Evaluation of a Rehabilitation System for the Elderly in a Day Care Center



Abstract
1. Introduction
- it proposes a new physical rehabilitation exergame protocol for the elderly;
- the exergame protocol is multilevel and customizable according to the physical capabilities and clinical needs of the elderly by physiotherapists;
- the system is based on low-cost depth sensors and no calibration, or training phases are required making the system feasible in home settings;
- the proposed system was qualitatively evaluated on healthy adult volunteers;
- the proposed system was qualitatively and quantitatively evaluated on elderly people;
- the evaluation of the system was carried out in a real scenario;
- long-term follow-up (six months);
- this study provides the clinical perspectives on exergames in rehabilitation systems for the elderly.
2. Related Work
3. System Overview
- a Tele-Monitoring (TM) module;
- a Rehabilitation and Gaming (RG) module;
- a Medical Business Intelligence (MBI) module.
3.1. Tele-Monitoring Module
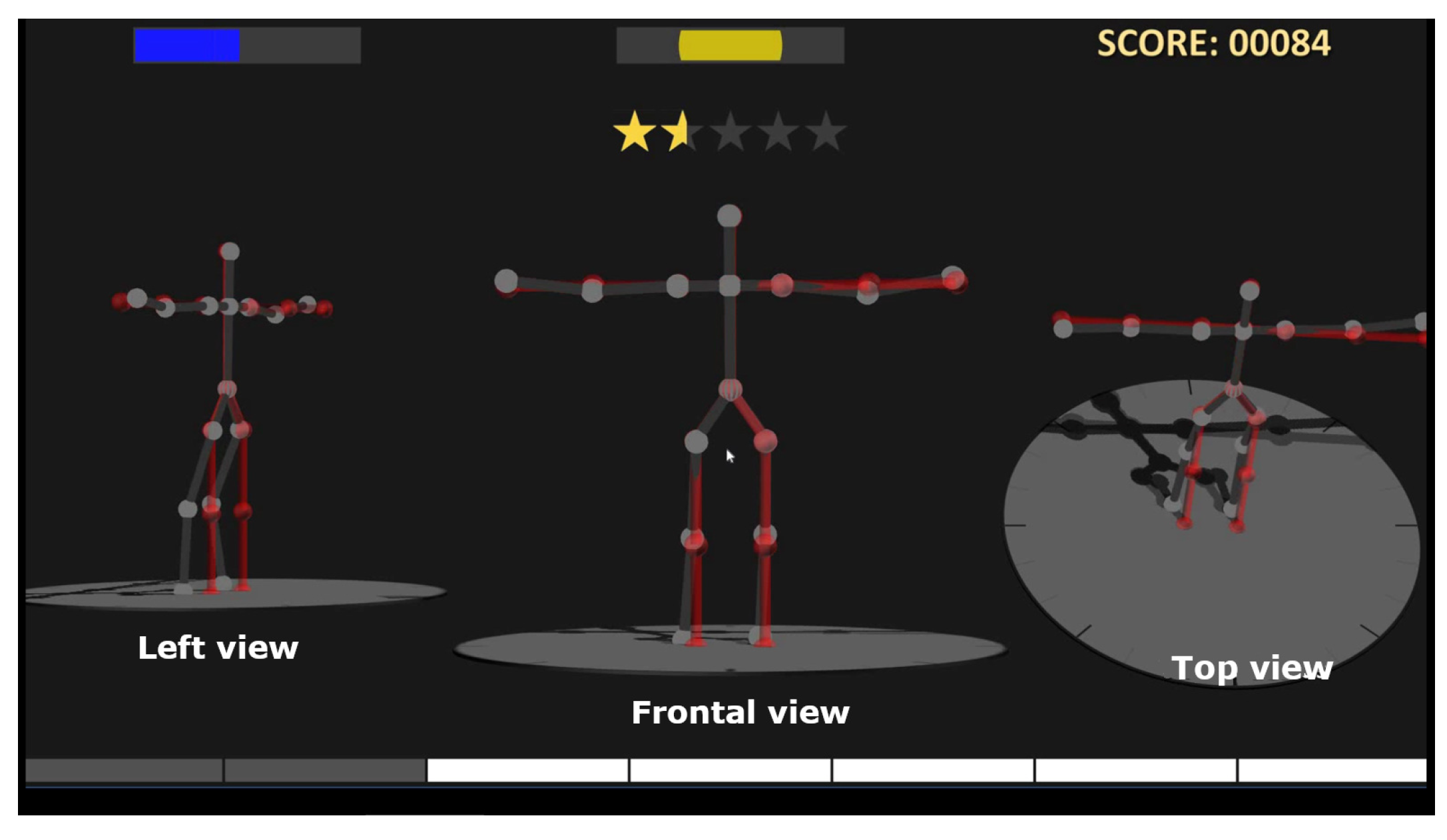
3.2. Rehabilitation and Gaming Module
3.3. Medical Business Intelligence Module
4. KINOPTIM Exergame Protocol
4.1. Extension of the Arms
4.2. Extension of the Knees
4.3. Sideways Lift of the Legs
5. Experiments
5.1. Experimental Setup
5.2. Procedure
5.3. Participants
6. Experimental Results
6.1. Pilot Study
- Q1:
- Overall, I am satisfied with how easy it is to use this system
