

‘Existential’ in Scandinavian Healthcare Journals: An Analysis of the Concept and Implications for Future Research

 ,
,  ,
,  , and
, and 
Abstract
1. Introduction
1.1. Evolution of the Concept of ‘Existential’ in Scandinavian Healthcare Research
1.2. The Aim
2. Materials and Methods
2.1. Search Strategy
2.2. Inclusion Criteria and Presentation of Data
2.3. Data Analysis
3. Results
3.1. Findings from Stage 1: Trajectory of the Concept of ‘Existential’
3.2. Findings from Stage 2: Keyword Analysis of Definitions of ‘Existential’
3.3. Findings from Stage 3: Thematic Analysis of the Articles’ Application of ‘Existential’
3.3.1. Suffering and Re-Orientation
3.3.2. Meaning and Meaninglessness
3.3.3. Existential Philosophy in Relation to Health
3.3.4. Existential Questions as Approaches to Care
3.3.5. Usage and Demarcation of Existential, Spiritual and Religious Concepts
3.3.6. Additional to the Overarching Themes
3.4. Integration and Significance of the Findings from the Three Analytical Stages
4. Discussion
4.1. Increasing Use of ‘Existential’
4.2. A Concept without Consensus
‘Spirituality is a dynamic and intrinsic aspect of humanity through which persons seek ultimate meaning, purpose, and transcendence, and experience relationship to self, family, others, community, society, nature, and the significant or sacred. Spirituality is expressed through beliefs, values, traditions, and practices.’
4.3. An Attempt to Define ‘Existential’ for the Healthcare Context
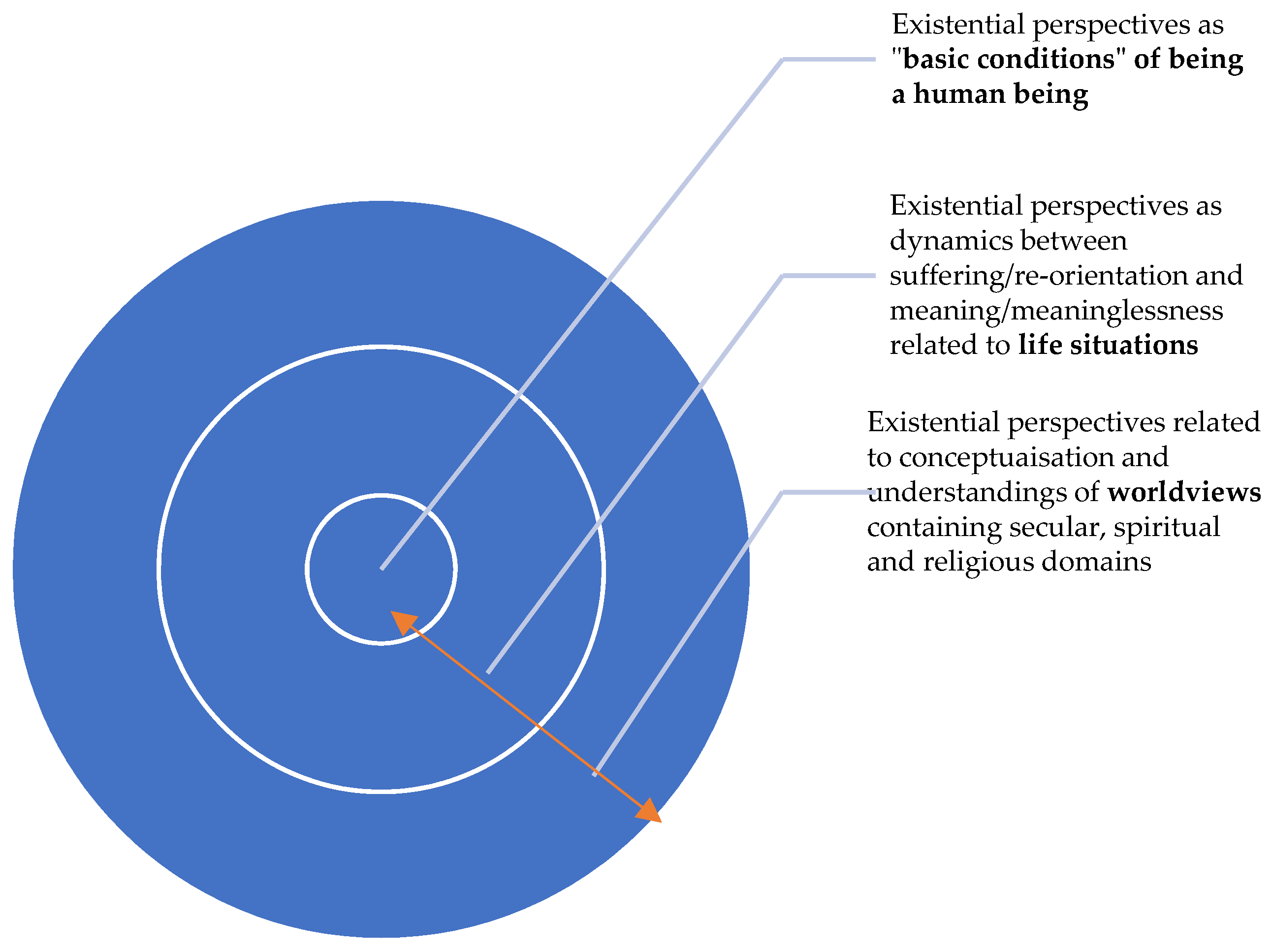
The term ‘existential’ related to health refers to the fundamental, basic condition of being a human. The existential is based on the irrefutable fact that we live and will die, facing conditions and uncertainties along the way beyond our control. The existential is expressed primarily through a quest for making and seeking meaning in life in general, as well as in demanding life situations. This may involve movements between suffering and re-orientation and meaning and meaninglessness. Existential concerns can be integrated into both religious, secular, and spiritual worldviews.
4.4. Limitations of the Concept Based on Our Findings
4.5. Strength and Limitations of the Study
5. Conclusions
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Author, Year, Country | Discipline and Language of the Articles | Research Design | Definition of Existential | Themes—Key Attributes | Some Exemplars | Overarching Categories | |
|---|---|---|---|---|---|---|---|
| 1. | (Gonzalez 1999) Norway | Nursing Norwegian | Literature review | No | Pair Meaning | Existential –threat, –struggling, –frustration, –alienated, –isolation Existential and spiritual as meaning related phenomena | Usage and demarcation of existential, spiritual, and religious concepts Meaning and meaninglessness |
| 2. | (Berg and Sarvimäki 2003) Norway, Sweden, Finland | Nursing, researchers in the field English | Theoretical, philosophical | No | Holistic being in the world | A holistic existential perspective focuses on individual’s ‘being in-theworld’ promote health | Existential philosophy in relation to health |
| 3. | (Bullington et al. 2003) Sweden | Dance Therapist, Clinicians in the field English | Empirical | No | Existential Pain Meaning | From chaos to meaning Existential, psychological/psychosomatic aspects of chronic pain, as seen from the clinicians’ perspective | Meaning and meaninglessness Suffering and reorientation |
| 4. | (Ladegaard Jensen 2004) Denmark | Nursing Danish | Professional article | No | Questions | Existential questions Existential unrest | Existential questions as approaches for care Suffering and reorientation |
| 5. | (Rehnsfeldt and Eriksson 2004) Sweden, Finland | Researchers in the field English | Empirical | No | Suffering Caring encounter Meaning | The human existence …experienced suffering can mean not to be able to hold oneself together as a whole ‘Existential caring | Existential philosophy in relation to health Suffering and reorientation Meaning and meaninglessness Existential questions as approaches for care Usage and demarcation of existential, spiritual, and religious concepts |
| encounter’…the encounter between patient and caregiver can create meaning in communion and thereby alleviate suffering by making it bearable. Existential movement of suffering that makes it possible to understand life in a more profound spiritual or ontological way and in this way experience alleviated suffering. | |||||||
| 6. | (Erdner et al. 2005) Sweden | Health professions English | Empirical | No | Social alienation | Experiencing existential and social alienation | Suffering and reorientation |
| 7. | (Lundmark 2005) Sweden | Chaplaincy and nursing Swedish | Empirical | No | Problems Freedom Meaning Isolation Death | Existential—patients’ challenges related freedom, meaning/meaninglessness, existential isolation, and death Spiritual care means making possible/facilitating for the patient, with help of suitable nursing interventions, to express and discuss existential questions and to practice his/her spirituality | Meaning and meaninglessness Suffering and reorientation Existential philosophy in relation to health Existential questions as approaches for care Usage and demarcation of existential, spiritual, and religious concepts |
| 8. | (Nyman and Sivonen 2005) | Nursing Swedish | Conceptual analysis | No | Meaning | Existential perspectives on the ultimate meaning is belief in the ultimate being | Meaning and meaninglessness Existential questions as approaches for care |
| 9. | (Rehnsfeldt and Arman 2005) Sweden | Healthcare professionals Swedish | Professional article | No | Questions | Existential questions Existential and spiritual Existential suffering | Existential questions as approaches for care Usage and demarcation of existential, spiritual, and religious concepts Suffering and reorientation |
| 10. | (Rydahl-Hansen 2005) Denmark | Nursing English | Empirical | No | Suffering | Existential and theological theories about human suffering | Suffering and reorientation |
| 11. | (Carlstedt 2006) Denmark | Nursing Danish | Professional article | No | Basic condition | Basic conditions Existential freedom | Existential philosophy in relation to health |
| 12. | (Dam et al. 2006) Denmark | Nursing Danish | Professional article | No | Dialogue | Existential/spiritual Existential dialogue | Usage and demarcation of existential, spiritual, and religious concepts Existential questions as approaches for care |
| 13. | (Frølund 2006) Denmark | Nursing Danish | Empirical | No | Spiritual existential Death Loss | Loss of existents because of imminent death. Terminally ill patient…focusing on the spiritual/existential dimension. | Usage and demarcation of existential, spiritual, and religious concepts Suffering and reorientation |
| 14. | (Hummelvoll 2006, p. 22) | Nursing Norwegian | Professional article | Yes | Existential suffering and holistic care | “Existential here means what concerns the human existence and life situation, ie problems and challenges that people encounter related to, e.g., freedom of will and responsibility of choice» “Eksistensiell betyr her det som angår menneskets eksistens og livssituasjon, dvs. problemer og utfordringer som mennesker møter knyttet til bl.a. viljens frihet og valgets ansvar» From a perspective of a holistic existential understanding of suffering in psychiatric nursing practice four overlapping aspects emerge: (1) suffering from illness, (2) existential suffering as lack of meaning with life and that the human being carries insight about being separated and lonely, (3) suffering in the relation between care provider and receiver, (4) social suffering as reduced possibilities for taking part in the society | Meaning and meaninglessness Suffering and reorientation |
| 15. | (Nilsson et al. 2006) Norway, Finland | Nursing English | Literature study Philosophical | No | Isolation | Existential isolation Yalom perceives as a ‘separation from the world’ | Suffering and reorientation Existential philosophy in relation to health |
| 16. | (Stolt 2006) Sweden | Medicine Swedish | Empirical | No | Suffering | Existential questions | Existential questions as approaches for care |
| 17. | (Östergaard Jensen 2006) Denmark | Nursing Danish | Empirical | No | Threat | Existential threat | Suffering and reorientation |
| 18. | (Mjaaland 2007) Norway | Philosophical Norwegian | Professional article | No | Basic condition of being human being | An existential possibility as a dialectic between freedom and no freedom as Kirkegaard regards as basic condition of the human being | Existential philosophy in relation to health |
| 19. | (Nyström 2007) Sweden | Nursing English | Philosophical | No | Human needs, emotions, visions, possibilities Interpersonal | Existential—as human needs, frustration, dreams, possibilities Existen tial philosophy converted to lifeworldhermeneutics by Heidegger/Gadamer | Existential philosophy in relation to health |
| 20. | (Ausker et al. 2008) Denmark | Health care workers, researchers | Empirical | No | Religious and existential Meaning | Religious and existential thoughts Existential questions and meaning | Usage and demarcation of existential, spiritual, and religious concepts Meaning and meaninglessness |
| 21. | (Barremo et al. 2008) Sweden | Nursing Health professions Swedish | Systematic literature review | No | Suffering | Existential questions as adjustments to new meaning Existential suffering | Meaning and meaninglessness Suffering and reorientation Existential questions as approaches for care |
| 22. | (Fleischer and Jessen 2008) Denmark | Healthcare workers Danish | Professional article | No | Aging Transfers in life | Existential questions related to be older Who am I? What is the meaning of life? Where am I going? Why is the disorder a part of my life? | Existential questions as approaches for care Meaning and meaninglessness |
| 23. | (Holmgaard Thygesen and Appel Esbensen 2008) Denmark | Nursing Danish | Empirical | No | Problems | Existential problems | Suffering and reorientation |
| 24. | (Meiers and Brauer 2008) | Nursing English | Theoretical—conceptualization | No | Philosophy | Existential philosophy is understood as the basic underlying lens guiding the nurse in taking an existential caring orientation as depicted in the resultant conceptualization | Existential philosophy as an understanding of health and illness Existential philosophy in relation to health |
| 25. | (Olesen 2008) Denmark | Physiotherapist Danish | Professional article | No | Philosophy | Existence philosophy Existential themes | Existential philosophy in relation to health |
| 26. | (Ribe 2008) Norway | Health professionals Norwegian | Professional article | No | Existential suffering | Existential crisis | Suffering and reorientation |
| 27. | (Schärfe and Rosenkvist 2008) Denmark | Nursing Danish | Professional article | No | Questions | Existential questions Existential and religious search | Existential questions as approaches for care Usage and demarcation of existential, spiritual, and religious concepts |
| 28. | (Stålhandske 2008) Sweden | Healthcare professions Swedish | Professional article | No | Existential experiences | Existential experiences in a secular context | Suffering and reorientation |
| 29. | (Berg 2009) Norway | Nursing English | Empirical | No | Being Meaning | Existential approach focuses on “the human-being in the world” and individuals’ understanding of their being and the meaning they give their life. | Existential philosophy in relation to health Meaning and meaninglessness |
| 30. | (Borge and Rolfsnes 2009) Norway | Health professions Chaplaincy Norwegian | Empirical | No | Spiritual and existential questions | The dialog with pastors’ space for spiritual and existential questions | Usage and demarcation of existential, spiritual, and religious concepts Existential questions as approaches for care |
| 31. | (Enderlein 2009) Denmark | Nursing Danish | Professional article | No | Questions | Existential questions Meaning Existential anxiety | Existential questions as approaches for care Meaning and meaninglessness Suffering and reorientation |
| 32. | (Gudmannsdottir and Halldorsdottir 2009) Iceland | Nursing home residents living with chronic pain English | Empirical | No | Pain | The authors explore chronic pain and argue that chronic pain must be seen as closely related existential pain and suffering. | Suffering and reorientation |
| 33. | (Helle-Valle and Binder 2009) Norway | Psychology English | A phenomenological analysis of a literary work in light of psychology | No | Playfulness, selfassertion, insecurity, curiosity and more | An exploration of existential and phenomenological themes in Alice in Wonderland analyzed in light of psychology | Humanistic psychology and theories of selfexperience |
| 34. | (Hammerlin 2010) Norway | Sociology, suicide prevention Norwegian | Scientific essay | No | Suffering | Existential suffering is complex and the result of societal and individual factors. | Suffering and reorientation |
