Bioethics and Jainism: From Ahiṃsā to an Applied Ethics of Carefulness

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Bioethics and Religion
A Gap in the Field: A Lack of Jain Engagement in Medical Bioethics
3. Rare Accommodations for Medicine in the Early Canon through Practices of Carefulness
Four Tools of Carefulness
4. The Acceptance of Medicine in the Post-Canonical Period if Done Carefully
Carefulness versus “Intention”
The Jains argue ...that it is not possible for a person to be so ignorant and yet not guilty. His very ignorance and carelessness constitute an intent to do violence and imply correspondently his guilt. Only the Jain holy man, who has the right understanding and who is ever mindful of his acts, is truly devoid of the intention to commit violence.
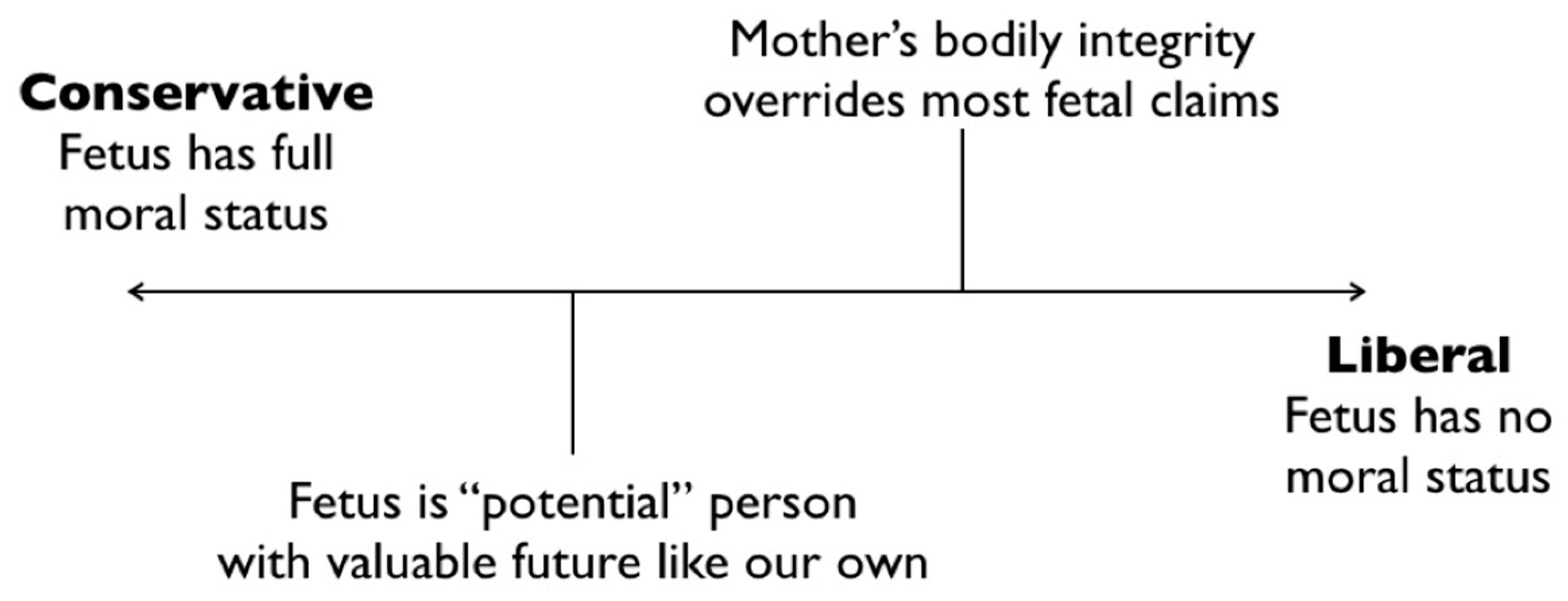
5. Reproductive Bioethics and a Jain Ethics of Carefulness
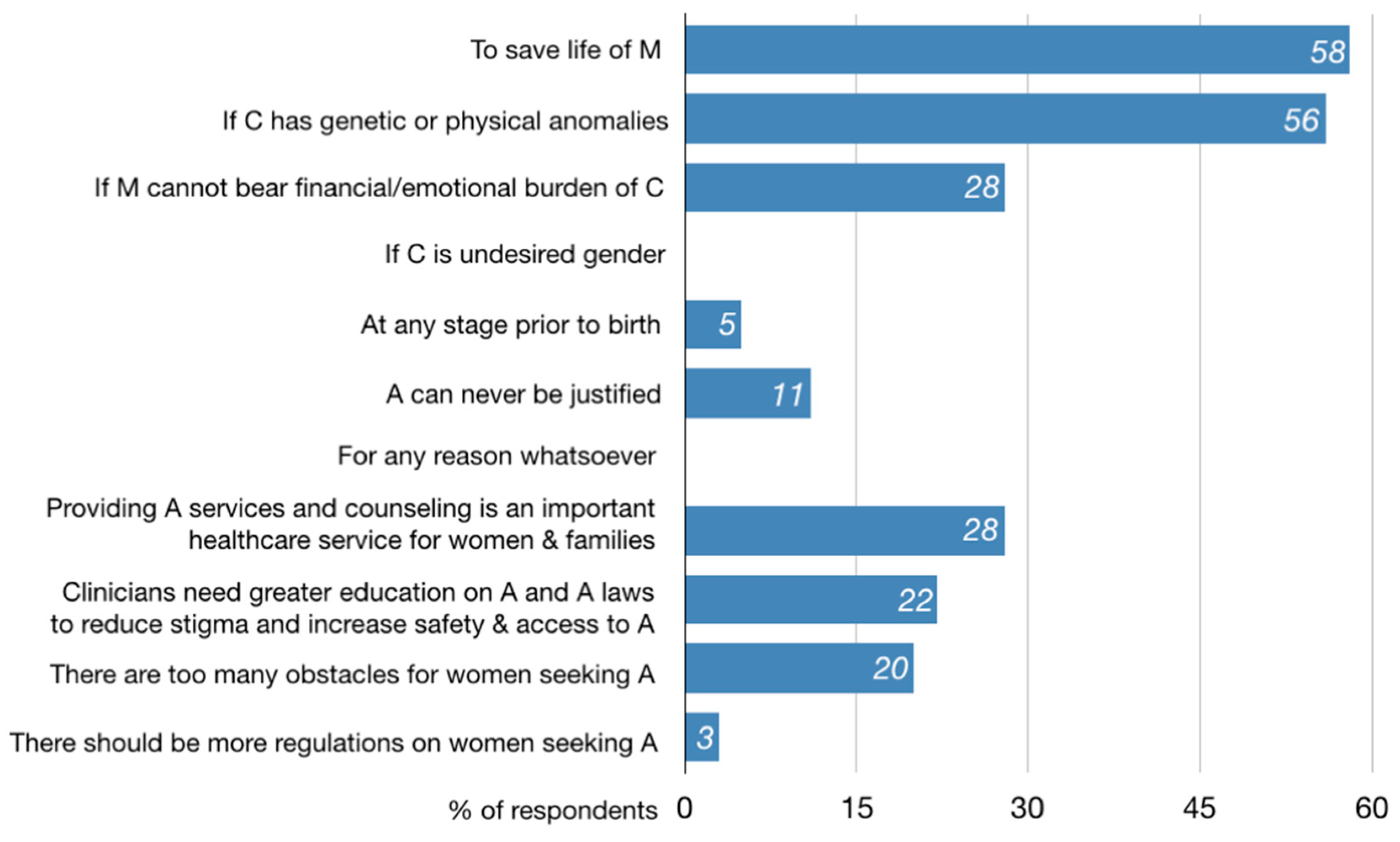
- “[It] depends on strong medical reason [such as the] mother’s health and her life”
- “[D]epends upon why abortion has to be done”
- “It is [a form of violence], but it needs to be taken on a case by case basis”
- “[I]f you are saving the life of the mother it should be okay. I would rather discourage the need for abortion.”
