The Effects of Erector Spinae Plane Block in Terms of Postoperative Analgesia in Patients Undergoing Laparoscopic Cholecystectomy: A Meta-Analysis of Randomized Controlled Trials


Abstract
1. Introduction
2. Materials and Methods
2.1. Protocol and Registration
2.2. Eligibility Criteria
2.3. Sources and Search
2.4. Study Selection, Data Collection Process, and Data Items
2.5. Risk of Bias in Individual Studies
2.6. Summary Measures and Synthesis of Results
3. Results
3.1. Study Selection
3.2. Risk of Bias
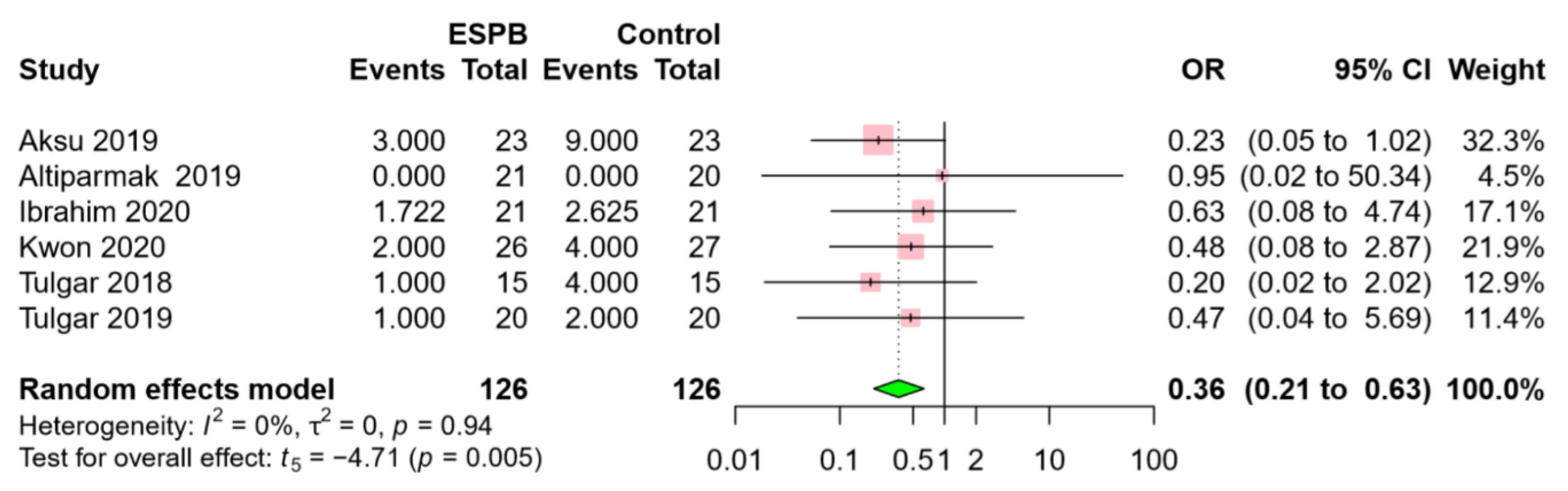
3.3. Erector Spinae Plane Block vs. Control
3.4. Erector Spinae Plane Block vs. Oblique Subcostal Transversus Abdominis Plane Block
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Cullen, K.A.; Hall, M.J.; Golosinskiy, A. Ambulatory surgery in the United States, 2006. In National Health Statistics Reports; United States Department of Health and Human Services: Washington, DC, USA, 2009; pp. 1–25. [Google Scholar]
- Barczynski, M.; Herman, R.M. A prospective randomized trial on comparison of low-pressure (LP) and standard-pressure (SP) pneumoperitoneum for laparoscopic cholecystectomy. Surg. Endosc. 2003, 17, 533–538. [Google Scholar] [CrossRef] [PubMed]
- Mitra, S.; Khandelwal, P.; Roberts, K.; Kumar, S.; Vadivelu, N. Pain relief in laparoscopic cholecystectomy—A review of the current options. Pain Pract. 2012, 12, 485–496. [Google Scholar] [CrossRef] [PubMed]
- Forero, M.; Adhikary, S.D.; Lopez, H.; Tsui, C.; Chin, K.J. The Erector Spinae Plane Block: A Novel Analgesic Technique in Thoracic Neuropathic Pain. Reg. Anesth. Pain Med. 2016, 41, 621–627. [Google Scholar] [CrossRef] [PubMed]
- Grocott, H.P. Erector Spinae Plane Block for Postoperative Analgesia: A Magic Bullet Too Good to Be True, or Is It Just Too Soon to Tell? Anesth. Analg. 2020, 130, e29. [Google Scholar] [CrossRef] [PubMed]
- Huang, J.; Liu, J.C. Ultrasound-guided erector spinae plane block for postoperative analgesia: A meta-analysis of randomized controlled trials. BMC Anesthesiol. 2020, 20, 83. [Google Scholar] [CrossRef]
- Kendall, M.C.; Alves, L.; Traill, L.L.; De Oliveira, G.S. The effect of ultrasound-guided erector spinae plane block on postsurgical pain: A meta-analysis of randomized controlled trials. BMC Anesthesiol. 2020, 20, 99. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; The PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. J. Clin. Epidemiol. 2009, 62, 1006–1012. [Google Scholar] [CrossRef]
- Higgins, J.P.; Altman, D.G.; Gotzsche, P.C.; Juni, P.; Moher, D.; Oxman, A.D.; Savovic, J.; Schulz, K.F.; Weeks, L.; Sterne, J.A. The Cochrane Collaboration’s tool for assessing risk of bias in randomised trials. BMJ 2011, 343, d5928. [Google Scholar] [CrossRef]
