1. Air Quality in a Large Area of Northern Italy (the Po Valley) has been Severely Compromised for Decades
For many years, studies have been conducted into interactions between environmental pollution and the incidence of acute and chronic diseases. By way of example, in 1997, Cesare Cislaghi and Pier Luigi Nimis published an authoritative paper [
1] on the striking correlation between lung cancer mortality in the “young” male population (<55 years) and the level of atmospheric pollution (
Figure 1). Lichens are exceptional for biomonitoring air quality, and the paper met with considerable interest from the scientific world. This multi-year experimental investigation was carried out across the entire Italian region of Veneto (approximately 4 million inhabitants at the time of the experiment). Whilst this authoritative study managed to raise the alarm, administrators have since failed to take any real steps to limit the impact of air pollution (and environmental contamination in general).
A number of years later, in 2013, the Lyon-based International Agency for Research on Cancer (IARC—an agency that analyzes and classifies cancer-causing agents and substances on behalf of the World Health Organization) formally ranked the cocktail of combustions caused by traffic, heating, and industrial emissions in “group 1—definitely carcinogenic”. Accordingly, since 2013 the IARC, as the world’s leading cancer authority, has officially stated that particulates and various substances found in the atmosphere of our cities represent an unequivocally carcinogenic mixture for humans. Consider in this regard that particulate matter and tropospheric ozone have such negative effects on human health that, in many areas of the world, they surpass the total toxicity attributable to all the other airborne substances.
Given the above, a clarification should be made: areas particularly susceptible to pollution (especially to atmospheric pollution) include the vast urban and suburban districts/territories of Los Angeles, Mexico City, Central/Southern Asia, and the Chinese metropolises. Unfortunately, they also comprise the Po Valley in Northern Italy [
2,
