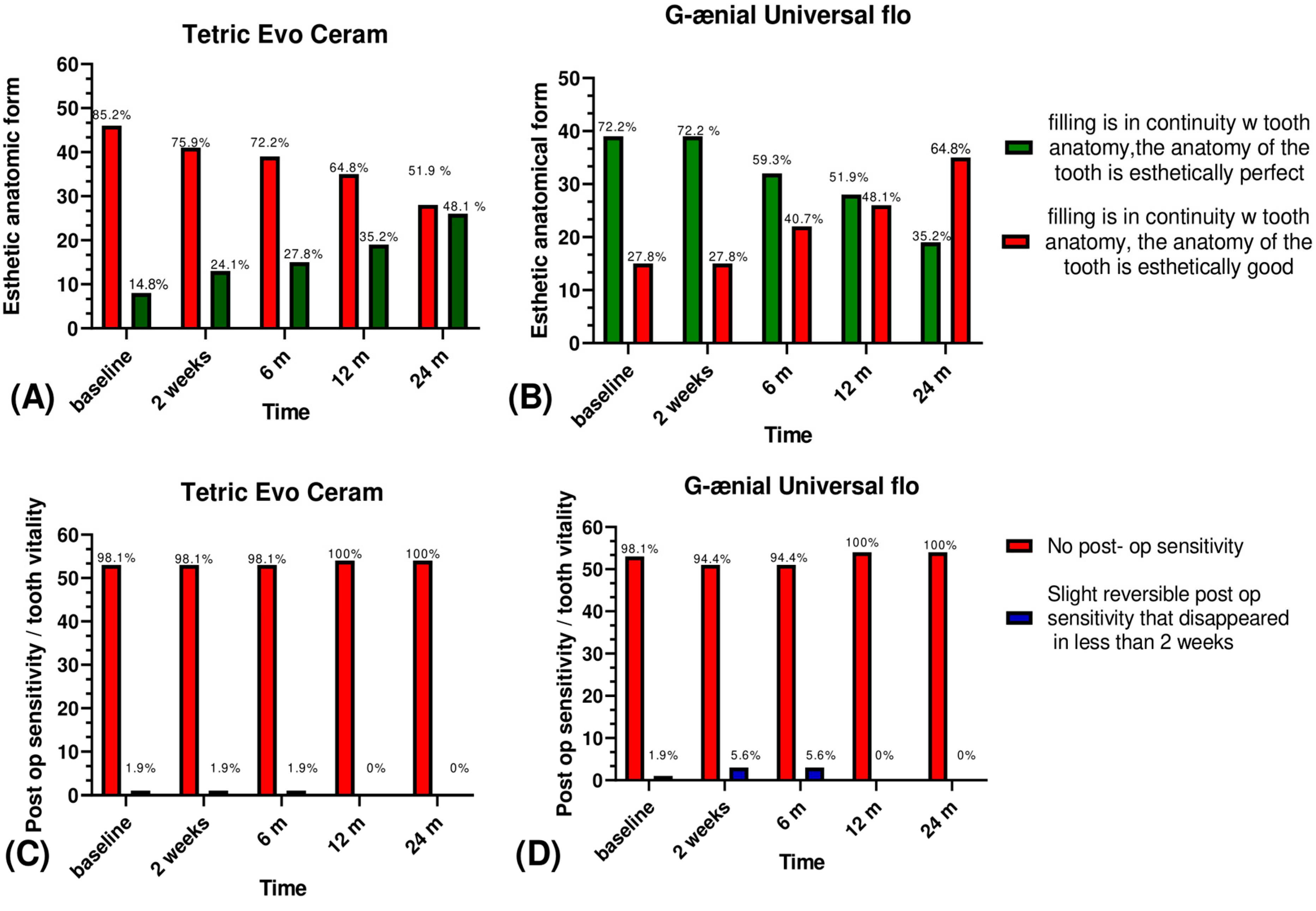
3.1. Esthetic Criteria
3.2. Biological Criteria
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Dietschi, D.; Argente, A. A comprehensive and conservative approach for the restoration of abrasion and erosion. part II: Clinical procedures and case report. Eur. J. Esthet. Dent. 2011, 6, 142–159. [Google Scholar] [PubMed]
- Pflaum, T.; Kranz, S.; Montag, R.; Güntsch, A.; Völpel, A.; Mills, R.; Jandt, K.; Sigusch, B. Clinical long-term success of contemporary nano-filled resin composites in class I and II restorations cured by LED or halogen light. Clin. Oral Investig. 2018, 22, 1651–1662. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ercan, E.; Dülgergil, Ç.T.; Soyman, M.; Dalli, M.; Yildirim, I. A field-trial of two restorative materials used with atraumatic restorative treatment in rural Turkey: 24-month results. J. Appl. Oral Sci. 2009, 17, 307–314. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Carvalho, A.A.; Leite, M.M.; Zago, J.K.M.; Nunes, C.A.B.C.M.; de Jesus Esteves Barata, T.; De Freitas, G.C.; De Torres, É.M.; Lopes, L.G. Influence of different application protocols of universal adhesive system on the clinical behavior of Class I and II restorations of composite resin—A randomized and double-blind controlled clinical trial. BMC Oral Health 2019, 19, 252. [Google Scholar] [CrossRef] [PubMed]
- Maran, B.M.; de Geus, J.L.; Gutiérrez, M.F.; Heintze, S.; Tardem, C.; Barceleiro, M.O.; Reis, A.; Loguercio, A.D. Nanofilled/nanohybrid and hybrid resin-based composite in patients with direct restorations in posterior teeth: A systematic review and meta-analysis. J. Dent. 2020, 99, 103407. [Google Scholar] [CrossRef] [PubMed]
- Angerame, D.; De Biasi, M. Do Nanofilled/Nanohybrid Composites Allow for Better Clinical Performance of Direct Restorations Than Traditional Microhybrid Composites? A Systematic Review. Oper. Dent. 2018, 43, E191–E209. [Google Scholar] [CrossRef] [PubMed]
- Alzraikat, H.; Burrow, M.F.; A Maghaireh, G.; A Taha, N. Nanofilled Resin Composite Properties and Clinical Performance: A Review. Oper. Dent. 2018, 43, E173–E190. [Google Scholar] [CrossRef]
- Spagnuolo, G.; Desiderio, C.; Rivieccio, V.; Amato, M.; Rossetti, D.V.; D’Antò, V.; Schweikl, H.; Lupi, A.; Rengo, S.; Nocca, G. In vitro cellular detoxification of triethylene glycol dimethacrylate by adduct formation with N-acetylcysteine. Dent. Mater. 2013, 29, e153–e160. [Google Scholar] [CrossRef]
- Kaisarly, D.; Meierhofer, D.; El Gezawi, M.; Rösch, P.; Kunzelmann, K. Effects of flowable liners on the shrinkage vectors of bulk-fill composites. Clin. Oral Investig. 2021, 25, 4927–4940. [Google Scholar] [CrossRef]
- Hervás-García, A.; Martínez-Lozano, M.A.; Cabanes-Vila, J.; Barjau-Escribano, A.; Fos-Galve, P. Composite resins. A review of the materials and clinical indications. Med. Oral Patol. Oral Cir. Bucal 2006, 11, E215–E220. Available online: https://pubmed.ncbi.nlm.nih.gov/16505805/ (accessed on 13 July 2021).
- Han, S.-H.; Sadr, A.; Shimada, Y.; Tagami, J.; Park, S.-H. Internal adaptation of composite restorations with or without an intermediate layer: Effect of polymerization shrinkage parameters of the layer material. J. Dent. 2019, 80, 41–48. [Google Scholar] [CrossRef]
