Association between Use of Hydrochlorothiazide and Nonmelanoma Skin Cancer: Common Data Model Cohort Study in Asian Population

 ,
,  ,
,  , ,
, ,
Abstract
1. Introduction
2. Experimental Section
2.1. Data Sources
2.2. Patient Selection
2.3. Outcomes and Other Covariates
2.4. Statistical Analysis
3. Results
3.1. Clinical Characteristics
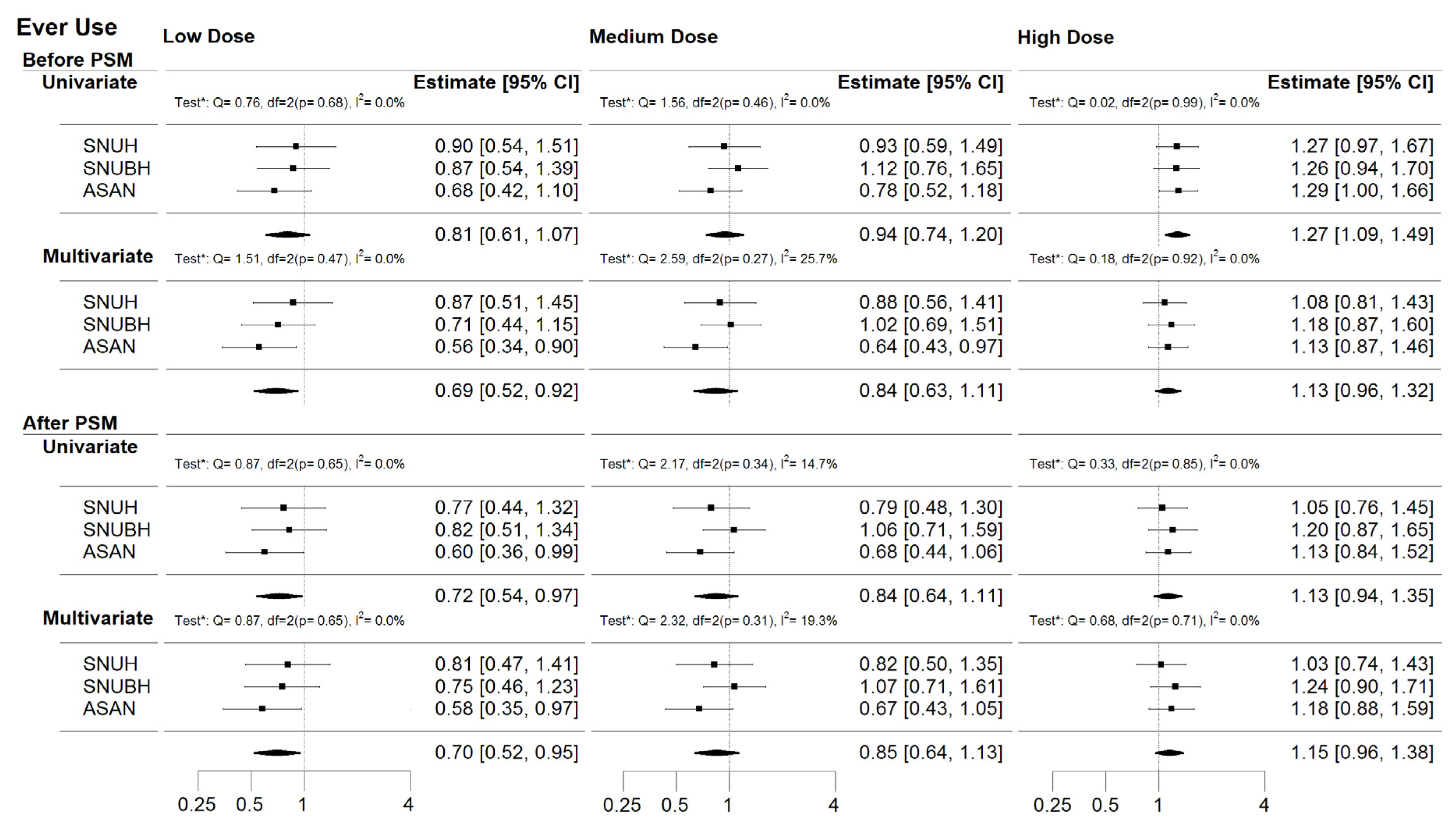
3.2. Risk of NMSC Associated with HCTZ Use
3.3. Additional Analyses
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Xie, X.; Atkins, E.; Lv, J.; Bennett, A.; Neal, B.; Ninomiya, T.; Woodward, M.; MacManon, S.; Turnbull, F.; Hillis, G.S.; et al. Effects of intensive blood pressure lowering on cardiovascular and renal outcomes: Updated systematic review and meta-analysis. Lancet 2016, 387, 435–443. [Google Scholar] [CrossRef]
- Gupta, R.; Xavier, D. Hypertension: The most important non communicable disease risk factor in India. Indian Heart J. 2018, 70, 565–572. [Google Scholar] [CrossRef] [PubMed]
- Whelton, P.K.; Carey, R.M.; Aronow, W.S.; Casey, N.E.; Collins, K.J.; Himmelfarb, C.R.D.; DePalma, S.M.; Gidding, S.; Jamerson, K.A.; Jones, D.W.; et al. 2017 ACC/AHA/AAPA/ABC/ACPM/AGS/APhA/ASH/ASPC/NMA/PCNA Guideline for the prevention, detection, evaluation, and management of high blood pressure in adults: A report of the American college of Cardiology/American heart association task force on clinical practice guidelines. Hypertension 2018, 71, e113–e115. [Google Scholar]
- Ritchey, M.D.; Gillespie, C.; Wozniak, G.; Shay, C.M.; Thompson-Paul, A.M.; Loustalot, F.; Hong, Y. Potential need for expanded pharmacologic treatment and lifestyle modification services under the 2017 ACC/AHA Hypertension Guideline. J. Clin. Hypertens. Greenwich 2018, 20, 1377–1391. [Google Scholar] [CrossRef] [PubMed]
- Hisamatsu, T. Control rates of systolic and diastolic blood pressure among hypertensive adults in Korea. Korean Circ. J. 2019, 49, 1049–1051. [Google Scholar] [CrossRef] [PubMed]
- Shin, J.; Cho, M.-C. Updated reasons and clinical implications of New Korean Hypertension Guidelines for cardiologists. Korean Circ. J. 2020, 50, 476–484. [Google Scholar] [CrossRef]
- Cheung, B.M.Y.; Or, B.; Fei, Y.; Tsoi, M.F. A 2020 vision of hypertension. Korean Circ. J. 2020, 50, 469–475. [Google Scholar] [CrossRef]
