
Sound Healing: Mood, Emotional, and Spiritual Well-Being Interrelationships


Abstract
1. Introduction
Sound Healing or “Sound Bath”
- (a)
- Gamma: over 30 Hz: the fastest brainwave. Processing of information from different brain areas.
- (b)
- Beta: 12–30 Hz: alert consciousness, concentration, focus, or anxiety.
- (c)
- Alpha: 8–12 Hz: relaxed, lucid, calm, peaceful.
- (d)
- Theta: 4–8 Hz: light sleep, meditation, or deep relaxation.
- (e)
- Delta: Less than 4 Hz: deep, dreamless sleep or deep state of meditation.
2. Method
2.1. Participants
2.2. Study Design
2.3. Sound Healing Protocol
2.4. Data Analysis
3. Results
4. Discussion
4.1. Limitations
4.2. Conclusions and Further Investigations
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A
- I feel peaceful.
- I have a reason for living.
- My life has been productive.
- I have trouble feeling peace of mind.
- I feel a sense of purpose in my life.
- I am able to reach down deep into myself for comfort.
- I feel a sense of harmony within myself.
- My life lacks meaning and purpose.
- I find comfort in my faith or spiritual beliefs.
- I find strength in my faith or spiritual beliefs.
References
- Ann, Ik-Soo, and Myungjin Bae. 2017. Analysis of Singing Bowl’s Sound. The Journal of the Acoustical Society of America 142: 2613. [Google Scholar] [CrossRef]
- Beri, Kavita. 2018. A future perspective for regenerative medicine: Understanding the concept of vibrational medicine. Future Science OA 4: FSO274. [Google Scholar] [CrossRef] [PubMed]
- Bidin, Livia, Luca Pigaiani, Manlio Casini, Pietro Seghini, and Luigi Cavanna. 2016. Feasibility of a trial with Tibetan Singing Bowls, and suggested benefits in metastatic cancer patients. A pilot study in an Italian Oncology Unit. European Journal of Integrative Medicine 8: 747–55. [Google Scholar] [CrossRef]
- Brady, Loretta L. C., and Amanda Hapenny. 2010. Giving Back and Growing in Service: Investigating Spirituality, Religiosity, and Generativity in Young Adults. Journal of Adult Development 17: 162–67. [Google Scholar] [CrossRef]
- Brown, David R., Jamie S. Carney, Mark S. Parrish, and John L. Klem. 2013. Assessing Spirituality: The Relationship Between Spirituality and Mental Health. Journal of Spirituality in Mental Health 15: 107–22. [Google Scholar] [CrossRef]
- Burtner, Matthew, Stephanie Serafin, and David Topper. 2002. Real-Time Spatial Processing and Transformations of a Singing Bowl. Paper presented at the 5th International Conference on Digital Audio Effects, Hamburg, Germany, September 26–28; p. 4. [Google Scholar]
- Carmody, James, George Reed, Jean Kristeller, and Phillip Merriam. 2008. Mindfulness, spirituality, and health-related symptoms. Journal of Psychosomatic Research 64: 393–403. [Google Scholar] [CrossRef]
- Cella, D. 2000. Assessment methods for quality of life in cancer patients: The FACIT measurement system. International Journal of Pharmaceutical Medicine 14: 78–81. [Google Scholar] [CrossRef]
- Chiesa, Alberto, and Alessandro Serretti. 2009. Mindfulness-Based Stress Reduction for Stress Management in Healthy People: A Review and Meta-Analysis. The Journal of Alternative and Complementary Medicine 15: 593–600. [Google Scholar] [CrossRef]
- de la Rubia Ortí, Jose Enrique, Maria Pilar García-Pardo, Carmen Cabanes Iranzo, Jose Juaquim Madrigal, Sandra Sancho Castillo, Mariano Julian Rochina, and Vicente Javier Gascó. 2018. Does Music Therapy Improve Anxiety and Depression in Alzheimer’s Patients? The Journal of Alternative and Complementary Medicine 24: 33–36. [Google Scholar] [CrossRef]
- Delgado, Cheryl. 2005. A Discussion of the Concept of Spirituality. Nursing Science Quarterly 18: 157–62. [Google Scholar] [CrossRef]