- R Core Team. A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria; Available online: https://www.R-project.org (accessed on 11 July 2020).
- Schwarzer, G. Meta: An R package for meta-analysis. R News 2007, 7, 40–45. [Google Scholar]
- Wan, X.; Wang, W.; Liu, J.; Tong, T. Estimating the sample mean and standard deviation from the sample size, median, range and/or interquartile range. BMC Med. Res. Methodol. 2014, 14, 135. [Google Scholar] [CrossRef]
- Robert, N.; Wong, G.W.; Wright, J.M. Effect of cyclosporine on blood pressure. Cochrane Database Syst. Rev. 2010, CD007893. [Google Scholar] [CrossRef] [PubMed]
- Friedrich, J.O.; Adhikari, N.K.; Beyene, J. Inclusion of zero total event trials in meta-analyses maintains analytic consistency and incorporates all available data. BMC Med. Res. Methodol. 2007, 7, 5. [Google Scholar] [CrossRef] [PubMed]
- IntHout, J.; Ioannidis, J.P.A.; Borm, G.F. The Hartung-Knapp-Sidik-Jonkman method for random effects meta-analysis is straightforward and considerably outperforms the standard DerSimonian-Laird method. BMC Med. Res. Methodol. 2014, 14, 25. [Google Scholar] [CrossRef] [PubMed]
- Aksu, C.; Kus, A.; Yorukoglu, H.U.; Kilic, C.T.; Gurkan, Y. The effect of erector spinae plane block on postoperative pain following laparoscopic cholecystectomy: A randomized controlled study. Anestezi Dergisi 2019, 27, 9–14. [Google Scholar] [CrossRef]
- Altiparmak, B.; Toker, M.K.; Uysal, A.İ.; Kuşçu, Y.; Demirbilek, S.G. Efficacy of ultrasound-guided erector spinae plane block for analgesia after laparoscopic cholecystectomy: A randomized controlled trial. Braz. J. Anesthesiol. 2019, 69, 561–568. [Google Scholar] [CrossRef]
- Altıparmak, B.; Korkmaz Toker, M.; Uysal, A.I.; Kuşçu, Y.; Gümüş Demirbilek, S. Ultrasound-guided erector spinae plane block versus oblique subcostal transversus abdominis plane block for postoperative analgesia of adult patients undergoing laparoscopic cholecystectomy: Randomized, controlled trial. J. Clin. Anesth. 2019, 57, 31–36. [Google Scholar] [CrossRef]
- Ibrahim, M. Erector spinae plane block in laparoscopic cholecystectomy, is there a difference? A randomized controlled trial. Anesth. Essays Res. 2020. (Epub ahead of print). [Google Scholar] [CrossRef]
- Kwon, H.M.; Kim, D.H.; Jeong, S.M.; Choi, K.T.; Park, S.; Kwon, H.J.; Lee, J.H. Does Erector Spinae Plane Block Have a Visceral Analgesic Effect?: A Randomized Controlled Trial. Sci. Rep. 2020, 10, 8389. [Google Scholar] [CrossRef]