6. Conclusions
Funding
Conflicts of Interest
References
Primary Sources
ĀS [Ācārāṇga-sūtra]. 2008. Jaina Sutras, Part I & II. The Âkârâṅga Sûtra. Translated by Hermann Georg Jacobi. Forgotten Books. First published 1884.BhS [Bhagavatī-sūtra]. 1973. Bhagavati Sutra. Translated by K. C. Lalwani. Calcutta: Jain Bhavan.KS [Kalpa-sūtra]. 2008. Jaina Sutras, Part I & II. The Kalpa Sûtra. Translated by Hermann Georg Jacobi. Forgotten Books. First published 1884.PS [Pravacanasāra]. 1984. Śrῑ Kundakundācārya’s Pravacanasāra (Pavayaṇasāra). Translated by A. N. Upadhye. Agas: Parama-Śruta-Prabhāvaka Mandal, Shrimad Rajachandra Ashrama.SKS [Sūtrakṛtāṅga-sūtra]. Jaina Sutras, Part I & II. Sûtrakritâṅga. Translated by Hermann Georg Jacobi. Forgotten Books. First published 1884.Sth [Sthānāṅga-sūtra]. 2004. Illustrated Sthananga Sutra. Vol. 1. Translated by Surendra Bothra. Delhi: Padma Prakashan.TS [Tattvārtha-sūtra]. 2011. That Which Is. Translated by Nathmal Tatia. New Haven, CT: Yale University Press.US [Uttarādhyayana-sūtra]. 2008. Jaina Sutras, Part I & II. Uttarâdyayana. Translated by Hermann Georg Jacobi. Forgotten Books. First published 1884.YŚ [Yoga-Śastra]. 1989. The Yoga Shastra of Hemchandracharya. Translated by A. S. Gopani. A.S. Jaipur: Prakrit Bharti Academy. http://www.prakritbharati.net/books-online/yoga-shastra-hemachandracharya/000-00-table-contents/.Secondary Sources
- ART Success Rate. 2016. Centers for Disease Control and Prevention. Available online: https://www.cdc.gov/art/artdata/index.html (accessed on 16 May 2018).
- Auckland, Knut. 2016. The Scientization and Academization of Jainism. Journal of the American Academy of Religion 84: 192–233. [Google Scholar] [CrossRef]
- Banks, Marcus. 1991. Orthodoxy and Dissent: Varieties of Religious Belief among Immigrant Gujarati Jains in Britain. In The Assembly of Listeners: Jains in Society. Edited by Michael Carrithers and Caroline Hmphrey. New York: Cambridge University Press, pp. 241–60. [Google Scholar]
- Bhargava, Dayanand. 1968. Jaina Ethics. Delhi: Motilal Banarsidass. [Google Scholar]
- Bobra, Dilip K. 2008. Bio Medical Ethics in Jainism. Available online: http://www.herenow4u.net/index.php?id=66653 (accessed on 30 July 2015).
- Buswell, Robert E., and Donald S. Lopez Jr. 2014. The Princeton Dictionary of Buddhism. Princeton: Princeton University Press. [Google Scholar]
- Cahill, Lisa Sowle. 2006. Theology’s Role in Public Bioethics. In Handbook of Bioethics and Religion. Edited by David E. Guinn. Oxford: Oxford University Press, pp. 37–60. [Google Scholar]
- Caillat, Colette. 2018. On the Medical Doctrines in the Tandulaveyāliya: 1. Teachings of Embryology. Translated by Brianne Donaldson. International Journal of Jaina Studies 14: 1–14. [Google Scholar]
- Caring for the Jain Patient. n.d. Ashford Peters Health System. Available online: https://www.ashfordstpeters.info/images/other/PAS08.pdf (accessed on 1 November 2018).
- Chapple, Christopher Key. 2002. Jainism and Ecology: Nonviolence in the Web of Life. Cambridge: Harvard University Press. [Google Scholar]
- Cort, John. 2002. Green Jainism? Notes and Queries toward a Possible Jain Environmental Ethic. In Jainism and Ecology: Nonviolence in the Web of Life. Edited by Christopher Key Chapple. Cambridge: Harvard University Press, pp. 63–94. [Google Scholar]
- Deo, S. B. 1954. The History of Jaina Monachism from Inscriptions and Literature. Bulletin of the Deccan College Research Institute 16: 1–137. [Google Scholar]
- Donaldson, Brianne, and Ana Bajželj. 2019. Insistent Life: Foundations for Bioethics in Jainism, Lexington Books: forthcoming.