- Q2:
- It was simple to use this system
- Q3:
- I can effectively complete my physical exercises using this system
- Q4:
- I am able to complete my physical exercises more quickly using this system
- Q5:
- I am able to efficiently complete my physical exercises using this system
- Q6:
- I feel comfortable using this system
- Q7:
- It was easy to learn to use this system
- Q8:
- The interface of this system is pleasant
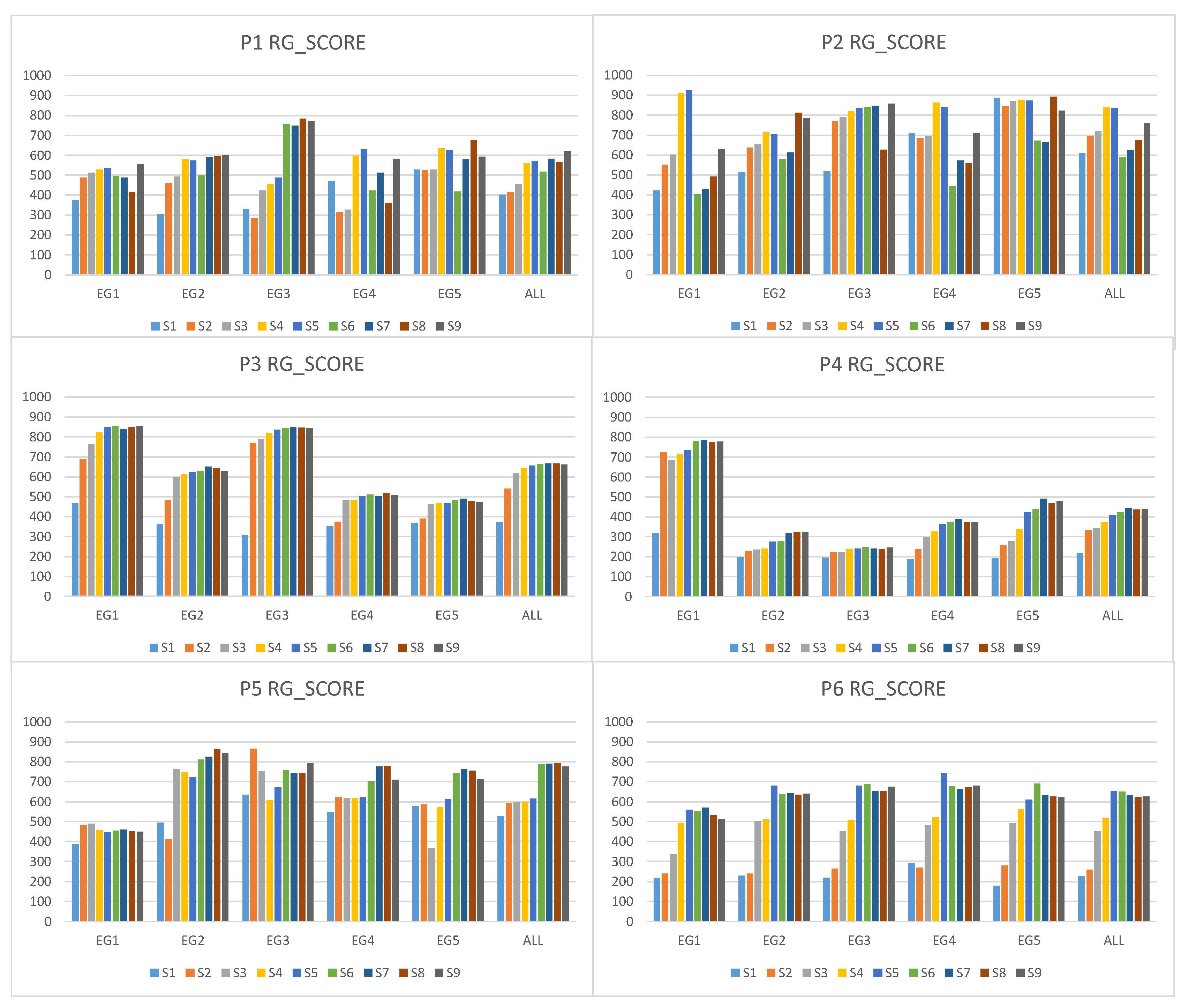
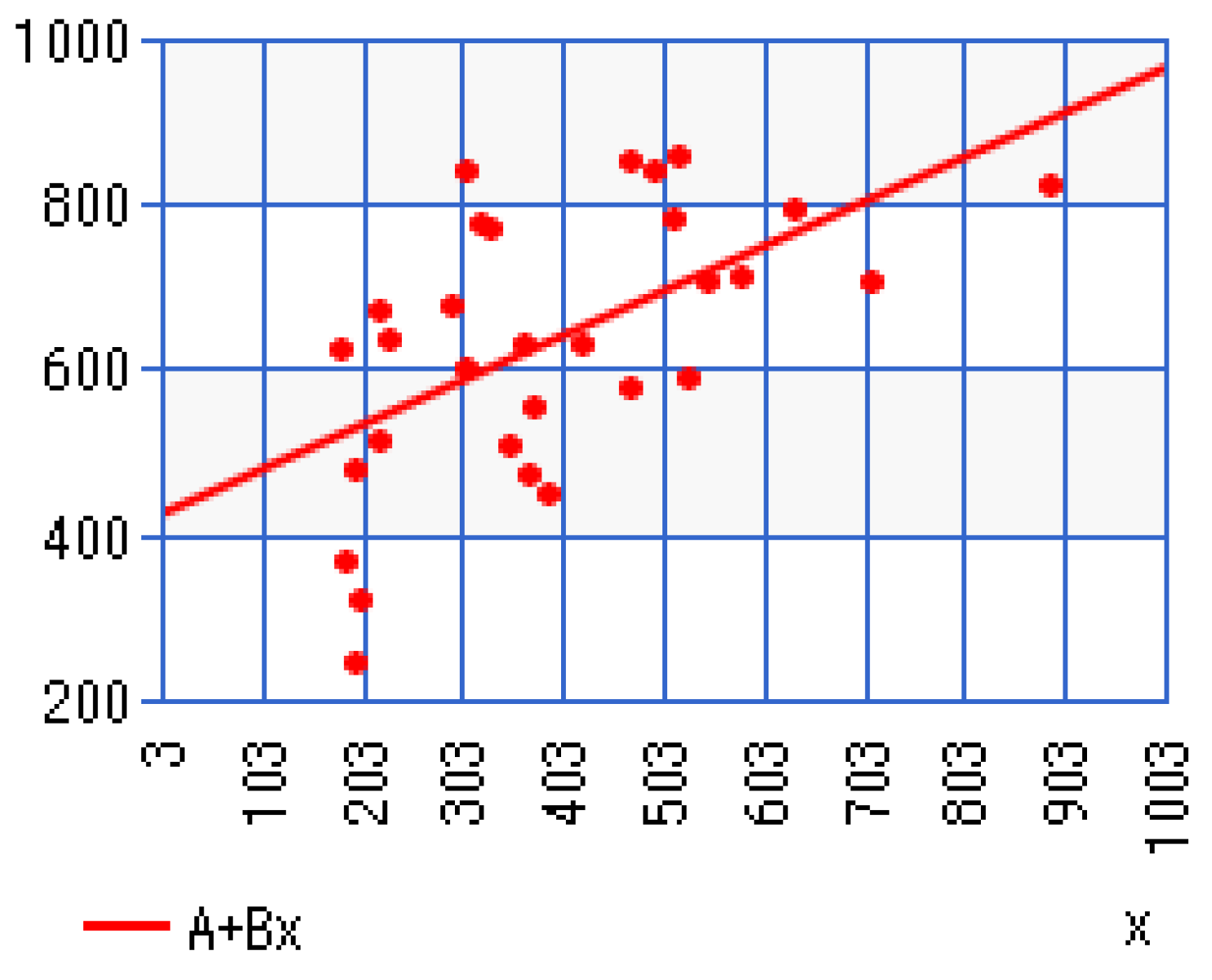
6.2. Quantitative Evaluation of the System
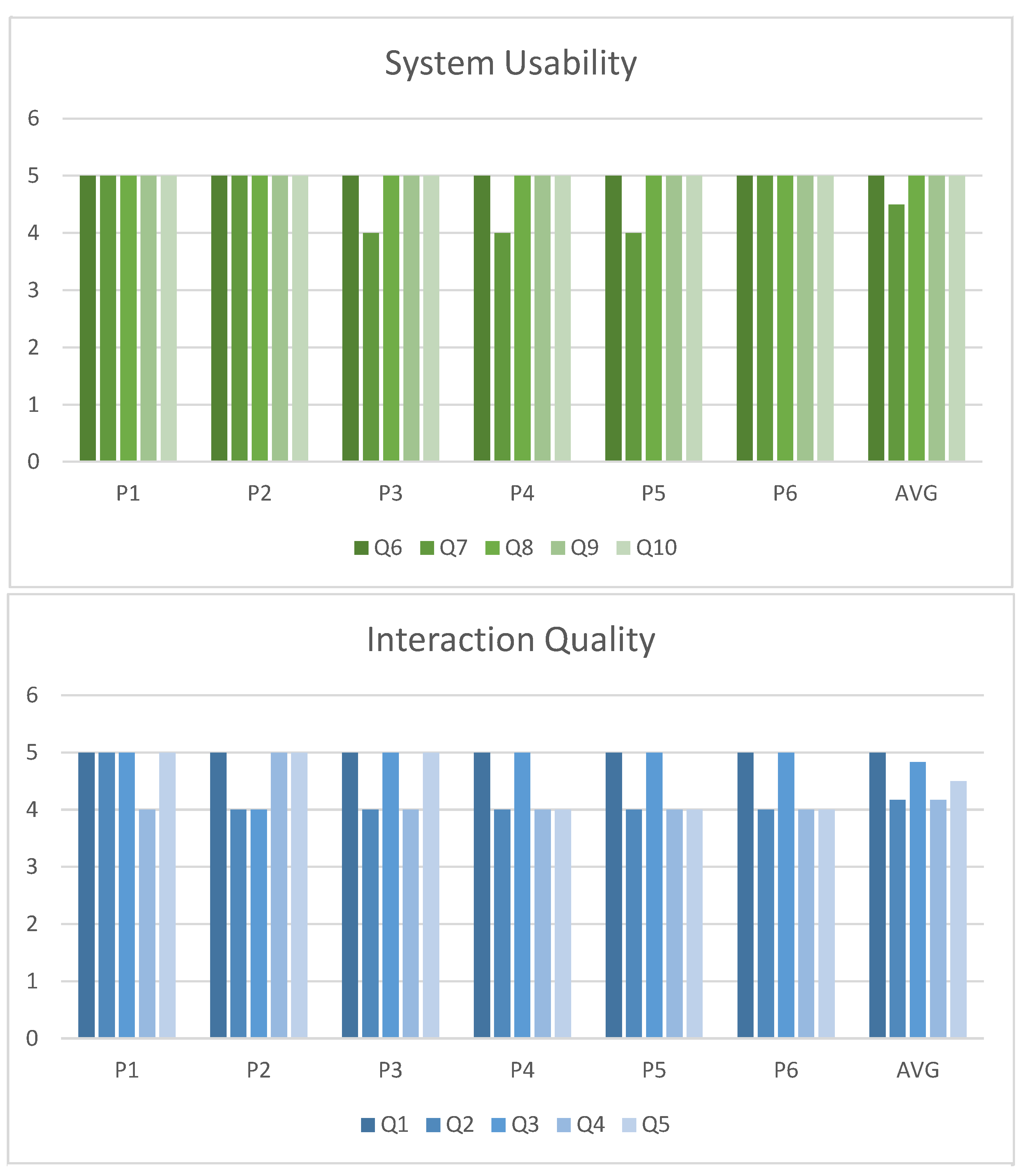
6.3. Qualitative Evaluation of the System
- Q1:
- The KINOPTIM system is easy to use:
- Q2:
- The KINOPTIM system is comfortable:
- Q3:
- The KINOPTIM system is easy to learn:
- Q4:
- The KINOPTIM system is efficient to complete the exercises:
- Q5:
- The graphical interface of this system is pleasant:
- Q6:
- The system stimulates the level of involvement:
- Q7:
- You are interested in the KINOPTIM system:
- Q8:
- The system helps in the physical activity:
- Q9:
- The system enhances physical activity:
- Q10:
- The presence of the score helps to improve the postures:
7. Discussion
8. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- World Health Organization. Fact Sheet 404 September 2015. 2015. Available online: http://www.who.int/mediacentre/factsheets/fs404/en/ (accessed on 16 January 2017).