| 35. | (Jonsen et al. 2010) Sweden | Nursing English | Empirical | No | Meaning Pair | Meaning of existence, death, choice and retirement Frankl’s existential theory | Meaning and meaninglessness |
| 36. | (Jystad and Bongaard 2010) Norway | Parents who have lost a child Norwegian | Empirical | No | Loss Questions Meaning | The loss of a child triggers existential questions and existential challenges. These are related to the loss/continuing bond with the child, the question of guilt, of embodied grief, relationship to others and finding meaning in grief. | Suffering and reorientation Meaning and meaninglessness Existential questions as approaches for care |
| 37. | (Arman et al. 2011, p. 300) Sweden | Nursing English | Empirical | No | Burnout Deficiency meaning | “Existential deficiencies” as part of the lived experience for people with burnout. Existential “blindness” and reflection that can be seen as avoiding one suffering. Burnout implies a “lack of conscious reflection on existential issues such as the meaning of life and existence” Katie Eriksson’s theory which sees health as an ontological condition where spiritual and existential/universal dimensions are crucial | Suffering and reorientation Meaning and meaninglessness Existential questions as approaches for care Usage and demarcation of existential, spiritual, and religious concepts |
| 38. | (Bjelland and Severinsson 2011) Norway | Nursing English | Literature review | No | Pair | “existential problems”, “existential questions”, “existential care”, etc | (Only pair) |
| 39. | (DeMarinis 2011) Sweden | Psychiatry and mental health Swedish | Theoretical with one empirical case | No | Meaning Existential information | Existential meaning is tied to religion and spirituality. ” Existential information” as part of cultural perspective is vital for understanding what is providing meaning t a person’s life. | Meaning and meaninglessness Usage and demarcation of existential, spiritual, and religious concepts Existential questions as approaches for care Existential philosophy in relation to health |
| 40. | (Poulsen 2011) Denmark | Nursing Danish | Professional article | No | Existential/religious | Usage and demarcation of existential, spiritual, and religious concepts | |
| 41. | (Bondevik 2012) Norway | Nursing Norwegian | Empirical | No | Questions | Dialogue about existential questions, Death | Existential questions as approaches for care |
| 42. | (Ekblad et al. 2012) Sweden | Mental health among seekers of asylum and refugees Swedish | Empirical | No | Meaning | Existential meaningfulness is essential for providing health for refugees | Meaning and meaninglessness |
| 43. | (Grelland 2012) Norway | Philosophy and psychology Norwegian | Theoretical | No | Anxiety in light of existential philosophy | Existential anxiety is understood in the theories of Kierkegaard, Heidegger and Sartre. | Existential philosophy in relation to health |
| 44. | (Rehnsfeldt and Arman 2012) Norway, Sweden | Health professions Researchers in the field English | Empirical | No | Pair | Existential health perspective existential and relational aspects Existential distress is to see a person as being in a ‘darkness of understanding of life’. struggling can therefore be understood as an existential health process (2). | Suffering and reorientation |
| 45. | (Wang et al. 2012) Norway | Psychotherapy Self-reflective film course for adolescence Norwegian | Professional article | No | Self-reflection | Existentialistic theory (Buber) used for selfreflection | Existential philosophy in relation to health |
| 46. | (Binder and Hjeltnes 2013) Norway | Researchers Health care professions Nursing Norwegian | Professional article | No | Present in joy and suffering Mindfulness | Basic condition | Existential philosophy in relation to health |
| 47. | (Lien Hansen et al. 2013) Denmark | Nursing Danish | Empirical | No | Death, isolation, meaningsless | Death, isolation and meaninglessness as existential conditions Yalom | Suffering and reorientation Meaning and meaninglessness |
| 48. | (Nielsen and Sørensen 2013) Denmark | Health professions Danish | Empirical | No | Struggle Meaning | Through one existential, inner struggle, a personal development is achieved Units of meaning as «Existential challenged» | Suffering and reorientation Meaning and meaninglessness |
| 49. | (Thorsen Gonzalez 2013) Norway | Health care professions and researchers Norwegian | Empirical | No | Depression Suffering meaning | Depression as a phenomenon has an existential dimension associated with deficiency on experience of meaning | Suffering and reorientation Meaning and meaninglessness |
| 50. | (Baklien and Bongaardt 2014) Norway | Health professionals Norwegian | Professional article | No | Anthropology | Phenomenological existential anthropology in psychiatry | Existential philosophy in relation to health |
| 51. | (Beck et al. 2014) Sweden | Nursing English | Empirical | No | Holistic | Palliative care is a holistic approach that integrates psychosocial and existential aspects in the care | Existential philosophy in relation to health |
| 52. | (Blegen et al. 2014) Norway | Mothers who are patients in psychiatric care Nursing English | Empirical | No | Pair In between Suffering and sources | Existential underpinning existential conditions existential assumptions existential meaning level The struggle between the darkness of suffering and their inner source of strength as mothers | Suffering and reorientation |
| 53. | (Brinkmann et al. 2014) Norway | Psychology Danish | Professional article | No | A critique of diagnostic culture with grief as example | Existential phenomenon as grief and depression. | Suffering and reorientation |
| 54. | (Dybvik et al. 2014) Norway | Nursing English | Empirical | No | Good life, meaning | Good life has a deeper meaning because it challenges the existential preconditions for life | Meaning and meaninglessness |
| 55. | (Ellingsen et al. 2014) Norway, Sweden | Nursing English | Empirical | No | Distress Loss existence, home safe | “Not knowing where to be in a time of change is like an existential cry of distress where the foothold in existence is lost.” | Suffering and reorientation |
| 56. | (Homme and Sæteren 2014) Norway | Nursing Norwegian | Empirical | No | Challenges Suffer Future | The patients suffer because of the existential challenges, such as concerns for the future and the progress of the disease, loss of life possibilities, guilt and shame and concerns about death. | Suffering and reorientation |
| 57. | (Kvaal et al. 2014) Norway | Nursing English | Empirical | No | Empty Boredom | Existential dimensions | Suffering and reorientation |
| 58. | (Slåttå and Madsen 2014) Norway | Psychology Norwegian | Professional article | No | Existential psychotherapy Nature | Yalom’s i existential psychotherapy and how four existential conditions for living | Existential philosophy in relation to health |
| 59. | (Biong et al. 2015) Norway | Medicine, psychiatrics Norwegian | Empirical | No | Thoughts Value | Existential thoughts—the value of ones’ own life | Existential questions as approaches for care |
| 60. | (Fridh et al. 2015) Sweden | Health professions Researchers in the field English | Empirical | No | Suffering Dialogues | Advanced and progressive illness brings existential suffering to patients as an inevitable consequence of the disease and its treatment. Limited time and a lack of undisturbed spaces have been shown to be obstacles to existential dialogues with patients Existential, phenomenological tradition as described by van Manen | Suffering and reorientation Existential questions as approaches for care |
| 61. | (Hammerlin 2015) Norway | Researchers in suicidology | Professional article | No | Suffering | Existential load and possibility | Suffering and reorientation |
| 62. | (Molnes 2015) Norway | Health professional, researchers Norwegian | Empirical | No | Meaning of problems | “Spiritual care for seriously ill patients can be understood as perceiving the patient’s existential problems, listening to the meaning of these problems in the patient’s life history” | Suffering and reorientation Meaning and meaninglessness Providing care |
| 63. | (Ozolins et al. 2015) Sweden | Health care workers, Nursing, researchers English | Empirical | No | View on human being Individuals’ own life force | Anthroposophical medicine and care take account of humanity and human existence as a whole. Existential nature, as an omnipresent human vulnerability. | Existential philosophy in relation to health |
| 64. | (Sjursen et al. 2015) Norway | Nursing Norwegian | Empirical | No | Crisis | Existential crisis of the patient, the courage to make the patient face his or her own ability to cope and find strength to carry on and finally | Suffering and reorientation |
| 65. | (Solvoll 2016) Norway | Nursing Norwegian | Professional article | No | Dilemma | Relatives may experience the situation strongly existential, being stuck in dilemmas, thus making them less responsive to the actions of the nurses. | Suffering and reorientation Existential questions as approaches for care |
| 66. | (Sörbye and Brunborg 2015) Norway | Nursing Norwegian | Empirical | No | Spiritual existential | In Norwegian literature it is common to use the word spiritual/existential | 1,demarcation of existential, spiritual, and religious concepts |
| 67. | (DeMarinis 2016) Sweden | Mental health workers English | Professional article | No | Meaning | Rituals and existential meaning making processes in a cultural context | Meaning and meaninglessness |
| 68. | (Lid et al. 2016) Norway | Nursing Norwegian | Empirical | No | Community Pair Source | Existential community The existential in the patient Existential in the togetherness Existential and touching in life Existential nursing | (Only pair) |
| 69. | (Rehnsfeldt and Arman 2016) Norway, Sweden | Nursing Health care workers and researchers English | Empirical | No | Pair | “existential strain”, “existential challenges”, “existential wounds”, Existential processes are natural, contains paradoxes (e.g., Life- death, meaning, meaninglessness) ‘existential life issues’ refers to the existential questioning of life values, priorities, people’s relationships with each other and the importance of health, suffering, love and death | Meaning and meaninglessness Existential questions as approaches for care |
| 70. | (Rykkje 2016) Norway | Nursing Norwegian | Literature study | No | Spirituality and existential meaning question | In old age, spirituality and existential issues may become salient Existential and spiritual questions The meaning of life and the existential in the form of the circle of life | Usage and demarcation of existential, spiritual, and religious concepts Meaning and meaninglessness Existential questions as approaches for care |
| 71. | (Hemberg 2017) Finland | Health care workers and researchers English | Empirical | No | Pain | Existential pain | Suffering and reorientation |
| 72. | (Rehnsfeldt et al. 2017) Norway/Sweden/Finland | Nursing Health care workers and researchers English | Theoretical | No | Health is at stake | Being a patient is mostly an existential condition where health or even life is at stake, and the patient suffers as a result | Suffering and reorientation |
| 73. | (Andermo et al. 2018) Sweden | Researchers Health care workers English | Empirical | Basis in life | Existential suffering and health means to pay attention to …experiences of significant meaning in their life. The term existential refers to our basis in life | Suffering and reorientation Existential philosophy in relation to health | |
| 74. | (Berland et al. 2018) Norway | Nursing Norwegian | Empirical | No | Loss Transition | The existential impact on age related loss | Suffering and reorientation |
| 75. | (Hemberg et al. 2018) Finland | Nursing English | Empirical | No | Suffering loneliness | Existential loneliness (34) can arise if an individual cannot find ways to deal with loneliness or find peace by listening to his/her inner voice. | Suffering and reorientation |