- Cho, S.M.J.; Lee, H.; Pyun, W.B.; Kim, H.C. Differential control rate of systolic and diastolic blood pressure among Korean adults with Hypertension: The sixth Korean national health and nutrition examination survey, 2013–2015 (KNHANES VI). Korean Circ. J. 2019, 49, 1035–1048. [Google Scholar] [CrossRef]
- Kwun, J.-S.; Kim, S.-H.; Kang, S.-H.; Yoon, C.-H.; Lee, H.-Y.; Kim, K.-I.; Youn, T.-J.; Chae, I.-H.; Kim, C.-H. Potential impact of 2018 Korean society of Hypertension guidelines on Korean population: A population-based cohort study. Clin. Hypertens. 2020, 26, 3–8. [Google Scholar] [CrossRef]
- Kim, H.C.; Ihm, S.-H.; Kim, G.-H.; Kim, J.H.; Kim, K.-I.; Lee, H.-Y.; Lee, J.H.; Park, J.-M.; Park, S.; Pyun, W.B.; et al. 2018 Korean Society of Hypertension guidelines for the management of hypertension: Part I-epidemiology of hypertension. Clin. Hypertens. 2019, 25, 1–16. [Google Scholar] [CrossRef]
- Kim, K.-I.; Ihm, S.-H.; Kim, G.-H.; Kim, H.C.; Kim, J.H.; Lee, H.-Y.; Lee, J.H.; Park, J.-M.; Park, S.; Pyun, W.B.; et al. 2018 Korean society of hypertension guidelines for the management of hypertension: Part III-hypertension in special situations. Clin. Hypertens. 2019, 25, 1–14. [Google Scholar] [CrossRef]
- Lee, H.-Y.; Shin, J.; Kim, G.-H.; Park, S.; Ihm, S.-H.; Kim, H.C.; Kim, K.-I.; Kim, J.H.; Lee, J.H.; Park, J.-M.; et al. 2018 Korean society of Hypertension guidelines for the management of hypertension: Part II-diagnosis and treatment of hypertension. Clin. Hypertens. 2019, 25, 20. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.R.; Alexander, G.C.; Stafford, R.S. Outpatient hypertension treatment, treatment intensification, and control in Western Europe and the United States. Arch. Intern. Med. 2007, 167, 141–147. [Google Scholar] [CrossRef] [PubMed]
- Pedersen, S.A.; Schmidt SA, J.; Hölmich, L.R.; Friis, S.; Pottegård, A.; Gaist, D. Hydrochlorothiazide use and risk for Merkel cell carcinoma and malignant adnexal skin tumors: A nationwide case-control study. J. Am. Acad. Dermatol. 2019, 80, 460–465. [Google Scholar] [CrossRef] [PubMed]
- Pedersen, S.A.; Gaist, D.; Schmidt, M.; Hölmich, L.R.; Friis, S.; Pottegård, A. Hydrochlorothiazide use and risk of nonmelanoma skin cancer: A nationwide case-control study from Denmark. J. Am. Acad. Dermatol. 2018, 78, 673–681. [Google Scholar] [CrossRef]
- Pottegård, A.; Pedersen, S.A.; Schmidt, S.A.J.; Hölmich, L.R.; Friis, S.; Gaist, D. Association of hydrochlorothiazide use and risk of malignant melanoma. JAMA Intern. Med. 2018, 178, 1120–1122. [Google Scholar] [CrossRef]
