Implementing Mobile Games into Care Services—Service Models for Finnish and Chinese Elderly Care

 ,
,
Abstract
:1. Introduction
2. Research Methods and Test Set-Up
2.1. User Experiences
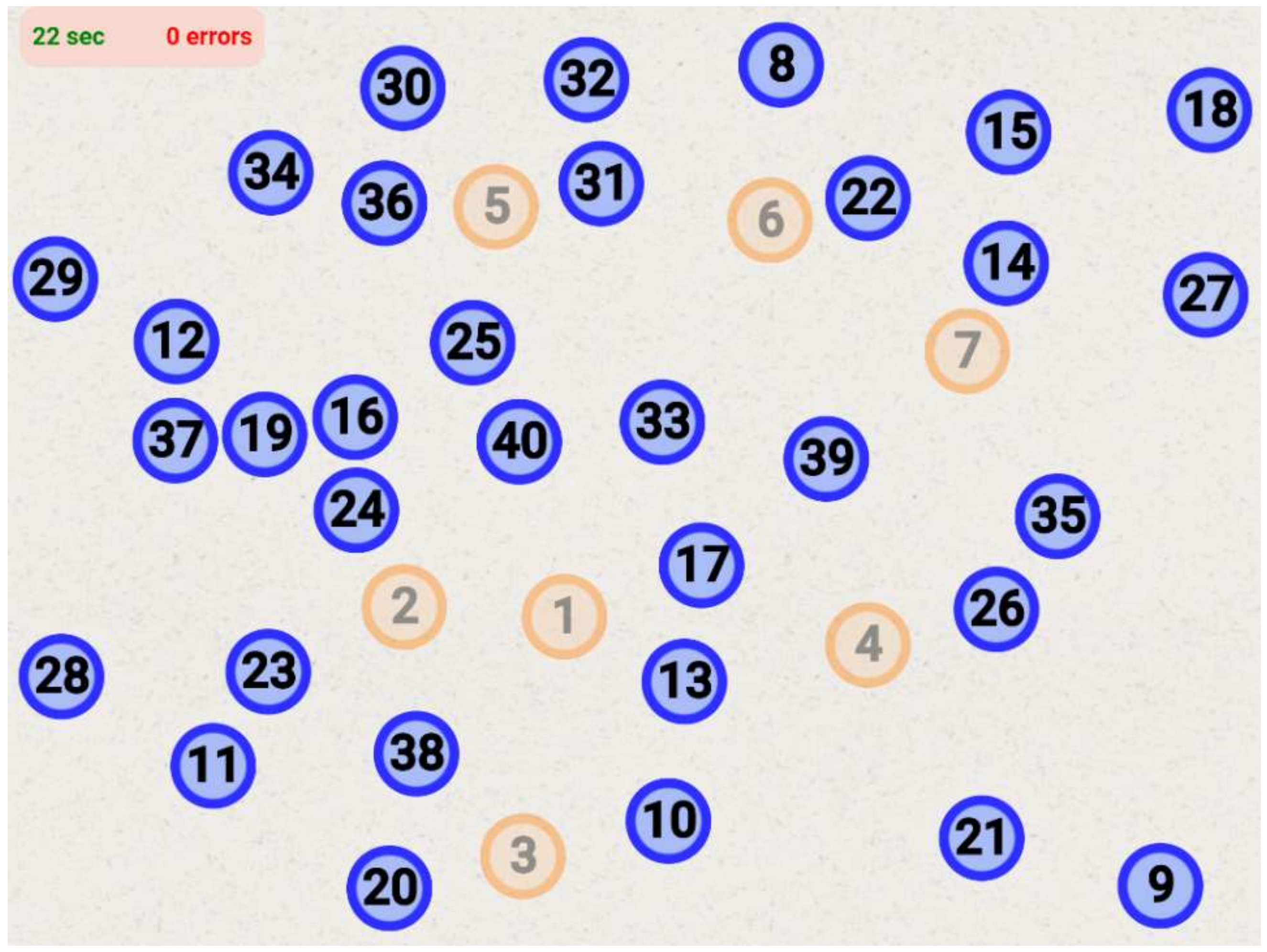
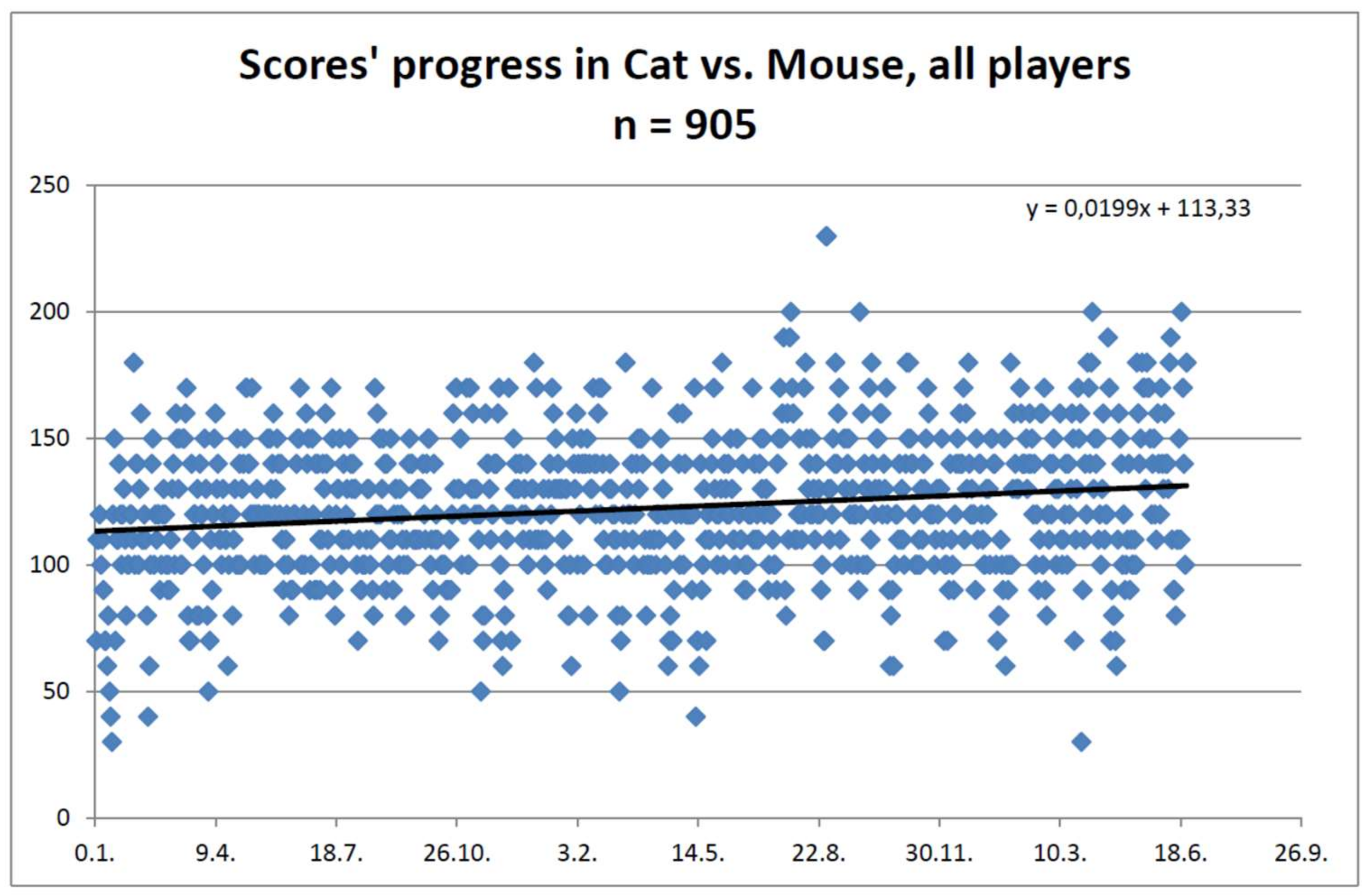
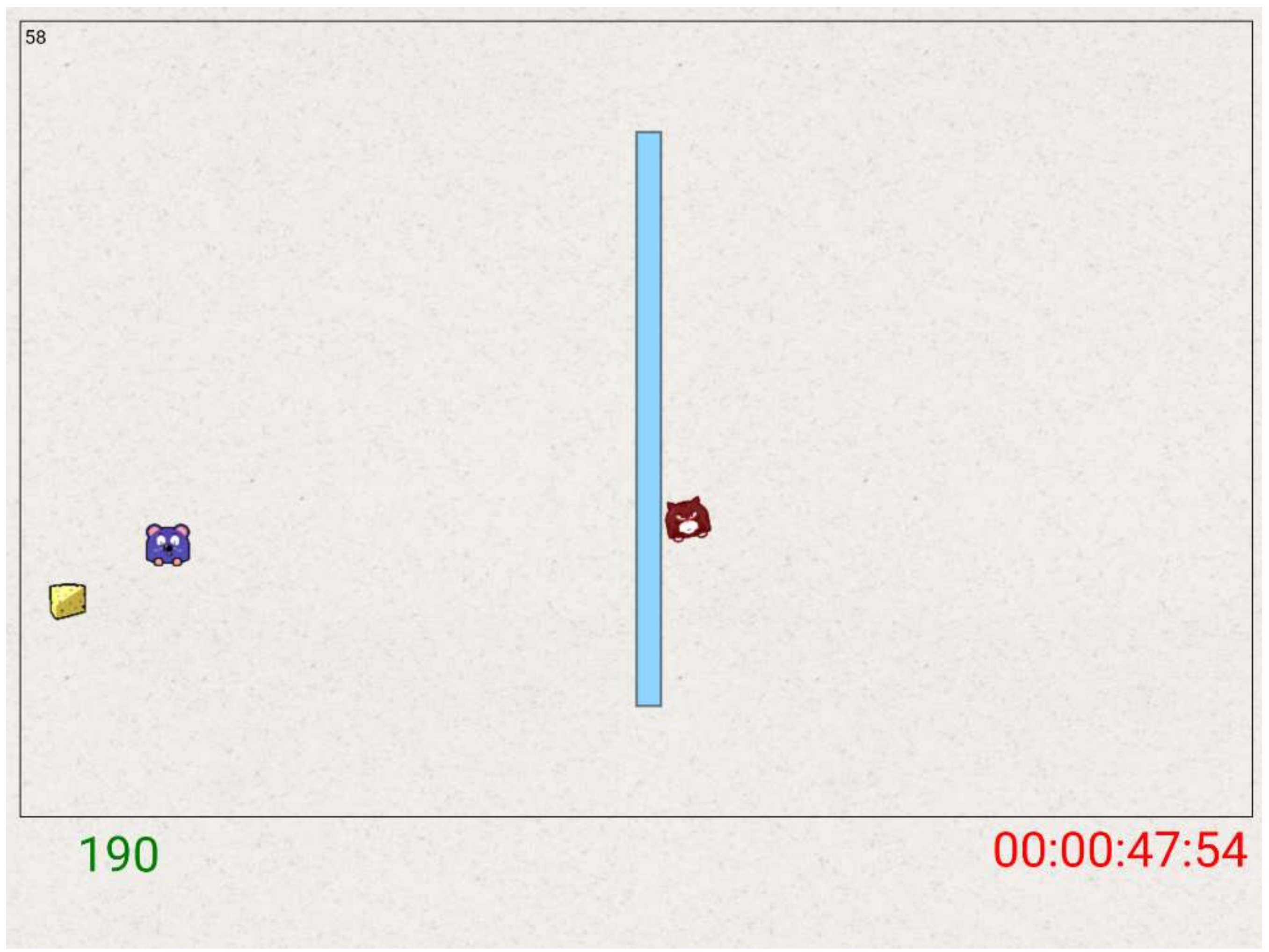
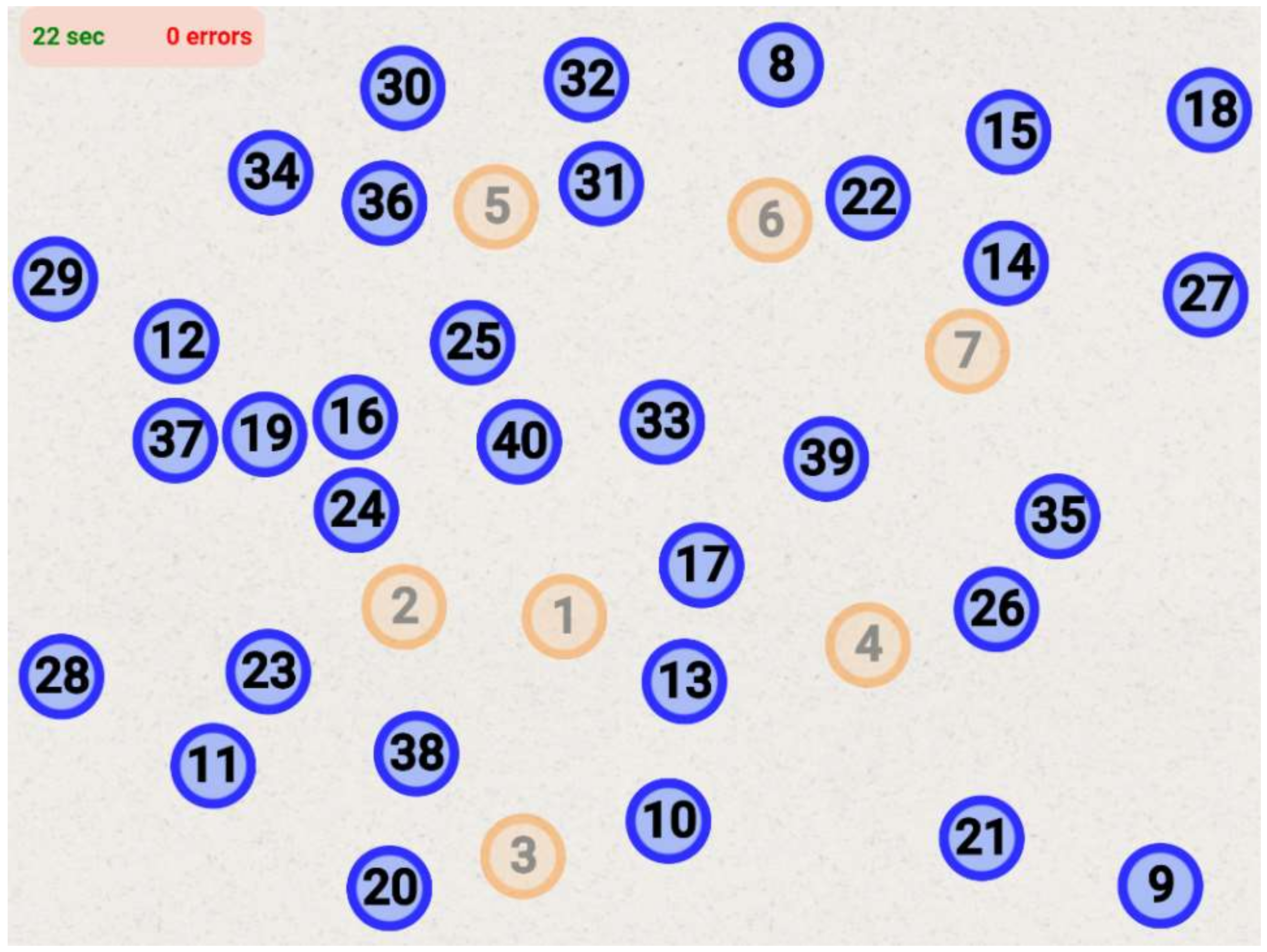
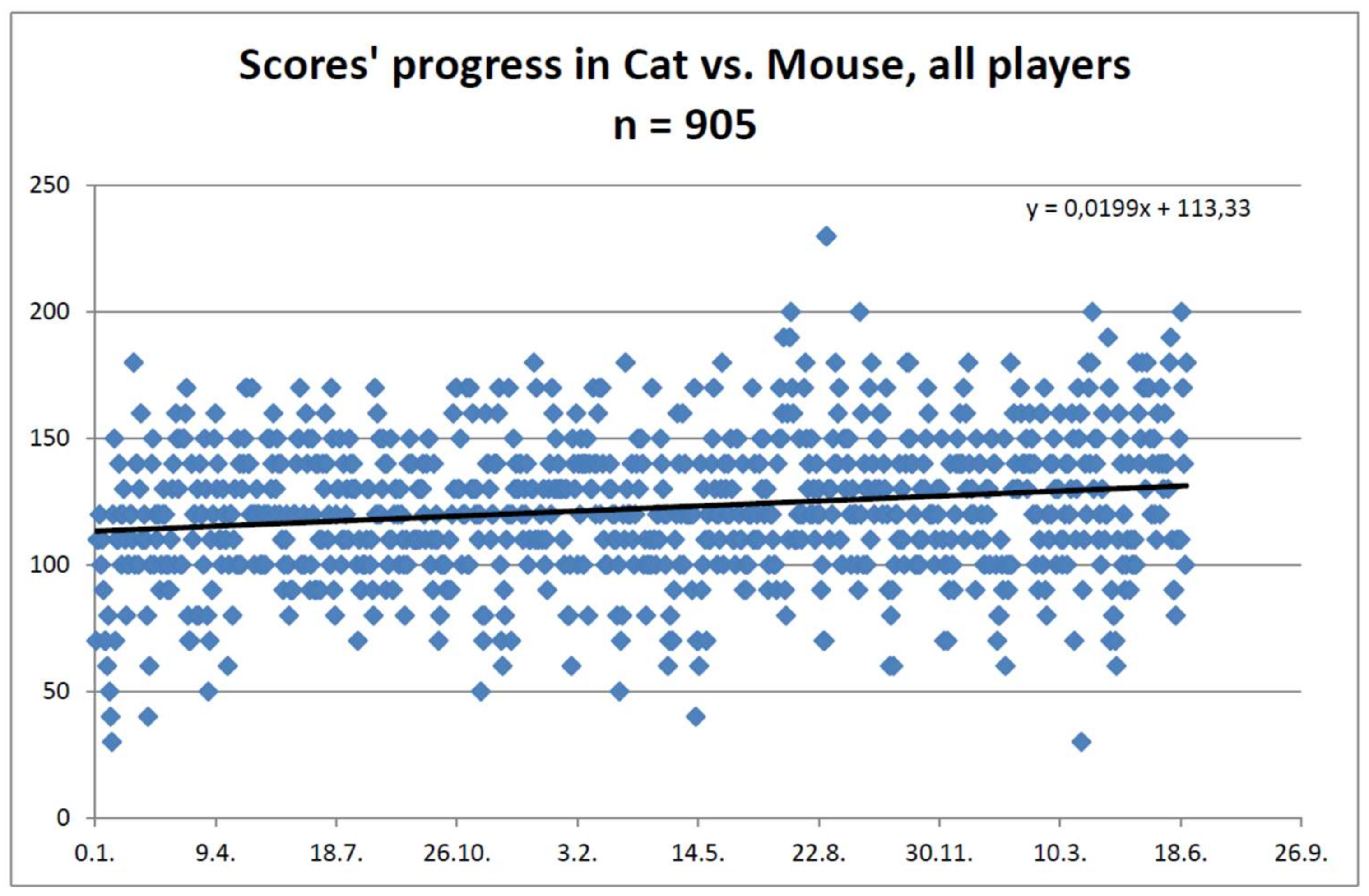
2.2. Gaming Scores
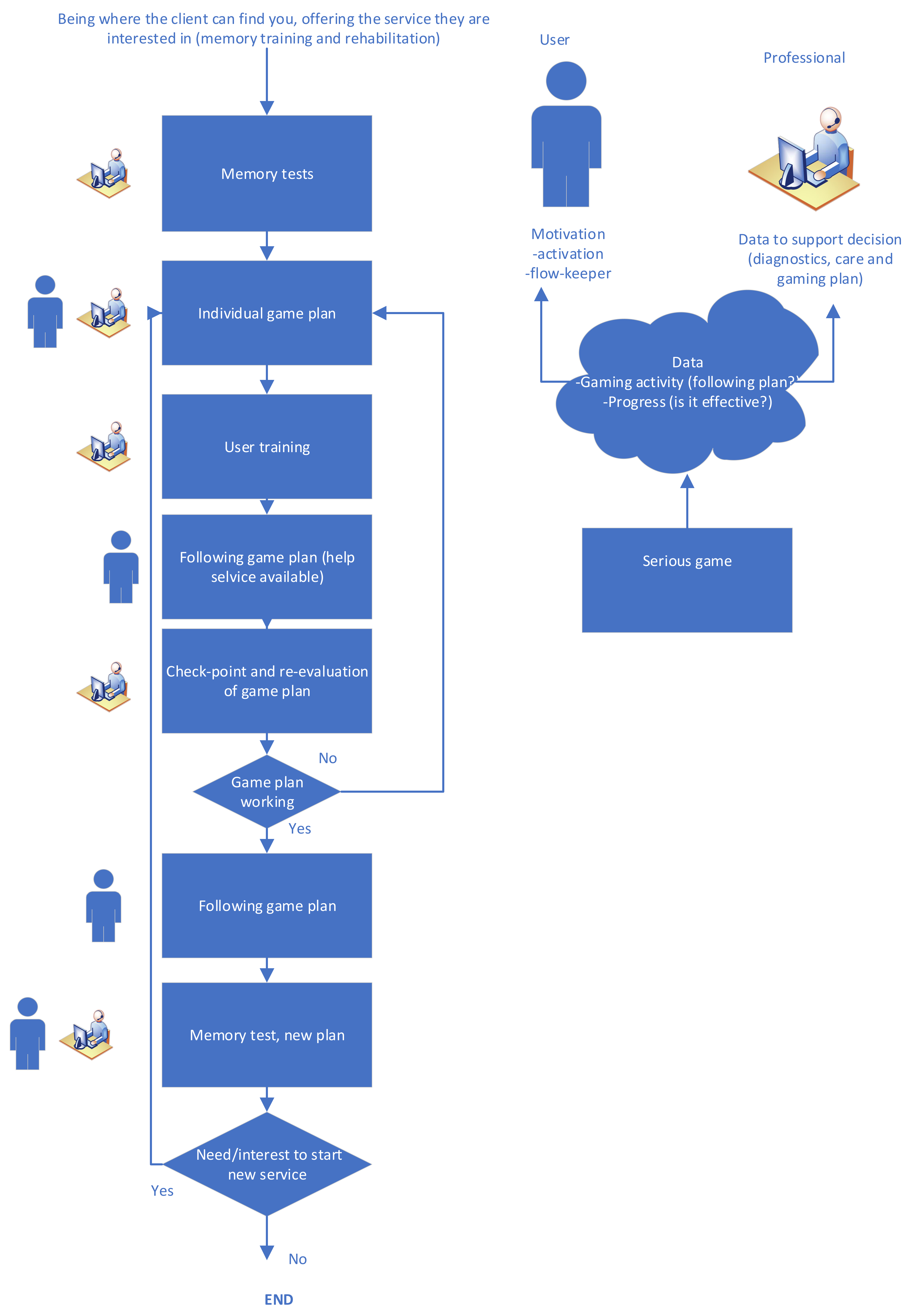
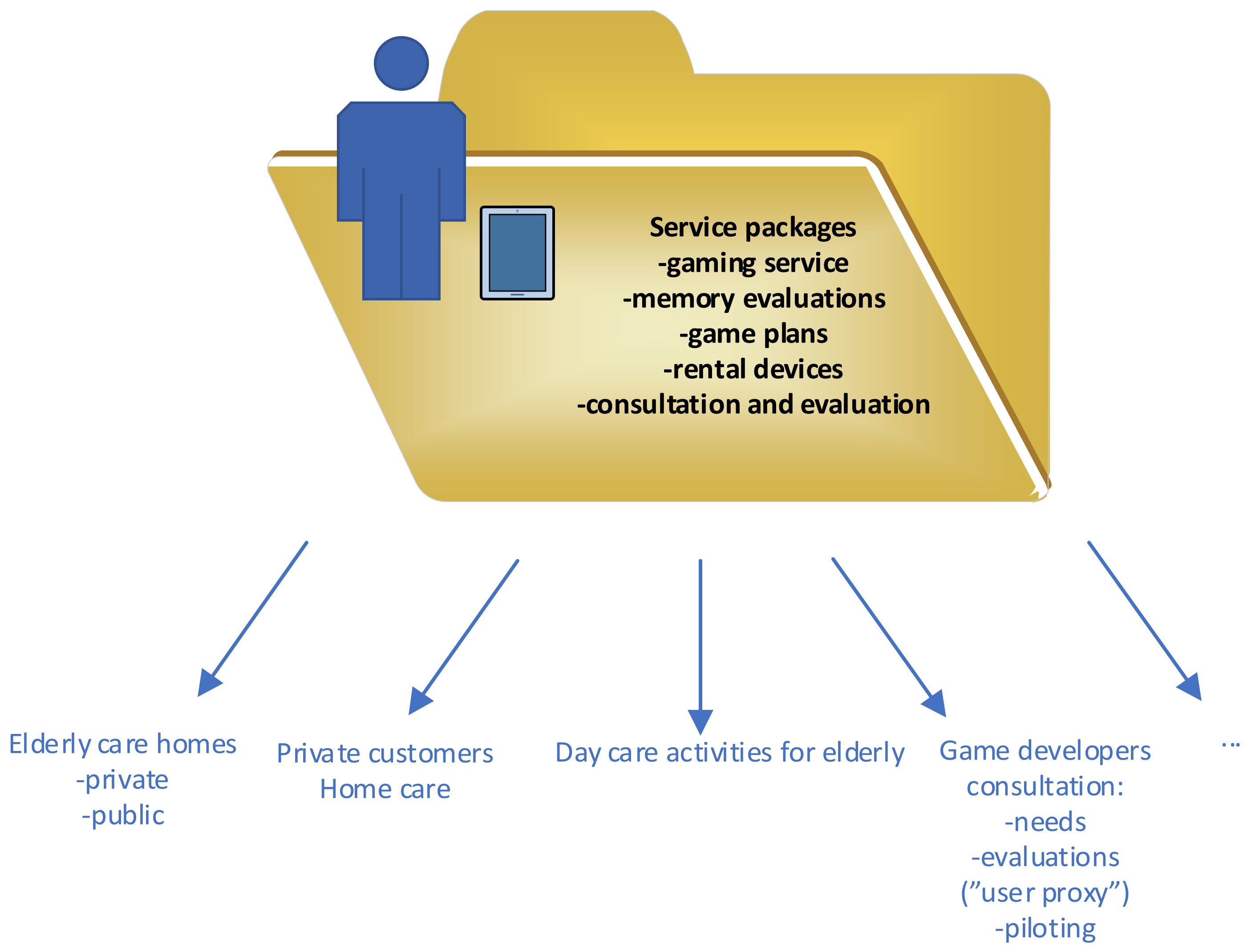
2.3. Gaming Service Models
3. Results and Discussion
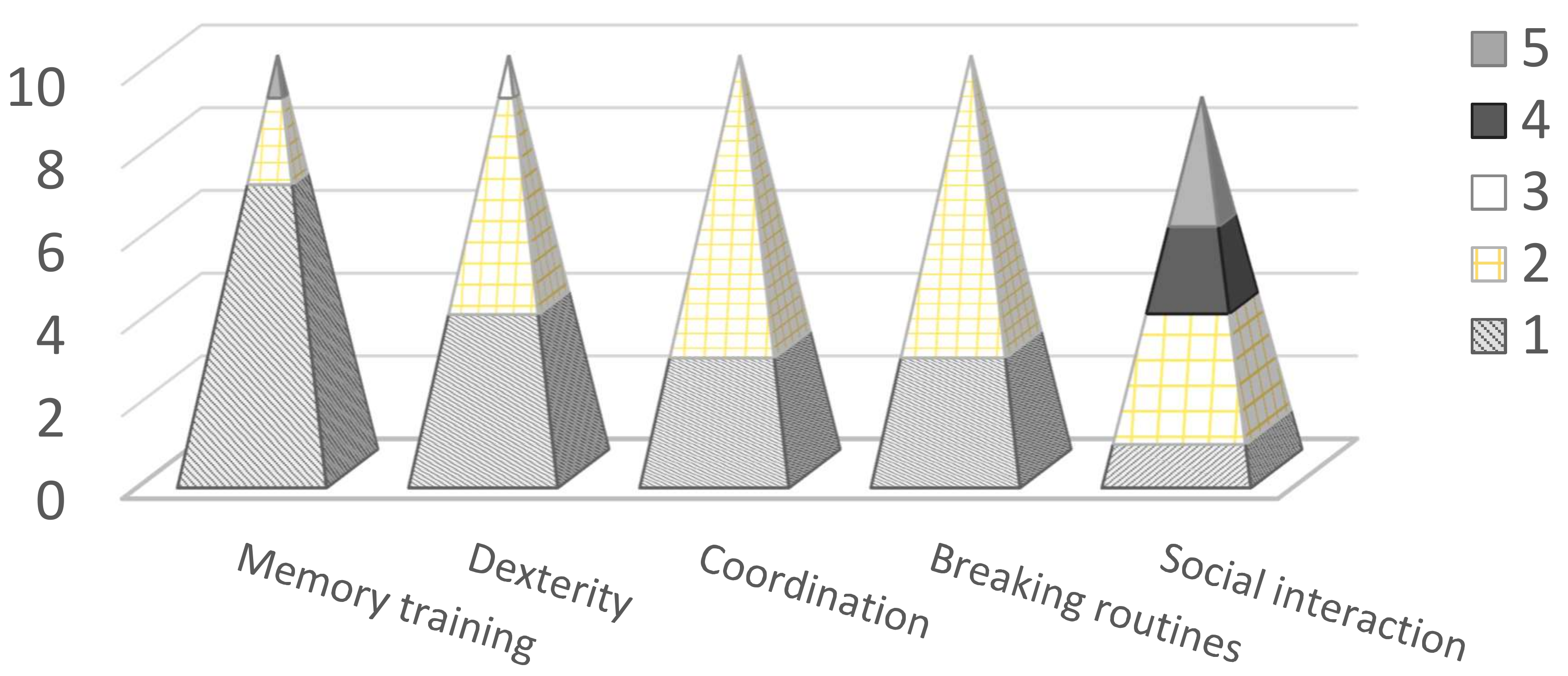
3.1. User Experiences
3.2. Gaming Scores
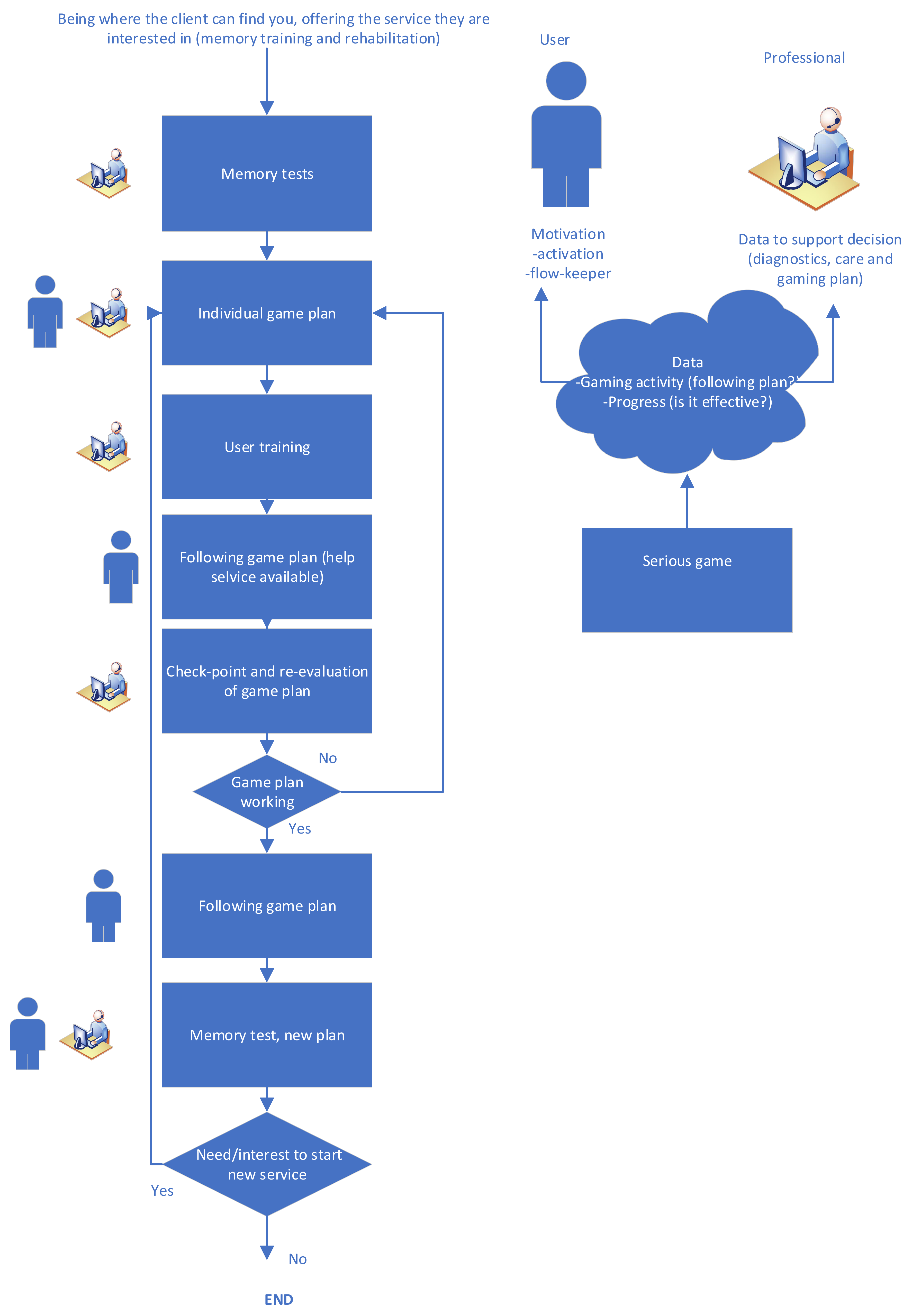
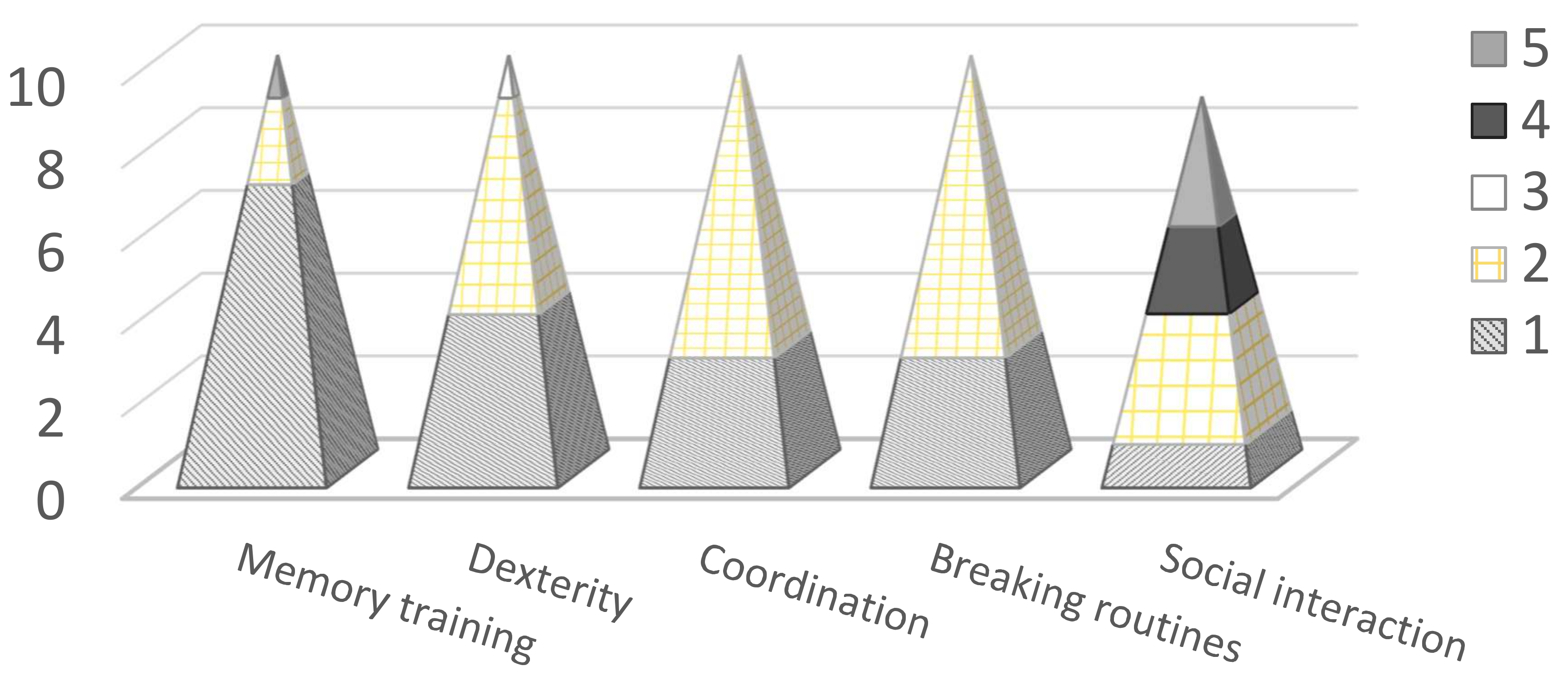
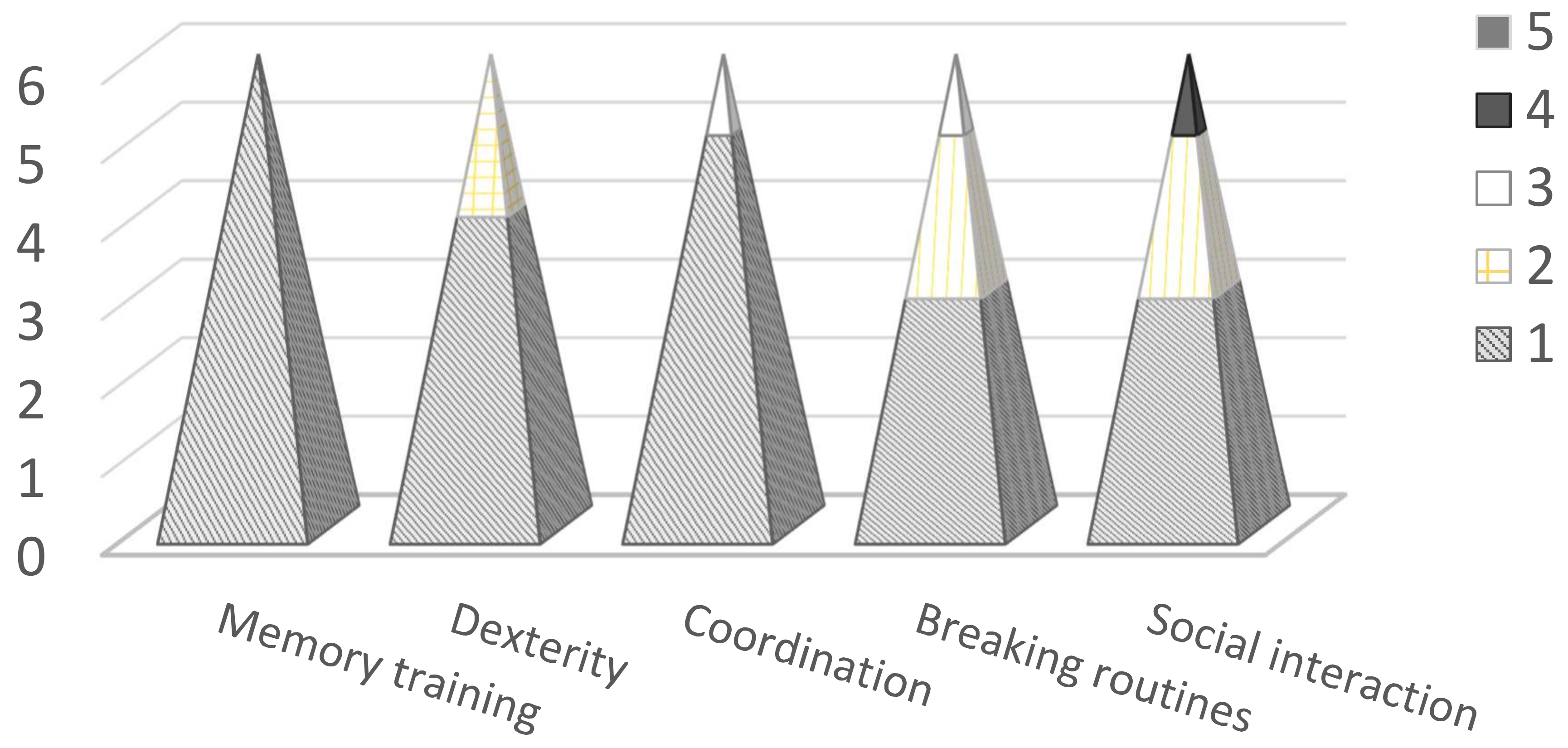
3.3. Gaming Service Models
- How would the technology solutions become a service?
- How would the solution become accessible and user-centric?
- What kinds of services are needed to implement the technology?
- What actually provides the most value for the customer?
- Are there any other application possibilities or user groups for the technology?
- Who could be the service provider for the customer?
4. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Serious Gaming for Future Seniors. Available online: https://stt.nl/stt/wp-content/uploads/2013/01/STT_SG_ouderen_eng_HR-los.pdf (accessed on 5 February 2019).
- Wiemeyer, J.; Kliem, A. Serious games in prevention and rehabilitation—A new panacea for elderly people? Eur. Rev. Aging Phys. Act. 2012, 9, 41–50. [Google Scholar] [CrossRef]
- Nauta, H.; Spil, T.A.M. Change your lifestyle or your game is over: The design of a serious game for diabetes. In Proceedings of the IEEE 1st International Conference on Serious Games and Applications for Health (SeGAH), Braga, Portugal, 16–18 November 2011; pp. 1–7. [Google Scholar]
- Ferreira, C. Gamification of stroke rehabilitation exercises using a smartphone. In Proceedings of the 8th International Conference on Pervasive Computing Technologies for Healthcare. ICST (Institute for Computer Sciences, Social-Informatics and Telecommunications Engineering), Oldenburg, Germany, 20–23 May 2014; pp. 282–285. [Google Scholar]
- Martins, T.; Carvalho, V.; Soares, F. A serious game for rehabilitation of neurological disabilities: Premilinary study. In Proceedings of the IEEE 4th Portuguese Meeting on Bioengineering (ENBENG), Porto, Portugal, 26–28 February 2015; pp. 1–5. [Google Scholar]