- Dennis, Kingsley L. 2010. Quantum Consciousness: Reconciling Science and Spirituality Toward Our Evolutionary Future(s). World Futures 66: 511–24. [Google Scholar] [CrossRef]
- Feller, Silke, Matthaeus Vigl, Manuela M. Bergmann, Heiner Boeing, Clemens Kirschbaum, and Tobias Stalder. 2014. Predictors of hair cortisol concentrations in older adults. Psychoneuroendocrinology 39: 132–40. [Google Scholar] [CrossRef] [PubMed]
- Fernando Pietro Peres, Mario, Helder H. Kamei, Patricia R. Tobo, and Giancarlo Lucchetti. 2018. Mechanisms Behind Religiosity and Spirituality’s Effect on Mental Health, Quality of Life and Well-Being. Journal of Religion and Health 57: 1842–55. [Google Scholar] [CrossRef]
- Garland, Sheila N., Linda E. Carlson, Sarah Cook, Laura Lansdell, and Michael Speca. 2007. A non-randomized comparison of mindfulness-based stress reduction and healing arts programs for facilitating post-traumatic growth and spirituality in cancer outpatients. Supportive Care in Cancer 15: 949–61. [Google Scholar] [CrossRef] [PubMed]
- Gaynor, Mitchell L. 1999. Sounds of Healing: A Physician Reveals the Therapeutic Power of Souond, Voice, and Music. New York: Broadway Books. [Google Scholar]
- Giordano, Filippo, Elide Scarlata, Mariagrazia Baroni, Eleonora Gentile, Filomena Puntillo, Nicola Brienza, and Loreto Gesualdo. 2020. Receptive music therapy to reduce stress and improve wellbeing in Italian clinical staff involved in COVID-19 pandemic: A preliminary study. The Arts in Psychotherapy 70: 101688. [Google Scholar] [CrossRef] [PubMed]
- Goldsby, Tamara L., and Michael E. Goldsby. 2020. Eastern Integrative Medicine and Ancient Sound Healing Treatments for Stress: Recent Research Advances. Integrative Medicine: A Clinician’s Journal 19: 7. [Google Scholar]
- Goldsby, Tamara L., Michael E. Goldsby, Mary McWalters, and Paul J. Mills. 2017. Effects of Singing Bowl Sound Meditation on Mood, Tension, and Well-being: An Observational Study. Journal of Evidence-Based Complementary & Alternative Medicine 22: 401–6. [Google Scholar] [CrossRef]
- Goldsby, Tamara. L., Michael E. Goldsby, Madisen Haines, Chiara Marrapodi, Jesus Saiz Galdos, Deepak Chopra, and Paul J. Mills. 2021. The Promise of Applying Systems Theory and Integrative Health Approaches to the Current Psychosocial Stress Pandemic. Journal of Public Health Issues and Practices 5: 1–11. [Google Scholar] [CrossRef]
- González-Sanguino, Clara, Berta Ausín, Miguel Ángel Castellanos, Jesús Saiz, Aída López-Gómez, Carolina Ugidos, and Manuel Muñoz. 2020. Mental Health Consequences of the Coronavirus 2020 Pandemic (COVID-19) in Spain. A Longitudinal Study. Frontiers in Psychiatry 11: 1256. [Google Scholar] [CrossRef]
- Goodin, Peter, Joseph Ciorciari, Kate Baker, Anne-Marie Carrey, Michelle Harper, and Jordy Kaufman. 2012. A High-Density EEG Investigation into Steady State Binaural Beat Stimulation. PLoS ONE 7: e34789. [Google Scholar] [CrossRef]
- Grayman-Simpson, Nyasha, and Jacqueline S. Mattis. 2013. “If It Wasn’t for the Church…”: Organizational Religiosity and Informal Community Helping among African American Adults. Journal of African American Studies 17: 243–52. [Google Scholar] [CrossRef]
- Guétin, S., F. Portet, M. C. Picot, C. Pommié, M. Messaoudi, L. Djabelkir, A. L. Olsen, M. M. Cano, E. Lecourt, and J. Touchon. 2009. Effect of Music Therapy on Anxiety and Depression in Patients with Alzheimer’s Type Dementia: Randomised, Controlled Study. Dementia and Geriatric Cognitive Disorders 28: 36–46. [Google Scholar] [CrossRef] [PubMed]