- Su, K.; Habel, L.; Achacoso, N.; Friedman, G.; Asgari, M.M. Photosensitizing antihypertensive drug use and risk of cutaneous squamous cell carcinoma. Br. J. Dermatol. 2018, 179, 1088–1094. [Google Scholar] [CrossRef]
- Gandini, S.; Palli, M.; Spadola, G.; Bendinelli, B.; Cocorocchio, E.; Stanganelli, I.; Miligi, L.; Masala, G.; Caini, S. Anti-hypertensive drugs and skin cancer risk: A review of the literature and meta-analysis. Crit. Rev. Oncol. Hematol. 2018, 122, 1–9. [Google Scholar] [CrossRef]
- Pottegaard, A.; Pedersen, S.A.; Schmidt, S.A.J.; Lee, C.-N.; Hsu, C.-K.; Liao, T.-C.; Shao, S.-C.; Lai, E.C.-C. Use of hydrochlorothiazide and risk of skin cancer: A nationwide Taiwanese case-control study. Br. J. Cancer 2019, 121, 973–978. [Google Scholar] [CrossRef]
- Oh, C.-M.; Cho, H.; Won, Y.-J.; Kong, H.-J.; Roh, Y.H.; Jeong, K.-H.; Jung, K.-W. Nationwide trends in the incidence of melanoma and non-melanoma skin cancers from 1999 to 2014 in South Korea. Cancer Res. Treat. 2018, 50, 729–737. [Google Scholar] [CrossRef]
- Kuoppala, J.; Lamminpää, A.; Pukkala, E. Statins and cancer: A systematic review and meta-analysis. Eur. J. Cancer 2008, 44, 2122–2132. [Google Scholar] [CrossRef] [PubMed]
- Reinau, D.; Surber, C.; Jick, S.S.; Meier, C.R. Nonsteroidal anti-inflammatory drugs and the risk of nonmelanoma skin cancer. Int. J. Cancer 2015, 137, 144–153. [Google Scholar] [CrossRef] [PubMed]
- Zhu, Y.; Cheng, Y.; Luo, R.-C.; Li, A.-M. Aspirin for the primary prevention of skin cancer: A meta-analysis. Oncol. Lett. 2015, 9, 1073–1080. [Google Scholar] [CrossRef] [PubMed]
- Thygesen, S.K.; Christiansen, C.F.; Christensen, S.; Lash, T.L.; Sørensen, H.T. The predictive value of ICD-10 diagnostic coding used to assess Charlson comorbidity index conditions in the population-based Danish National Registry of Patients. BMC Med. Res. Methodol. 2011, 11, 83. [Google Scholar] [CrossRef] [PubMed]
- Littnerova, S.; Jarkovsky, J.; Parenica, J.; Pavlik, T.; Spinar, J.; Dusek, L. Why to use propensity score in observational studies? Case study based on data from the Czech clinical database AHEAD 2006–2009. Cor. et Vasa. 2013, 55, e383–e390. [Google Scholar] [CrossRef]
- Huedo-Medina, T.B.; Sánchez-Meca, J.; Marín-Martínez, F.; Botella, J. Assessing heterogeneity in meta-analysis: Q statistic or I2 index? Psychol. Methods 2006, 11, 193–206. [Google Scholar] [CrossRef]