| 76. | (Hvidt et al. 2018, p. 272) Denmark | Health care workers and researchers Danish | Scientific debate article | Partly, see rubric for exemplars | Existential Spiritual | The National Board of Health therefore also translates spiritual care in not one but two words: existential and spiritual (care), precisely because spiritual as term both contain an existential dimension of meaning and orientation as well as human life’s own inner dynamics, it inner life The existential …a broad category… A factor analysis indicated four understandings of the existential: 1. Essential meaning of life, 2. Spirituality, 3. Existential thinking, oriented about philosophical traditions, and 4. Crisis management. («det eksistentielle …en meget bred kategori…Faktoranalysen indikerede her fire forståelser af det eksistentielle: 1. Essentiel livsmening, 2. Spiritualitet, 3. Eksistentiel tænkning, orienteret om filosofiske traditioner, samt 4. Krisehåndtering») People find meaning in primarily three existential domains of meaning: Secular (not spiritual nor religious, for instance the significance of family or the work), spiritual (the inner spiritual life, for instance meditation, experienced connectedness with nature or the univers), and religious (understood as beliefs one shares and practices with others, typically on the basis of holy scriptures such as the Bible) » («… mennesker finder mening i tre primære eksistentielle meningsdomæner: sekulære (hverken spirituelle eller religiøse, fx familiens eller arbejdets betydning), spirituelle/åndelige (det indre åndelige liv, fx meditation, oplevet forbindelse med natur eller univers) og religiøse (forstået som overbevisninger, man deler og praktiserer med andre, typisk på basis af hellige skrifter som Bibelen).») | Meaning and meaninglessness Usage and demarcation of existential, spiritual, and religious concepts Existential questions as approaches for care Existential philosophy in relation to health |
| 77. | (Jakobsen and Hvidt 2018) Denmark | Health care workers, researchers | Empirical | No | Existential and spiritual care are defined by Stifoss Hansen and Kallenberg as “to pay attention to the patient’s existential and spiritual questions and resources. To listen to the opinion they have in the patient’s life history, and to assist the patient in his/her work with existential questions based on his/her own view of life | Existential questions as approaches for care Meaning and meaninglessness Usage and demarcation of existential, spiritual, and religious concepts | |
| 78. | (Jensen and Hvidt 2018) Denmark | Nursing | Professional article | No | Pair | Existential view of life Existential issues | (Only pair) |
| 79. | (Lisander Larsen et al. 2018) Denmark | Nursing/health care English | Empirical | No | Loss | The existential experience of being in the diagnostic phase of SLE | Suffering and reorientation |
| 80. | (Paque et al. 2018) Belgium | Health care workers and researchers English | Empirical | No | Loneliness | Existential loneliness is defined as ‘a universal human characteristic, inborn in all persons and not related to object loss or lack of intimate relationships | Suffering and reorientation |
| 81. | (Prause and Sørlie 2018) Norway | Nursing Norwegian | Empirical | No | Nature Creativity Connectedness | Existential needs are seen as opportunities to (1) experience nature, (2) express oneself creatively, (3) feeling connectedness | Exception of the overarching categories |
| 82. | (Thorsen 2018) Norway | Nursing Norwegian | Scientific essay | No | Human condition Philosophy | Existential concern is part of the human condition. Based on the philosophy of Løgstrup, the focus is on the loving concern which forms the basis for care. | Existential philosophy in relation to health |
| 83. | (Toivonen et al. 2018) Finland | Health care workers and researchers English | Empirical | No | Spirituality Existential Meaning | Spirituality is defined as a search for answers to existential questions about the meaning of life and the individual’s relationship with the sacred or transcendent | Usage and demarcation of existential, spiritual, and religious concepts Meaning and meaninglessness |
| 84. | (Ueland et al. 2018) Norway, Finland | Health workers, researchers English | Empirical | No | Pair | existential longing, also existential worlds, existential loneliness etc. | (Only pair) |
| 85. | (Breistig and Huser 2019) Norway | Health workers, researchers Norwegian | Empirical | No | Pair Suffering | What alleviates existential pain Existential pain, existential questions, existential suffering | Suffering and reorientation |
| 86. | (Bremer et al. 2019) Sweden | Health care workers and researchers English | Empirical | No | Pair | Existential wholeness, uncertainty, insecurity, thoughts, consequences, transition, distress, coping, aspects | (Only pair) |
| 87. | (Delmar 2019) Denmark | Health workers, researchers Danish | Empirical | No | Life phenomenon Loneliness | Life-promoting existential life phenomena: Courage, hope, joy, longing, longing, loneliness. Life-limiting existential life phenomena: Loneliness, loneliness, homelessness, hopelessness, despair, anxiety, powerlessness, vulnerability, longing. | Existential philosophy in relation to health |
| 88. | (Gabre et al. 2019) Sweden | Nursing English | Empirical | No | Struggles | Existential struggles in self-care | Suffering and reorientation |
| 89. | (Gregersen et al. 2019) Denmark | Nursing English | Empirical, literature review | No | Pair | When deciding to opt for participation on clinical trials “existential matters” or “existential issues” are important. | (Only pair) |
| 90. | (Lundvall et al. 2019) Sweden | Healthcare workers English | Empirical | Partly, see rubric for exemplars | Health | Existential concerns can cause stress, doubts and worries. According to Sigurdsson, existential health should not be defined as a separate dimension of health; instead, it encompasses all aspects of health and is related to human beings’ ability to reflect on their health and well-being | Suffering and reorientation Existential philosophy in relation to health |
| 91. | (Maehre 2019) Norway | Health care workers Norwegian | Empirical | No | Suffering Pair | The patient’s existence and life history Existence threatened Existential conditions Existential despair and pain | Suffering and reorientation |
| 92. | (Midlöv and Lindberg 2019) Sweden | Nursing English | Empirical | No | Existential needs | Good palliative care means considering both physical, mental, social, and existential needs. | Usage and demarcation of existential, spiritual, and religious concepts |
| 93. | (Andersson et al. 2020) Sweden | Nursing English | Empirical | No | Meaning | Existential meaning of illness Existential loneliness | Suffering and re-orientation Meaning and meaninglessness |
| 94. | (Angel 2020) Denmark | Nursing English | Theoretical | No | Existential core in vulnerability | The existential core in vulnerability can be explained by Heidegger’s theory of living authentically based on Being and potentiality for Being | Existential philosophy in relation to health |
| 95. | (Drageset et al. 2020) Norway | Health care professions English | Empirical | No | Existential fear | Existential awareness and fear | Suffering and reorientation |
| 96. | (Edvardsen et al. 2020) Norway | Nursing English | Empirical | No | Issues | Palliative treatment may alter the symptoms and that complex mental, social and existential issues also can aggregate symptoms | Suffering and reorientation |
| 97. | (Furnes et al. 2020) Norway | Nursing Norwegian | Empirical | No | Experiences | Existential experiences of living with obesity | Suffering and reorientation |
| 98. | (Haga et al. 2020) Norway | Healthcare English | Empirical | No | Existential experiences | Existential experiences when dealing with obesity. …Lifeworld theory can help to describe the existential world in which all humans live. Lifeworld is the world of lived experiences, the world in which we live our daily lives. Existential view of being human | Existential philosophy in relation to health |
| 99. | (Holmberg et al. 2020) Sweden | Nursing English | Empirical | No | Holistic perspective | Holistic perspective comprising both physical and an existential dimension. Existential/spiritual suffering | Suffering and reorientation Usage and demarcation of existential, spiritual, and religious concepts |
| 100. | (Jakobsson et al. 2020) Sweden | Healthcare English | Empirical | No | Existential thoughts | Existential thoughts and sleep disturbance Existential thoughts were not about school but more about life, relationships, days that had come and gone, and the future | Meaning and meaninglessness Suffering and reorientation |
| 101. | (Jakobsen and Nørgaard 2020) Denmark | Nursing Danish | Professional article | No | Question | Existential questions | Existential questions as approaches for care |
| 102. | (Nagel Delica 2020) Denmark | Professionals, social innovation, and health | Professional article | No | Creativity | Existential (Self-expression, creativity) | Exception |
| 103. | (Netsey-Afedo et al. 2020) Denmark | Health professionals English | Empirical | No | Existential issues | Almost no health professional show interest in patients’ feelings or existential issues. Hence, patients had unmet needs and dissatisfaction | Suffering and reorientation |
| 104. | (Prause et al. 2020, p. 281) Norway | Nursing English | Empirical | Partly, see rubric for exemplars | Existential care | “Giske and Cone (2019) point out that existential concerns can be expressed through the psychosocial and physical level. However, they also describe existential care as an own dimension characterized by “touching the innermost of a human being” (2019, p. 20) in times of seeking and pain. Pargament (2013) relates the existential dimension explicitly to an experience of a sacred quality through interconnecting and caring.” | Exception of the overarching categories |
| 105. | (Slang et al. 2020) Norway | Nursing English | Scoping review | No | Existential and spiritual | Beyond physical effects…symptoms exert significant psychological, social, existential, and spiritual impact on the patients’ experience | Usage and demarcation of existential, spiritual, and religious concepts |
| 106. | (Stranden et al. 2020) Noway | Medicine Norwegian | Article in professional journal | No | Safety | Morbidly obese related to lack of existential safety in childhood | Suffering and reorientation |
| 107. | (Sundal and Lykkeslet 2020) Norway | Healthcare Professionals English | Empirical | No | Being in the world Existentials | Heidegger expanded the concept of being-in-theworld through basic structures or “existentials” | Existential philosophy in relation to health |
| 108. | (Viftrup et al. 2020, p. 162) Denmark | Health care workers, researchers Danish | Empirical | Partly, see rubric for exemplars | Language Meanings domains Secularity, Spirituality Religiosity | Existential language we define as words, concepts and understandings within three existential domains of meaning: the secular (life relationship, that are meaningful and significant to the individual, but which are not religious, e.g., values, meaning of family or work), the spiritual (the inner spiritual life experienced as transcendent for the individual) and/or the religious (beliefs and understandings, which one shares and practices with others, e.g., bible reading and church attendance) (“Eksistentiel sprogbrug definerer vi som ord, begreber og forståelser inden for tre eksistentielle meningsdomæner: det sekulære (livsforhold, der er menings- og betydningsfulde for individet, men som ikke er religiøse, f.eks. værdier, familiens eller arbejdets betydning), det åndelige (det indre åndelige liv, der opleves som transcendent for den enkelte) og/eller det religiøse (overbevisninger og forståelser, som man deler og praktiserer med andre, f.eks. bibellæsning og kirkegang)») | Meaning and meaninglessness Usage and demarcation of existential, spiritual, and religious concepts |
| 1 | ‘Existential’ was found paired with other words in articles 1, 35, 38, 44, 52, 68, 69, 78, 84, 85, 86, 89, 91. |
| 2 | See European Association for Palliative Care (https://www.eapcnet.eu/eapc-groups/reference/spiritual-care/) (accessed on 1 May 2022), and the Enhancing Nurses’ and Midwives’ Competence in Providing Spiritual Care through Innovative Education and Compassionate Care (EPICC) Spiritual Care Education Standard (https://blogs.staffs.ac.uk/epicc/files/2020/08/EPICC-Spiritual-Care-Education-Standard.pdf) (accessed on 1 May 2022). |
References
- Afdal, Geir. 2010. Researching Religious Education as Social Practice. Münster: Waxmann. [Google Scholar]
- Andermo, Susanne, Tobias Sundberg, Torkel Falkenberg, Johanna Hök Nordberg, and Maria Arman. 2018. Measuring patients’ health and suffering—The first stages of instrument development. Scandinavian Journal of Caring Sciences 32: 1322–31. [Google Scholar] [CrossRef] [PubMed]
- Andersson, Niklas, Margaretha Ekebergh, and Ulrica Hörberg. 2020. Patient experiences of being cared for by nursing students in a psychiatric education unit. Nordic Journal of Nursing Research 40: 142–50. [Google Scholar] [CrossRef]
- Angel, Sanne. 2020. Mutual vulnerability of patients and nurses contextualised by a broader understanding of the phenomenon. Nordisk Sygeplejeforskning 10: 139–44. [Google Scholar] [CrossRef]
- Arman, Maria, Anne-Sofie Hammarqvist, and Arne Rehnsfeldt. 2011. Burnout as an existential deficiency—Lived experiences of burnout sufferers. Scandinavian Journal of Caring Sciences 25: 294–302. [Google Scholar] [CrossRef]
- Asbring, Pia, and Madeleine Jeanneau. 2006. Group reflections about existential questions have a positive effect on empowerment and mental health. [Reflektion i grupp kring existentiella frågor främjar egenmakt och psykisk hälsa]. Läkartidningen 103: 2743–46. Available online: http://www.lakartidningen.se/07engine.php?articleId=4894 (accessed on 1 March 2021).
