1. Introduction
In recent years, several studies have demonstrated the impact of spirituality on health outcomes (
Koenig 2012;
Moreira-Almeida 2007). Thus, studies on the integration of spirituality in health care have been gaining attention, as it is observed that although the benefits are, in general, more positive than negative, there are some segments that indicate a more controversial relationship, as is the case, for example, of sexual and gender minorities (
Fontenot 2013). By the term sexual and gender minorities, we are referring to people with affective-sexual orientations, gender identities, and the development of sexual characteristics other than cis-heteronormativity, i.e., the assumption that heterosexuality is the norm and that everyone is straight and identifies themselves with their biological sex (cisnormativity).
A recent literature review identified the ambivalence concerning the impacts of spirituality and religion on the mental health of sexual and gender minorities, demonstrating that this dimension can contribute both to better mental health outcomes and to its worsening (
Rosa and Esperandio 2022). This review also highlighted the importance of developing more studies that provide more clarity regarding the impacts of this association, especially in the Brazilian context.
In this study, we understand spirituality as a “dynamic and intrinsic aspect of humanity through which persons seek ultimate meaning, purpose, and transcendence, and experience relationship to self, family, others, community, society, nature, and the significant or sacred.” (
Puchalski et al. 2014, p. 646). Therefore, it is understood that spirituality is a central dimension of human subjectivity and existentiality itself. According to (
Esperandio 2020b, p. 161), it is this dimension “that moves the human being in search of objects, situations and experiences in order to meet the ‘human need for meaning’”. Likewise, in his theory known as “logotherapy” or “meaning-centered psychotherapy”, the psychiatrist Viktor Frankl conceives that the human being is a spiritual being moved by the “will to meaning” (
Frankl 1987, p. 69). For the author, finding meaning does not mean a feeling of mere well-being, as the absence of suffering, but rather having something to live for and give one’s life purpose (
Frankl 1987, pp. 62, 79–80). Therefore, finding meaning in a situation of suffering does not indicate a change in this situation, but a change in the person’s attitude (
Frankl 1987, p. 76).
Religion is understood as a set of beliefs, practices, and rituals related to transcendence in its most varied and distinct names (
Koenig et al. 2012, p. 45). The term religiosity derives from religion and refers to personal involvement in specific religious activities, such as prayers and attendance at services, masses, meetings, and others. As
Esperandio (
2014 p. 808) observes, “in general, the religious person assumes certain truths and ethical-moral practices and values linked to an established religion”. Therefore, binomial spirituality/religiosity (S/R) is used as a broader term, clarifying that in the search for meaning and purpose, the answers can be found inside or outside the parameters of established religion.
The use of spiritual/religious elements to cope with stress and suffering situations has been theorized and defined by the religious psychologist Kenneth
Pargament (
1997) as spiritual and religious coping (SRC). The large number of empirical research developed in the emerging field “Spirituality & Health” attests that, in this context of searching for meaning and facing life’s adversities, the role played by spirituality can be assessed (
Esperandio 2020a). Therefore, several instruments have been validated and provide theoretical and scientific support for an accurate assessment of these elements. Thus, the goal of this study was to assess the S/R of sexual and gender minorities, seeking to identify spiritual resources and the correlation between RSS and style of attachment to God.
2. Materials and Methods
This is a cross-sectional, descriptive, and exploratory study. Data were collected online by means of a questionnaire hosted on the Qualtrics Platform.
The hypothesis of the study was that this group would have a high prevalence of RSS, a more private religious practice, and unlike the Brazilian population, which is highly religious (
Huber and Huber 2012;
Esperandio et al. 2019), religiosity would not occupy a central place in the lives of this group. This hypothesis is based on the empirical observation of the authors that this group moves away from religious communities because they feel little understood and not welcomed in their gender identity and sexual orientation. However, deidentification with the religious group does not necessarily express a solution to spiritual and religious struggles due to “religious residues”, as noted by
Van Tongeren et al. (
2021).