- Hackett, Ruth A., and Andrew Steptoe. 2017. Type 2 diabetes mellitus and psychological stress—A modifiable risk factor. Nature Reviews Endocrinology 13: 547–60. [Google Scholar] [CrossRef] [PubMed]
- Haney, Alison M., and David Rollock. 2020. A matter of faith: The role of religion, doubt, and personality in emerging adult mental health—PsycNET. Psychology of Religion and Spirituality 12: 247–53. [Google Scholar] [CrossRef]
- Hassan, Hasminda, Zunairah Haji Murat, Valerie Ross, and Norlida Buniyamin. 2012. A preliminary study on the effects of music on human brainwaves. Paper presented at the 2012 International Conference on Control, Automation and Information Sciences (ICCAIS), Saigon, Vietnam, November 26–29; pp. 176–80. [Google Scholar] [CrossRef]
- Hodapp, Bastian, and Christian Zwingmann. 2019. Religiosity/Spirituality and Mental Health: A Meta-analysis of Studies from the German-Speaking Area. Journal of Religion and Health 58: 1970–98. [Google Scholar] [CrossRef]
- Hohashi, Naohiro, Daiji Araki, Hisato Nakamae, and Naoki Motoda. 2004. Psychosomatic effects of healing music in comparison with noise: From changes in a brain waves, systolic blood pressure and pulse rate, and multiple mood as biological indicators. Japanese Journal of Health and Human Ecology 70: 134–45. [Google Scholar] [CrossRef]
- Inácio, Octávio, Luís L. Henrique, and José Antunes. 2006. The Dynamics of Tibetan Singing Bowls. Acta Acustica United with Acustica 92: 637–53. [Google Scholar]
- Kaplan, Ronna S., and Anita Louise Steele. 2005. An Analysis of Music Therapy Program Goals and Outcomes for Clients with Diagnoses on the Autism Spectrum. Journal of Music Therapy 42: 2–19. [Google Scholar] [CrossRef]
- Landry, Jayan Marie. 2014. Physiological and Psychological Effects of a Himalayan Singing Bowl in Meditation Practice: A Quantitative Analysis. American Journal of Health Promotion 28: 306–9. [Google Scholar] [CrossRef]
- Lavallee, Christina F., Stanley A. Koren, and Michael A. Persinger. 2011. A Quantitative Electroencephalographic Study of Meditation and Binaural Beat Entrainment. The Journal of Alternative and Complementary Medicine 17: 351–55. [Google Scholar] [CrossRef]
- Lucchetti, Giancarlo, Leonardo Garcia Góes, Stefani Garbulio Amaral, Gabriela Terzian Ganadjian, Isabelle Andrade, Paulo Othávio de Almeida, Victor Mendes do Carmo, and Maria Elisa Gonzalez Manso. 2020. Spirituality, religiosity and the mental health consequences of social isolation during COVID-19 pandemic. The International Journal of Social Psychiatry, 0020764020970996. [Google Scholar] [CrossRef] [PubMed]
- Luis, Merna, Ramy Doss, Basel Zayed, and Magdi Yacoub. 2019. Effect of live oud music on physiological and psychological parameters in patients undergoing cardiac surgery. Global Cardiology Science & Practice 2019: e201917. [Google Scholar] [CrossRef][Green Version]
- McEwen, Bruce S. 2017. Neurobiological and Systemic Effects of Chronic Stress. Chronic Stress 1: 2470547017692328. [Google Scholar] [CrossRef] [PubMed]
- Melchior, Maria, Avshalom Caspi, Barry J. Milne, Andrea Danese, Richie Poulton, and Terrie E. Moffitt. 2007. Work stress precipitates depression and anxiety in young, working women and men. Psychological Medicine 37: 1119–29. [Google Scholar] [CrossRef] [PubMed]
- Miles, Pamel, and Gala True. 2003. Reiki—Review of a Biofield Therapy History, Theory, Practice, and Research. Alter Ther Health Medicine 9: 62–72. [Google Scholar]
- Miller, Iona. 2012. The Whole Sum Infinity: Merging Spirituality and Integrative Biophysics. Journal of Consciousness Exploration & Research 3. Available online: https://jcer.com/index.php/jcj/article/view/208 (accessed on 1 November 2021).