- Ozel, E.; Korkmaz, Y.; Attar, N.; Karabulut, E. Effect of one-step polishing systems on surface roughness of different flowable restorative materials. Dent. Mater. J. 2008, 27, 755–764. [Google Scholar] [CrossRef] [Green Version]
- Ikeda, I.; Otsuki, M.; Sadr, A.; Nomura, T.; Kishikawa, R.; Tagami, J. Effect of filler content of flowable composites on resin-cavity interface. Dent. Mater. J. 2009, 28, 679–685. [Google Scholar] [CrossRef] [Green Version]
- Hirata-Tsuchiya, S.; Yoshii, S.; Ichimaru-Suematsu, M.; Washio, A.; Saito, N.; Urata, M.; Hanada, K.; Morotomi, T.; Kitamura, C. Two-year clinical comparison of a flowable-type nano-hybrid composite and a paste-type composite in posterior restoration. J. Investig. Clin. Dent. 2017, 8, e12227. [Google Scholar] [CrossRef]
- Shaalan, O.O.; Abou-Auf, E.; El Zoghby, A.F. Clinical evaluation of self-adhering flowable composite versus conventional flowable composite in conservative Class I cavities: Randomized controlled trial. J. Conserv. Dent. 2018, 21, 485–490. [Google Scholar] [CrossRef]
- Hickel, R.; Peschke, A.; Tyas, M.; Mjör, I.; Bayne, S.; Peters, M.; Hiller, K.-A.; Randall, R.; Vanherle, G.; Heintze, S.D. FDI World Dental Federation: Clinical criteria for the evaluation of direct and indirect restorations—Update and clinical examples. Clin. Oral Investig. 2010, 14, 349–366. [Google Scholar] [CrossRef]
- Eckhardt, A.; Müller, P.; Hiller, K.-A.; Krifka, S.; Bolay, C.; Spagnuolo, G.; Schmalz, G.; Schweikl, H. Influence of TEGDMA on the mammalian cell cycle in comparison with chemotherapeutic agents. Dent. Mater. 2010, 26, 232–241. [Google Scholar] [CrossRef] [PubMed]
- Shaalan, O.O.; Abou-Auf, E.; El Zoghby, A.F. Clinical evaluation of flowable resin composite versus conventional resin composite in carious and noncarious lesions: Systematic review and meta-analysis. J. Conserv. Dent. 2017, 20, 380–385. [Google Scholar] [CrossRef]
- Haugen, H.J.; Marovic, D.; Par, M.; Le Thieu, M.K.; Reseland, J.E.; Johnsen, G.F. Bulk Fill Composites Have Similar Performance to Conventional Dental Composites. Int. J. Mol. Sci. 2020, 21, 5136. [Google Scholar] [CrossRef]
- Blume, J.; Peipert, J.F. Randomization in controlled clinical trials: Why the flip of a coin is so important. J. Am. Assoc. Gynecol. Laparosc. 2004, 11, 320–325. [Google Scholar] [CrossRef]
- Gallo, J.R.; Burgess, J.O.; Ripps, A.H.; Walker, R.S.; Maltezos, M.B.; Mercante, D.E.; Davidson, J.M. Three-year clinical evaluation of two flowable composites. Quintessence Int. 2010, 41, 497–503. [Google Scholar]
- Collins, C.; Bryant, R.; Hodge, K.-L. A clinical evaluation of posterior composite resin restorations: 8-year findings. J. Dent. 1998, 26, 311–317. [Google Scholar] [CrossRef]
- da Rosa Rodolpho, P.A.; Cenci, M.; Donassollo, T.A.; Loguércio, A.D.; Demarco, F.F. A clinical evaluation of posterior composite restorations: 17-year findings. J. Dent. 2006, 34, 427–435. [Google Scholar] [CrossRef] [PubMed]
- Balkaya, H.; Arslan, S.; Pala, K. A randomized, prospective clinical study evaluating effectiveness of a bulk-fill composite resin, a conventional composite resin and a reinforced glass ionomer in Class II cavities: One-year results. J. Appl. Oral Sci. 2019, 27, e20180678. [Google Scholar] [CrossRef] [PubMed]