- Madeira, R.N.; Costa, L.; Postolache, O. PhysioMate—Pervasive physical rehabilitation based on NUI and gamification. In Proceedings of the International Conference and Exposition on Electrical and Power Engineering (EPE), Iasi, Romania, 16–18 October 2014; pp. 612–616. [Google Scholar]
- Deponti, D.; Maggiorini, D.; Palazzi, C.E. Smartphone’s physiatric serious game. In Proceedings of the IEEE 1st International Conference on Serious Games and Applications for Health (SeGAH), Braga, Portugal, 16–18 November 2011; pp. 1–8. [Google Scholar]
- Miloff, A.; Marklund, A.; Carlbring, P. The challenger app for social anxiety disorder: New advances in mobile psychological treatment. Int. Interven. 2015, 2, 382–391. [Google Scholar] [CrossRef]
- Martins, T.; Carvalho, V.; Soares, F.; Moreira, M.F. Serious game as a tool to intellectual disabilities therapy: Total challenge. In Proceedings of the IEEE 1st International Conference on Serious Games and Applications for Health (SeGAH), Braga, Portugal; 16–18 November 2011; pp. 1–7. [Google Scholar]
- Chang, C.; Hinze, A.; Bowen, J.; Gilbert, L.; Starkey, N. Mymemory: A mobile memory assistant for people with traumatic brain injury. Int. J. Hum.-Comput. Stud. 2018, 117, 4–19. [Google Scholar] [CrossRef]