- Norhazman, H., N. Mohamad Zaini, M. N. Taib, R. Jailani, and H. A. Omar. 2014. The investigation of alpha frontal energy asymmetry on normal and stress subjects after listening to the binaural beats 10 Hz. Paper presented at the 2014 IEEE 10th International Colloquium on Signal Processing and Its Applications, Kuala Lumpur, Malaysia, March 7–9; pp. 246–50. [Google Scholar] [CrossRef]
- Oxhandler, Holly K., Kenneth I. Pargament, Michelle J. Pearce, Cassandra Vieten, and Kelsey M. Moffatt. 2021. The Relevance of Religion and Spirituality to Mental Health: A National Survey of Current Clients’ Views. Social Work 66: 254–64. [Google Scholar] [CrossRef]
- Peterman, Amy H., George Fitchett, Marianne J. Brady, Lesbia Hernandez, and David Cella. 2002. Measuring spiritual well-being in people with cancer: The functional assessment of chronic illness therapy—spiritual well-being scale (FACIT-Sp). Annals of Behavioral Medicine 24: 49–58. [Google Scholar] [CrossRef]
- Piedmont, Ralph L. 2009. The Contribution of Religiousness and Spirituality to Subjective Wellbeing and Satisfaction with Life. In International Handbook of Education for Spirituality, Care and Wellbeing. Edited by Marian de Souza, Leslie J. Francis, James O’Higgins-Norman and Daniel Scott. Dordrecht: Springer, pp. 89–105. [Google Scholar] [CrossRef]
- Puccinelli, Paulo José, Taline Santos da Costa, Aldo Seffrin, Claudio Andre Barbosa de Lira, Rodrigo Luiz Vancini, Pantelis T. Nikolaidis, Beat Knechtle, Thomas Rosemann, Lee Hill, and Marilia Santos Andrade. 2021. Reduced level of physical activity during COVID-19 pandemic is associated with depression and anxiety levels: An internet-based survey. BMC Public Health 21: 425. [Google Scholar] [CrossRef]
- R Core Team. 2020. A Language and Environment for Statistical Computing. Available online: https://www.r-project.org (accessed on 1 November 2021).