For the recruitment of participants, convenience sampling and snowball techniques were used, initiated through an invitation to participate in the study. The inclusion criteria in the research were voluntary participation, being older than 18 years of age, being able to understand the questions, and self-identification as a sexual and gender minority, in addition to signing the Free and Informed Consent Form (ICF).
This invitation was made available to the authors’ contacts and also to groups of activists, gender and sexuality scholars, sexual and gender minorities, and non-government organizations (NGOs) for the protection and defense of the rights of these groups, which were previously mapped.
This study was approved by the Research Ethics Committee (Process 4,122,312). There was no sample calculation to define the number of participants. People who self-identified as cis male, cis female, and heterosexual, and people who did not respond completely to the survey instrument, were excluded, leaving 308 valid samples for analysis. Data were collected between July and November 2020. In the assessment of spirituality, the following instruments were used: (1) A sociodemographic questionnaire; (2) the Centrality of Religiosity Scale (CRS); (3) the SRCOPE Scale—14 items; (4) the Religious and Spiritual Struggles (RSS) Scale; (5) the Attachment to God Inventory (AGI-BR); and (6) the Satisfaction with Life Scale (SWLS). The sociodemographic questionnaire included questions about religious transit and deidentification, the influence of S/R in the process of accepting the own gender identity and/or affective/sexual orientation, and participation in “gay healing” therapies, in addition to questions regarding “coming out” (or not) to the faith community and family and the support received from them, and also the assessment of the suicidal ideation in this population group.
The S/R assessment scales were chosen according to their relevance to the objective of the study. The Centrality of Religiosity Scale (CRS—5) (
Esperandio et al. 2019) identifies five dimensions that can be seen as representative of religious life. Such dimensions are intellectual (indicated by the frequency with which the person thinks about religious issues), ideological (indicated by the plausibility of the existence of a transcendent reality), public practice (indicated by the frequency with which the individual participates in religious activities), private practice (indicated by the intensity with which the individual performs practices such as prayer and meditation), and the dimension of religious experience (indicated by the intensity with which the individual is confronted with questions about the ultimate reality). This instrument also allows for assessing whether religiosity is central to a person’s life and can be characterized as highly religious, religious, and non-religious.
The Brief SRCOPE-14 items (
Esperandio et al. 2018) were applied to measure the use of positive and negative religious coping with major life stressors. This instrument consists of an open question and 14 closed items, answered on a five-point Likert scale (1—not at all; 5—very much). The first seven items indicate positive SRCOPE and the other seven refer to negative SRCOPE strategies.
The first open question asks the participant to describe, in a few words, the most stressful situation experienced in the last 3 years. The alternatives lead the participants to indicate how much they did or did not do what is described in each alternative, based on the experienced situation. These questions were analyzed using the qualitative data analysis software ATLAS.ti. For the analysis process, we used
Saldaña’s (
2013) coding cycles. Initially, we used holistic coding, which consists of applying “a single code to a large unit of data in the corpus, rather than detailed coding, to capture a sense of the overall contents and the possible categories that may develop” (
Saldaña 2013, p. 264). Finally, focused coding was used, which allowed for the categorization of the coded data based on thematic similarities.
Struggle experiences that are based on beliefs, practices, interpersonal relationships, or experiences related to the sacred are called “religious and spiritual struggles” (
Exline et al. 2014). RSS was assessed using the full Brazilian version of the RSS Scale—24 items (
Esperandio et al. 2022). This scale aims to measure 6 domains of RSS: Divine (negative emotions based on beliefs about God, or the perceived relationship with God); demonic (concerns related to the belief that the devil or evil spirits are attacking and causing negative events); interpersonal (concern about negative experiences with people or religious institutions); moral (struggles in an attempt to follow the own moral principles; worry or guilt related to committed offenses); doubt (discomfort generated by doubts or questions related to the own spiritual/religious beliefs); and ultimate meaning (conflicts related to issues around meaning and purpose in life) (
Exline and Rose 2013;
Exline et al. 2014). The answers to the 24 items, on a Likert scale from 1 to 5, allow the following classification, based on the scale parameters: None or negligible: 1.00 to 1.50; low: 1.51 to 2.50; average: 2.51 to 3.50; high: 3.51 to 4.50; very high: 4.51 to 5.00.