- World Health Organization. WHO Global Report on Falls Prevention in Older Age; World Health Organization: Geneva, Switzerland, 2008. [Google Scholar]
- Ejupi, A.; Gschwind, Y.J.; Valenzuela, T.; Lord, S.R.; Delbaere, K. A kinect and inertial sensor-based system for the self-assessment of fall risk: A home-based study in older people. Hum. Comput. Interact. 2016, 31, 261–293. [Google Scholar] [CrossRef]
- Choi, S.D.; Guo, L.; Kang, D.; Xiong, S. Exergame technology and interactive interventions for elderly fall prevention: A systematic literature review. Appl. Ergonom. 2016, 65, 570–581. [Google Scholar] [CrossRef] [PubMed]
- Byrne, C.A.; Collier, R.; O’Hare, G.M.P. A Review and Classification of Assisted Living Systems. Information 2018, 9, 182. [Google Scholar] [CrossRef]
- Heinz, M.; Cho, J.; Kelly, N.; Martin, P.; Wong, J.; Franke, W.; Hsieh, W.H.; Blaser, J. The Potential of Three Computer-Based Communication Activities for Supporting Older Adult Independent Living. Information 2016, 7, 26. [Google Scholar] [CrossRef]
- Meekes, W.; Stanmore, E.K. Motivational Determinants of Exergame Participation for Older People in Assisted Living Facilities: Mixed-Methods Study. J. Med. Internet Res. 2017, 19, e238. [Google Scholar] [CrossRef] [PubMed]
- Civita, A.; Fiori, S.; Romani, G. A Mobile Acquisition System and a Method for Hips Sway Fluency Assessment. Information 2018, 9, 321. [Google Scholar] [CrossRef]
- Konstantinidis, E.; Billis, A.; Paraskevopoulos, I.T.; Bamidis, P. The interplay between IoT and serious games towards personalised healthcare. In Proceedings of the IEEE 9th International Conference on Virtual Worlds and Games for Serious Applications (VS-Games), Athens, Greece, 6–8 September 2017; pp. 249–252. [Google Scholar]
- Bieryla, K.A.; Dold, N.M. Feasibility of Wii Fit training to improve clinical measures of balance in older adults. Clin. Interv. Aging 2013, 8, 775–781. [Google Scholar] [CrossRef] [PubMed]
- Madhushri, P.; Dzhagaryan, A.; Jovanov, E.; Milenkovic, A. An mHealth Tool Suite for Mobility Assessment. Information 2016, 7, 47. [Google Scholar] [CrossRef]
- Birt, J.; Stromberga, Z.; Cowling, M.; Moro, C. Mobile Mixed Reality for Experiential Learning and Simulation in Medical and Health Sciences Education. Information 2018, 9, 31. [Google Scholar] [CrossRef]
- Mittelstadt, B. Designing the Health-related Internet of Things: Ethical Principles and Guidelines. Information 2017, 8, 77. [Google Scholar] [CrossRef]
- Mortazavi, B.; Nyamathi, S.; Lee, S.I.; Wilkerson, T.; Ghasemzadeh, H.; Sarrafzadeh, M. Near-realistic mobile exergames with wireless wearable sensors. IEEE J. Biomed. Health Inform. 2014, 18, 449–456. [Google Scholar] [CrossRef] [PubMed]
- Morando, M.; Ponte, S.; Ferrara, E.; Dellepiane, S. Definition of Motion and Biophysical Indicators for Home-Based Rehabilitation through Serious Games. Information 2018, 9, 105. [Google Scholar] [CrossRef]