- Rasic, Daniel, Steve Kisely, and Donald B. Langille. 2011. Protective associations of importance of religion and frequency of service attendance with depression risk, suicidal behaviours and substance use in adolescents in Nova Scotia, Canada. Journal of Affective Disorders 132: 389–95. [Google Scholar] [CrossRef]
- Reed, Rebecca G., and Charles L. Raison. 2016. Stress and the Immune System. In Environmental Influences on the Immune System. Edited by Charlotte Esser. Berlin: Springer, pp. 97–126. [Google Scholar] [CrossRef]
- Regehr, Cheryl, Dylan Glancy, and Annabel Pitts. 2013. Interventions to reduce stress in university students: A review and meta-analysis. Journal of Affective Disorders 148: 1–11. [Google Scholar] [CrossRef] [PubMed]
- Ronneberg, Corina R., Edward Alan Miller, Elizabeth Dugan, and Frank Porell. 2016. The Protective Effects of Religiosity on Depression: A 2-Year Prospective Study. The Gerontologist 56: 421–31. [Google Scholar] [CrossRef] [PubMed]
- Rubik, Beverly, David Muehsam, Richard Hammerschlag, and Shamini Jain. 2015. Biofield Science and Healing: History, Terminology, and Concepts. Global Advances in Health and Medicine 4 Suppl. 1: 8–14. [Google Scholar] [CrossRef] [PubMed]
- Saiz, Jesús, Xin Chen-Chen, and Paul J. Mills. 2021. Religiosity and Spirituality in the Stages of Recovery From Persistent Mental Disorders. The Journal of Nervous and Mental Disease 209: 106–13. [Google Scholar] [CrossRef] [PubMed]
- Shacham, Saya. 1983. A shortened version of the Profile of Mood States. Journal of Personality Assessment 47: 305–6. [Google Scholar] [CrossRef]
- Shifriss, Roni, Ehud Bodner, and Yuval Palgi. 2020. Don’t let me down: The effect of age and chosen music on mood is moderated by focus on emotions. The Journal of Positive Psychology 15: 254–66. [Google Scholar] [CrossRef]