- Hornos, M.J.; Rute-Pérez, S.; Rodríguez-Domínguez, C.; Rodríguez-Almendros, M.L.; Rodríguez-Fórtiz, M.J.; Caracuel, A. Visual Working Memory Training of the Elderly in VIRTRAEL Personalized Assistant. In Personal Assistants: Emerging Computational Technologies; Costa, A., Julian, V., Novais, P., Eds.; Intelligent Systems Reference Library; Springer: Cham, Switzerland, 2018; Volume 132. [Google Scholar]
- Silva, B.M.; Rodrigues, J.J.; de la Torre Díez, I.; López-Coronado, M.; Saleem, K. Mobile-health: A review of current state in 2015. J. Biomed. Inform. 2015, 56, 265–272. [Google Scholar] [CrossRef] [PubMed]
- Oh, H.; Rizo, C.; Enkin, M.; Jadad, A. What is eHealth (3): A systematic review of published definitions. J. Med. Inter. Res. 2005, 7, e1. [Google Scholar] [CrossRef] [PubMed]
- Lanyu, X.; Heather, A.F.; Weisong, S. User centric design for aging population: Early experiences and lessons. In Proceedings of the IEEE Connected Health: Applications, Systems and Engineering Technologies (CHASE), Washington, DC, USA, 27–29 June 2016. [Google Scholar]
- Merilampi, S.; Koivisto, A.; Sirkka, A.; Xiao, X.; Min, Y.; Ye, L.; Chujun, X.; Chen, J.; Raumonen, P.; Virkki, J. The Cognitive Mobile Games for Older Adults—A Chinese User Experience Study. In Proceedings of the IEEE International Conference on Serious Games and Applications for Health (SEGAH), Perth, Australia, 2–4 April 2017. [Google Scholar]