Regarding Attachment to God, this theory was developed by
Kirkpatrick and Shaver (
1992) based on Bowlby’s Attachment Theory. The authors observed that secure attachment relationships are those in which the individual maintains a comfortable relationship with God and perceives him as being cordial, sensitive, and prompt to support and protect, even when people make mistakes. The avoidant type of attachment, on the other hand, is characterized by the image of God as an impersonal, distant figure who shows little or no interest in the individual’s personal issues. Anxious is a type of attachment characterized by the image of a fickle God, who is sometimes affectionate and responsive and sometimes not. Finally, anxious-avoidant, or disorganized attachment, identified by
Main and Solomon (
1986), consists of the development of inconsistent and contradictory behaviors towards the attachment figure (
Esperandio and August 2014).
The literature points out that different patterns of attachment to God have implications for the mental health of individuals (
Rowatt and Kirkpatrick 2002;
Leman et al. 2018), hence “the attachment to God can be an important means to alleviate suffering and repair the person’s internal functioning models after a loss or because of experiences of abandonment by other attachment figures” (
August and Esperandio 2020, p. 303). According to
Esperandio and August (
2014, p. 252), “people can reproduce the same type of human attachment in their relationship with God”. Attachment styles can be secure, anxious, avoidant, and anxious-avoidant.
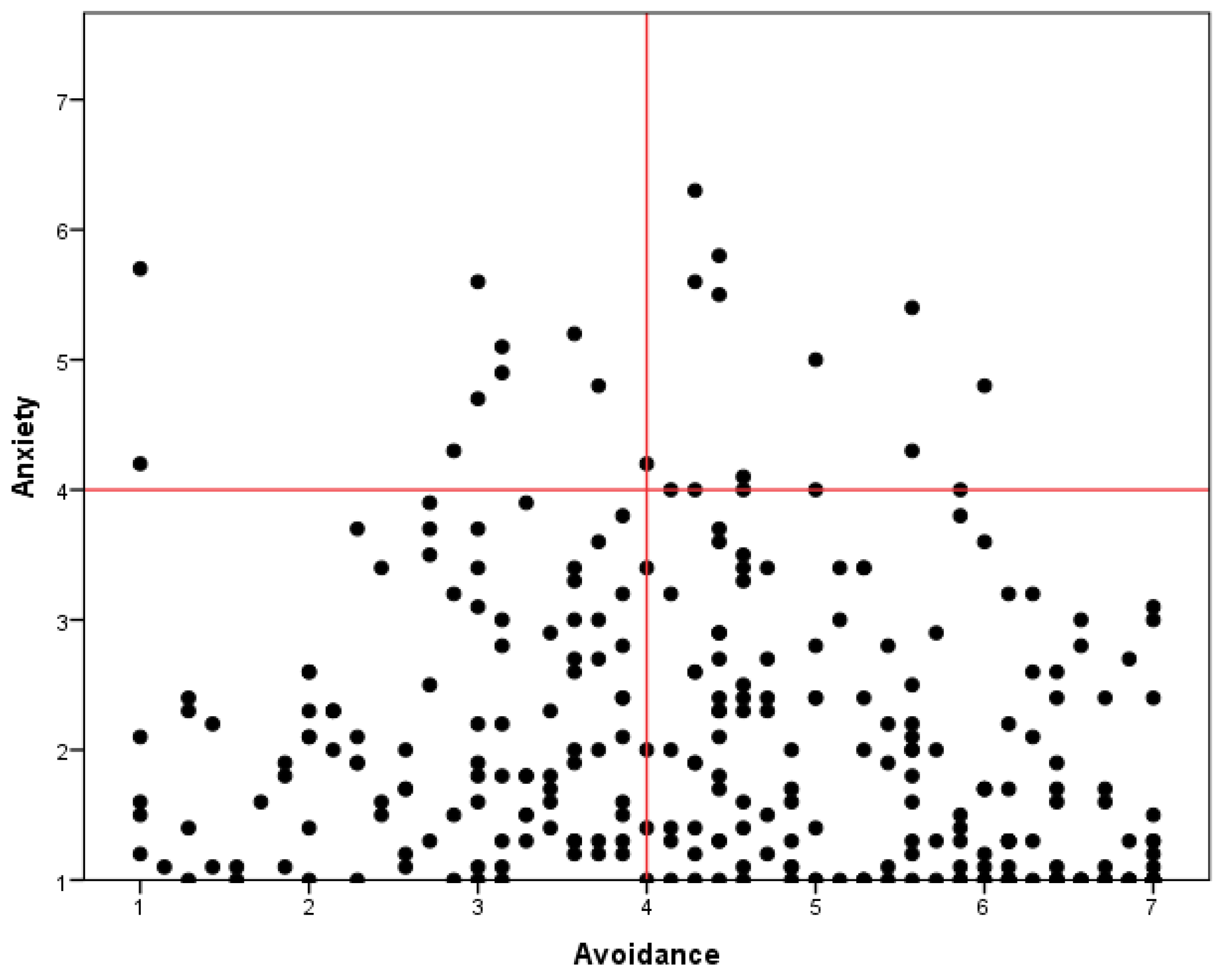
The styles of Attachment to God were identified through the application of the AGI-BR (
August et al. 2018). This instrument consists of 17 questions, answered on a Likert scale with seven points (1—strongly disagree to 7—strongly agree), with the first seven questions referring to the Avoidance of Intimacy with God dimension and the other 10 to the dimension of Anxiety for Abandonment by God. Such an instrument makes it possible to assess how the person experiences his or her relationship with God.
Concerning satisfaction with life (SWL), this was measured using the SWL Scale (