- Ausker, Nadja Hørdam, Peter La Cour, Christian Busch, Henning Nabe-Nielsen, and Lotte Mörk Pedersen. 2008. Danske patienter intensiverer eksistentielle tanker og religiöst liv [Danish patatients intensify existential thoughts and religious life]. Ugeskrift for Laeger 170: 1828–33. Available online: http://ugeskriftet.dk/videnskab/danske-patienter-intensiverer-eksistentielle-tanker-og-religioest-liv (accessed on 4 April 2021).
- Austad, Anne, Hans Stifoss-Hanssen, Lisbet Borge, and Linda Rykkje. 2020. Innledning: Det eksistensielle. In Eksistensielle begreper i helse- og sosialfaglig praksis [Existential Concepts in Health- and Social Work Practices]. Edited by Linda Rykkje and Anne Austad. Oslo: Universitetsforlaget. [Google Scholar]
- Baklien, Børge, and Rob Bongaardt. 2014. Jan Hendrik van den Berg (1914–2012)—The changing nature of man. [Jan Hendrik van den Berg (1914–2012)—Menneskets foranderlige essens]. Tidsskrift for Psykisk Helsearbeid 11: 339–47. Available online: http://www.idunn.no/tph/2014/04/j_h_van_den_berg_1914-2012__menneskets_foranderlige_es (accessed on 5 May 2021). [CrossRef]
- Barremo, Ann-Sofi, Elisabeth Bruce, Monica Salander, and Karin Sundin. 2008. Personal experiences of living with congestive heart failure—A systematic literature review. [Personers upplevelse av att leva med kronisk hjärtsvikt—Systematisk litteraturstudie]. Vård i Norden 28: 34–38. [Google Scholar] [CrossRef]
- Beck, Ingela, Ulf Jakobsson, and Anna-Karin Edberg. 2014. Applying a palliative care approach in residential care: Effects on nurse assistants’ experiences of care provision and caring climate. Scandinavian Journal of Caring Sciences 28: 830–41. [Google Scholar] [CrossRef]
- Berg, Geir V. 2009. Promoting elderly hospital patients’ health with a holistic–Existential approach. Norsk tidsskrift for sykepleieforskning 11: 3–15. [Google Scholar]
- Berg, Geir V., and Anneli Sarvimäki. 2003. A holistic-existential approach to health promotion. Scandinavian Journal of Caring Science 17: 384–91. [Google Scholar] [CrossRef] [PubMed]
- Berland, Astrid, Astrid Solheim, and Anne Lise Holm. 2018. Elderly patients who wish to die. [Eldre pasienter som önsker å dö]. Nordisk Sygeplejeforskning 8: 63–74. [Google Scholar] [CrossRef]
- Binder, Per-Einar. 2022. Suffering a healthy life—On the existential dimension of health. Frontiers in Psychology 13: 803792. [Google Scholar] [CrossRef]
- Binder, Per-Einar, and Aslak Hjeltnes. 2013. To be present in joy and suffering—Mindfulness and therapeutic work with emotions. [Tilstede i glede og smerte—Mindfulness og arbeid med emosjoner i psykoterapi]. Tidsskrift for Norsk Psykologforening 50: 814–21. Available online: http://www.psykologtidsskriftet.no/index.php?seks_id=329971&a=2 (accessed on 5 May 2021).
- Biong, Stian, Eli Jorid Sveipe, and Edle Ravndal. 2015. “Everything aches and everything is stuck”: About relative’s experiences with overdose deaths. [“Alt verker og alt har satt seg fast”: Om pårörendes erfaringer med overdosedödsfall]. Tidsskrift for Psykisk Helsearbeid 12: 278–87. Available online: https://www.idunn.no/tph/2015/04/alt_verker_og_alt_har_satt_seg_fast_om_paaroerendes_erfar (accessed on 4 April 2021). [CrossRef]
- Bischofberger, E. 2000. The neglected inside of human beings. Lack of competence among personnel when it comes to patients’ need for existential and spiritual talks. [Människans eftersatta insida. Personalen saknar kompetens för att svara mot patienternas behov av existentiella och andliga samtal]. Läkartidningen 97: 6054–56. [Google Scholar] [PubMed]
- Bjelland, Stine Dyste, and Elisabeth Severinsson. 2011. Experiences of existential problems and psychiatric nurses ways of addressing them. Nordisk Sygeplejeforskning 1: 111–27. Available online: http://www.idunn.no/ts/nsf/2011/02/art04 (accessed on 3 April 2021). [CrossRef]
- Björklund, L., and B. Eriksson. 1997. Hope and powerlessness. Meeting existential questions connected with a child’s disease and death. [Hoppet och vanmakten. Att möta existentiella frågor i samband med barns sjukdom och död]. Socialmedicinsk Tidskrift 74: 240–41. [Google Scholar]
- Blegen, Nina Elisabeth, Katie Eriksson, and Terese Bondas. 2014. Through the depths and heights of darkness; mothers as patients in psychiatric care. Scandinavian Journal of Caring Sciences 28: 852–60. [Google Scholar] [CrossRef]
- Bondevik, M. 2012. Quality of life among Norwegian centenarians. [Livskvalitet hos norske hundreåringer]. Geriatrisk Sykepleie 4: 16–24. Available online: http://sykepleien.no/sites/sykepleien.no/files/electronic-issues/articles/livskvalitet_blant_hundrearinger_9572.pdf (accessed on 5 April 2021).
- Borge, Lisbet, and John Kristian Rolfsnes. 2009. Patients’ experiences with pastoral care in a psychiatric clinic. [Pasienters erfaring med sjelesorg i en psykiatrisk klinikk]. Sykepleien Forskning 4: 142–49. [Google Scholar] [CrossRef]
- Braun, Virginia, Victoria Clarke, and Debra Gray. 2017. Collecting Qualitative Data: A Practical Guide to Textual, Media and Virtual Techniques. West Nyack: Cambridge University Press. [Google Scholar]
- Breistig, Sigrund, and Benny Huser. 2019. Healthcare personnel as a source of comfort in recurrent ovarian cancer. [Helsepersonell som kjelde til tröyst ved tilbakevendande eggstokkreft]. Sykepleien Forskning 14: 1–16. [Google Scholar] [CrossRef]
- Bremer, Anders, Tova Dahné, Lovisa Stureson, Kristofer Årestedt, and Ingela Thylén. 2019. Lived experiences of surviving in-hospital cardiac arrest. Scandinavian Journal of Caring Sciences 33: 156–64. [Google Scholar] [CrossRef] [PubMed]
- Brenne, Anne-Tove, Arve Nordbø, Siri Steine, Anne Fasting, Maren Anne Berglund, Endre Røynstrand, and Nina E. Hjorth. 2020. Palliativ behandling av pasienter med COVID-19. [Palliative care of patients with COVID-19]. Tidsskrift for Den Norske Laegeforening 140: 1–4. [Google Scholar] [CrossRef]
- Brinkmann, Svend, Anders Petersen, Ester Holte Kofod, and Rasmus Birk. 2014. Diagnostic Culture—An analytical perspective on psychiatric diagnoses in contemporary society. [Diagnosekultur—Et analytisk perspektiv på psykiatriske diagnoser i samtiden]. Tidsskrift for Norsk Psykologforening 51: 629–27. Available online: http://www.psykologtidsskriftet.no/index.php?seks_id=427403&a=3 (accessed on 5 May 2021).
- Bullington, Jennifer, Rolf Nordemar, Kristina Nordemar, and Charlotte Sjöström-Flanagan. 2003. Meaning out of chaos: A way to understand chronic pain. Scandinavian Journal of Caring Sciences 17: 325–31. [Google Scholar] [CrossRef] [PubMed]
- Carlstedt, Else. 2006. Counselling in cancer prevention. [Rådgivning i kraeftens bekaempelse]. Klinisk Sygepleje 20: 29–35. Available online: http://www.idunn.no/klinisk_sygepleje/2006/01/raadgivning_i_kraeftens_bekaempelse (accessed on 6 May 2021). [CrossRef]
- Clarke, Virginia, and Victoria Braun. 2022. Thematic Analysis: A Practical Guide. Los Angeles: SAGE. [Google Scholar]
- Cullberg, J. 1996. Depression is an existential phenomenon, too (letter). [Depressionen är också ett existentiellt fenomen]. Läkartidningen 93: 4244–45. [Google Scholar]
- Dahn, I. 1984. Patients with existential pain are a challenge for physicians and society. [Patienter med existentiell smärta en utmaning för läkare och samhälle.]. Läkartidningen 81: 2041–43. [Google Scholar]
- Dam, Ettie, Lars Johansen, Beate Herup Jørgensen, and Olga Winck. 2006. Spiritual care should play a greater role in nursing. [Åndelig omsorg bör have mere plads i sygeplejen]. Sygeplejersken 106: 54–57. Available online: http://www.dsr.dk/Sygeplejersken/Sider/SY-2006-05-56-1-Aandelig_omsorg.aspx (accessed on 6 April 2021).
- Damásio, Bruno Figueiredo, Sílvia Helena Koller, and Tatjana Schnell. 2013. Sources of meaning and meaning in life questionnaire (SoMe): Psychometric properties and sociodemographic findings in a large Brazilian sample. Acta de Investigación Psicológica 3: 1205–27. [Google Scholar] [CrossRef]
- Delmar, Charlotte. 2019. The impact of close relations on life courage. [Naere relationers indvirkning på livsmodet]. Nordisk Tidsskrift for Helseforskning 15: 1–14. [Google Scholar] [CrossRef]
- DeMarinis, Valerie. 2003. Pastoral Care, Existential Health and Existential Epidemiology: A Swedish Postmodern Case Study. Stockholm: Verbum. [Google Scholar]
- DeMarinis, Valerie. 2006. Existential dysfunction as a public mental health issue for post-modern Sweden: A cultural challenge and a challenge to culture. In Tro på Teateret [Faith at the Theatre]. Copenhagen: Copenhagen University, p. 229. [Google Scholar]
- DeMarinis, Valerie. 2008. The impact of postmodernization on existential health in Sweden: Psychology of religion’s function in existential public health analysis. Archive for the Psychology of Religion 30: 57–74. [Google Scholar] [CrossRef]
- DeMarinis, Valerie. 2011. The interplay between philosophy, theory and clinical practice in cultural conscious psychiatry. [Samspelet mellan filosofi, teori och klinisk praktik i kulturellt medveten psykiatri]. Socialmedicinsk Tidskrift 88: 512–23. Available online: http://www.socialmedicinsktidskrift.se/index.php/smt/article/view/839/658 (accessed on 5 May 2021).