- Dundas, Paul. 2002. The Limits of a Jain Environmental Ethic. In Jainism and Ecology: Nonviolence in the Web of Life. Edited by Christopher Key Chapple. Cambridge: Harvard University Press, pp. 95–118. [Google Scholar]
- Evans, John H. 2006. Who Legitimately Speaks for Religion in Public Bioethics. In Handbook of Bioethics and Religion. Edited by David E. Guinn. Oxford: Oxford University Press, pp. 61–80. [Google Scholar]
- Glasenapp, Helmuth von. 1942. Doctrine of Karman in Jain Philosophy. Translated by G. Barry Gifford. Bombay: Bai Vijibai Jivanlal Panalal Charity Fund. [Google Scholar]
- Granoff, Phyllis. 1992. The Violence of Non-Violence: A Study of Some Jain Responses to Non-Jain Religious Practices. The Journal of the International Association of Buddhist Studies 15: 1–43. [Google Scholar]
- Granoff, Phyllis. 1998a. Cures and Karma: Attitudes Towards Healing in Medieval Jainism. In Self, soul and Body in Religious Experience. Edited by Albert I. Baumgarten. Leiden: Brill, pp. 218–56. [Google Scholar]
- Granoff, Phyllis. 1998b. Cures and Karma II: Some Miraculous Healings in the Indian Buddhist Story Tradition. Bulletin de l’Ecole Francaise d’Extrême-Orient 85: 285–304. [Google Scholar] [CrossRef]
- Granoff, Phyllis. 2013. Between Monk and Layman: Paścātkṛta and the Care of the Sick in Jain Monastic Rules. In Buddhist and Jaina Studies: Proceedings of the Conference in Lumbini. Lumbini: Lumbini International Research Institute, pp. 229–53. [Google Scholar]
- Guidelines for Health Care Providers Interacting with Patients of the Jain Religion and Their Families. n.d. Metropolitan Chicago Healthcare Council. Available online: https://www.kyha.com/assets/docs/PreparednessDocs/cg-jain.pdf (accessed on 1 November 2018).
- Jain, Jyoti Prasad. 1950. Ugrāditya’s Kalyāṇakāraka and Ramagiri. Proceedings of the Indian History Congress 13: 127–33. [Google Scholar]
- Jain, Pankaj. 2010. Jainism, Dharma, and Environmental Ethics. Union Seminary Quarterly Review 63: 121–35. [Google Scholar]
- Jaini, Padmanabh S. 2010. Collected Papers on Jaina Studies. Delhi: Motilal Banarsidass. [Google Scholar]
- Kelting, M. Whitney. 2009. Heroic Wives: Rituals, Stories, and the Virtues of Jain Wifehood. Cambridge: Oxford University Press. [Google Scholar]
- King, Richard. 1999. Orientalism and Religion: Postcolonial Theory, India, and ‘The Mystic East’. New York: Routledge. [Google Scholar]
- Kulkarni, Aniket D. 2013. Fertility treatments and multiple births. New England Journal of Medicine 369: 2218–25. [Google Scholar] [CrossRef] [PubMed]
- Laidlaw, James. 1995. Riches and Renunciation: Religion, Economy, and Society among the Jains. Oxford: Clarendon Press. [Google Scholar]
- Long, Jeffery. 2009. Jainism: An Introduction. New York: I. B. Tauris. [Google Scholar]
- Patel, Vibhuti. 2014. Sex Determination and Sex Pre-Selection Tests in India. In Global Bioethics and Human Rights: Contemporary Issues. Edited by Wanda Teays, John-Steward Gordon, Alison Dundes and Renteln. Lanham: Rowman and Littlefield, pp. 242–47. [Google Scholar]
- Patil, Dhanashri, Nitin Patel, Darshan Babu N., Umapati C. Baragi, and Gouda H. Pampanna. 2015. Kalyanakarakam: A Gem of Ayurveda. Ayushdhara 2: 141–49. [Google Scholar]
- Qvarnström, Olle. 2000. Stability and Adaptability: A Jain Strategy for Survival and Growth. In Jain Doctrine and Practice: Academic Perspectives. Edited by Joseph T. O’Connell. Toronto: University of Toronto, pp. 113–35. [Google Scholar]
- Rankin, Aidan. 2018. Jainism and Environmental Philosophy: Karma and Web of Life. New York: Routledge. [Google Scholar]
- Saddhatissa, Hammalawa. 1997. Buddhist Ethics. Somerville: Wisdom Publications. [Google Scholar]
- Sarma, Deepak. 2013. Jain Bioethics: Pontiff Charukeerthi Bhattaraka Sri Swamiji [Interview]. YouTube. Available online: https://www.youtube.com/watch?v=-h-5tTX9R14 (accessed on 5 April 2013).