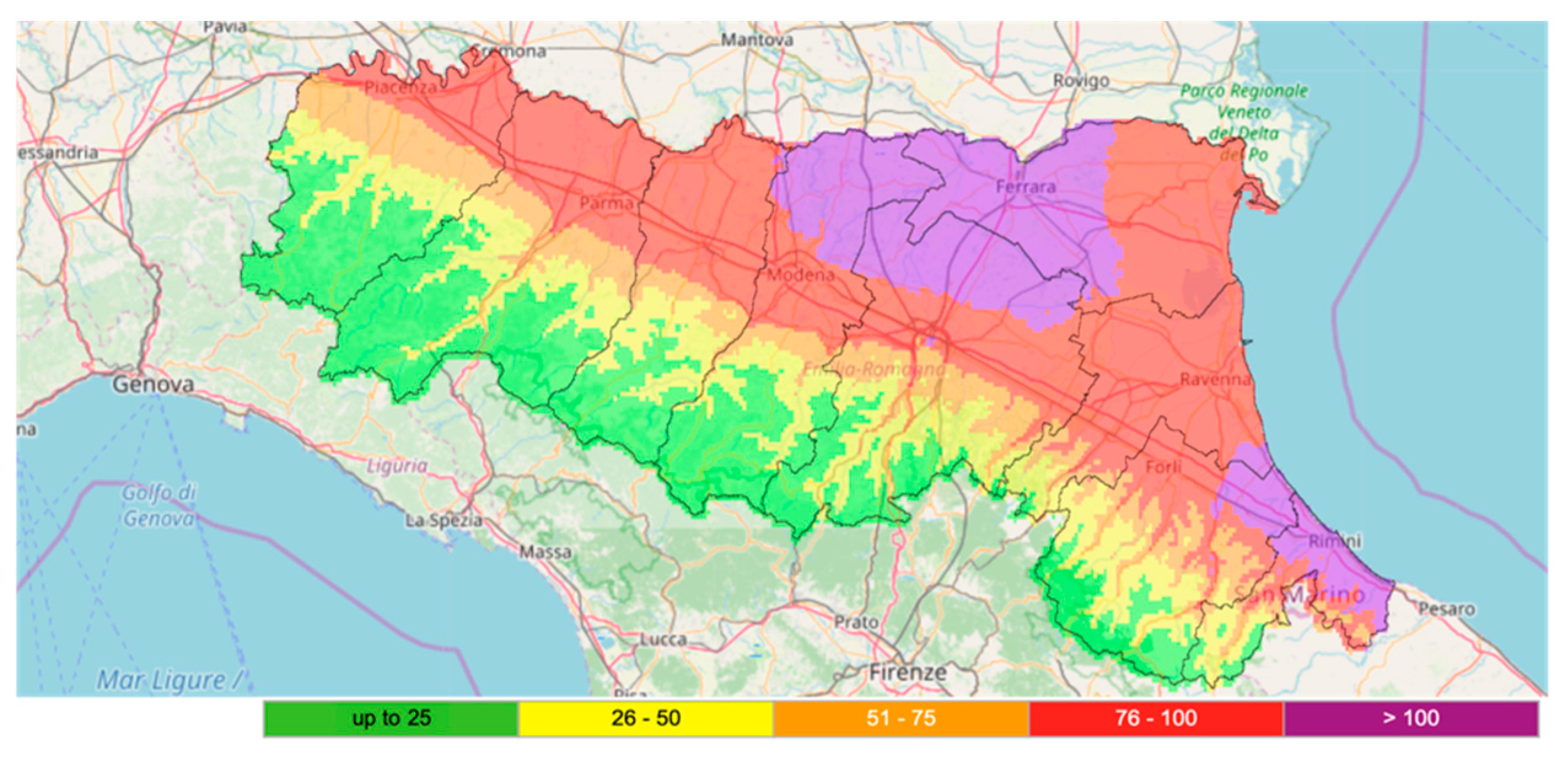
3], formed by part of the regions of Piedmont, Lombardy, Emilia-Romagna, Veneto, and Friuli-Venezia Giulia. In actual fact, values of air pollution in the Po Valley exceed target limits to an almost chronic and sometimes alarming extent (see
Figure 2 for a representative example). Due to the presence of the Alps (Central-Southern Europe’s highest mountains), which close the Italian peninsula to the northwest, overall reduced wind speed, average continental temperatures, high atmospheric humidity, and huge anthropic pressure, the Po Valley unfortunately has a series of characteristics that make it ideal for chronic persistence of pollutants, which are damaging for air, water, soil, and the organisms that populate them, including people.
Thus, it is no coincidence that in the Po Valley, as indeed in Chinese metropolises, trends in certain contaminants are not decreasing over time; instead they are stationary, or even increasing. In relatively restricted, highly urbanized areas, the levels of pollutants often reach extreme peaks that damage the environment and pose a serious threat to human health. The damp climate, the absence of adequate ventilation, and in some cases the low temperatures are clearly all factors that combine to causing atmospheric stagnation, thus contributing towards air pollution.
2. Origin and Characteristics of Particulates
Particulates are microscopic solid or liquid particles temporarily suspended in the air. Aerosols, i.e., a combination of liquid droplets and solid particles, are also a form of particulate. The main natural and anthropogenic sources are volcano emissions, sand, rock erosion, forest fires, leaf litter, sewage manure spreading, pollens, lichen propagules, micrometeorites, quarries, mines, landfills, incinerators, cement plants, crumbled plaster, asphalt, motorized traffic, wear of brakes and tires, exhaust gases from aircraft engines, industrial fumes, domestic heating, foundries, steel mills, coal or heavy oil power plants, etc. Particulates also form abundantly in the atmosphere when low vapor pressure substances condensate, and/or following (photo)chemical reactions between gaseous primary pollutants, such as nitrogen and sulfur oxides, ozone, volatile organic compounds, and ammonia; all these are substances found in considerable amounts in densely-populated areas.