- DeMarinis, Valerie. 2016. Interactions among rituals, palliative care, and ethnicity/culture from a public mental health perspective. Omsorg 33: 47–51. [Google Scholar]
- Dhollande, Shannon, Annabel Taylor, Silke Meyer, and Mark Scott. 2021. Conducting integrative reviews: A guide for novice nursing researchers. Journal of Research in Nursing 26: 427–38. [Google Scholar] [CrossRef]
- Drageset, Sigrunn, Torill Christine Lindstrøm, and Sidsel Ellingsen. 2020. “Cancer changed my life”—Women’s experiences 1 and 9 years after primary breast cancer surgery. Nordisk Sygepleieforskning 10: 20–33. [Google Scholar] [CrossRef]
- Dybvik, Tove Katrin, Eva Gjengedal, and Else Lykkeslet. 2014. At the mercy of others—For better or worse. Scandinavian Journal of Caring Sciences 28: 537–43. [Google Scholar] [CrossRef]
- Edvardsen, Trine Lise, Geir F. Lorem, and Grete Mehus. 2020. Palliative care in rural and remote areas. Nordisk Sygeplejeforskning 10: 150–63. [Google Scholar] [CrossRef]
- Ekblad, Solvig, Julia Lindgren, Maria Asplund, and Bo Burström. 2012. Existential insecurity increases vulnerability to mental illness—Analysis of health interviews among adult asylum seekers and qualitative interviews with refugees. [Existentiell osäkerhet ökar sårbarheten för psykisk ohälsa—Analys av hälsosamtal bland vuxna asylsökande och kvalitativa intervjuer med flyktingar]. Socialmedicinsk Tidskrift 89: 150–60. Available online: http://www.socialmedicinsktidskrift.se/index.php/smt/article/view/842/694 (accessed on 5 May 2021).
- Ellingsen, Sidsel, Åsa Roxberg, Kjell Kristoffersen, Jan Henrik Rosland, and Herdis Alvsvåg. 2014. Being in transit and in transition. The experience of time at the place, when living with severe incurable disease—A phenomenological study. Scandinavian Journal of Caring Sciences 28: 458–68. [Google Scholar] [CrossRef] [PubMed]
- Enderlein, Anne-Marie. 2009. Aesthetics as an insight possibility. [Aestetik som insigtsmulighed]. Klinisk Sygepleje 23: 32–40. Available online: http://www.idunn.no/klinisk_sygepleje/2009/03/aestetik_som_indsigtsmulighed (accessed on 4 April 2021). [CrossRef]
- Erdner, Anette, Annabella Magnusson, Maria Nyström, and Kim Lützen. 2005. Social and existential alienation experienced by people with long-term mental illness. Scandinavian Journal of Caring Sciences 19: 373–80. [Google Scholar] [CrossRef]
- Fleischer, Elene, and Gert Jessen. 2008. Existential talks with elderly people: Difficult conversation and tough topics. [Eksistentielle samtaler med äldre mennesker: Vanskelige samtaler og tunge emner]. Suicidologi 13: 16–19. Available online: https://www.journals.uio.no/index.php/suicidologi/article/view/1944 (accessed on 3 February 2021).
- Fridh, Isabell, Elisabeth Kenne Sarenmalm, Kristin Falk, Ingela Henoch, Joakim Öhlén, Anneli Ozanne, and Eva Jakobsson Ung. 2015. Extensive human suffering: A point prevalence survey of patients’ most distressing concerns during inpatient care. Scandinavian Journal of Caring Sciences 29: 444–53. [Google Scholar] [CrossRef] [PubMed]
- Frøkedal, Hilde. 2020. Existential Groups Led by Healthcare Chaplains within Norwegian Specialist Mental Health Services. Patient and Interdisciplinary Perspectives. Oslo: VID Specialized University. [Google Scholar]
- Frøkedal, Hilde, Torgeir Sørensen, Torleif Ruud, Valerie DeMarinis, and Hans Stifoss-Hanssen. 2019. Addressing the existential dimension in treatment settings: Mental health professionals’ and healthcare chaplains’ attitudes, practices, understanding and perceptions of value. Archive for the Psychology of Religion 41: 253–76. [Google Scholar] [CrossRef]
- Frølund, Jannie Christina. 2006. Existential care—A neglected subject! [Åndelig omsorg -et forsömt område!]. Klinisk Sygepleje 20: 38–47. Available online: http://www.idunn.no/klinisk_sygepleje/2006/03/aandelig_omsorg_et_forsoemt_omraade (accessed on 2 July 2021).
- Furnes, Bodil, Elin Dysvik, and Venke Ueland. 2020. Å lide når en lever med overvekt og fedme: En utfordring i omsorg og behandling. [Suffering when living with overweight and obesity: A challenge in care and treatment]. Nordisk Sygeplejeforskning 10: 201–12. [Google Scholar] [CrossRef]
- Gabre, Marita, Birgitta Wireklint Sundström, and S. Olausson. 2019. “A little good with the bad”: Newly diagnosed type 2 diabetes patients’ perspectives on self-care: A phenomenological approach. Nordic Journal of Nursing Research 39: 20–28. [Google Scholar] [CrossRef]
- Getz, Linn. 2020. Dannelse i koronaens tid. [Formation in the time of the corona]. Tidsskrift for Den Norske Laegeforening. [Google Scholar] [CrossRef]
- Giske, Tove, and Pamela Cone. 2019. Å ta vare på heile mennesket: Handbok i åndeleg omsorg [Taking Care of the Whole Human Being: A Handbook of Spiritual Care]. Oslo: Samlaget. [Google Scholar]
- Gonzalez, Marianne Thorsen. 1999. Phenomena related to meaning and purpose in life—Core issues in nursing: Theoretical frameworks and perspectives. [Mening og meningsrelaterte fenomener—Sentrale tema i sykepleie: Teoretiske referanserammer og perspektiver]. Vård i Norden 19: 40–45. [Google Scholar] [CrossRef]
- Gregersen, Trine A., Regner Birkelund, Maiken Wolderslund, Mette Løwe Netsey-Afedo, Karina Dahl Steffensen, and Jette Ammentorp. 2019. What matters in clinical trial decisionmaking: A systematic review of interviews exploring cancer patients’ experiences. Scandinavian Journal of Caring Sciences 33: 266–78. [Google Scholar] [CrossRef] [PubMed]
- Grelland, Hans Herlof. 2012. Philosophy of anxiety (angst). [Filosofer om angst]. Tidsskrift for Psykisk Helsearbeid 9: 100–9. Available online: http://www.idunn.no/ts/tph/2012/02/filosofer_om_angst (accessed on 8 April 2021). [CrossRef]
- Gudmannsdottir, Gudrun Dora, and Sigridur Halldorsdottir. 2009. Primacy of existential pain and suffering in residents in chronic pain in nursing homes: A phenomenological study. Scandinavian Journal of Caring Sciences 23: 317–27. [Google Scholar] [CrossRef] [PubMed]
- Haga, Britt Marit, Bodil Furnes, Elin Dysvik, and Venke Ueland. 2020. Putting life on hold: Lived experiences of people with obesity. Scandinavian Journal of Caring Sciences 34: 514–23. [Google Scholar] [CrossRef]
- Hammerlin, Yngve. 2010. Society and everyday life suffering and the suicide problem. Attempts to a critical reflection. [Samfunnets og hverdagslivets lidelsesproduksjon og selvmordsproblematikken. Ansatser til en kritisk refleksjon]. Suicidologi 15: 30–36. Available online: https://www.journals.uio.no/index.php/suicidologi/article/view/2028 (accessed on 4 August 2020).
- Hammerlin, Yngve. 2015. Å bryte livet i fengsel. [To break life in prison]. Suicidologi 15: 20–29. [Google Scholar] [CrossRef]
- Harder, Ingegerd, Bente Martinsen, Elisabeth Hall, and Anita Haahr. 2012. Menneskelige grundtræk i sygeplejen [Basic human traits in nursing]. Klinisk Sygepleje 32: 15–26. [Google Scholar]
- Hartvig, P. 1984. Existential pain—Somatizing disorders—Folk-disease in disguise. [Eksistentiell smerte—Somatoforme tilstander—Folkesykdom i forkledninger]. Läkartidningen 81: 3797. [Google Scholar]
- Haug, Sigrid Helene Kjørven, Valerie DeMarinis, Lars Johan Danbolt, and Kari Kvigne. 2016. The illness reframing process in an ethnic-majority population of older people with incurable cancer: Variations of cultural- and existential meaning-making adjustments. Mental Health, Religion & Culture 19: 150–63. [Google Scholar] [CrossRef]
- Hedberg, C. 1992. Body and existence. [Kropp og existens]. Tidsskrift for Den Norske Laegeforening 112: 923–25. [Google Scholar] [PubMed]
- Heidegger, Martin. 1957. Zein und Zeit [Being and Time]. Tübingen: Max Niemeyer Verlag. [Google Scholar]
- Helle-Valle, Anna, and Per-Einar Binder. 2009. In Wonderland: A phenomenological, developmental and self psychological analysis of a child’s playful encounter with a new reality. Nordic Psychology 61: 16–28. [Google Scholar] [CrossRef]
- Hemberg, Jessica. 2017. The dark corner of the heart—Understanding and embracing suffering as portrayed by adults. Scandinavian Journal of Caring Sciences 31: 995–1002. [Google Scholar] [CrossRef] [PubMed]
- Hemberg, Jessica, Fredrica Nyqvist, and Marina Näsman. 2018. ‘Homeless in life’—Loneliness experienced as existential suffering by older adults living at home: A caring science perspective. Scandinavian Journal of Caring Science 33: 446–56. [Google Scholar] [CrossRef] [PubMed]
- Henriksen, Jan-Olav, and Arne Johan Vetlesen. 1997. Nærhet og Distanse: Grunnlag, Verdier og etiske teorier i arbeid med mennesker. [Proximity and Distance: Basis, Values and Ethical Theories in Working with People]. Oslo: Ad notam Gyldendal. [Google Scholar]
- Henriksen, Jan-Olav, and Arne Johan Vetlesen. 2006. Nærhet og distanse: Grunnlag, verdier og etiske teorier i arbeid med mennesker, 3rd ed. Oslo: Gyldendal akademisk. [Google Scholar]
- Holm, J. 2003. Meaning (letter). [Mening]. Tidsskrift for Den Norske Laegeforening 123: 2332. Available online: http://www.tidsskriftet.no/pls/lts/pa_lt.visSeksjon?vp_SEKS_ID=872497 (accessed on 4 August 2020). [PubMed]
- Holmberg, Mats, Staffan Hammarbäck, and Henrik Andersson. 2020. Registered nurses’ experiences of assessing patients with mental illness in emergency care: A qualitative descriptive study. Nordic Journal of Nursing Research 40: 151–61. [Google Scholar] [CrossRef]
- Holmgaard Thygesen, Kristina Holmegaard, and Bente Appel Esbensen. 2008. Disease-related problems in everyday life of patients with lung cancer—Part I. [Sygdomsrelaterede probleer i hverdagen hos patienter med lungekraeft—Del I]. Klinisk Sygepleje 22: 33–43. Available online: http://www.idunn.no/klinisk_sygepleje/2008/01/sygdomsrelaterede_problemer_i_hverdagen_hos_patienter_med_l (accessed on 8 April 2021). [CrossRef]
- Homme, Jorunn, and Berit Sæteren. 2014. Living with cystic fibrosis—A lonely, lifelong work. [Å leve med cystisk fibrose—Et ensomt, livslangt arbeid]. Nordisk Sygeplejeforskning 4: 15–27. Available online: http://www.idunn.no/ts/nsf/2014/01/aa_leve_med_cystisk_fibrose_et_ensomt_livslangt_arbeid (accessed on 7 May 2021). [CrossRef]
- Hummelvoll, Jan Kåre. 2006. A holistic-existential approach to psychiatric nursing from the perspective of a local community. [En helhetlig-eksistensiell psykiatrisk sykepleietilnaerming i et lokalsamfunnsperspektiv]. Klinisk Sygepleje 20: 13–23. Available online: http://www.idunn.no/klinisk_sygepleje/2006/01/en_helhetlig-eksistensiell_psykiatrisk_sykepleietilnaerming_ (accessed on 7 May 2021). [CrossRef]
- Hvidt, Niels Christian, Jette Ammentorp, Jane Clemensen, Vibeke Østergaard Steenfeldt, Lene Moestrup, and Jens Söndergaard. 2018. Existential and spiritual care in Denmark:. Why, what, how and who? [Eksistentiel og åndelig omsorg i Danmark: Hvorfor, hvad, hvordan og hvem?]. Klinisk Sygepleje 32: 265–80. [Google Scholar] [CrossRef]
