Thromboprophylaxis for Hospitalized Patients with Inflammatory Bowel Disease—Are We There Yet?

 ,
, 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Collection of Patients with IBD
2.2. Cohort IBD Analysis
2.3. VTE Diagnosis and Treatment
2.4. Statistical Analysis
3. Results
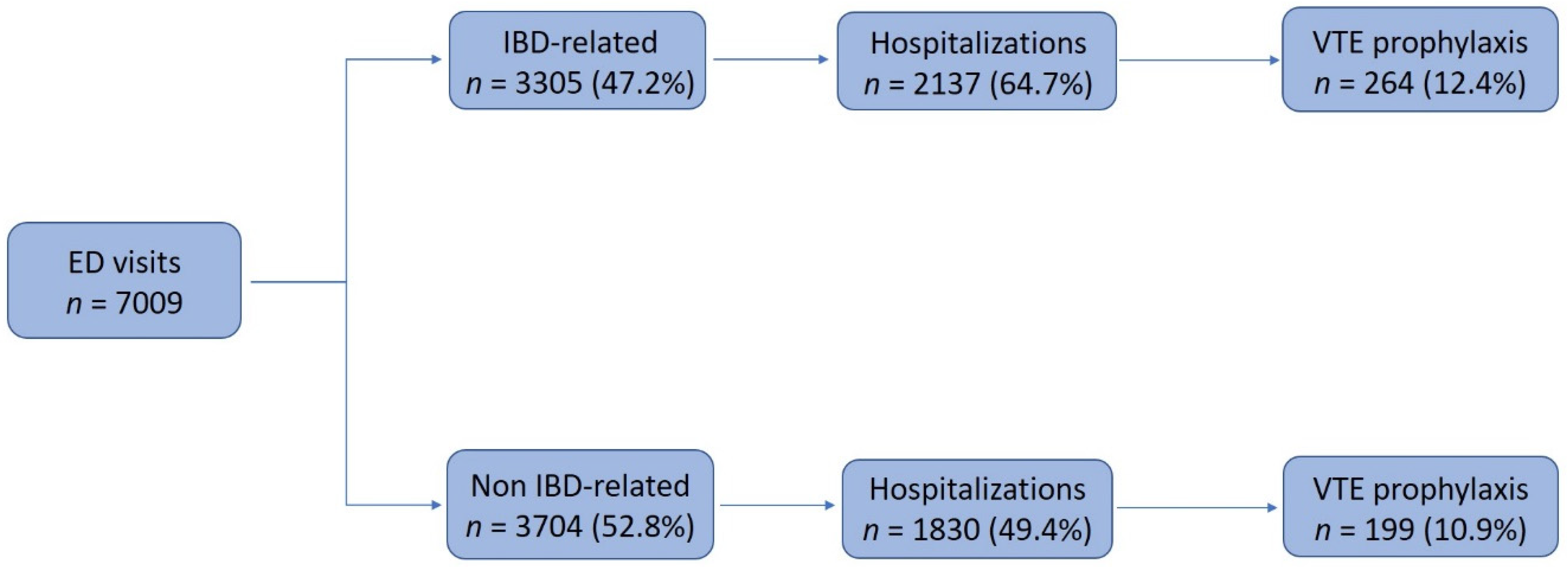
3.1. Emergency Department Visits of Patients with IBD
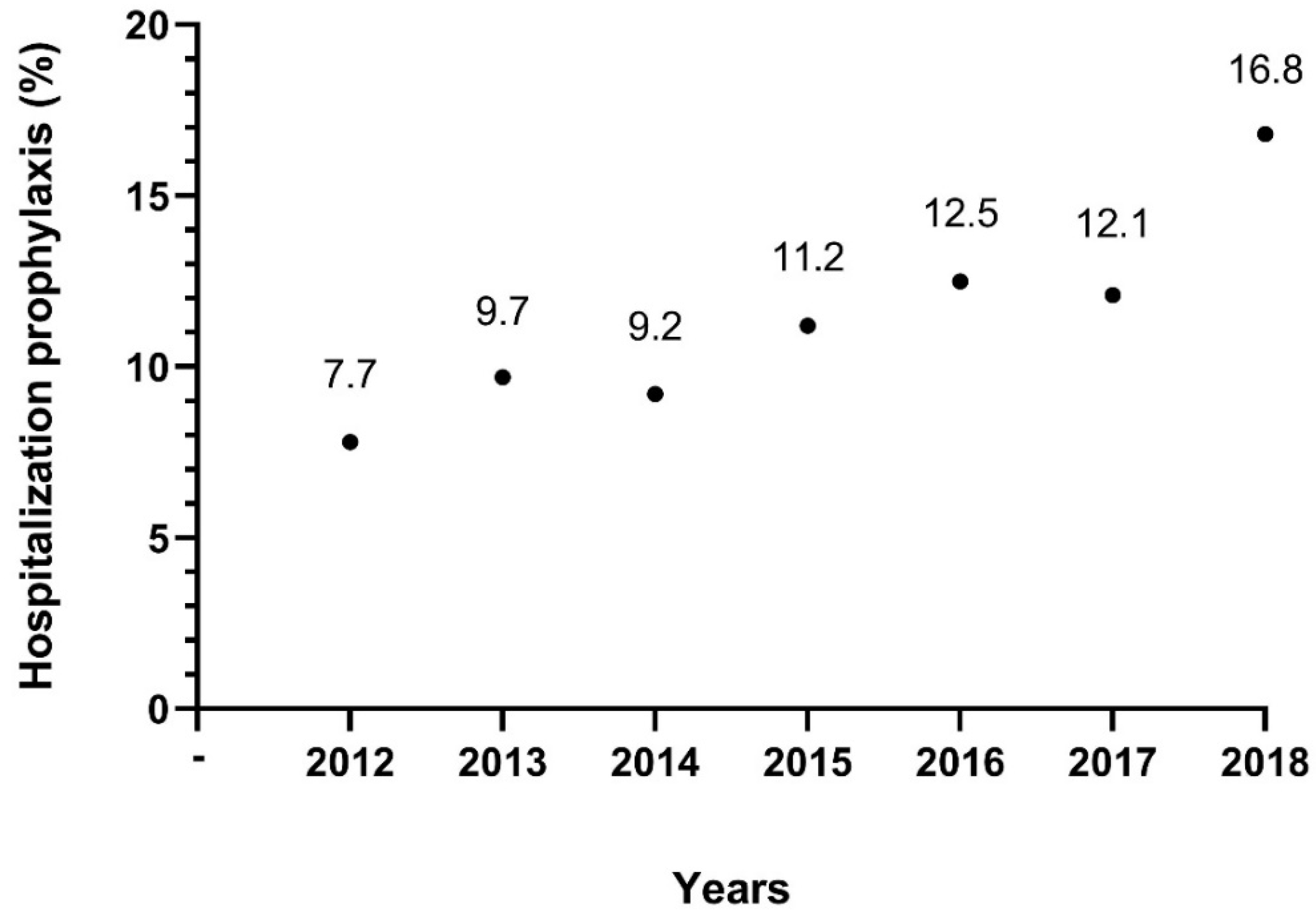