- Park, E.; Lee, Y.; Jue, M.-S. Hydrochlorothiazide use and the risk of skin cancer in patients with hypertensive disorder: A nationwide retrospective cohort study from Korea. Korean J. Intern. Med. 2019, 35, 906. [Google Scholar] [CrossRef]
- Kreutz, R.; AlGharably, E.A.H.; Douros, A. Reviewing the effects of thiazide and thiazide-like diuretics as photosensitizing drugs on the risk of skin cancer. J. Hypertens. 2019, 37, 1950–1958. [Google Scholar] [CrossRef]
- Hripcsak, G.; Duke, J.D.; Shah, N.H.; Reich, C.G.; Huser, V.; Schuemie, M.J.; A Suchard, M.; Park, R.W.; Wong, I.C.K.; Rijnbeek, P.R.; et al. Observational health data sciences and informatics (OHDSI): Opportunities for observational researchers. Stud. Health Technol. Inform. 2015, 216, 574–578. [Google Scholar]
- Platt, R.; Wilson, M.; Chan, K.A.; Benner, J.S.; Marchibroda, J.; McClellan, M. The new Sentinel Network--improving the evidence of medical-product safety. N. Engl. J. Med. 2009, 361, 645–647. [Google Scholar] [CrossRef]
- Shin, D.; Lee, E.S.; Kim, J.; Guerra, L.; Naik, D.; Prida, X. Association Between the use of thiazide diuretics and the risk of skin cancers: A meta-analysis of observational studies. J. Clin. Med. Res. 2019, 11, 247–255. [Google Scholar] [CrossRef] [PubMed]
- Humbert, X.; Dolladille, C.; Chrétien, B.; Sassier, M.; Fedrizzi, S.; Puddu, P.-E.; Alexandre, J. Thiazides and nonmelanoma skin cancer: Is it a class effect? J. Am. Acad. Dermatol. 2020, 82, e25–e26. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Center | PSM | Case | Subjects | Skin Cancer | Incident Density * | NMSC | Incident Density * | MSC | Incident Density * |
|---|---|---|---|---|---|---|---|---|---|
| SNU | Before | Never use | 198,173 | 366 | 27.1 | 296 | 21.9 | 70 | 5.2 |
| Ever use 1 | 47,557 | 119 | 30.3 | 97 | 24.7 | 22 | 5.6 | ||
| HCTZ-only use 2 | 7435 | 12 | 21.4 | 9 | 16.0 | 3 | 5.4 | ||
| After | Never use | 47,557 | 107 | 31.3 | 89 | 26.1 | 18 | 5.3 | |
| Ever use 1 | 47,557 | 119 | 30.3 | 97 | 24.7 | 22 | 5.6 | ||
| HCTZ-only use 2 | 7435 | 12 | 21.4 | 9 | 16.0 | 3 | 5.4 | ||
| SNUB | Before | Never use | 57,270 | 134 | 39.3 | 124 | 36.4 | 10 | 2.9 |
| Ever use 1 | 36,784 | 127 | 44.2 | 120 | 41.7 | 7 | 2.4 | ||
| HCTZ-only use 2 | 14,331 | 42 | 38.3 | 41 | 37.4 | 1 | 0.9 | ||
| After | Never use | 36,784 | 93 | 42.0 | 85 | 38.4 | 8 | 3.6 | |
| Ever use 1 | 36,784 | 127 | 44.2 | 120 | 41.7 | 7 | 2.4 | ||