- Merilampi, S.; Koivisto, A.; Virkki, J. Activation Game for Older Adults—Development and Initial User Experiences. In Proceedings of the IEEE International Conference on Serious Games and Applications for Health (SEGAH), Vienna, Austria, 16–18 May 2018. [Google Scholar]
- Merilampi, S.; Sirkka, A.; Leino, M.; Koivisto, A.; Finn, E. Cognitive mobile games for memory impaired older adults. J. Assist. Technol. 2014, 8, 207–223. [Google Scholar] [CrossRef]
- Fairchild, J.K.; Scogin, F.R. Training to enhance Adult Memory (TEAM): An investigation of the effectiveness of a memory training program with older adults. Aging Mental Health 2010, 14, 364–373. [Google Scholar] [CrossRef] [PubMed]
- McCough, E.L.; Kelly, V.E.; Logsdon, R.G.; McCurry, S.M.; Cochrane, B.B.; Engel, J.M.; Teri, L. Associations between physical performance and executive function in older adults with mild cognitive impairment: Gait speed and the timed “Up & Go” test. Phys. Ther. 2011, 91, 1198–1210. [Google Scholar]
- Szturm, T.; Betker, A.L.; Moussavi, Z.; Desai, A.; Goodman, V. Effects of an interactive computer game exercise regimen on balance impairment in frail community-dwelling older adults: A randomized controlled trial. Phys. Ther. 2011, 91, 1449–1462. [Google Scholar] [CrossRef] [PubMed]