- SC Stays Rajasthan [High Court] Verdict Declaring Santhara Illegal. 2016. The Hindu. March 29. Available online: https://www.thehindu.com/news/national/sc-stays-rajasthan-hc-verdict-declaring-santhara-illegal/article7599349.ece (accessed on 18 March 2019).
- Schubring, Walther. 2000. The Doctrine of the Jainas: Described after the Old Sources. Delhi: Motilal Banarsidass. First published 1962. [Google Scholar]
- Sethi, Manisha. 2012. Escaping the World: Women Renouncers among Jains. New York: Routledge. [Google Scholar]
- Sethia, Tara, ed. 2004. Ahiṃsā, Anekānta and Jainism. Delhi: Motilal Banarsidass. [Google Scholar]
- Shah, Bindi V. 2014. Religion in the Everyday Lives of Second-Generation Jains in Britain and the USA: Resources Offered by a Dharma-Based South Asian Religion for the Construction of Religious Biographies, and Negotiating Risk and Uncertainty in Late Modern Societies. The Sociological Review 62: 512–29. [Google Scholar] [CrossRef]
- Sherwin, Susan. 2011. Feminist Ethics and In Vitro Fertilization. In Biomedical Ethics. Edited by David DeGrazia, Thomas A. Mappes and Jeffrey Brand-Ballard. New York: McGraw Hill, pp. 553–59. [Google Scholar]
- Singhvi, Laxmi Mall. 2002. The Jain Declaration on Nature. In Jainism and Ecology: Nonviolence in the Web of Life. Edited by Christopher Key Chapple. Cambridge: Harvard University Press, pp. 217–24. [Google Scholar]
- Stuart, Mari Jyväsjärvi. 2014. Mendicants and Medicine: Āyurveda in Jain Monastic Texts. History of Science in South Asia 2: 63–100. [Google Scholar] [CrossRef]
- Vallely, Anne. 2002. From Liberation to Ecology: Ethical Discourses among Orthodox and Diaspora Jains. In Jainism and Ecology: Nonviolence in the Web of Life. Edited by Christopher Key Chapple. Cambridge: Harvard University Press, pp. 193–216. [Google Scholar]
- Wiles, Royce. 2006. The Dating of the Jaina Councils: Do Scholarly Presentations Reflect the Traditional Sources? In Studies in Jaina History and Culture: Disputes and Dialogues. Edited by Peter Flügel. New York: Routledge, pp. 61–86. [Google Scholar]
- Wiley, Kristi. 2009. The A to Z of Jainism. Lanham: The Scarecrow Press, Inc. [Google Scholar]
- Williams, Robert. 1991. Jaina Yoga: A Survey of the Mediaeval Śrāvakācāras. Delhi: Motilal Banarsidass. [Google Scholar]
- Zysk, Kenneth. 1998. Asceticism and Healing in Ancient India: Medicine in the Buddhist Monastery. Delhi: Motilal Banarsidass. [Google Scholar]
| 1 | 1 The National Commission for the Protection of Human Subjects of Biomedical and Behavioral Research (1974–78) is generally viewed as the first national bioethics commission; it issued the foundational Belmont Report for consent in human subjects research; The Presidential Commission for the Study of Ethical Problems in Medicine and Biomedical and Behavioral Research (1978–83) produced studies on foregoing life-sustaining treatment, and access to health care, among other topics. The 1981 report Defining Death was the basis of the Uniform Determination of Death Act, a model law that was enacted by most U.S. states. |
| 2 | See, for example Paul Ramsey, The Patient as Person: Explorations in Medical Ethics (Yale University Press 1977), Richard McCormick, How Brave a New World? Dilemmas in Bioethics (Georgetown University Press 1985) and Immanuel Jakobovits, Jewish Medical Ethics (Bloch Publishing Co. 1959/1975). |
| 3 | Tīrthaṅkaras are also called Jinas, meaning “victors,” who show the pathway of perception, knowledge, and action toward mokṣa; the name “Jain” derives from this latter term. |