- Hvidt, Niels Christian, Elisabeth Assing Hvidt, and Peter la Cour. 2021. Meanings of ‘the existential’ in a secular country: A survey study. Journal of Religion and Health 61: 3276–301. [Google Scholar] [CrossRef] [PubMed]
- Jacobsson, L. 2001. Is the ‘inside of human beings’ the responsibility of health care services? [Är ‘människans insida’ sjukvårdens ansvar?]. Läkartidningen 98: 2851–54. [Google Scholar] [PubMed]
- Jakobsen, Randi Kjelde, and Trine Tønners Nørgaard. 2020. Hvilke talenter har primærsektor brug for til fremtidens sygepleje? [Which talents does the primary sector need for the nursing of the future?]. Klinisk Sygepleje 34: 133–49. [Google Scholar] [CrossRef]
- Jakobsen, Louise Vissing, and Niels Christian Hvidt. 2018. Eksistentiel og åndelig omsorg i akutmodtagelsen. [Existential and spiritual care in the emergency department.]. Klinisk Sygepleje 32: 229–42. [Google Scholar] [CrossRef]
- Jakobsson, Malin, Karin Josefsson, and Karin Högberg. 2020. Reasons for sleeping difficulties as perceived by adolescents: A content analysis. Scandinavian Journal of Caring Sciences 34: 464–73. [Google Scholar] [CrossRef] [PubMed]
- Jebb, Andrew T., Scott Parrigon, and Sang Eun Woo. 2017. Exploratory data analysis as a foundation of inductive research. Human Resource Management Review 27: 265–76. [Google Scholar] [CrossRef]
- Jensen, Ellen Refsgaard, and Elisabeth Assing Hvidt. 2018. Hvordan bliver tro forstået og inddraget af sygeplejersker på et hospice?: En hermeneutisk-fænomenologisk undersøgelse. [How is faith understood and incorporated by nurses in a hospice?: A hermeneutic-phenomenological study.]. Klinisk Sygepleje 32: 281–93. [Google Scholar] [CrossRef]
- Johansson, F. 1984. Existential pain—Neurological aspects. [Existentiell smärta—Neurologiska synpunkter]. Läkartidningen 81: 3112–13. [Google Scholar]
- Jonsen, Elisabeth, Lisbeth Fagerström, Berit Lundman, Björn Nygren, Magdalena Vähäkangas, and Gunilla Strandberg. 2010. Psychometric properties of the Swedish version of the Purpose in Life scale. Scandinavian Journal of Caring Sciences 24: 41–48. [Google Scholar] [CrossRef]
- Jystad, Marte A., and Rob Bongaard. 2010. Living with a child who is not longer alive. A phenomenologic descriptive study. [Om a leve med et barn som ikke lenger er i live. En fenomenologisk deskriptiv studie]. Nordisk Tidsskrift for Helseforskning 6: 14–25. Available online: http://www.ub.uit.no/baser/septentrio/index.php/helseforsk/article/view/806/772 (accessed on 4 March 2021). [CrossRef]
- Kvaal, Kari, Anne-Grethe Halding, and Kari Kvigne. 2014. Social provision and loneliness among older people suffering from chronic physical illness. A mixed-methods approach. Scandinavian Journal of Caring Sciences 28: 104–11. [Google Scholar] [CrossRef] [PubMed]
- la Cour, Peter, and Niels C. Hvidt. 2010. Research on meaning-making and health in secular society: Secular, spiritual and religious existential orientations. Social Science & Medicine 71: 1292–99. [Google Scholar] [CrossRef]
- Ladegaard Jensen, Karin. 2004. Children, death and grief. [Börn, döden og sorg]. Klinisk Sygepleje 18: 50–58. Available online: http://www.idunn.no/klinisk_sygepleje/2004/01/boern_doeden_og_sorg (accessed on 5 May 2021).
- Lid, Else Marie, Kari Kvigne, and Per Kristian Roghell. 2016. Following the patient into his/her world. Thoughts about a nursing narration. [Å gå med i pasienten si livsverd. Tankar omkring ei sjukepleieforteljing]. Nordisk Tidsskrift for Helseforskning 12: 93–105. [Google Scholar] [CrossRef]
- Lien Hansen, Maria, Anette Wendelboe Christiansen, and Nanna Kappel. 2013. “This concerns my heart only”—Existential considerations in patients with atrial fibrillation. [“Det er mit hjerte, det drejer sig om”—Eksistentielle overvejelser hos patienter med atrieflimren]. Klinisk Sygepleje 27: 50–60. Available online: http://www.idunn.no/klinisk_sygepleje/2013/02/det_er_mit_hjerte_det_drejer_sig_om_eksistentielle_ove (accessed on 7 May 2021). [CrossRef]
- Lisander Larsen, Janni, Elisabeth O. C. Hall, Søren Jacobsen, and Regner Birkelund. 2018. Being in a standstill-of-life: Women’s experience of being diagnosed with systemic lupus erythematosus: A hermeneutic-phenomenological study. Scandinavian Journal of Caring Sciences 32: 654–62. [Google Scholar] [CrossRef] [PubMed]
- Lloyd, Christina Sophia, Britt af Klinteberg, and Valerie DeMarinis. 2017. An assessment of existential worldview function among young women at risk for depression and anxiety—A multi-method study. Archive for the Psychology of Religion 39: 165–203. [Google Scholar] [CrossRef]
- Lundmark, Mikael. 2005. Spiritual care—Definition of the concept and difficulties providing it according to Swedish nursing staff. [Andlig omvårdnad—Definition av begreppet och svårigheter med att ge sådan enligt svensk vårdpersonal]. Vård i Norden 25: 30–36. [Google Scholar] [CrossRef]
- Lundvall, Maria, Elisabeth Lindberg, Ulrica Hörberg, Lina Palmér, and Gunilla Carlsson. 2019. Healthcare professionals’ lived experiences of conversations with young adults expressing existential concerns. Scandinavian Journal of Caring Sciences 33: 136–43. [Google Scholar] [CrossRef]
- Lyons, J. 1977. Semantics: Vol. 1. Cambridge: Cambridge University Press. [Google Scholar]
- Maehre, Kjersti Sunde. 2019. The importance of the story to promote hope and life courage in the face of serious illness. [Fortellingens betydning for å fremme livsmotet i möte med alvorlig sykdom]. Nordisk Tidsskrift for Helseforskning 15: 1–16. [Google Scholar] [CrossRef]
- Maslow, Abraham Harold. 1943. A theory of human motivation. Psychological Review 50: 370–96. [Google Scholar] [CrossRef]
- McSherry, Wilfred, and Linda Ross. 2017. Spiritual care should be part of the Code. Nursing Standard 31: 29. [Google Scholar] [CrossRef] [PubMed]
- Meiers, Sonja J., and Donna J. Brauer. 2008. Existential caring in the family health experience: A proposed conceptualization. Scandinavian Journal of Caring Science 22: 110–17. [Google Scholar] [CrossRef] [PubMed]
- Midlöv, Elina Mikaelsson, and Terese Lindberg. 2019. District nurses’ experiences of providing palliative care in the home: An interview study. Nordic Journal of Nursing Research 40: 15–24. [Google Scholar] [CrossRef]
- Mjaaland, Marius Timmann. 2007. In the hands of death: Sören Kierkegaard about suicide, freedom and despair. [I dödens hule selv: Sören Kierkegaard om selvmord, frihet og fortvilelse]. Suicidologi 12: 3–7. Available online: https://www.journals.uio.no/index.php/suicidologi/article/view/1782 (accessed on 8 May 2021).
- Molnes, Sven Inge. 2015. Helping patients facing death. [Sammen går vi döden i möte]. Nordisk Tidsskrift for Helseforskning 11: 141–52. [Google Scholar] [CrossRef]
- Myers, Bryant L. 2011. Walking with the Poor: Principles and Practices of Transformational Development. Maryknoll: Orbis Books. [Google Scholar]
- Nagel Delica, Kristian. 2020. Linking Critical Social Innovation and Health Promotion—Reflections on a Project working with Young Marginalzed Mothers in the Outskirts of Denmark. Socialmedicinsk Tidskrift 97: 478–87. [Google Scholar]
- Netsey-Afedo, Mette Margrethe Løwe, Jette Ammentorp, Palle Jørn Sloth Osther, and Regner Birkelund. 2020. No time for reflection: Patient experiences with treatment-related decisionmaking in advanced prostate cancer. Scandinavian Journal of Caring Sciences 34: 880–88. [Google Scholar] [CrossRef]
- Nielsen, Rita, and Erik Elgaard Sørensen. 2013. The dying human being as the master of life. [Det döende menneske som livets laeremester]. Nordisk Sygeplejeforskning 3: 117–29. Available online: http://www.idunn.no/ts/nsf/2013/02/det_doeende_menneske_somlivets_laeremester (accessed on 7 May 2021). [CrossRef]
- Nilsson, Brita, Unni Å. Lindström, and Dagfinn Nåden. 2006. Is loneliness a psychological dysfunction? A literary study of the phenomenon of loneliness. Scandinavian Journal of Caring Sciences 20: 93–101. [Google Scholar] [CrossRef]
- Niu, Yanping, Wilfred McSherry, and Martin Partridge. 2021. Spirituality and spiritual care among ethnic chinese residing in england: Implications for nursing. Religions 12: 887. [Google Scholar] [CrossRef]
- NOU Norges offentlige utreninger [Official Norwegian Reports]. 2018. Available online: https://www.regjeringen.no/no/dokumenter/nou-2018-16/id2622153/ (accessed on 1 May 2022).
- Nyman, Ann-Charlotte, and Kerstin Sivonen. 2005. The concept of meaning of life in caring sciences. [Livsmening som vårdvetenskapligt begrepp]. Vård i Norden 25: 20–24. [Google Scholar] [CrossRef]
- Nyström, Maria. 2007. A patient-oriented perspective in existential issues: A theoretical argument for applying Peplau’s interpersonal relation model in healthcare science and practice. Scandinavian Journal of Caring Sciences 21: 282–88. [Google Scholar] [CrossRef]
- Olesen, Jens. 2008. Hope is the reward for those who dare to believe in the future. [Håbet er belönningen til den der vover at tro på fremtiden]. Fysioterapeuten 75: 18–23. Available online: http://www.fysioterapeuten.no/xp/pub/mx/filer/0108_Fagartikkel.pdf (accessed on 9 May 2021).
- Östergaard Jensen, Birte. 2006. Illness experiences of patients after first episode myocardial infarction—Secondary publication. [Sygdomsoplevelser hos patienter efter et förstegangs myokardieinfarkt—Sekundaer publikation]. Tidsskrift for Sygeplejeforskning 22: 15–23. [Google Scholar]
- Ozolins, Lise-Lotte, Ulrica Hörberg, and Karin Dahlberg. 2015. Caring touch—Patients’ experiences in an anthroposophic clinical context. Scandinavian Journal of Caring Sciences 29: 834–42. [Google Scholar] [CrossRef] [PubMed]
- Page, Matthew J., Joanne E. McKenzie, Patrick M. Bossuyt, Isabelle Boutron, Tammy C. Hoffmann, Cynthia D. Mulrow, and Larissa Shamseer. 2021. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 372: n71. [Google Scholar] [CrossRef]
- Paque, Kristel, Hilde Bastiaens, Peter Van Bogaert, and Tinne Dilles. 2018. Living in a nursing home: A phenomenological study exploring residents’ loneliness and other feelings. Scandinavian Journal of Caring Sciences 32: 1477–84. [Google Scholar] [CrossRef]
- Pargament, Kenneth I. 2013. Conversations with Eeyore: Spirituality and the generation of hope among mental health providers. Bulletin of the Menninger Clinic 77: 395–412. [Google Scholar] [CrossRef]
- Poulsen, Lena. 2011. Nursing and the terminal patient in pain. [Sygepleje til den döende patient med smerter]. Sygeplejersken 111: 56–60. Available online: http://www.dsr.dk/Sygeplejersken/Sider/SY-2011-2-56-1-Fag.aspx (accessed on 9 May 2021).