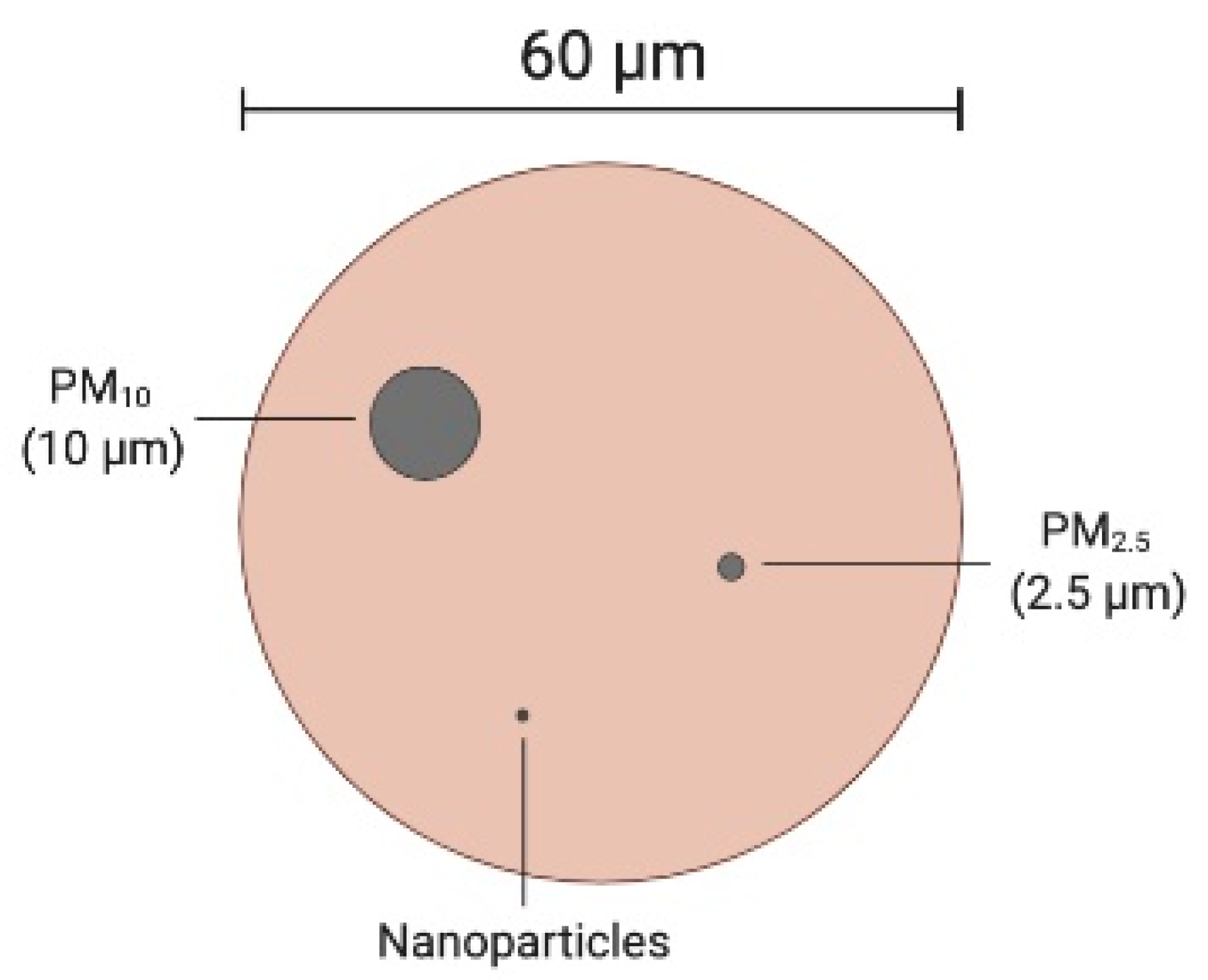
From a dimensional standpoint, particles that make up particulates are considered “coarse” if they have a diameter greater than 2.5 µm. Below this size, they are called “fine or thin” (<2.5 µm, up to 100 nm), “ultrafine” (up to 10 nm), or “nanoparticles” (up to 2 or very few nm). Refer to
Figure 3 for a comparison between the average diameter of a human hair and some different airborne particles.
The amount of particulate matter in a certain volume of air is indicated by an index, called PM (which stands for “particulate matter”). The most common PM indices are PM
10 and PM
2.5, which indicate the total concentration of particles with a diameter of less than 10 and 2.5 µm, respectively. PM concentrations are currently expressed in µg m
−3 of air. Unfortunately, there are still no official indices for ultrafine particles and nanoparticles. We can get an understanding of the “order of magnitude” if we bear in mind that the amount of particulate matter that can accumulate annually in a polluted area is in the order of hundreds of tons per 10,000 m
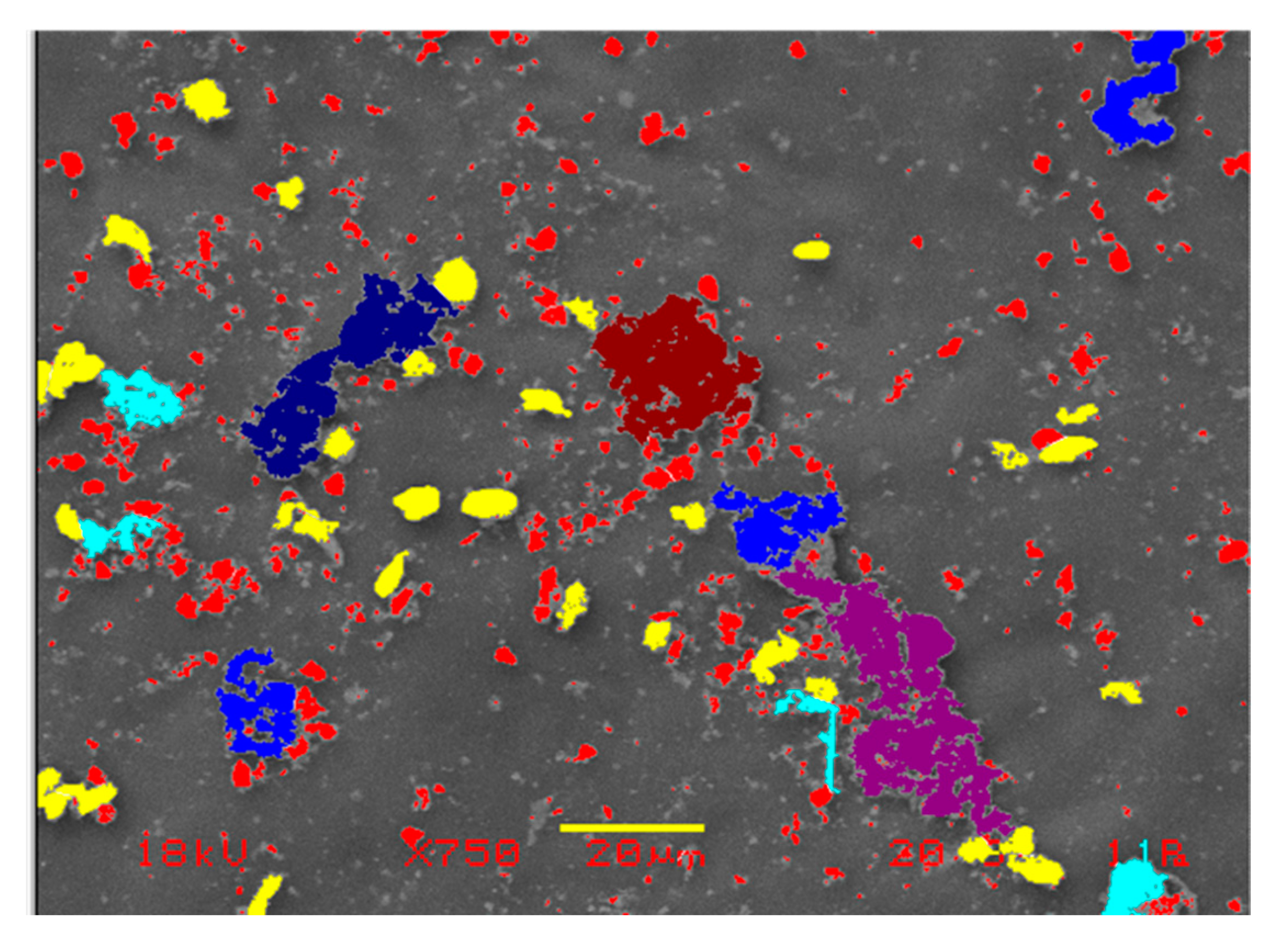
2 (per hectare). See
Figure 4 for a microscopic observation of the particulate matter deposited on a biological surface.
The World Health Organization has established that the maximum tolerable limits of PM10 and PM2.5 must not exceed an annual average of 20 and 10 µg m−3 of air, respectively; and 50 and 25 µg m−3 of air in 24 h, respectively. In the European Union and in Italy, the limits are as follows (Legislative Decree 155 of 13/8/2010 and EU Directive 2008/50/EC):
PM10: 40 µg m−3 not to be exceeded as annual mean; and 50 µg µg m−3 not to be exceeded more than 35 times per year as daily mean.
PM2.5: 25 µg m−3 not to be exceeded as annual mean, with the aim of not exceeding 20 µg m−3 as an annual mean starting from 1 January 2020.
3. Particulate Matter has Very Negative Effects on Environmental and Human Health