Diener et al. 1985). This instrument assesses how satisfied people are with their lives and how close they believe their lives are to their ideals. This scale has five items, answered on a seven-point Likert scale, ranging from 1 (strongly disagree) to 7 (strongly agree). The parameters used for classification are extremely satisfied, very satisfied, slightly satisfied, neutral, slightly dissatisfied, dissatisfied, and extremely dissatisfied.
As for the analysis procedures, data were analyzed using Excel (Microsoft Office 2016. Excel. USA) and SPSS—Statistical Package for Social Science (IBM Corp. Released 2011. IBM SPSS Statistics for Windows, Version 20.0. Armonk, NY, USA: IBM Corp.). Initially, descriptive analyses were performed (mean, frequency, and percentage) of all variables in the sample. Cronbach’s alpha coefficient was used to assess the reliability of the used scales. All presented values above 0.7, namely SWLS (0.849), SRCOPE (0.884), CRS (0.844), AGI-BR (0.787), and RSS (0.770). Subsequently, Pearson correlations were performed in order to investigate the relationships between some of the study variables. The non-parametric Mann–Whitney U test was used to assess the differences in the means of the RSS Scale and Satisfaction with Life, in relation to the support received from the faith community and/or family members in the process of coming out. This test was also used to evaluate the differences in the means of RSS, in relation to the transition of religious affiliation.
4. Discussion
One of the main constructs that explain how stigma and discriminatory attitudes impact mental health outcomes of sexual and gender minorities is the Minority Stress Model. Emerging from a range of psychological and social studies, the Minority Stress Model suggests that stigma, prejudice, and discrimination create a hostile social environment that results in specific stressors that impair the mental health of marginalized populations (
Meyer 2003). Applying this model to gay men,
Meyer (
1995) postulated three processes of minority stress, namely internalized homophobia, perceived stigma, and experiences of discrimination and violence.
Meyer (
2003) classifies such stressors as distal (related to external factors such as antigay violence, discrimination, and experiences of prejudice events in several social contexts), and proximal stressors (referred to as internal stressors, related to one’s own identity such as the devaluation of the self and poor self-regard).