- Peker, K.; Akçaboy, Z.N.; Aydın, G.; Gençay, I.; Şahin, A.T.; Koçak, Y.F.; Peker, S.A. The Effect of Erector Spinae Plane Block on Laparoscopic Cholecystectomy Anesthesia: Analysis of Opioid Consumption, Sevoflurane Consumption, and Cost. J. Laparoendosc. Adv. S. 2020, 30, 725–729. [Google Scholar] [CrossRef]
- Tulgar, S.; Kapakli, M.S.; Senturk, O.; Selvi, O.; Serifsoy, T.E.; Ozer, Z. Evaluation of ultrasound-guided erector spinae plane block for postoperative analgesia in laparoscopic cholecystectomy: A prospective, randomized, controlled clinical trial. J. Clin. Anesth. 2018, 49, 101–106. [Google Scholar] [CrossRef]
- Tulgar, S.; Kapakli, M.S.; Kose, H.C.; Senturk, O.; Selvi, O.; Serifsoy, T.E.; Thomas, D.T.; Ozer, Z. Evaluation of Ultrasound-Guided Erector Spinae Plane Block and Oblique Subcostal Transversus Abdominis Plane Block in Laparoscopic Cholecystectomy: Randomized, Controlled, Prospective Study. Anesth. Essays Res. 2019, 13, 50–56. [Google Scholar] [CrossRef] [PubMed]
- Ng, K.F.; Tsui, S.L.; Yang, J.C.; Ho, E.T. Increased nausea and dizziness when using tramadol for post-operative patient-controlled analgesia (PCA) compared with morphine after intraoperative loading with morphine. Eur. J. Anaesthesiol. 1998, 15, 565–570. [Google Scholar] [CrossRef] [PubMed]
- Shaheen, P.E.; Walsh, D.; Lasheen, W.; Davis, M.P.; Lagman, R.L. Opioid equianalgesic tables: Are they all equally dangerous? J. Pain Symptom Manag. 2009, 38, 409–417. [Google Scholar] [CrossRef] [PubMed]
- Cai, Q.; Liu, G.Q.; Huang, L.S.; Yang, Z.X.; Gao, M.L.; Jing, R.; Liu, Z.; Pan, L.H. Effects of erector spinae plane block on postoperative pain and side-effects in adult patients underwent surgery: A systematic review and meta-analysis of randomized controlled trials. Int. J. Surg. 2020, 80, 107–116. [Google Scholar] [CrossRef]
- Shafi, S.; Collinsworth, A.W.; Copeland, L.A.; Ogola, G.O.; Qiu, T.; Kouznetsova, M.; Liao, I.C.; Mears, N.; Pham, A.T.; Wan, G.J.; et al. Association of Opioid-Related Adverse Drug Events With Clinical and Cost Outcomes Among Surgical Patients in a Large Integrated Health Care Delivery System. JAMA Surg. 2018, 153, 757–763. [Google Scholar] [CrossRef]
- Kumar, K.; Kirksey, M.A.; Duong, S.; Wu, C.L. A Review of Opioid-Sparing Modalities in Perioperative Pain Management: Methods to Decrease Opioid Use Postoperatively. Anesth. Analg. 2017, 125, 1749–1760. [Google Scholar] [CrossRef]
- Fregoso, G.; Wang, A.; Tseng, K.; Wang, J. Transition from Acute to Chronic Pain: Evaluating Risk for Chronic Postsurgical Pain. Pain Phys. 2019, 22, 479–488. [Google Scholar]