| HCTZ-only use 2 | 14,331 | 42 | 38.3 | 41 | 37.4 | 1 | 0.9 | ||
| ASAN | Before | Never use | 262,306 | 458 | 24.2 | 413 | 21.8 | 45 | 2.4 |
| Ever use 1 | 65,258 | 131 | 25.6 | 112 | 21.9 | 19 | 3.7 | ||
| HCTZ-only use 2 | 11,998 | 16 | 18.0 | 10 | 11.2 | 6 | 6.8 | ||
| After | Never use | 36,784 | 93 | 42.0 | 85 | 38.4 | 8 | 3.6 | |
| Ever use 1 | 36,784 | 127 | 44.2 | 120 | 41.7 | 7 | 2.4 | ||
| HCTZ-only use 2 | 14,331 | 42 | 38.3 | 41 | 37.4 | 1 | 0.9 |
| SNU | ||||||
|---|---|---|---|---|---|---|
| Before Matching | After Matching | |||||
| Never Use | Ever Use 1 | Never Use | Ever Use 1 | |||
| N (%) | N (%) | SMD 2 | N (%) | N (%) | SMD 2 | |
| Age, Mean (SD) | 50.60 (16.0) | 51.36 (15.7) | 0.048 | 51.35 (15.6) | 51.36 (15.7) | <0.001 |
| Female | 112,452 (56.7) | 27,111 (57.0) | 0.005 | 27,275 (57.4) | 27,111 (57.0) | 0.007 |
| CCI | 0.271 | 0.008 | ||||
| 0 | 84,327 (42.6) | 15,553 (32.7) | 15,375 (32.3) | 15,553 (32.7) | ||
| 1 | 68,293 (34.5) | 15,618 (32.8) | 15,666 (32.9) | 15,618 (32.8) | ||
| ≥2 | 45,553 (23.0) | 16,386 (34.5) | 16,516 (34.7) | 16,386 (34.5) | ||
| Disease history | ||||||
| Diabetes | 43,360 (21.9) | 17,911 (37.7) | 0.350 | 17,901 (37.6) | 17,911 (37.7) | <0.001 |
| COPD | 13,266 (6.7) | 5070 (10.7) | 0.141 | 4747 (10.0) | 5070 (10.7) | 0.022 |
| Drug use | ||||||
| Aspirin | 50,255 (25.4) | 22,542 (47.4) | 0.471 | 22,573 (47.5) | 22,542 (47.4) | 0.001 |
| NSAIDS | 70,329 (35.5) | 17,181 (36.1) | 0.013 | 16,831 (35.4) | 17,181 (36.1) | 0.015 |
| Statins | 52,885 (26.7) | 21,434 (45.1) | 0.391 | 21,535 (45.3) | 21,434 (45.1) | 0.004 |
| ASAN | ||||||
| Age, Mean (SD) | 59.15 (13.13) | 62.66 (11.78) | 0.281 | 62.69 (11.73) | 62.66 (11.78) | 0.003 |
| Female | 119,243 (45.5) | 32,207 (49.4) | 0.078 | 32,177 (49.3) | 32,207 (49.4) | 0.001 |
| CCI | 0.169 | 0.004 | ||||
| 0 | 99,225 (37.8) | 19,793 (30.3) | 19,684 (30.2) | 19,793 (30.3) | ||
| 1 | 73,747 (28.1) | 18,962 (29.1) | 18,947 (29.0) | 18,962 (29.1) | ||
| ≥2 | 89,334 (34.1) | 26,503 (40.6) | 26,627 (40.8) | 26,503 (40.6) | ||
| Disease history | ||||||
| Diabetes | 65,625 (25.0) | 21,033 (32.2) | 0.160 | 21,076 (32.3) | 21,033 (32.2) | 0.001 |
| COPD | 18,120 (6.9) | 5831 (8.9) | 0.075 | 5583 (8.6) | 5831 (8.9) | 0.013 |
| Drug use | ||||||
| Aspirin | 79,195 (30.2) | 24,217 (37.1) | 0.147 | 24,075 (36.9) | 24,217 (37.1) | 0.005 |
| NSAIDS | 100,020 (38.1) | 33,107 (50.7) | 0.256 | 33,064 (50.7) | 33,107 (50.7) | 0.001 |