- Schroeder, T.; Da Silva, P.B.; Basso, G.R.; Franco, M.C.; Maske, T.T.; Cenci, M. Factors affecting the color stability and staining of esthetic restorations. Odontology 2019, 107, 507–512. [Google Scholar] [CrossRef] [PubMed]
- Mundim, F.M.; da Fonseca Roberti Garcia, L.; de Carvalho Pires-De-Souza, F. Effect of staining solutions and repolishing on color stability of direct composites. J. Appl. Oral Sci. 2010, 18, 249–254. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mitra, S.B.; Wu, D.; Holmes, B.N. An application of nanotechnology in advanced dental materials. J. Am. Dent. Assoc. 2003, 134, 1382–1390. [Google Scholar] [CrossRef] [Green Version]
- Ilie, N.; Hickel, R. Investigations on a methacrylate-based flowable composite based on the SDR™ technology. Dent. Mater. 2011, 27, 348–355. [Google Scholar] [CrossRef]
- Sumino, N.; Tsubota, K.; Takamizawa, T.; Shiratsuchi, K.; Miyazaki, M.; Latta, M.A. Comparison of the wear and flexural characteristics of flowable resin composites for posterior lesions. Acta Odontol. Scand. 2013, 71, 820–827. [Google Scholar] [CrossRef]
- Torres, C.R.G.; Rêgo, H.M.C.; Perote, L.C.C.; Santos, L.F.T.F.; Kamozaki, M.B.B.; Gutierrez, N.C.; Di Nicoló, R.; Borges, A.B. A split-mouth randomized clinical trial of conventional and heavy flowable composites in class II restorations. J. Dent. 2014, 42, 793–799. [Google Scholar] [CrossRef]
- Ruivo, M.A.; Pacheco, R.R.; Sebold, M.; Giannini, M. Surface roughness and filler particles characterization of resin-based composites. Microsc. Res. Tech. 2019, 82, 1756–1767. [Google Scholar] [CrossRef] [PubMed]
- Barutcigil, Ç.; Barutcigil, K.; Özarslan, M.M.; Dündar, A.; Yilmaz, B. Color of bulk-fill composite resin restorative materials. J. Esthet. Restor. Dent. 2017, 30, E3–E8. [Google Scholar] [CrossRef]
- Nair, S.R.; Niranjan, N.T.; Jayasheel, A.; Suryakanth, D.B. Comparative Evaluation of Colour Stability and Surface Hardness of Methacrylate Based Flowable and Packable Composite—In vitro Study. J. Clin. Diagn. Res. 2017, 11, ZC51–ZC54. [Google Scholar] [CrossRef] [PubMed]
- Senawongse, P.; Pongprueksa, P. Surface Roughness of Nanofill and Nanohybrid Resin Composites after Polishing and Brushing. J. Esthet. Restor. Dent. 2007, 19, 265–273. [Google Scholar] [CrossRef] [PubMed]
- Suzuki, T.; Kyoizumi, H.; Finger, W.J.; Kanehira, M.; Endo, T.; Utterodt, A.; Hisamitsu, H.; Komatsu, M. Resistance of nanofill and nanohybrid resin composites to toothbrush abrasion with calcium carbonate slurry. Dent. Mater. J. 2009, 28, 708–716. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Manhart, J.; Chen, H.-Y.; Hickel, R. Clinical Evaluation of the Posterior Composite Quixfil in Class I and II Cavities: 4-year Follow-up of a Randomized Controlled Trial. J. Adhes. Dent. 2010, 12, 237–243. [Google Scholar] [CrossRef] [PubMed]
- Fugolin, A.; Pfeifer, C. New Resins for Dental Composites. J. Dent. Res. 2017, 96, 1085–1091. [Google Scholar] [CrossRef]
- Demarco, F.F.; Correa, M.B.; Cenci, M.; Moraes, R.; Opdam, N.J. Longevity of posterior composite restorations: Not only a matter of materials. Dent. Mater. 2012, 28, 87–101. [Google Scholar] [CrossRef]