- Prause, Daniel, and Venke Sørlie. 2018. Taking care of the existential needs: Quality care for people with deafblindness. [Å ta vare på de eksistensielle behov: God omsorg for personer med dövblindhet]. Nordisk Sygeplejeforskning 8: 150–62. [Google Scholar] [CrossRef]
- Prause, Daniel, Venke Sørlie, Lars Johan Danbolt, and Kirsten Anne Tornøe. 2020. Sensing loneliness—Nurses’ experiences with providing existential care to older patients with acquired deafblindness. Nordisk Sygeplejeforskning 10: 280–91. [Google Scholar] [CrossRef]
- Puchalski, Christina M., Robert Vitillo, Sharon K. Hull, and Nancy Reller. 2014. Improving the Spiritual Dimension of Whole Person Care: Reaching National and International Consensus. Journal of Palliative Medicine 17: 642–56. [Google Scholar] [CrossRef] [PubMed]
- Rehnsfeldt, Arne, and Maria Arman. 2005. Ethics of understanding of life and bearing witness—Aspects of caring ethics. [Livsförståelseetik och vittnesbörd—Vårdetiska aspekter]. Vård i Norden 25: 19–23. [Google Scholar] [CrossRef]
- Rehnsfeldt, Arne, and Maria Arman. 2012. Significance of close relationships after the tsunami disaster in connection with existential health—A qualitative interpretive study. Scandinavian Journal of Caring Sciences 26: 537–44. [Google Scholar] [CrossRef]
- Rehnsfeldt, Arne, and Maria Arman. 2016. Dressing an existential wound (DEW)—A new model for long-term care following disasters. Scandinavian Journal of Caring Sciences 30: 518–25. [Google Scholar] [CrossRef]
- Rehnsfeldt, Arne, and Katie Eriksson. 2004. The progression of suffering implies alleviated suffering. Scandinavian Journal of Caring Sciences 18: 264–72. [Google Scholar] [CrossRef]
- Rehnsfeldt, Arne, Maria Arman, and Unni Å. Lindström. 2017. Clinical caring science as a scientific discipline. Scandinavian Journal of Caring Sciences 31: 641–46. [Google Scholar] [CrossRef]
- Ribe, Kristin. 2008. About self mutilation and healing: Dare to believe in your own capacity. [Om kutting og bedring: Å våge å tro på egne krefter]. Suicidologi 13: 26–27. Available online: https://www.journals.uio.no/index.php/suicidologi/article/view/1970 (accessed on 9 May 2021).
- Rydahl-Hansen, Susan. 2005. Hospitalized patients experienced suffering in life with incurable cancer. Scandinavian Journal of Caring Sciences 19: 213–22. [Google Scholar] [CrossRef]
- Rykkje, Linda. 2016. Understanding spirituality and spiritual care for older people—A hermeneutical study. [Forståelse av åndelighet og åndelig omsorg for gamle mennesker—En hermeneutisk studie]. Nordisk Tidsskrift for Helseforskning 12: 49–63. [Google Scholar] [CrossRef]
- Schärfe, Grete, and Solveig Rosenkvist. 2008. Be prepared for spiritual care. [Bliv parat til åndelig omsorg]. Sygeplejersken 108: 44–49. Available online: http://www.dsr.dk/Sygeplejersken/Sider/SY-2008-05-44-1-aandelig_omsorg.aspx (accessed on 5 May 2021).
- Schnell, Tatjana. 2010. Existential indifference: Another quality of meaning in life. Journal of Humanistic Psychology 50: 351–73. [Google Scholar] [CrossRef]
- Seale, Clive, and Jonathan Charteris-Black. 2010. Keyword analysis: A new tool for qualitative research. In The SAGE Handbook of Qualitative Methods in Health Research. Edited by Ivy Bourgeault, Robert Dingwall and Ray De Vries. London: SAGE. [Google Scholar]
- Sigurdson, Ola. 2016. Existential health: Philosophical and historical perspectives. LIR Journal 6: 8–26. [Google Scholar]
- Sinclair, Shane, and Harvey Max Chochinov. 2012. Communicating with patients about existential and spiritual issues: SACR-D work. Progress in Palliative Care: Spiritual Care 20: 72–78. [Google Scholar] [CrossRef]
- Sjursen, Irene, Eva Gjengedal, and Kari Kvigne. 2015. The courage of the nurse is critical to strengthen the trust and courage of major burn patients. [Sjukepleiaren sitt mot fremmar tillit og styrkar livsmotet hjå alvorleg brannskadde pasientar]. Nordisk Sygeplejeforskning 5: 166–78. Available online: http://www.idunn.no/nsf/2015/02/sjukepleiaren_sitt_mot_fremmar_tillit_og_styrkar_livsmotet_ (accessed on 6 May 2021). [CrossRef]
- Skaiå, Anders. 2003. The importance of meaning. [Betydningen av mening]. Tidsskrift for Den Norske Laegeforening 123: 1877–79. Available online: http://tidsskriftet.no/2003/06/kronikk/betydningen-av-mening (accessed on 9 May 2021).
- Slang, Renate, Lene T. Finsrud, and Brita F. Olsen. 2020. Nursing interventions in intensive care unit patients with breathing difficulties: A scoping review of the evidence. Nordic Journal of Nursing Research 40: 176–87. [Google Scholar] [CrossRef]
- Slåttå, Lina Søreide, and Ole Jacob Madsen. 2014. ‘I swim alone’—An ecopsychological exploration of the final conditions in existential psychotherapy. [‘Jeg svömmer alene’. En ökopsykologisk utforskning av de endelige vilkår i eksistensiell psykoterapi]. Scandinavian Psychologist 1: 1–15. [Google Scholar] [CrossRef]
- Søberg, Ane Inger Bondahl, Sigrid Helene Kjørven Haug, Lars Johan Danbolt, Lars Lien, and Torgeir Sørensen. 2018. Existential themes in the treatment of people at suicide risk. Understandings and practices of specialist healthcare professionals. Mental Health, Religion & Culture 21: 588–600. [Google Scholar] [CrossRef]
- Solvoll, Betty-Ann. 2016. Relatives’ experiences during the dying process of a loved one. [Erfaringer med å vaere pårörende når en naerstående er döende]. Nordisk Tidsskrift for Helseforskning 12: 1–13. [Google Scholar] [CrossRef][Green Version]
- Sörbye, Liv Wergeland, and Birgit Brunborg. 2015. Managing life is more than physical functioning. [Å mestre livet er mer enn fysisk fungering]. Geriatrisk Sykepleie 7: 6–12. Available online: https://sykepleien.no/sites/sykepleien.no/files/gs_0115.pdf#Page=6 (accessed on 5 May 2021).
- SOU Statens offentlige utredningar [Swedish Government Official Report]. 2000. Döden angår oss alla: Värdig vård vid livets slut: Delbetänkand: Utveckla kvaliteten i den palliativa vården [Death Concerns Us All: Dignified Care at the End of Life: Interim Report: Developing the Quality of Palliative carE]: Bilaga til SOU 2000:6. 0375-250X9138211173. Stockholm: Fakta Info Direkt. [Google Scholar]
- Stålhandske, Maria Liljas. 2008. Omöjligt och nödvändigt-Kvinnors livsfrågor och psykiska välbefinnande i samband med abort. [Necessary and impossible. Women’s world views and psychological wellbeing in relation to abortion]. Social-medicinsk tidskrift 85: 139–49. [Google Scholar]
- Stifoss-Hanssen, Hans. 1999. Religion and spirituality: What a European ear hears. The International Journal for the Psychology of Religion 9: 25–33. [Google Scholar] [CrossRef]
- Stifoss-Hanssen, Hans, and Kjell Kallenberg. 1996. Existential Questions and Health: Research FRONTLINES and Challenges. Stockholm: Swedish Council for Planning and Coordination of Research, vol. 96. [Google Scholar]
- Stolt, Carl-Magnus. 2006. “The lonely secret”. Medical history and existential aspects of the HIV-infection. A qualitative text study in patient records. [“Den ensamma hemligheten”. Samtidshistoria och existentiella aspekter vid HIV-infektion. En kvalitativ studie av den medicinska journalens texter]. Socialmedicinsk Tidskrift 83: 347–54. [Google Scholar]
- Stranden, Elin, Ida Foyn Gundersen, Linn Okkenhaug Getz, Anna Luise Kirkengen, Kai Brynjar Hagen, and Bente Prytz Mjølstad. 2020. Belastende livserfaringer blant pasienter med sykelig overvekt. [Stressful life experiences among patients with morbid obesity.]. Tidsskrift for Den Norske Laegeforening 140: 1–10. [Google Scholar] [CrossRef]
- Strang, Peter. 2016. Existential anxiety might reinforce bodily symptoms. [Existentiell kris i livets slutskede förstärker de fysiska symtomen]. Läkartidningen 113: 2105–107. Available online: http://www.lakartidningen.se/Klinik-och-vetenskap/Temaartikel/2016/11/Existentiell-kris-i-livets-slutskede-forstarker-de-fysiska-symtomen/ (accessed on 5 May 2021).
- Strang, Peter, and Susann Adelbratt. 1999. Spiritual values can make the suffering meaningful and manageable. Existential questions are of current interest in palliative care. [Andlighet kan göra lidandet meningsfullt och hanterbart. Existentiella frågor aktualiseras i palliativ vård]. Läkartidningen 96: 2942–44. [Google Scholar]
- Strang, Peter, and Barbro Beck-Friis. 1999. Better routines for existential support are required (letter). [Bättre rutiner för existentiellt stöd behövs]. Läkartidningen 96: 4410. [Google Scholar]
- Sundal, Hildegunn, and Else Lykkeslet. 2020. Sometimes falling out of normal life. Nordisk Sygeplejeforskning 10: 213–22. [Google Scholar] [CrossRef]
- Sundhetsstyrelsen [Danish Health Authority]. 2017. Anbefalinger for den Palliative Indsats [Recommendations for Palliative Care]. Available online: https://www.sst.dk/da/sygdom-og-behandling/~/media/79CB83AB4DF74C80837BAAAD55347D0D.ashx (accessed on 1 May 2020).
- Thörn, Å. 1998. Existential crisis of the medical profession? [Är läkarkårens kris existentiell?]. Läkartidningen 95: 4451–52. [Google Scholar] [PubMed]
- Thorsen, Rolf. 2018. Reflections on the ethics of concern. [Å, hvordan skal dette gå—En undring omkring bekymringens etikk]. Tidsskrift for Omsorgsforskning 4: 233–40. [Google Scholar] [CrossRef]
- Thorsen, Rolf. 2019. Reflections on life courage. [En sang til (livs)motet—En undring omkring fenomenet livsmot]. Nordisk Tidsskrift for Helseforskning 15: 1–16. [Google Scholar] [CrossRef]
- Thorsen Gonzalez, Marianne. 2013. Existential benefits of therapeutic horticulture for clinical depression: A prospective study. [Betydningen av terapeutisk hagebruk ved klinisk depresjon: En prospektiv studie i et eksistensielt perspektiv]. Tidsskrift for Psykisk Helsearbeid 10: 138–48. Available online: http://www.idunn.no/ts/tph/2013/02/betydningen_av_terapeutisk_hagebruk_ved_kliniskdepresjon_ (accessed on 4 May 2021). [CrossRef]
- Toivonen, Kristiina, Andreas Charalambous, and Riitta Suhonen. 2018. Supporting spirituality in the care of older people living with dementia: A hermeneutic phenomenological inquiry into nurses’ experiences. Scandinavian Journal of Caring Sciences 32: 880–88. [Google Scholar] [CrossRef]
- Torraco, Richard J. 2016. Writing integrative literature reviews: Using the past and present to explore the future. Human Resource Development Review 15: 404–28. [Google Scholar] [CrossRef]
- Ueland, Venke, Dagfinn Nåden, and Unni Å. Lindström. 2018. Longing—A dynamic power in the becoming of health when suffering from cancer. Scandinavian Journal of Caring Sciences 32: 924–32. [Google Scholar] [CrossRef]
- Ulland, Dagfinn, and Valerie DeMarinis. 2014. Understanding and working with existential information in a Norwegian adolescent psychiatry context: A need and a challenge. Mental Health, Religion & Culture 17: 582–93. [Google Scholar] [CrossRef]
- Urstad, Sivert Skålvoll. 2017. The Religiously Unaffiliated in Norway. Nordic Journal of Religion and Society 30: 61–81. [Google Scholar] [CrossRef]
- Viftrup, Dorte Toudal, Christina Prinds, Vibeke Østergaard Steenfeldt, and Niels Christian Hvidt. 2020. Nu er det hele snart forbi: Et kvalitativt studie af terminale patienters sproglighed omkring død og efterliv [Now it’s all over soon: A qualitative study of terminal patients’ linguistics about death and afterlife]. Klinisk Sygepleje 34: 161–75. [Google Scholar] [CrossRef]
- Wang, Catharina Elisabeth Arfwedson, Reni J. Wright, Siren Hope, and Trond Waage. 2012. Youth Gaze: Self-reflective filmmaking as a therapeutic method. [Ungdomsblikk: Selvrefleksivt filmkurs som terapeutisk metode]. Tidsskrift for Norsk Psykologforening 49: 861–69. Available online: http://www.psykologtidsskriftet.no/index.php?seks_id=272903&a=2 (accessed on 4 May 2021).