- Shirani Bidabadi, Shahrzad, and Amirhooshang Mehryar. 2015. Music therapy as an adjunct to standard treatment for obsessive compulsive disorder and co-morbid anxiety and depression: A randomized clinical trial. Journal of Affective Disorders 184: 13–17. [Google Scholar] [CrossRef]
- Sigurdardóttir, Gudrun Agusta, Peter Michael Nielsen, Jesper Rønager, and August Gabriel Wang. 2019. A pilot study on high amplitude low frequency–music impulse stimulation as an add-on treatment for depression. Brain and Behavior 9: e01399. [Google Scholar] [CrossRef]
- Sinha, Rajita, and Ania M. Jastreboff. 2013. Stress as a Common Risk Factor for Obesity and Addiction. Biological Psychiatry 73: 827–35. [Google Scholar] [CrossRef]
- Snaith, R. Phillip. 2003. The Hospital Anxiety And Depression Scale. Health and Quality of Life Outcomes 1: 29. [Google Scholar] [CrossRef]
- Stanhope, Jessica, and Philip Weinstein. 2020. The human health effects of singing bowls: A systematic review. Complementary Therapies in Medicine 51: 102412. [Google Scholar] [CrossRef] [PubMed]
- Staufenbiel, Sabine M., Brenda W. J. H. Penninx, Anne T. Spijker, Bernet M. Elzinga, and Elisabeth F. C. van Rossum. 2013. Hair cortisol, stress exposure, and mental health in humans: A systematic review. Psychoneuroendocrinology 38: 1220–35. [Google Scholar] [CrossRef] [PubMed]
- Tang, Fang, Jing Liang, Hai Zhang, Mohammedhamid Mohammedosman Kelifa, Qiqiang He, and Peigang Wang. 2021. COVID-19 related depression and anxiety among quarantined respondents. Psychology & Health 36: 164–78. [Google Scholar] [CrossRef]