- Trail Making Test. Available online: http://apps.usd.edu/coglab/schieber/psyc423/pdf/IowaTrailMaking.pdf (accessed on 1 November 2018).
- Lezak, M.D.; Howieson, D.B.; Loring, D.W. Neuropsychological Assessment, 4th ed.; Oxford University Press: New York, NY, USA, 2004. [Google Scholar]
- Reitan, R.M. Validity of the Trail Making test as an indicator of organic brain damage. Percept Mot Skills 1958, 8, 271–276. [Google Scholar] [CrossRef]
- Garrett, J.J. Elements of User Experience, the: User-Centered Design for the Web and Beyond; Pearson Education: New York, NY, USA, 2010. [Google Scholar]
- Hwang, M.-Y.; Hong, J.-C.; Hao, Y.; Jong, J-T. Elders’ usability, dependability, and flow experiences on embodied interactive video games. Educ. Gerontol. 2011, 37, 715–731. [Google Scholar] [CrossRef]
- Snowden, M.; Steinman, L.; Mochan, K.; Grodstein, F.; Prohaska, T.R.; Thurman, D.J.; Brown, D.R.; Laditka, J.N.; Soares, J.; Zweiback, D.J.; et al. Effect of exercise on cognitive performance in community-dwelling older adults: Review of intervention trials and recommendations for public health practice and research. J. Am. Geriat. Soc. 2011, 59, 704–716. [Google Scholar] [CrossRef] [PubMed]