Given the above, based on current legislation, the overall situation in Italy (particularly in the Po Valley) is far from reassuring, because the legal limits are frequently exceeded, sometimes constantly in autumn/winter. The United Nations Environmental Program predicts that from 2020 the number of deaths in the world from air pollution could exceed 8 million (whilst in 2001 they numbered around 3 million). Unfortunately, little or nothing is known about fine, ultrafine, and nanoparticles, although they can in fact have a devastating impact on human health [
4,
5,
6,
7]. However, one thing is clear: fine, ultrafine, and nanoparticles are like gases, and tend to remain in suspension almost indefinitely. Simply put, a particle with a diameter half that of another, settles four times slower than the first. Indeed, the smaller the particles, the deeper they penetrate tissues and cells (even in our lungs), causing serious damage and/or carrying toxic substances, spores, viruses, bacteria [
8,
9,
10,
11,
12,
13], and in general anything that should not normally enter the body. One significant example is cadmium oxide (CdO), a constituent of particulate matter that has been associated with a 2.5-fold increase in the risk of chronic obstructive pulmonary disease [
14].
In this regard, we should bear in mind one serious issue as regards indices coded by law for measuring the atmospheric particulate matter. For many years now, it has been a given that 1000 atmospheric particles of 1 µm (and, what is even more serious, one million particles from 100 nm) weigh as much as a single 10 µm particle [
15]. However, as Dr. Stefano Montanari correctly points out, “the law makes no difference between a large particle and a million small particles. For science, however, the difference is immense. The absurd paradox is that we could breathe air that is “officially” clean (i.e., polluted below the law limits), but in fact composed of thousands of particles that have a potentially devastating impact on our lungs, our blood and our health” [
15]. As a result, current legal limits are by no means a guarantee that the particulates have little impact on the environment or indeed on our bodies.