- Blichfeldt-Eckhardt, M.R.; Ording, H.; Andersen, C.; Licht, P.B.; Toft, P. Early visceral pain predicts chronic pain after laparoscopic cholecystectomy. Pain 2014, 155, 2400–2407. [Google Scholar] [CrossRef]
- Gan, T.J.; Diemunsch, P.; Habib, A.S.; Kovac, A.; Kranke, P.; Meyer, T.A.; Watcha, M.; Chung, F.; Angus, S.; Apfel, C.C.; et al. Consensus guidelines for the management of postoperative nausea and vomiting. Anesth. Analg. 2014, 118, 85–113. [Google Scholar] [CrossRef]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study | Sample Size | Local Anesthetics | Level | PCA Regimen | ||
|---|---|---|---|---|---|---|
| ESPB | Control | OSTAP | Bolus–Infusion–Lockout | |||
| Aksu 2019 [16] | 23 | 23 | 0.25% BUPI 20 mL | T8 | MP, 1–6 mg/hr–8 min | |
| Altiparmak 2019 (1) [17] | 21 | 20 | 0.375% BUPI 20 mL × 2 | T7 | TMD, 10 mg–0–20 min | |
| Altiparmak 2019 (2) [18] | 34 | 34 | 0.25% BUPI 20 mL × 2 | T7 | TMD, 20 mg–0–15 min | |
| Ibrahim 2020 [19] | 21 | 21 | 21 | 0.25% BUPI 20 mL × 2 | T8 | MP, 1 mg–0–12 min |
| Kwon 2020 [20] | 26 | 27 | 0.20% ROPI 20 mL × 2 | T7 | - | |
| Peker 2020 [21] | 39 | 42 | 0.25% BUPI 20 mL × 2 | T7 | - | |
| Tulgar 2018 [22] | 15 | 15 | 0.375% BUPI 20 mL × 2 | T9 | TMD, 10 mg–0–20 min | |
| Tulgar 2019 [23] | 20 | 20 | 20 | 0.5% BUPI 20 mL + 2% LDC 10 mL+ NS 10 mL | T9 | TMD, 10 mg–0–20 min |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Koo, C.-H.; Hwang, J.-Y.; Shin, H.-J.; Ryu, J.-H. The Effects of Erector Spinae Plane Block in Terms of Postoperative Analgesia in Patients Undergoing Laparoscopic Cholecystectomy: A Meta-Analysis of Randomized Controlled Trials. J. Clin. Med. 2020, 9, 2928. https://doi.org/10.3390/jcm9092928
Koo C-H, Hwang J-Y, Shin H-J, Ryu J-H. The Effects of Erector Spinae Plane Block in Terms of Postoperative Analgesia in Patients Undergoing Laparoscopic Cholecystectomy: A Meta-Analysis of Randomized Controlled Trials. Journal of Clinical Medicine. 2020; 9(9):2928. https://doi.org/10.3390/jcm9092928
Chicago/Turabian StyleKoo, Chang-Hoon, Jin-Young Hwang, Hyun-Jung Shin, and Jung-Hee Ryu. 2020. "The Effects of Erector Spinae Plane Block in Terms of Postoperative Analgesia in Patients Undergoing Laparoscopic Cholecystectomy: A Meta-Analysis of Randomized Controlled Trials" Journal of Clinical Medicine 9, no. 9: 2928. https://doi.org/10.3390/jcm9092928
APA StyleKoo, C.-H., Hwang, J.-Y., Shin, H.-J., & Ryu, J.-H. (2020). The Effects of Erector Spinae Plane Block in Terms of Postoperative Analgesia in Patients Undergoing Laparoscopic Cholecystectomy: A Meta-Analysis of Randomized Controlled Trials. Journal of Clinical Medicine, 9(9), 2928. https://doi.org/10.3390/jcm9092928