- Vekara, J. International Business Negotiations between Finnish and Chinese Business People. Master’s Thesis, University of Vaasa, Vaasa, Finland, 2014. [Google Scholar]
- Purmonen, M. Influence of Cultural Differences on Finnish-Chinese Cooperation at UPM-Kymmene’s three Asian Sales Offices. Master’s Thesis, University of Jyväskylä, Jyväskylä, Finland, 2000. [Google Scholar]
- King, P.C.; Zhang, W. The role of face in a Chinese context of trust and trust building. Int. J. Cross Cult. Manag. 2018, 18, 149–173. [Google Scholar] [CrossRef]
- Näsi, M.J.; Räsänen, P.; Keipi, T.; Oksanen, A. Trust and victimization: A cross-national comparison of Finland, the U.S., Germany and UK. Res. Finnish Soc. 2017, 10, 119–131. [Google Scholar]
- ISO 9241-210:2010. Ergonomics of Human–System Interaction—Part 210: Human-Centred Design for Interactive Systems. Available online: https://www.iso.org/obp/ui/#iso:std:iso:9241:-210:ed-1:v1:en (accessed on 5 February 2019).




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| (Number of Digits) | Slope (All Results) | Number of Games Played |
|---|---|---|
| 5 | 0.0537 | 84 |
| 10 | 0.1634 | 54 |
| 15 | −0.1579 | 95 |