| 4 | The dates of Mahāvīra’s birth and death vary; Śvetāmbara sources estimate 599-527 BCE; however Digambara sources believe Mahāvīra died in 510 BCE. More recently, scholars have adjusted the dates approximately 100 years later to coincide with the Buddha’s revised dating, i.e., 499-427 BCE (Dundas 2002, p. 24). |
| 5 | This mutuality, however, does not erase the differences. The Sūtrakṛtāṇga-sūtra states plainly that “householders are killers (of beings) and acquirers of property…They themselves kill movable and immovable living beings, have them killed by another person, or consent to another’s killing them” (SKS 2.1.43). |
| 6 | I served on the steering committee for the 2012 International Jain Bioethics Conference (24–25 August 2012), in Claremont, California, see Dilip Shah, “First Ever International Jain Bioethics Conference,” Institute of Jainology, https://www.jainology.org/jain-bioethics-conference/. See also, the 2017 National Seminar: Engaging Jainism With Modern Issues (24–26 February 2017) at Jain Vishva Bharati Institute, Ladnun (summary available at “BMIRC National Seminar” at HereNow4U, http://www.herenow4u.net/index.php?id=123357). |
| 7 | The Gyan Sagar Science Foundation (GSSF), for example, was started in 2009 by 41 founding Jain scientists in India for the purposes of “bridging science and society” (“Gyan Sagar” at HereNow4U, http://www.herenow4u.net/index.php?id=110933). In addition to a hosting annual conferences, GSSF has published a journal with relevant articles, and also co-sponsored the 18th Jaina Studies Workshop on Jainism and Science (2016) at the School of Oriental and Asian Studies (SOAS) in London. |
| 8 | For two examples of such healthcare guidelines in the U.K. and U.S., see (Caring for the Jain Patient n.d.) and (Guidelines for Health Care Providers Interacting with Patients of the Jain Religion and Their Families n.d.). |
| 9 | Anekāntavāda also describes the superior knowledge of the Tīrthaṅkaras who, having shed all deluding karma, possesses perfect perception of all contradictory truths in unison (SKS 1.6.28). |
| 10 | Banks describes the “neo-orthodox” tendency, alongside orthodox and heterodox tendencies, not as fixed groups but rather as three categories of informal belief that can overlap and shift within a given person (Banks 1991, pp. 244–57). |
| 11 | For details on alternate dates for this Council, see Royce Wiles (2006). |
| 12 | Deo identifies the acceptance of medicine within post-canonical commentaries on the Mūla-sūtras, referring to four “root texts” mendicants used at the start of their vocation (Deo 1954, pp. 29–33); Stuart examines three post-canonical commentaries: Niśītha-bhāṣya, Vyavahāra-bhāṣya, and Bṛhatkalpa-bhāṣya (6th–7th-century CE). |
| 13 | A small sampling of verses that reference the desires of mind, speech, and body include ĀS I.1.7.6, I.5.1.1–3, I.5.3.4, I.5.4.5, I.6.5.3–5. |
| 14 | A small sampling of verses that reference direct, indirect, and approved of harms include ĀS I.1.1.5, I.1.2.3, I.1.5.7, I.1.6.6, I.1.7.3, I.2.5.2, I.3.2.3. |
| 15 | evaṃ se appamāeṇa vivegaṃ keṭṭati veyavī. |
| 16 | |
| 17 | Williams provides the Śvetāmbara list in a hierarchy of desirability as: trade, practice of medicine, agriculture, artisanal crafts, animal husbandry, service of a ruler, and begging. The Digambara list includes: trade, clerical occupations, agriculture, artisanal crafts, and military occupations (Williams 1991, p. 122). |