Up to the beginning of data collection, there were no instruments adapted for the assessment of Minority Stress in the Brazilian context. However, the first open question of the SRCOPE Scale revealed that specific stressors, related to the recognition of these people as sexual and gender minorities, are existing, being either a recognition that comes from themselves or a recognition that comes from other people. As we can see, the most prevalent category of stress situation (
Table 2) was “Interpersonal problems”, which includes stressful situations related to conflicts with other people. This category mainly gathers love/affective problems. Another category that stands out is “Family problems”, and this category has a high rate of co-occurrence with the category “Prejudice/violence”, as expressed in the following narratives:
My father used to hit me because of my sexual orientation, so I tried to seek support from the church to recover. He said that church was for “softies” and forbade me to go, however, I kept going without him knowing. In church, I felt like they wanted to exorcise me. (Cis male, Homosexual, 28 years old);
I suffered physical and verbal aggression from my family because of my sexuality. (Cis female, Homosexual, 18 years old).
In the absence of specific instruments, it was not possible to carry out a precise assessment of the prevalence of stress in minorities and its relationship with other aspects that were evaluated in this study. It is also important to note that during the study period, the COVID-19 pandemic was ongoing. In this context of crisis, the vulnerabilities faced by sexual and gender minorities have significantly increased (
Outright Action International 2020). A national study, carried out by the collective #VoteLGBT and Box1824 (
#VOTELGBT 2021), identified the main challenges faced by Brazilian sexual and gender minorities in the context of continuing social isolation because of the Coronavirus pandemic: Worsening of financial vulnerability; worsening of mental health and withdrawal from the support network; and marked dissatisfaction with the government (
#VOTELGBT 2021). The greater vulnerability of this population group during the COVID-19 pandemic is confirmed through the situations reported in intrafamily or domestic violence reports, financial problems, and reports that demonstrate the worsening of mental health.
The literature shows that in contexts of increased stress and suffering, S/R can play an important role, as the study of
Lucchetti et al. (
2021) on mental health and social isolation in times of COVID-19 has been demonstrated. The researchers found that religiosity was associated with higher levels of hope, better health outcomes, and lower levels of fear, preoccupation, and sadness. However, there are no studies on the role played by S/R in coping with stress among Brazilian sexual and gender minorities. Therefore, we sought to investigate whether this population group used S/R as a coping strategy in stressful situations, and the correlation with attachment to God.
The general Brazilian population is classified as “Highly Religious” with a centrality of religiosity mean of 4.01 (
Esperandio et al. 2019). As demonstrated in the study, sexual and gender minorities differ from the Brazilian religious scenario, and are classified as “Religious”, which indicates that
the personal religious system holds merely a subordinate position within the personality’s cognitive and emotional architecture. Though religious content can indeed be found in the person’s life-horizon, it cannot be expected to have a clearly determinant effect on experience and behavior. Religion plays more of a background role.
It is also important to emphasize that the centrality of religiosity “is related to the efficacy of religion. The more central religion is, the greater is its impact on the experience and behavior of a person” (
Huber 2006, p. 2). In this sense, the parameters for using the SRCOPE also point to the secondary role of religion in the experiences of a large part of the sample, and the use of spiritual/religious resources in the management of stressful situations was classified as “medium”. However, it should be noted that the positive correlations between the variables of the centrality of religiosity, positive SRCOPE, and satisfaction with life demonstrate that religiosity can play a protective role for those who have it as a central dimension.
McCarthy (
2008), in a study that aimed to evaluate SRCOPE strategies among Christian LGB adolescents in the USA, revealed that they do not use positive SRCOPE strategies to deal with minority stress. One of the hypotheses raised by the author is that the homonegative spiritual and cultural context interferes with access to positive religious resources. Similarly,
Ritter and O’Neill (
1989) argue that sexual and gender minorities can experience tremendous loss because traditional religions fail to provide a viable religious experience. In part, these statements are confirmed in our study, considering the presence of a significant positive correlation between the anxious Attachment to God and Centrality of religiosity. A significant correlation was also found between negative SRCOPE strategies and anxiety. The negative correlation between anxiety and satisfaction with life is also highlighted. These data show the paradoxical aspect of religiosity in the experiences of Brazilian sexual and gender minorities, which reinforces the need for spiritual assistance.