One notable feature of all particulates is that they can convey (and release) toxic molecules and/or microorganisms and/or spores and/or viral particles, etc. [
8,
9,
10,
11,
12,
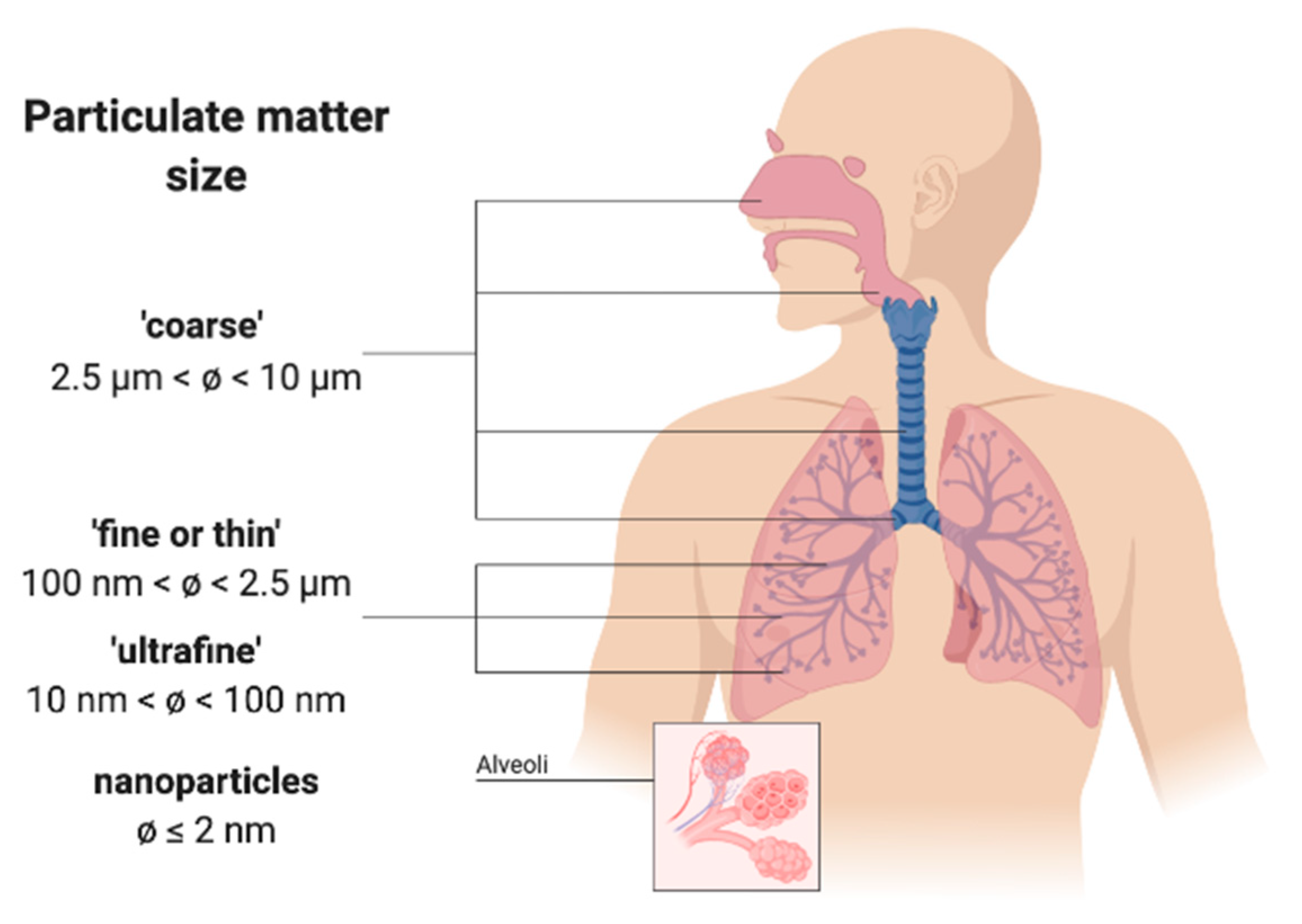
13]. These components can be absorbed or adsorbed by the particulate particles, depending on whether they enter them (where they are potentially solubilized), or whether they bind to the external surface. Moreover, the particles can be broken, thus multiplying their polluting and carrying power. Particulate matter, especially fine/ultrafine/nanoparticles, can enter the bronchi and the lung alveoli (
Figure 5) as well as the blood (both plasma and erythrocytes), the coronary arteries, the heart, the lymphatic system, and, ultimately, almost all organs, with serious or very serious consequences for health (e.g., carcinogenic and/or teratogenic effects). Last but not least, the smallest particles can enter the cell nucleus and target DNA, with devastating results [
16].