| 18 | Samiti is a -ti suffix noun formed from the prefix sam + verbal root √i (to go, come, continue, etc.), often referring to a “coming together” such as an association, council, group, etc. However, in the Jain tradition samiti refers to a series of five supportive rules that mendicants strive to adhere to as a supplement to the five “great vows” taken at ordination (mahā-vratas). Akin to apramatta, samiti vows require extreme care in: (1) walking (i), (2) speaking (bhāṣā-samiti), (3) accepting alms (eṣaṇā-samiti), (4) picking items up and setting items down (ādāna-nikṣepaṇa-samiti), and (5) performing excretory functions (utsarga-samiti). |
| 19 | The 13th and 14th stages describe the shedding of all karma, the full actualization of the jīva’s qualities. In a small twist of Jain cosmology, no liberation is actually possible in our current time cycle until the balance of ignorance and knowledge is regained so that moral decision is possible, which is estimated to be about 80,000 more years (Schubring [1962] 2000, pp. 225–26). |
| 20 | The authorship of the Śrāvaka-prajñāpti is uncertain; it was perhaps written by Umāsvāti or others (Williams 1991, p. 3). |
| 21 | The National Health Portal of India offers a hospital directory database at https://www.nhp.gov.in/directoryservices/hospitals. The number of Jain-sponsored hospitals was calculated by searching this directory using the keywords “Jain,” “Jaina,” “Mahavir” (including alternate spellings), and “Parshva(natha)” (including alternate spellings), arriving at a total of 213 facilities, though there are likely hospitals with Jain affiliations that were not included in this count. |
| 22 | 22 This history of IVF begins in the late 1800s with animal models in Europe. The first successful human procedure was completed by Patrick Steptoe and Robert Edwards when baby Louise Brown was born in the U.K. in 1978. |
| 23 | Sethi also describes commonalities that Jain nuns share in common with lay women, such as “male dominance, vulnerability to sexual and physical violence and so on” (Sethi 2012, p. 39). Sethi’s research describes how renunciation is still portrayed as an essential male pursuit, in spite of its recognition that women are equal participants in the Jain community and spiritual vision (p. 64). |
| 24 | 24 Based on CDC’s 2016 Fertility Clinic Success Rates Report, there were 263,577 ART cycles performed at 463 reporting clinics in the United States during 2016, resulting in 65,996 live births (deliveries of one or more living infants) and 76,930 live born infants. See ART Success Rate (2016). |
| 25 | While some countries permit only two embryos to be transferred during IVF—Canada, U.K., Australia, and New Zealand—The U.S. has no transfer limit. But after an increase in multi-fetal pregnancies through the 80s and late 90s, US medical associations offered a recommended limit rather than prohibition on transfers of 3 or more embryos which has reduced overall numbers. Still, twins or triplets increase the entanglement with children and resources. |
© 2019 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Donaldson, B. Bioethics and Jainism: From Ahiṃsā to an Applied Ethics of Carefulness. Religions 2019, 10, 243. https://doi.org/10.3390/rel10040243
Donaldson B. Bioethics and Jainism: From Ahiṃsā to an Applied Ethics of Carefulness. Religions. 2019; 10(4):243. https://doi.org/10.3390/rel10040243
Chicago/Turabian StyleDonaldson, Brianne. 2019. "Bioethics and Jainism: From Ahiṃsā to an Applied Ethics of Carefulness" Religions 10, no. 4: 243. https://doi.org/10.3390/rel10040243
APA StyleDonaldson, B. (2019). Bioethics and Jainism: From Ahiṃsā to an Applied Ethics of Carefulness. Religions, 10(4), 243. https://doi.org/10.3390/rel10040243