- Terwagne, Denis, and John W. M. Bush. 2011. Tibetan singing bowls. Nonlinearity 24: R51–R66. [Google Scholar] [CrossRef]
- Wahbeh, Helané, Carlo Calabrese, Heather Zwickey, and Dan Zajdel. 2007. Binaural Beat Technology in Humans: A Pilot Study to Assess Neuropsychologic, Physiologic, And Electroencephalographic Effects. The Journal of Alternative and Complementary Medicine 13: 199–206. [Google Scholar] [CrossRef] [PubMed]
- Wang, Jianli, and Scott B. Patten. 2001. Perceived work stress and major depression in the Canadian employed population, 20–49 years old—PsycNET. Journal of Occupational Health Psychology 64: 283–89. [Google Scholar] [CrossRef]
- Wepner, Florian, Julia Hahne, Angelika Teichmann, Gertraud Berka-Schmid, Annette Hördinger, and Martin Friedrich. 2008. Treatment with crystal singing bowls for chronic spinal pain and chronobiologic activities—A randomized controlled trial. Forschende Komplementarmedizin (2006) 15: 130–37. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Baseline | Post-Sound Healing | ||||||
|---|---|---|---|---|---|---|---|
| Measures | N | Mean | SD | Mean | SD | p-Value | η2 |
| Tension (POMS) | 62 | 1.26 | 1.03 | 0.14 | 0.57 | 0.000 | 0.51 |
| Anxiety (HADS) | 58 | 1.11 | 0.66 | 0.44 | 0.49 | 0.000 | 0.49 |
| Depression (HADS) | 57 | 0.62 | 0.51 | 0.42 | 0.36 | 0.002 | 0.16 |
| Faith (FACIT) | 62 | 3.18 | 1.10 | 3.46 | 0.96 | 0.005 | 0.12 |
| Spirituality (FACIT) | 57 | 2.85 | 0.94 | 3.64 | 0.46 | 0.000 | 0.49 |
| Fatigue Imp | Anger Imp | Confuse Imp | Vigor Imp | Faith Imp | Spiritual Imp | Tension Imp | Anxiety Imp | |
|---|---|---|---|---|---|---|---|---|
| Fatigue Imp | 1.00 | |||||||
| Anger Imp | 0.54 **** | 1.00 | ||||||
| Confuse Imp | 0.67 **** | 0.64 **** | 1.00 | |||||