As long ago as 1997–2001, official studies carried out by the Environmental Protection Agency of Italy’s Emilia-Romagna region (in the March–April 2020 “red zone”, due to the novel coronavirus spread) stated that “the qualitative and quantitative differences of the mutagenic effects found in samples of atmospheric particulate taken at different points of the network, as well as on the same site at different times, underline how urban atmospheric particulate matter is a complex mixture of mutagenic substances in continuous evolution, following changes in pressure factors and sources of pollutants, the influence of weather-climate conditions, place, seasonality, etc. The evidence of biological activity and the presence of ultrafine particles, above all PM2.5, poses an important risk factor for the health of citizens; it is therefore necessary to commit resources to primary prevention, particularly for long-term health effects, as a consequence of exposure to the finest particles”. The above was published in a report by Dr. Francesca Cassoni back in August 2002. What has changed in the intervening decades? Almost nothing, unfortunately.
4. Particulate Matter Causes Severe Diseases, but Drastic Measures to Reduce It have yet to be Taken
Taking all the above into account, we reach here the core of the whole issue: authoritative international publications have correlated atmospheric particulate matter with increased incidence of human diseases, including viral ones. In particular, lung diseases are significantly affected by the level of contamination in the atmosphere.
Italy’s Po Valley is doubtless one of the most polluted areas in the world [
2,
3]. Alarmingly, in this area, atmospheric particulate levels are comparable with those found in the Chinese metropolises, such as Wuhan (Central-Eastern China, over 6 million inhabitants). Of course, we are not presenting here a simplistic argument that deterioration of the environment is the
only cause of the increase in viral diseases, in this case, of viruses associated with respiratory infections such as the novel coronavirus, but we are very inclined to believe that it is a
significant contributing cause.
We examined authoritative scientific literature in the world’s leading databases. By way of example, this included an interesting publication entitled: “PM
10 exposure is associated with increased hospitalizations for respiratory syncytial virus bronchiolitis among infants in Lombardy, Italy” [
17]. This viral disease affecting children can become very severe and therefore require immediate hospitalization. The aforementioned scientists write that “exposure to environmental factors (e.g., air pollution) could influence the immune system and compromise its ability to limit the spread of infectious agents”, as is the case with the virus they studied. In addition, they add, “Exposure to air pollution is related to the worsening of respiratory diseases in adults and children”, along the same lines of the findings reported by Jo et al. [
18] in relation to Korea (also badly affected by the novel coronavirus). Carugno and et al. [
17] conclude that the concentration of PM
10 in Lombardy, Italy, in the two weeks preceding hospitalization was strongly associated with an increased risk of hospitalization for the viral pathology they studied. This general conclusion is also supported by research carried out by various groups in Israel, Chile, Canada, Australia, and New Zealand, to name a few [
19,
20,
21,
22].
Another distinguished study carried out in China on over 36,000 children (city of Hangzhou, over 6 million inhabitants, Eastern China), reveals a positive correlation between infection with respiratory syncytial virus and atmospheric levels of PM
2.5 and PM
10 (almost systematically above the limits imposed by the World Health Organization); conversely, there is a negative correlation with temperature [
23]. This means that higher temperatures have led to a decrease in the infection rate. Within the framework of the research, the most critical situation arose below 9 °C, while there was a marked improvement in health where temperatures were upwards of 20 °C. Essentially, similar results have been found by a number of studies conducted worldwide. In fact, dozens of experimental works published in international scientific journals have highlighted the close link between the level of air pollution and the incidence of respiratory diseases (including viral ones). They include Gordon et al., 2014; Liang et al., 2014; Walton et al., 2010; and Xu et al., 2013, to name a few [
4,
24,
25,
26].
In this regard, some scientists believe that the oxidative stress caused by air pollution, and in particular by particulate matter, may have negative effects on immune responses by interfering with the body’s antiviral defenses. Some studies actually support the theory that exposure to atmospheric pollutants can in fact (1) reduce the ability of macrophages to phagocytize pathogens, even viral ones; and (2) decrease the expression or activity of particular protective proteins against viral infections [
10].
A large number of epidemiological studies conducted worldwide have found a clear link between air pollution levels and hospitalization for various diseases, particularly of a respiratory kind, as well as greater associated morbidity and mortality. Viral respiratory infections can be caused by over 200 different viruses, including rhinovirus, respiratory syncytial virus, influenza and parainfluenza virus, coronavirus, and adenovirus [
27]. Unfortunately, regulations concerning microbial air contamination are lacking.