| Statins | 89,715 (34.2) | 27,593 (42.3) | 0.167 | 27,615 (42.3) | 27,593 (42.3) | 0.001 |
| SNUB | ||||||
| Age, Mean (SD) | 61.37 (13.69) | 63.43 (13.07) | 0.154 | 63.52 (13.18) | 63.43 (13.07) | 0.007 |
| Female | 25,276 (44.1) | 19,379 (52.7) | 0.172 | 19,506 (53.0) | 19,379 (52.7) | 0.007 |
| CCI | 0.095 | 0.019 | ||||
| 0 | 18,669 (32.6) | 11,760 (32.0) | 12,066 (32.8) | 11,760 (32.0) | ||
| 1 | 21,802 (38.1) | 12,713 (34.6) | 12,637 (34.4) | 12,713 (34.6) | ||
| ≥2 | 16,799 (29.3) | 12,311 (33.5) | 12,081 (32.8) | 12,311 (33.5) | ||
| Disease history | ||||||
| Diabetes | 16,872 (29.5) | 11,467 (31.2) | 0.037 | 11,174 (30.4) | 11,467 (31.2) | 0.017 |
| COPD | 2011 (3.5) | 1459 (4.0) | 0.024 | 1308 (3.6) | 1459 (4.0) | 0.022 |
| Drug use | ||||||
| Aspirin | 27,751 (48.5) | 19,150 (52.1) | 0.072 | 18,773 (51.0) | 19,150 (52.1) | 0.021 |
| NSAIDS | 4300 (7.5) | 3347 (9.1) | 0.058 | 2972 (8.1) | 3347 (9.1) | 0.036 |
| Statins | 13,666 (23.9) | 8420 (22.9) | 0.023 | 8078 (22.0) | 8420 (22.9) | 0.022 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lee, S.M.; Kim, K.; Yoon, J.; Park, S.K.; Moon, S.; Lee, S.E.; Oh, J.; Yoo, S.; Kim, K.-I.; Yoon, H.-J.; et al. Association between Use of Hydrochlorothiazide and Nonmelanoma Skin Cancer: Common Data Model Cohort Study in Asian Population. J. Clin. Med. 2020, 9, 2910. https://doi.org/10.3390/jcm9092910
Lee SM, Kim K, Yoon J, Park SK, Moon S, Lee SE, Oh J, Yoo S, Kim K-I, Yoon H-J, et al. Association between Use of Hydrochlorothiazide and Nonmelanoma Skin Cancer: Common Data Model Cohort Study in Asian Population. Journal of Clinical Medicine. 2020; 9(9):2910. https://doi.org/10.3390/jcm9092910
Chicago/Turabian StyleLee, Seung Min, Kwangsoo Kim, Jihoon Yoon, Sue K. Park, Sungji Moon, Sang Eun Lee, JiSeon Oh, Sooyoung Yoo, Kwang-Il Kim, Hyung-Jin Yoon, and et al. 2020. "Association between Use of Hydrochlorothiazide and Nonmelanoma Skin Cancer: Common Data Model Cohort Study in Asian Population" Journal of Clinical Medicine 9, no. 9: 2910. https://doi.org/10.3390/jcm9092910
APA StyleLee, S. M., Kim, K., Yoon, J., Park, S. K., Moon, S., Lee, S. E., Oh, J., Yoo, S., Kim, K.-I., Yoon, H.-J., & Lee, H.-Y. (2020). Association between Use of Hydrochlorothiazide and Nonmelanoma Skin Cancer: Common Data Model Cohort Study in Asian Population. Journal of Clinical Medicine, 9(9), 2910. https://doi.org/10.3390/jcm9092910