- Whittemore, Robin, and Kathleen Knafl. 2005. The integrative review: Updated methodology. Journal of Advanced Nursing 52: 546–53. [Google Scholar] [CrossRef] [PubMed]
- Yalom, Irvin D. 1980. Existential Psychotherapy. New York: Basic. [Google Scholar]





| Purpose/Method | Outcome | Cumulative Insight | |
|---|---|---|---|
| Stage 1 | Exploratory review of the trajectory and evolution of the concept within the published literature | Mapping the evolution of the concept | Synthesis of the components and elements that have informed the evolution and contemporary understanding of the concept |
| Stage 2 | Keyword analysis of the definitions published in the literature | Identification of definitions and key attributes of the concept | |
| Stage 3 | Thematic analysis of the application and implementation of the concept as used in healthcare research and professional journals | Thematic representation of how the concept is applied in healthcare journals |
| Definition No. | Author(s) (Year) | Definition |
|---|---|---|
| 1. | Yalom (1980, pp. 5, 8) | ‘… four ultimate concerns: death, freedom, isolation, and meaninglessness. The individual’s confrontation with each of these facts of life constitutes the content of the existential dynamic conflict.’ (p. 8) ‘The label for this approach, “existential psychotherapy”, defies succinct definitions, for the underpinnings of the existential orientation are not empirical but are deeply intuitive … I shall elucidate that definition: existential psychotherapy is a dynamic approach to therapy which focuses on concerns that are rooted in the individual’s existence … but, of all the therapy vocabularies, none rivals the existential in vagueness and confusion. Therapists associate the existential approach with such intrinsically imprecise and apparently unrelated terms as “authenticity”, “encounter”, “responsibility”, “choice”, “humanistic”, “self-actualization”, “centring”, “Sartean” and “Heideggerian”.’ (p. 5) |
| 2 | DeMarinis (2006, pp. 44–45; 2008, p. 60) | ‘The existential dimension is focused on the individual’s understanding of existentiality and the way meaning is created. This dimension includes worldview conception, life approach, decision-making structure, way of relating, and way of understanding. It also includes activities or expressions of symbolic significance, such as rituals and other ways of making meaning. As each individual has an existential dimension and spiritual nature, the varieties of their expression include many different kinds of meaning systems. These can be associated with traditional religious systems or with other meaning-making systems. For the individual it is also possible to have elements of different systems combined.’ |
| 3 | Hummelvoll (2006, p. 22) | ‘Existential here means what concerns human existence and life situations—that is, problems and challenges that people encounter related to, for example, freedom of will and responsibility of choice.’ |
| 4 | la Cour and Hvidt (2010, p. 1293) | ‘… secular existential orientations, such as meaning, the value of life, personal values, freedom, responsibility, loneliness, etc., all concepts that are not centered in the belief in a transcendent reality. These concepts often have the potential for including the spiritual and religious domains, but they rarely do so in any elaborative or concise way.’ |
| 5 | Sigurdson (2016, p. 21) | ‘I argue that existential health should not be seen as yet another dimension of health—not even spiritual health, the most likely candidate as Valerie DeMarinis and Cecilia Melder, two prominent Swedish psychologists of religion, have argued—but rather as a reflexive experience of health. By “reflexive” I mean an intentional relation to one’s own experience of ailment and health, including a relation to these experiences as one’s own. My conclusion is that existential health as a concept should be reserved for this reflexive feature of human subjectivity in relation to health, cutting across all other health dimensions, so as not to confuse the conceptuality in speaking of health.’ (Abstract) ‘Existential health is, I would suggest, a non-instrumentalizable aspect of our subjectivity or personhood; it is not something I need to get along with my life, it is rather the very act of living this life as I am living it. Despite all its flaws and shortcomings and diseases, I am healthy, existentially, when this life is mine!’ |
| 6 | Hvidt et al. (2018, p. 272) | ‘The existential … a broad category… A factor analysis indicated four understandings of the existential: 1. Essential meaning of life, 2. Spirituality, 3. Existential thinking, oriented about philosophical traditions, and 4. Crisis management. People find meaning in primarily three existential domains of meaning: Secular (not spiritual nor religious, for instance the significance of family or the work), spiritual (the inner spiritual life, for instance, meditation, experienced connectedness with nature or the universe), and religious (understood as beliefs one shares and practices with others, typically on the basis of holy scriptures, such as the Bible)’ |
| 7 | Prause et al. (2020, p. 281) | ‘Giske and Cone (2019) point out that existential concerns can be expressed through the psychosocial and physical level. However, they also describe existential care as a dimension characterized by “touching the innermost of a human being” (p. 20) in times of seeking and pain. Pargament (2013) relates the existential dimension explicitly to an experience of a sacred quality through interconnecting and caring.’ |
| 8 | Frøkedal (2020, pp. 17–18) | ‘The existential dimension is viewed as an overarching concept, encompassing secular, religious and spiritual domains (DeMarinis 2003, 2008; la Cour and Hvidt 2010). The existential dimension is a broad concept that includes a worldview conception, a life approach, and a decision-making structure, as well as a way of relating to and understanding rituals and other ways of making meaning (DeMarinis 2003, 2006, 2008).’ (p. 17) ‘Existential issues within the secular, religious and spiritual domains (DeMarinis 2003, 2008; la Cour and Hvidt 2010) have been used interchangeably to describe beliefs, values and ultimate meaning in human life (Sinclair and Chochinov 2012).’ (p. 18) |
| 9 | Viftrup et al. (2020, p. 162) | ‘Existential language we define as words, concepts and understandings within three existential domains of meaning: the secular (life relationship, that are meaningful and significant to the individual, but which are not religious, e.g., values, meaning of family or work), the spiritual (the inner spiritual life experienced as transcendent for the individual) and/or the religious (beliefs and understandings, which one shares and practices with others, e.g., bible reading and church attendance).’ |
| 10 | Binder (2022, p. 3) | ‘A possible modification of Yalom’s concepts that might be useful … is to describe these existential concerns as polarities: Death and awareness of living a life of one’s own, meaning and meaninglessness, being with and isolation, and freedom and limitation and conditionings.’ |
| Definition No. and Frequency of Words | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Attribute | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | Total |
| Authenticity | 1 | 1 | |||||||||
| Belief(s) | 1 | 1 | 1 | 1 | 4 | ||||||
| Care/caring | 1/1 | 1/1 | |||||||||
| Centring | 1 | 1 | |||||||||
| Choice | 1 | 1 | 2 | ||||||||
| Death | 1 | 1 | 2 | ||||||||
| Decision-making | 1 | 1 | 2 | ||||||||
| Dimension/dimensions/ domains | 3/0/0 | 0/0/1 | 1/1/0 | 0/0/1 | 2/0/0 | 2/0/2 | 0/0/1 | 8/1/5 | |||
| Encounter | 1 | 1 | 2 | ||||||||
| Existence | 1 | 1 | 2 | ||||||||
| Existential/existentiality/ existentially | 6 | 2/1/0 | 1 | 1 | 3/0/1 | 4 | 3 | 3 | 3 | 1 | 26/1/1 |
| Freedom | 1 | 1 | 1 | 1 | 4 | ||||||
| Health/y | 10/1 | 10/1 | |||||||||
| human being/life/existence | 0/0/1 | 1/0/0 | 0/1 | 1/1/1 | |||||||
| Humanistic | 1 | 1 | |||||||||
| Individual/s | 0/1 | 1/2 | 2/0 | 3/3 | |||||||
| Inner/spiritual/most | 1/0 | 0/1 | 1/0 | 2/1 | |||||||
| Isolation | 1 | 1 | 2 | ||||||||
| Interconnecting | 1 | 1 | |||||||||
| Intuitive | 1 | 1 | |||||||||
| Loneliness | 1 | 1 | |||||||||
| Meaning/meaningful | 3 | 1 | 3 | 2 | 2/1 | 2 | 13/1 | ||||
| Meaninglessness | 1 | 1 | 2 | ||||||||
| Making meaning | 1 | 1 | 2 | ||||||||
| Personal/personhood | 1 | 1 | 1/1 | ||||||||
| Reflexive | 3 | 3 | |||||||||
| Religion | 1 | 1 | |||||||||
| Religious | 1 | 1 | 2 | 2 | 2 | 8 | |||||
| Responsibility | 1 | 1 | 1 | 3 | |||||||
| Rituals | 1 | 1 | 2 | ||||||||
| Sacred | 1 | 1 | |||||||||
| Secular | 1 | 1 | 2 | 1 | 5 | ||||||
| Self-actualisation | 1 | 1 | |||||||||
| Spiritual/spirituality | 1 | 1 | 1 | 3/1 | 2 | 2 | 10/1 | ||||
| Symbolic significance | 1 | 1 | |||||||||
| Systems | 4 | 4 | |||||||||
| Transcendent | 1 | 1 | 2 | ||||||||
| Value/values | 1/1 | 0/1 | 0/1 | 1/3 | |||||||
| Worldview | 2 | 1 | 2 | ||||||||
| Overarching Themes | Numbers of the Articles | Total Numbers |
|---|---|---|
| Suffering and re-orientation | 3,4,5,6,7,9,10,13,14,15,17, 21, 23, 26, 28, 31, 32, 33, 36, 37,44, 47, 48, 49, 52, 53, 55, 56, 57, 60,61, 62, 64, 65, 71, 72, 73, 74, 75, 79, 80, 85, 88, 90, 91, 93, 95, 96, 97, 99, 100, 103, 106 | 53 |
| Meaning and meaninglessness | 1, 3, 5, 7, 8, 14, 20, 21, 22, 29, 31, 35, 36, 37, 39, 42, 47, 48, 49, 54, 62, 67, 69, 70, 76, 77, 83, 93, 100, 108 | 30 |
| Existential philosophy in relation to health | 2, 5, 7, 11, 15, 18, 19, 24, 25, 29, 39, 43, 45, 46, 50, 51, 58, 63, 73, 76, 82, 87, 90, 94, 98, 107 | 26 |
| Existential questions as approaches to care | 4, 5, 7, 8, 9, 12, 16, 21, 27, 30, 31, 36, 37, 39, 41, 59, 60, 65, 69, 70, 76, 77, 101, | 23 |
| Usage and demarcation of existential, spiritual and religious concepts | 1, 5, 7, 9, 12, 13, 20, 27, 30, 37, 39, 40, 70, 76, 77, 83, 92, 99, 105, 108 | 20 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nygaard, M.R.; Austad, A.; Sørensen, T.; Synnes, O.; McSherry, W. ‘Existential’ in Scandinavian Healthcare Journals: An Analysis of the Concept and Implications for Future Research. Religions 2022, 13, 979. https://doi.org/10.3390/rel13100979
Nygaard MR, Austad A, Sørensen T, Synnes O, McSherry W. ‘Existential’ in Scandinavian Healthcare Journals: An Analysis of the Concept and Implications for Future Research. Religions. 2022; 13(10):979. https://doi.org/10.3390/rel13100979
Chicago/Turabian StyleNygaard, Marianne Rodriguez, Anne Austad, Torgeir Sørensen, Oddgeir Synnes, and Wilfred McSherry. 2022. "‘Existential’ in Scandinavian Healthcare Journals: An Analysis of the Concept and Implications for Future Research" Religions 13, no. 10: 979. https://doi.org/10.3390/rel13100979
APA StyleNygaard, M. R., Austad, A., Sørensen, T., Synnes, O., & McSherry, W. (2022). ‘Existential’ in Scandinavian Healthcare Journals: An Analysis of the Concept and Implications for Future Research. Religions, 13(10), 979. https://doi.org/10.3390/rel13100979