- Wierichs, R.; Kramer, E.; Meyer-Lueckel, H. Risk Factors for Failure of Direct Restorations in General Dental Practices. J. Dent. Res. 2020, 99, 1039–1046. [Google Scholar] [CrossRef]
- Bellezza, J.J.; McCartha, C.D.; Bradley, E.L.; Denys, F.R.; Retief, D.H. Four-year in vivo evaluation of the composite/bonding resin-tooth interface. Dent. Mater. 1990, 6, 237–240. [Google Scholar] [CrossRef]
- Soares, C.J.; Faria-E-Silva, A.L.; Rodrigues, M.D.P.; Vilela, A.B.F.; Pfeifer, C.; Tantbirojn, D.; Versluis, A. Polymerization shrinkage stress of composite resins and resin cements—What do we need to know? Braz. Oral Res. 2017, 31, 49–63. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Letzel, H. Survival rates and reasons for failure of posterior composite restorations in multicentre clinical trial. J. Dent. 1989, 17, S10–S17. [Google Scholar] [CrossRef]
- Stangel, I.; Barolet, R.Y. Clinical evaluation of two posterior composite resins: Two-year results. J. Oral Rehabil. 1990, 17, 257–268. [Google Scholar] [CrossRef] [PubMed]
- Kaisarly, D.; El Gezawi, M.; Keßler, A.; Rösch, P.; Kunzelmann, K.-H. Shrinkage vectors in flowable bulk-fill and conventional composites: Bulk versus incremental application. Clin. Oral Investig. 2021, 25, 1127–1139. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Material | Resin | Filler | Filler wt/vol % | Shade |
|---|---|---|---|---|
| Tetric Evo Ceram Ivoclar Vivadent, Schaan, Lichtenstein | Bis-GMA, UDMA, Ethoxylated Bis-EMA | Barium Glass, mixed oxide, filler, YbF3, prepolymers | 75–76/53–55 | |
| G-ænial Universal Flo, GC corporation, Tokyo, Japan | UDMA, Bis-MEPP, TEGDMA, | Silicon Dioxide, Strontium glass, pigmen | 69/50 | |
| Material | Composition | Application | ||
| G-ænial Bond GC, Corporation, Tokyo, Japan | 4-META, TEGDMA, UDMA, | Apply 1 coat of Adhesive, leave undisturbed for 10 s, Air dry vigorously, Light cure for 10 s | ||
| AdheSE One Ivoclar Vivadent, Schaan, Lichtenstein | Bis-Acryl, Bis-Meth, H2PO4, Amino acid Acryl, -OH alkyl Methacryl | |||
| Clinically Excellent/Very Good | Clinically Good | Clinically Sufficient/Satisfactory | Clinically Unsatisfactory | Clinically Poor | |||
|---|---|---|---|---|---|---|---|
| Esthetic criteria | Surface luster | The surface of the filling is smooth with high luster | The surface of the filling is smooth but with a low luster | The surface of the filling is rough but could be reduced with a polishing | The surface of the filling is rough but could not be reduced with a polishing | The surface of the filling is severely rough with deep or irregular grooves | |
| Staining | Surface | No visible staining or discolouration at the surface of the tooth | Very light superficial discolouration or staining is visible at the tooth surface | Visible staining and discolouration at the tooth surface could be removed by polishing | Visible staining and discolouration at the tooth surface with deep penetration that could not be removed by polishing | Very deep surface discolouration | |
| Margin | No visible marginal discolouration at the tooth-filling junction | Very light superficial marginal discolouration is visible at the tooth-filling junction | Visible marginal discolouration at the tooth-filling junction that could be removed by polishing | Visible marginal discolouration at the tooth-filling junction with deep penetration that could not be removed by polishing | Very deep marginal discolouration | ||