| 20 | −0.3489 | 171 |
| 25 | 0.1615 | 158 |
| 30 | −0.3159 | 184 |
| 35 | −0.3168 | 141 |
| 40 | −0.3973 | 215 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Merilampi, S.; Koivisto, A.; Leino, M.; Pombo, N.; Felizardo, V.; Lu, J.; Poberznik, A.; Virkki, J. Implementing Mobile Games into Care Services—Service Models for Finnish and Chinese Elderly Care. Information 2019, 10, 55. https://doi.org/10.3390/info10020055
Merilampi S, Koivisto A, Leino M, Pombo N, Felizardo V, Lu J, Poberznik A, Virkki J. Implementing Mobile Games into Care Services—Service Models for Finnish and Chinese Elderly Care. Information. 2019; 10(2):55. https://doi.org/10.3390/info10020055
Chicago/Turabian StyleMerilampi, Sari, Antti Koivisto, Mirka Leino, Nuno Pombo, Virginie Felizardo, Jue Lu, Anja Poberznik, and Johanna Virkki. 2019. "Implementing Mobile Games into Care Services—Service Models for Finnish and Chinese Elderly Care" Information 10, no. 2: 55. https://doi.org/10.3390/info10020055
APA StyleMerilampi, S., Koivisto, A., Leino, M., Pombo, N., Felizardo, V., Lu, J., Poberznik, A., & Virkki, J. (2019). Implementing Mobile Games into Care Services—Service Models for Finnish and Chinese Elderly Care. Information, 10(2), 55. https://doi.org/10.3390/info10020055