| Vigor Imp | −0.32 * | −0.15 | −0.11 | 1.00 | ||||
| Faith Imp | 0.30 * | 0.48 **** | 0.32 * | −0.22 | 1.00 | |||
| Spiritual Imp | 0.56 **** | 0.57 **** | 0.56 **** | −0.40 ** | 0.48 **** | 1.00 | ||
| Tension Imp | 0.66 **** | 0.64 **** | 0.69 **** | −0.06 | 0.39 ** | 0.50 **** | 1.00 | |
| Anxiety Imp | 0.57 **** | 0.60 **** | 0.49 **** | −0.12 | 0.44 *** | 0.63 **** | 0.73 **** | 1.00 |
| Depression Imp | 0.66 **** | 0.44 *** | 0.42 *** | −0.45 *** | 0.33 ** | 0.67 **** | 0.43 *** | 0.48 **** |
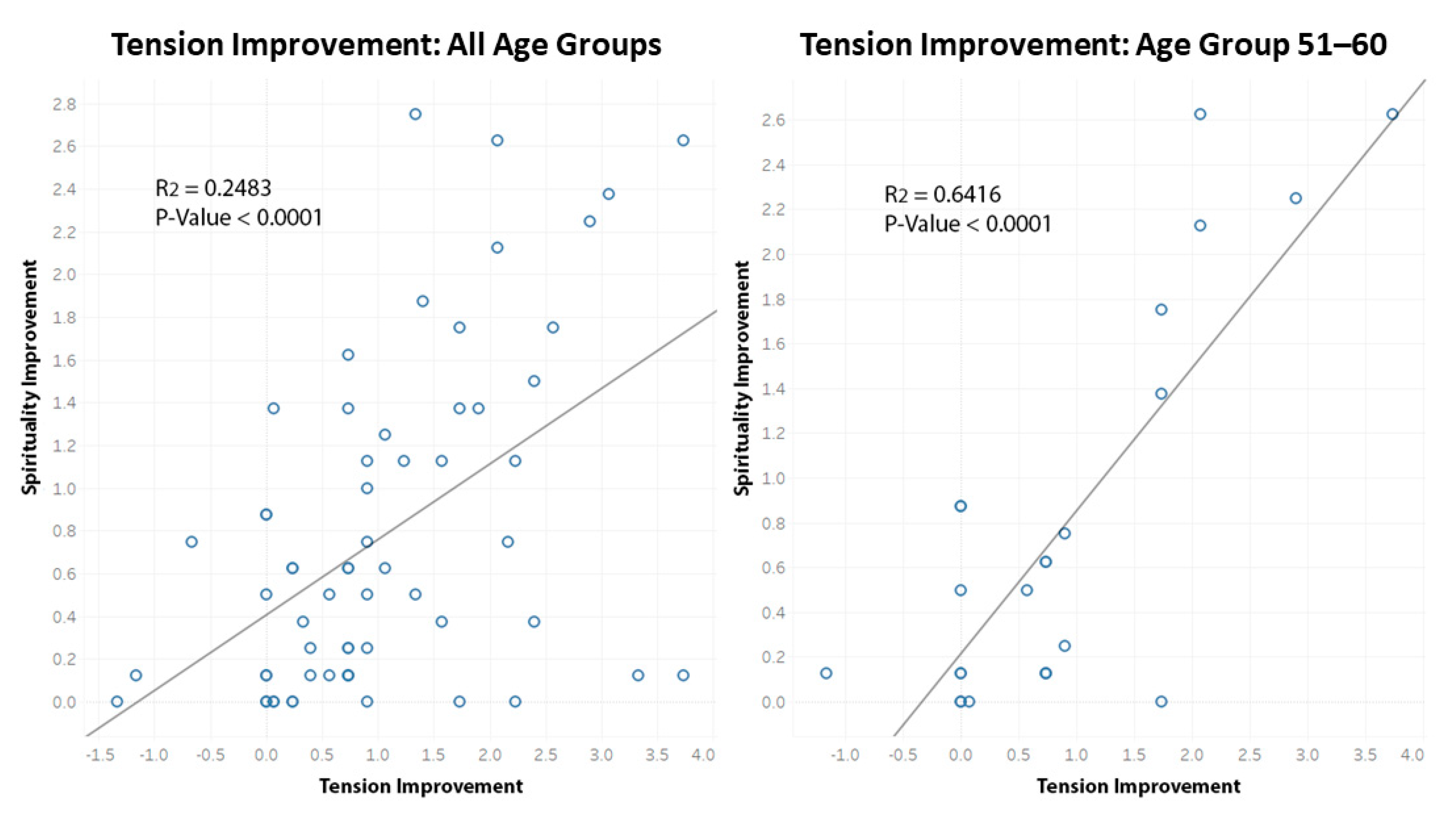
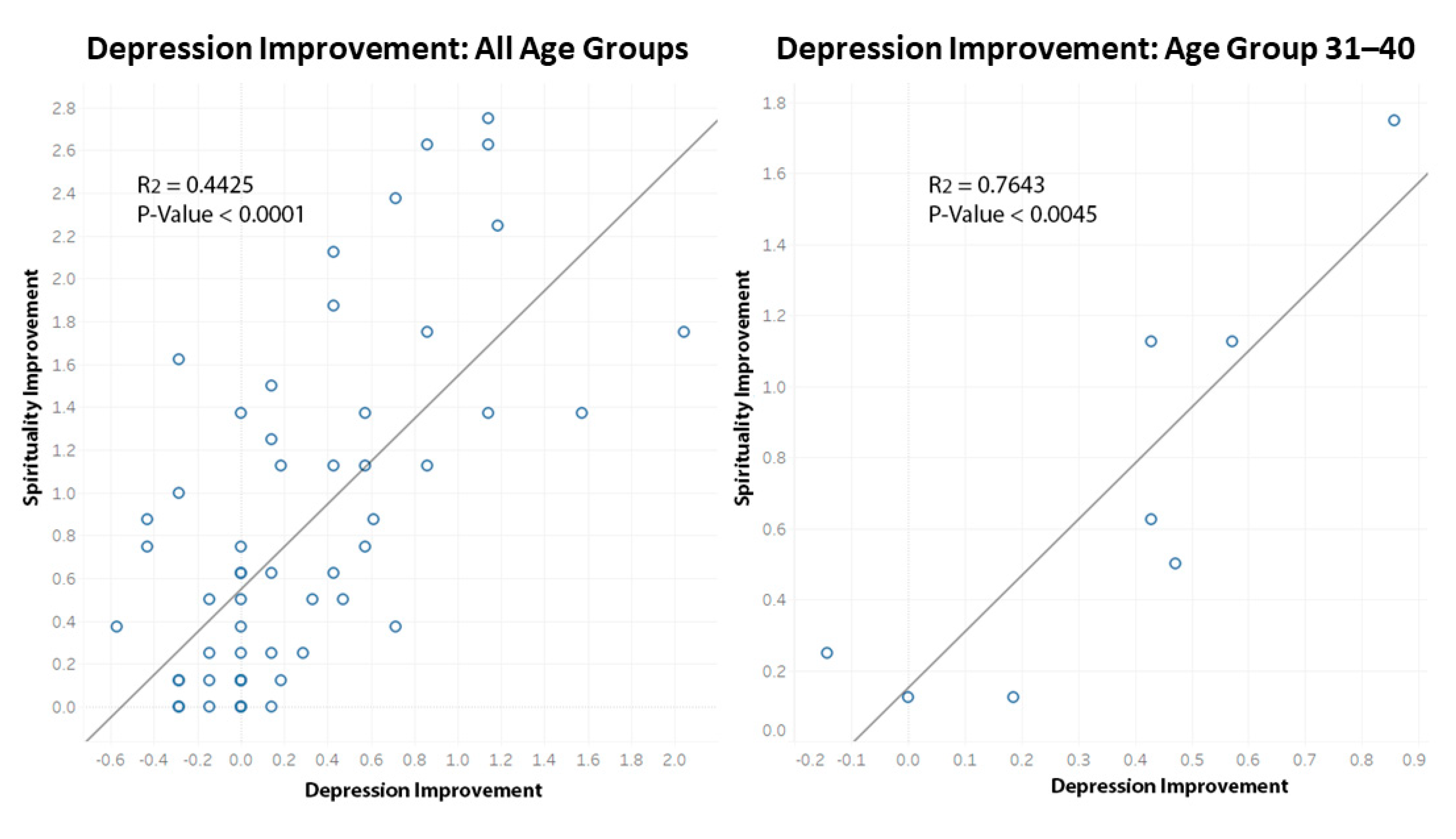
| Age Group | Tension Improvement Correlation | Depression Improvement Correlation |
|---|---|---|
| 20–30 | −0.06 | 0.80 * |
| 31–40 | 0.28 | 0.87 ** |
| 41–50 | 0.35 | 0.62 |
| 51–60 | 0.80 **** | 0.77 **** |
| 61-Plus | 0.36 | 0.46 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Goldsby, T.L.; Goldsby, M.E.; McWalters, M.; Mills, P.J. Sound Healing: Mood, Emotional, and Spiritual Well-Being Interrelationships. Religions 2022, 13, 123. https://doi.org/10.3390/rel13020123
Goldsby TL, Goldsby ME, McWalters M, Mills PJ. Sound Healing: Mood, Emotional, and Spiritual Well-Being Interrelationships. Religions. 2022; 13(2):123. https://doi.org/10.3390/rel13020123
Chicago/Turabian StyleGoldsby, Tamara L., Michael E. Goldsby, Mary McWalters, and Paul J. Mills. 2022. "Sound Healing: Mood, Emotional, and Spiritual Well-Being Interrelationships" Religions 13, no. 2: 123. https://doi.org/10.3390/rel13020123
APA StyleGoldsby, T. L., Goldsby, M. E., McWalters, M., & Mills, P. J. (2022). Sound Healing: Mood, Emotional, and Spiritual Well-Being Interrelationships. Religions, 13(2), 123. https://doi.org/10.3390/rel13020123