- Lauzé, M.; Martel, D.; Agnoux, A.; Sirois, M.J.; Émond, M.; Daoust, R.; Aubertin-Leheudre, M. Feasibility, acceptability and effects of a home-based exercise program using a gerontechnology on physical capacities after a minor injury in community-living older adults: A pilot study. J. Nutr. Health Aging 2018, 22, 16–25. [Google Scholar] [CrossRef] [PubMed]
- Courtial, E.; Palestra, G.; Rebiai, M. A Tailored Serious Game for Preventing Falls of the Elderly. In Proceedings of the International Conference on Augmented Reality, Virtual Reality and Computer Graphics, Ugento, Italy, 12–15 June 2017; Springer: Berlin, Germany, 2017; pp. 230–239. [Google Scholar]
- Smeddinck, J.D.; Herrlich, M.; Malaka, R. Exergames for physiotherapy and rehabilitation: A medium-term situated study of motivational aspects and impact on functional reach. In Proceedings of the 33rd Annual ACM Conference on Human Factors in Computing Systems, Seoul, Korea, 18–23 April 2015; pp. 4143–4146. [Google Scholar]
- Brox, E.; Konstantinidis, S.T.; Evertsen, G.; Fernandez-Luque, L.; Remartinez, A.; Oesch, P.; Civit, A. Gameup: Exergames for mobility—A project to keep elderly active. In Proceedings of the XIV Mediterranean Conference on Medical and Biological Engineering and Computing, Paphos, Cyprus, 31 March–2 April 2016; Springer: Berlin, Germany, 2016; pp. 1225–1230. [Google Scholar]
- Brox, E.; Konstantinidis, S.T.; Evertsen, G. User-Centered Design of Serious Games for Older Adults Following 3 Years of Experience With Exergames for Seniors: A Study Design. JMIR Serious Games 2017, 5, e2. [Google Scholar] [CrossRef] [PubMed]
- Eltoukhy, M.A.; Kuenze, C.; Oh, J.; Signorile, J.F. Validation of static and dynamic balance assessment using Microsoft Kinect for young and elderly populations. IEEE J. Biomed. Health Inform. 2018, 22, 147–153. [Google Scholar] [CrossRef] [PubMed]
- Kawamoto, A.L.S.; da Silva, F.S.C. Depth-Sensor Applications for the Elderly: A Viable Option to Promote a Better Quality of Life. IEEE Consum. Electron. Mag. 2018, 7, 47–56. [Google Scholar] [CrossRef]
- Bird, M.; Clark, B.; Millar, J.; Whetton, S.; Smith, S. Exposure to ’Exergames’ Increases Older Adults’ Perception of the Usefulness of Technology for Improving Health and Physical Activity: A Pilot Study. JMIR Serious Games 2015, 3, e8. [Google Scholar] [CrossRef] [PubMed]
- Barelle, C.; Courtial, E.; Vellidou, E.; Tsirbas, H.; Tagaris, T.; Ibanez, F.; Sanchez, E.; Koutsouris, D. Tele-monitoring and diagnostic for fall prevention: The KINOPTIM concept. In Proceedings of the IEEE-EMBS International Conference on Biomedical and Health Informatics (BHI), Valencia, Spain, 1–4 June 2014; pp. 342–345. [Google Scholar]
- Barelle, C.; Tsirbas, C.; Ibanez, F.; Vellidou, E.; Tagaris, T.; Koutsouri, G.; Koutsouris, D. KINOPTIM: A Tele-rehabilitation gaming Platform for Fall Prevention in the Elderly Community. Int. J. Health Res. Innov. 2014, 2, 37–49. [Google Scholar]
- Courtial, E.; Brulin, D. A Decision Support System for Preventing Falls in Elderly People. In Proceedings of the 5th EAI International Conference on Wireless Mobile Communication and Healthcare, London, UK, 14–16 October 2015; pp. 108–112. [Google Scholar]