Critical components of religion, namely RSS and negative SRCOPE strategies, were classified as “Low” in this sample. However, the higher prevalence of struggles with meaning as well as the suicidal ideation rate in this sample caught our attention. In addition, participants that reported having difficulties accepting their sexuality due to religiosity had higher scores in all dimensions of struggles, with an emphasis on interpersonal problems with a mean of 3.03. The importance of family and religious reception is highlighted, considering that participants that reported receiving support from their faith communities and/or their families in the process of “coming out” had lower scores in the dimensions of struggles, which seems to indicate that the support received in this process was fundamental for better self-acceptance.
Another fact that draws attention is the religious transit and deidentification of this group, which is presented in the literature as a strategy to face conflicts between sexual and religious identity (
Schuck and Liddle 2001;
Escher et al. 2019) and may also be related specifically to dealing with RSS (
Exline et al. 2021).
Rodriguez and Ouellette (
2000) postulated that Christian gays and lesbians, when facing struggles between sexual orientation and religious beliefs, may reject their Christian religious identity by becoming atheists, engaging in non-Christian religions, or rejecting aspects of their spiritual/religious practices, for example, no longer attending celebrations and no longer performing prayers. Therefore, it is postulated that leaving a denomination is a way of freeing oneself from the oppression present in heterosexist environments, as stated by
Davidson (
2000). However, according to
Sowe et al. (
2014), distancing from the religious denomination does not automatically eliminate trauma, in a way that past prejudices can still cultivate lasting psychological damage, considering that in the aforementioned study, former Christians continued to report higher levels of suffering than those who were never religious.
Van Tongeren et al. (
2021) theorize this process by stating that vestiges of spiritual/religious beliefs, practices, or behaviors can remain even after the process of deidentification, which has been termed as “religious residue”.
In summary, the operationalization of this population’s religiosity occurs mainly in the intellectual and ideological dimensions, that is, they demonstrate that they believe in God or something divine and think about religious issues. Consequently, the experience of religiosity for this population is more self-reflective, which is also confirmed by the low rate of public practice. The thoughts about religious issues in this sample may be related to seeking the reinterpretation of religious teachings of condemnation and violence and even the re-signification of the image of God. As the literature points out, it is possible that these strategies are being used as ways to face the struggle between sexual/gender identity and religious identity (
Schuck and Liddle 2001;
Dahl and Galliher 2010;
Hansen and Lambert 2011).
Concerning the literature about attachment to god, there is a greater anxious relationship with God among Christian sexual and gender minorities, being associated with greater internalized heterosexism, depression, anxiety, experiences of prejudice and discrimination, and greater suffering (
Maughan 2020). In the same study, Maughan also argues that the messages such people hear from their parents and/or religious leaders about how God sees them impact their God-attachment styles. As such, supportive messages for sexual and gender minorities are central to better mental health and a secure Attachment to God (
Maughan 2020).
The data from the present study demonstrate an expected result that, on one hand. a large part of the sample claims to believe in God, but on the other hand, there is a prevalence of an avoidant attachment style. We also expected a greater presence of RSS, which was not confirmed; however, the prevalence of the avoidant attachment to God can explain such a result. This raises the suspicion that the withdrawal from a personal relationship with God may be a strategy for dealing with RSS. This hypothesis should be further investigated in future studies. This result, however, already contributes to raising questions as to whether sexual and gender minorities are being excluded from the opportunity to develop their spiritual dimension because of religious oppression. In other words, sexual and gender minorities are pushed towards a “struggle solution” that takes away the possibility of fully living the dimension of spirituality/religiosity. In the dominant mode of contemporary subjectivation, it is as if a secure relationship with God and gender identities other than normative are not compatible, leaving sexual and gender minorities to withdraw from God as a way of dealing with RSS. Future studies investigating the relationship between the attachment to God and RSS will greatly contribute to elucidating points of “irresolvability” in the existential process that, given the burden of suffering, alienate people from the central dimension of human subjectivity and of existentiality itself: The spiritual dimension.