| Colour match and translucency | The translucency and shade of the filling confound perfectly with the surrounding tooth structure | The translucency and shade of the filling present a very slight difference with the surrounding tooth structure | The translucency and shade of the filling do not confound perfectly with the surrounding tooth structure but the difference remains acceptable | The translucency and shade of the filling do not confound perfectly with the surrounding tooth structure. The difference is important | The shade difference is severe | ||
| Esthetic anatomical form | The filling is in continuity with tooth anatomy, the anatomy of the tooth is esthetically perfect | The filling is in continuity with tooth anatomy, the anatomy of the tooth is esthetically good | The anatomy of the tooth is not at all esthetic but still clinically acceptable | The anatomy of the tooth is not at all respected | The anatomy of the tooth is completely lost. | ||
| Biological criteria | Postoperative sensitivity and tooth vitality | No post-op sensitivity | Slight reversible post-op sensitivity that disappeared in less than 2 weeks | Slight post-op sensitivity | Severe post-op sensitivity | Severe irreversible post-op sensitivity that led to root canal treatment | |
| Recurrence of caries, erosion and abfraction | No caries at the tooth-filling junction | Caries detected at the tooth-filling junction | |||||
| Tooth integrity | - | - | - | - | - | ||
| Periodontal response | No inflammation. Good oral health | Slight inflammation around the restoration | Severe inflammation around the restoration. Bleeding and pain | ||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Badr, C.; Spagnuolo, G.; Amenta, F.; Khairallah, C.; Mahdi, S.S.; Daher, E.; Battineni, G.; Baba, N.Z.; Zogheib, T.; Qasim, S.S.B.; et al. A Two-Year Comparative Evaluation of Clinical Performance of a Nanohybrid Composite Resin to a Flowable Composite Resin. J. Funct. Biomater. 2021, 12, 51. https://doi.org/10.3390/jfb12030051
Badr C, Spagnuolo G, Amenta F, Khairallah C, Mahdi SS, Daher E, Battineni G, Baba NZ, Zogheib T, Qasim SSB, et al. A Two-Year Comparative Evaluation of Clinical Performance of a Nanohybrid Composite Resin to a Flowable Composite Resin. Journal of Functional Biomaterials. 2021; 12(3):51. https://doi.org/10.3390/jfb12030051
Chicago/Turabian StyleBadr, Carelle, Gianrico Spagnuolo, Francesco Amenta, Carlos Khairallah, Syed Sarosh Mahdi, Elie Daher, Gopi Battineni, Nadim Z. Baba, Tatiana Zogheib, Syed Saad B. Qasim, and et al. 2021. "A Two-Year Comparative Evaluation of Clinical Performance of a Nanohybrid Composite Resin to a Flowable Composite Resin" Journal of Functional Biomaterials 12, no. 3: 51. https://doi.org/10.3390/jfb12030051
APA StyleBadr, C., Spagnuolo, G., Amenta, F., Khairallah, C., Mahdi, S. S., Daher, E., Battineni, G., Baba, N. Z., Zogheib, T., Qasim, S. S. B., Daher, T., Chintalapudi, N., & Zogheib, C. M. (2021). A Two-Year Comparative Evaluation of Clinical Performance of a Nanohybrid Composite Resin to a Flowable Composite Resin. Journal of Functional Biomaterials, 12(3), 51. https://doi.org/10.3390/jfb12030051