- Kouris, I.; Tsirbas, C.; Tagaris, T.; Vellidou, E.; Vartholomeos, P.; Rizou, S.; Koutsouris, D. KINOPTIM: The medical business intelligence module for fall prevention of the elderly. In Proceedings of the IEEE 15th International Conference on Bioinformatics and Bioengineering (BIBE), Belgrade, Serbia, 2–4 November 2015; pp. 1–4. [Google Scholar]
- Cavanagh, P.; Evans, J.; Fiatarone, M.; Hagberg, J.; McAuley, E.; Startzell, J. Exercise and physical activity for older adults. Med. Sci. Sports Exerc. 1998, 30, 1–29. [Google Scholar]
- Chodzko-Zajko, W.J.; Proctor, D.N.; Singh, M.A.F.; Minson, C.T.; Nigg, C.R.; Salem, G.J.; Skinner, J.S. Exercise and physical activity for older adults. Med. Sci. Sports Exerc. 2009, 41, 1510–1530. [Google Scholar] [CrossRef]
- Asakawa, Y.; Ikezoe, T.; Hazaki, K.; Kawano, I.; Irie, S.; Kanzaki, H.; Aoki, N. Relationship between falls and knee extension strength in the elderly. J. Phys. Ther. Sci. 2001, 8, 45–48. [Google Scholar] [CrossRef]
- Katz, S.; Downs, T.D.; Cash, H.R.; Grotz, R.C. Progress in development of the index of ADL. Gerontologist 1970, 10, 20–30. [Google Scholar] [CrossRef] [PubMed]
- Hunt, S.M.; McKenna, S.P.; McEwen, J.; Williams, J.; Papp, E. The Nottingham Health Profile: Subjective health status and medical consultations. Soc. Sci. Med. A Med. Psychol. Med. Sociol. 1981, 15, 221–229. [Google Scholar] [CrossRef]
- Palestra, G.; Rebiai, M.; Courtial, E.; Giokas, K.; Koutsouris, D. A Fall Prevention System for the Elderly: Preliminary Results. In Proceedings of the IEEE 30th International Symposium on Computer-Based Medical Systems (CBMS), Thessaloniki, Greece, 22–24 June 2017; pp. 550–551. [Google Scholar]
- Rusu, C.; Rusu, V.; Roncagliolo, S.; González, C. Usability and user experience: what should we care about? Int. J. Inf. Technol. Syst. Approach (IJITSA) 2015, 8, 1–12. [Google Scholar] [CrossRef]
- Gschwind, Y.J.; Schoene, D.; Lord, S.R.; Ejupi, A.; Valenzuela, T.; Aal, K.; Woodbury, A.; Delbaere, K. The effect of sensor-based exercise at home on functional performance associated with fall risk in older people—A comparison of two exergame interventions. Eur. Rev. Aging Phys. Act. 2015, 12, 11. [Google Scholar] [CrossRef] [PubMed]
- Ng, P.Y.; Ng, C.K.; Al-Haddad, S.A.R. Physiotherapy for Elderly through Exergames using Microsoft Kinect Sensor. Proc. Asia-Pac. Adv. Netw. 2015, 40, 119–129. [Google Scholar] [CrossRef][Green Version]
- Gioftsidou, A.; Vernadakis, N.; Malliou, P.; Batzios, S.; Sofokleous, P.; Antoniou, P.; Kouli, O.; Tsapralis, K.; Godolias, G. Typical balance exercises or exergames for balance improvement? J. Back Musculoskelet. Rehabil. 2013, 26, 299–305. [Google Scholar] [CrossRef] [PubMed]
- Sato, K.; Kuroki, K.; Saiki, S.; Nagatomi, R. The effects of exercise intervention using KinectTM on healthy elderly individuals: A quasi-experimental study. Open J. Ther. Rehabil. 2014, 2, 38. [Google Scholar] [CrossRef][Green Version]