Due to the pandemic context (COVID-19) and the consequent social isolation, data were collected virtually. One of the great challenges in conducting online surveys is to achieve greater sample heterogeneity due to several factors that are involved, such as the fact that many people do not have access to technological resources. In this study, we were not able to achieve heterogeneity, and the sample is restricted to cisgender, white people, with an income between one and eight minimum wages and with high levels of education. We emphasize the need for new studies that present greater heterogeneity so that we can have a better understanding of the functioning of these variables among Brazilian sexual and gender minorities.
5. Conclusions
This study is one of the first developed in Brazil that outlines an overview of the spiritual/religious scenario of Brazilian sexual and gender minorities. The study points out that for many of the participants, religiosity is not a central dimension. However, more than one-third of the participants presented the dimension of religiosity as central to their lives and greater use of coping resources that resulted in some benefits, such as greater life satisfaction and a more secure attachment style.
Causal relationships between the variables were not traced in this study, but based on the literature, we hypothesized that the heterosexism present in many religious environments may be an obstacle for this population to access positive spiritual/religious resources. In the same sense, a high rate of RSS among this population was expected, which was not confirmed. Part of this group, for whom the religious system was not central, presented a high rate of avoidance in a relationship with a personal God, and low use of spiritual/religious resources. Religious deidentification is a process that caught our attention, given that it occurred due to prejudice suffered in religious spaces. The exclusion of religious socialization, especially in Christian spaces, has prevented a large part of this sample from fully experiencing the S/R dimension and enjoying the benefits that this dimension can confer. The index of struggles with meaning shows us that many of these people are facing a meaning crisis.
It is understood, therefore, that for this sample, the S/R dimension can be both a source of resources and a locus of suffering, hence the need for an assessment of the religious background of people who seek support in psychological clinics or in religious communities. It is essential to understand that, although the results demonstrate that processes of religious deidentification and religious transit are used by the sample as a resource to face struggles, there is a need to assess the presence of religious residues and how much they still affect the experiences of these people. Identifying whether these residues are beliefs that negatively affect the mental health of sexual and gender minorities is a process for health professionals and professionals who offer spiritual care.
This study did not survey the spiritual/religious path since childhood to verify the relationship between attachment to God and RSS. Future studies will be promising in this field and may contribute significantly to the expansion of the Attachment to God Theory itself, as well as bring subsidies to theology and other sciences with regard to the proposition of practices (religious or not) aimed at the spiritual development of the human being. Other studies may also perform a more accurate assessment of the prevalence of minority stress and assess whether the S/R dimension is a mediator that acts to improve the mental health outcomes of sexual and gender minorities. There is already a protocol validated in our country that is very consistent with the theory (
Costa et al. 2020).
A limitation of this study relates to the difficulties in assessing transgender people. Our sample primarily consisted of cisgender white people with a high level of education, which does not represent the majority of the Brazilian population. Hence, there is a need to develop new studies with a greater number and greater diversity of participants, seeking to understand the functioning of this dimension in the experiences of this population more effectively, and thus contributing to care practices that are sensitive to the needs of these people.
Finally, this study points to the need and relevance of addressing this issue in the most varied training courses that deal with the care of sexual and gender minorities. In particular, theology is urged to employ a process of theological-pastoral decolonization that involves abandoning heterosexist and homotransphobic attitudes that are supported by shallow and decontextualized readings of biblical texts. Regarding counseling and pastoral care, it is of fundamental importance that the people who will serve these groups seek adequate training, so that they can act in helping these people to cope with the suffering related to issues of affective-sexual and emotional orientation and/or gender identity, as well as in the process of self-acceptance, and work toward the integration of the spiritual/religious and sexual components of the counseled person’s identity. In addition, these professionals can also work with family members of people with affective-sexual orientations and minority gender identities, identifying the conflicts experienced by them and addressing the importance of welcoming and care.
Future studies could further investigate the prevalence of religious struggles in different faith communities in Brazil and the relationship between distal-proximal stressors (
Meyer 2003) and religious deidentification. In a religious country such as Brazil, such studies could contribute to both faith communities and public health issues to reduce discrimination, violence, and prejudice against sexual and gender minorities.







{kind=link}