As regards the “novel coronavirus” (SARS-CoV-2), which causes the current COVID-19 disease (an acronym of COronaVIrus Disease), Conticini et al. (2020) [
28] showed that atmospheric pollution can be considered a co-factor contributing to the extremely high level of lethality currently occurring in Northern Italy. Of course, it is not easy to discern between the rate of novel coronavirus spread in the population versus frequency of severe cases, as data in authoritative literature have been almost absent until now. However, Wu et al. (2020) [
29] have demonstrated a large overlap between cause of death in COVID-19 patients and long-term exposure to PM
2.5. In particular, these authors state that an increase of just 1 µg m
−3 in PM
2.5 is associated with a 15% increase in the COVID-19 death rate. In addition, correctly, they conclude, “The study results underscore the importance of continuing to enforce existing air pollution regulations to protect human health, both during and after the COVID-19 crisis”. In addition, Yao et al. (2020) [
30] found in 49 Chinese cities (including Wuhan) that COVID-19 death rates in winter 2020 were higher where concentrations of PM
2.5–10 were greater, possibly affecting the outcome for patients with mild to severe symptoms, and influencing the prognosis of COVID-19 patients. Also Martelletti and Martelletti (2020) [
31] postulated a correlation between elevated concentrations of PM and the high spread and mortality rate of the novel coronavirus in Italy.
5. Atmospheric Particulate Acts as a Carrier for Viruses, and might also Have Promoted the Spread of the Novel Coronavirus
The novel coronavirus (SARS-CoV-2), which has a diameter of 60–140 nm, is highly contagious, and spreads through respiratory droplets and/or direct contact. In general, temperature and humidity are known factors affecting the diffusion of viral diseases; in fact, it is no coincidence that many respiratory viruses become particularly active in autumn and winter (see above). Interestingly, very recent studies hypothesized significant SARS-CoV-2 spread in cities and areas following a narrow east-to-west corridor; this roughly corresponds with the 30–50° Northern latitude, characterized by average daily temperatures of 5–11 °C [
32]. Another factor that might promote the spread of this and other pathogens is overcrowding and movement of large numbers of individuals at a given time in limited spaces, such as in cities or other highly populated areas.
Besides all that, both in Milan (Italy) and in Wuhan (China), the levels of atmospheric particulate matter have greatly and constantly exceeded legal limits. Indeed, preliminary studies conducted by research groups headed by Bologna University and the “A. Moro” University of Bari, Italy, together with the Italian Society of Environmental Medicine (SIMA) have resulted in the publication of an interesting “position paper” offering strong support to the possible correlations between atmospheric particulate matter and the spread of coronavirus among the population [
33]. The researchers have in fact highlighted “a relationship between the exceedances of the legal limits of PM
10 concentrations recorded in the period 10–29 February 2020, and the number of cases infected with COVID-19 updated to 3 March 2020”. In particular, their paper stresses the direct relationship (R
2 = 0.98) between the number of COVID-19 cases and the PM
10 pollution status of each Italian province. To this end, the authors state, “The expansion curves of the infection show anomalous accelerations precisely in the regions located in the Po Valley, where the outbreaks are particularly virulent, and reasonably suggest a carrier-mediated spread. These analyses seem therefore to demonstrate that, in relation to the period 10–29 February, high concentrations above the PM
10 limit in some provinces of Northern Italy may have exerted an impulse to the virulent spread of the epidemic in the Po Valley, which was not observed in other areas of Italy that had cases of contagion in the same period. In this regard, the case of Rome is emblematic in which the presence of contagions was manifested in the same days as the Po regions without, however, triggering such a virulent phenomenon”. Essentially, the atmospheric particulate may have acted (and indeed might continue to act) as a carrier of the virus, increasing its spread (
Figure 6).
In the period 10–29 February 2020, in the city of Milan alone, PM
10 values actually reached peaks of 70–80 µg m
−3 (the legal limit is µg m
−3), while in the second half of January, at least two peaks of about 90 µg m
−3 were recorded. Following there is some additional information on PM
10 levels in Milan (data from:
www.arpalombardia.it):
Daily average for January 2020: 67.2 µg m−3 (minimum value 34 and maximum value 131): daily limit exceeded 23 times.
Daily average for February 2020: 45.2 µg m−3 (minimum value 13 and maximum value 81): daily limit exceeded 11 times, and in particular 7 times in the 14 days preceding the start of the rapid increase in infections in Lombardy.
In the same time period as above, PM2.5 stood at 40–50 µg m−3 (the legal limit being 25 µg m−3), while in the second half of January there were 2–3 peaks of up to 70 µg m−3, making for a highly compromised situation.