- Planinc, R.; Nake, I.; Kampel, M. Exergame design guidelines for enhancing elderly’s physical and social activities. In Proceedings of the Third International Conference on Ambient Computing, Applications, Services and Technologies (AMBIENT 2013), Porto, Portugal, 29 September–3 October 2013; pp. 58–63. [Google Scholar]
- Bamidis, P.; Gabarron, E.; Hors-Fraile, S.; Konstantinidis, E.; Konstantinidis, S.; Rivera, O. Gamification and behavioral change: Techniques for health social media. In Participatory Health Through Social Media; Elsevier: Amsterdam, The Netherlands, 2016; pp. 112–135. [Google Scholar]
- De Carolis, B.; Ferilli, S.; Palestra, G. Simulating empathic behavior in a social assistive robot. Multimed. Tools Appl. 2017, 76, 5073–5094. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| ID | Gender | Age | ADL Score | Falls (in the Last 12 Months) |
|---|---|---|---|---|
| P1 | M | 85 | 5 | 0 |
| P2 | F | 74 | 6 | 3 |
| P3 | F | 81 | 6 | 1 |
| P4 | F | 85 | 5 | 0 |
| P5 | M | 78 | 6 | 1 |
| P6 | M | 79 | 5 | 0 |
| P1 | P2 | P3 | P4 | P5 | P6 | |
|---|---|---|---|---|---|---|
| Physical abilities (PA) | 0 | 21.15 | 21.13 | 22.9 | 0 | 0 |
| Social isolation (SI) | 0 | 0 | 34.95 | 20.43 | 40.86 | 0 |
| Pain (P) | 0 | 0 | 20.13 | 0 | 17.66 | 18.14 |
| Emotional reaction (ER) | 0 | 0 | 19.44 | 0 | 7.58 | 18.41 |
| Energy level (EL) | 0 | 0 | 0 | 0 | 0 | 0 |
| Sleep (S) | 0 | 0 | 20.36 | 0 | 0 | 46.69 |
| Participant | t-Test | p-Value |
|---|---|---|
| P1 | 3.240870 | 0.031648 * |
| P2 | 1.930274 | 0.125776 |
| P3 | 3.727427 | 0.020342 * |
| P4 | 3.123671 | 0.035401 * |
| P5 | 3.648106 | 0.021808 * |
| P6 | 14.121438 | 0.000146 *** |
| Exergame | t-Test | p-Value |
|---|---|---|
| Arm extension | −4.30733 | 0.000142 *** |
| Knee extension | −3.61104 | 0.00238 ** |
| Sideways leg lift | −2.22908 | 0.018169 * |
| S1 | S2 | S3 | S4 | S5 | S6 | S7 | S8 | S9 | |
|---|---|---|---|---|---|---|---|---|---|
| P1 | 401 | 414 | 456 | 559 | 570 | 518 | 583 | 565 | 621 |
| P2 | 610 | 697 | 721 | 837 | 835 | 588 | 624 | 676 | 761 |
| P3 | 371 | 540 | 619 | 641 | 656 | 664 | 666 | 666 | 662 |
| P4 | 218 | 333 | 344 | 372 | 407 | 425 | 445 | 435 | 440 |
| P5 | 527 | 592 | 597 | 600 | 615 | 786 | 789 | 793 | 776 |
| P6 | 227 | 259 | 451 | 518 | 654 | 648 | 631 | 623 | 626 |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Palestra, G.; Rebiai, M.; Courtial, E.; Koutsouris, D. Evaluation of a Rehabilitation System for the Elderly in a Day Care Center. Information 2019, 10, 3. https://doi.org/10.3390/info10010003
Palestra G, Rebiai M, Courtial E, Koutsouris D. Evaluation of a Rehabilitation System for the Elderly in a Day Care Center. Information. 2019; 10(1):3. https://doi.org/10.3390/info10010003
Chicago/Turabian StylePalestra, Giuseppe, Mohamed Rebiai, Estelle Courtial, and Dimitrios Koutsouris. 2019. "Evaluation of a Rehabilitation System for the Elderly in a Day Care Center" Information 10, no. 1: 3. https://doi.org/10.3390/info10010003
APA StylePalestra, G., Rebiai, M., Courtial, E., & Koutsouris, D. (2019). Evaluation of a Rehabilitation System for the Elderly in a Day Care Center. Information, 10(1), 3. https://doi.org/10.3390/info10010003