Likewise, Wuhan, where the outbreak preceded the one in Italy by about a month, PM10 peaks reached 120–130 µg m−3, whereas in the same dataset, PM2.5 displayed peaks of 100 µg m−3.
Thus, it is possible to make the assumption that particulate matter acts as a direct carrier for the novel coronavirus. “The finer the particles,” says Gianluigi de Gennaro of the University of Bari “the more highways are created for infections. It is necessary to reduce emissions to a minimum”. Concerning this, despite the current shortage of data showing that COVID-19 is “piggybacking” on air particulate matter, the assumption that air pollution facilitates the spread of different viruses was already shown by Cui et al. (2003) [
34] during the SARS-CoV-1 outbreak in China in November 2002. According to this research, the five areas under investigation (Guangdong, Shanxi, Hebei, Beijing, and Tianjin) presented a linear relationship between air pollution and fatality rate due to SARS. In this case, the lower the air pollution, the lower the mortality rate.
In fact, even animal viruses, which spread with ease in intensive farming, can be carried through the atmospheric particulate matter. By way of example, airborne transmission played a major role in the diffusion of the highly pathogenic avian influenza in the USA in 2015 [
35].
Interestingly, Reche et al. (2018) [
36] quantified the wet and dry deposition rates of free and attached viruses and bacteria in Spain (in areas located approximately 50 km southeast of Granada), demonstrating that billions of viruses per m
2 were deposited each day. Virus deposition rates were 9–461 times greater than bacteria rates, and positively correlated with organic aerosols <0.7 μm, implying that viruses could remain longer in the atmosphere, and might accordingly disperse further. Moreover, ~69% of viruses set down from the atmosphere were attached to dust or organic aggregates. Thus, a correlation between atmospheric particles and virus spread appears more likely than ever, if not certain.
Returning to the present day and to the novel coronavirus, van Doremalen et al. (2020) [
37] have stated that the stability of this virus on surfaces and in aerosols is, on average, very similar to that of SARS-CoV-1. In order to prove this, the authors employed a three-jet collision nebulizer to generate particles that, due to their small size (<5 μm), remained suspended in aerosols. As a consequence, active novel coronavirus was detected in aerosols up to 3 h post-aerosolization, up to 4 h on copper, and up to 7 days on other different surfaces. Novel coronavirus and SARS-CoV-1 exhibited similar half-lives in aerosols, with median estimates around 2.7 h. Thus, aerosol transmission of COVID-19 appears plausible, as the virus can remain active in aerosols for some hours, and even for days on surfaces. Last but not least, a recent study preliminarily recorded the presence of ribonucleic acid belonging to the novel coronavirus on the PM
10 collected in the province of Bergamo, Lombardy, [
38]. This could be a key piece of evidence, if definitely confirmed and integrated by further studies on the actual virulence of the virus vehiculated by the particulate, of the role of airborne particles in the direct spread of the SARS-CoV-2.
In this respect,
Table 1 indicates the ratio between the total COVID-19-positive cases (including those recovered and deceased) in each Italian region in the time range 24 February–17 April 2020, and the total population dwelling in the respective regions on 31 December 2019 (no more recent official data are available). From the values calculated in
Table 1, it is clear that in the regions of Northern Italy (and in particular the Po Valley) there is a greater number of COVID-19 cases in relation to the overall resident population than in the Central and Southern/Island regions. This north-to-south “downward gradient”, except for the Northern area of the Marche region (which we will not dwell on here for reasons of space), clearly reflects the far less alarming levels of atmospheric particulate that are largely found in Central and Southern Italy.
6. Conclusions
The Acting Secretary General of the European Public Health Alliance (EPHA) has declared: “The air may be clearing in Italy, but the damage has already been done to human health and people’s ability to fight off infection. Governments should have tackled chronic air pollution long ago, but have prioritised the economy over health. Science tells us that epidemics like COVID-19 will occur with increasing frequency. So, cleaning up the streets is a basic investment for a healthier future”. Indeed, administrators and governments must view potential interactions between exposure to pollutants (not only particulate matter, but also other solid, liquid, and gaseous contaminants) and the onset of pathologies (including those generated by respiratory viruses) as a tangible risk. The hypothesis that the novel coronavirus might exploit the “highways” made up of atmospheric particulates is a challenging point that, in our opinion, deserves further, immediate, and in-depth experimental investigations. It is to be hoped that steps will be taken promptly to clarify the dynamics involved in the current pandemic. However, above all, far-sighted measures are urgently needed to reduce air, water, and soil pollution drastically. The environment around us and our health demand it.










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}