3.2. Prophylactic Anticoagulation during All Hospitalizations
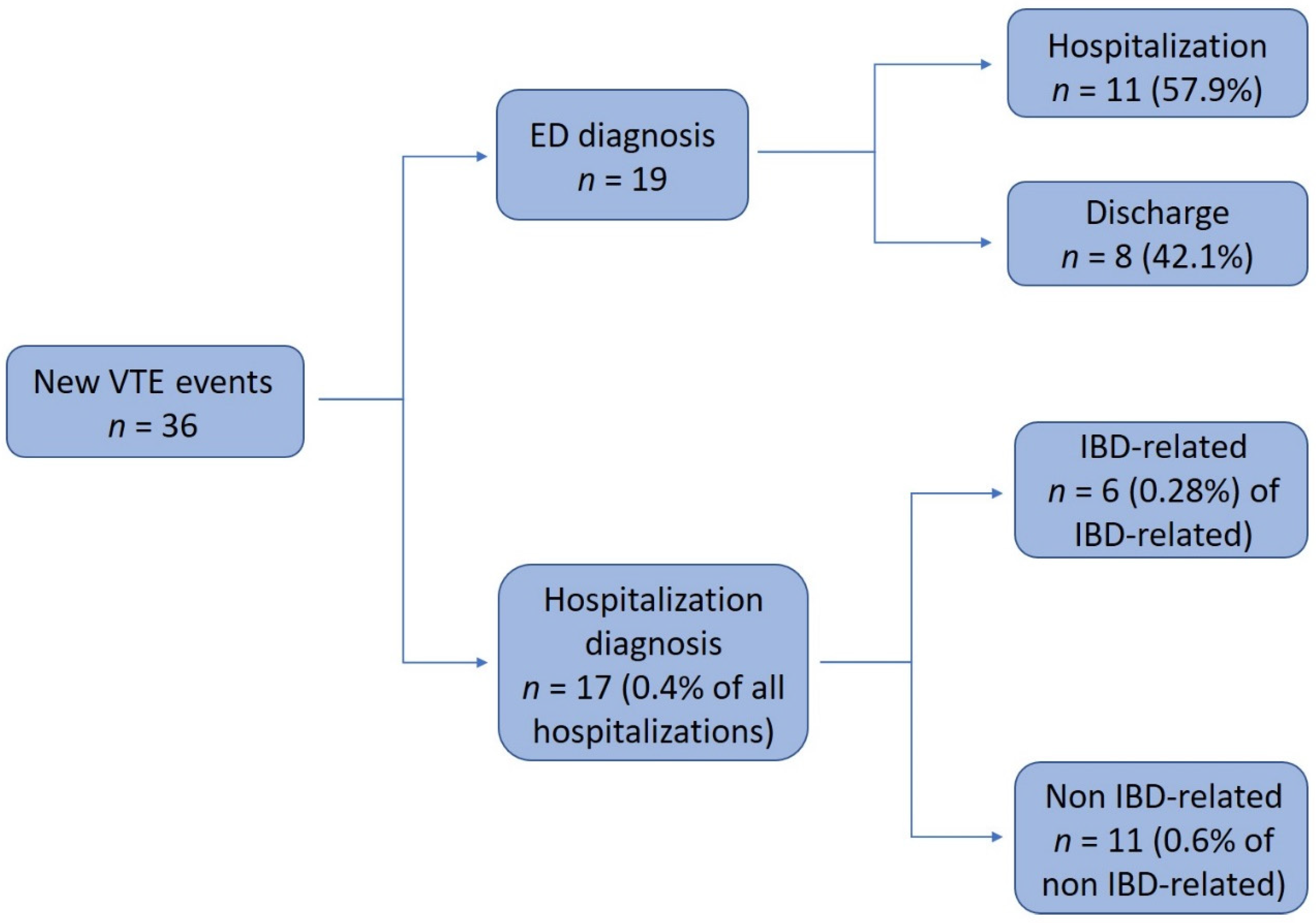
3.3. Clinical Characteristics of All New VTE Patients
3.4. Newly Diagnosed VTE during Hospitalization
3.5. Prophylactic Anticoagulation during Hospitalizations of VTE Events
3.6. Newly Diagnosed VTE in the ED
3.7. Hospitalizations in the Previous 14 Days before VTE Diagnosis
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Miehsler, W.; Reinisch, W.; Valic, E.; Osterode, W.; Tillinger, W.; Feichtenschlager, T.; Grisar, J.; Machold, K.; Scholz, S.; Vogelsang, H.; et al. Is inflammatory bowel disease an independent and disease specific risk factor for thromboembolism? Gut 2004, 53, 542–548. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Talbot, R.W.; Heppell, J.; Dozois, R.R.; Beart, R.W., Jr. Vascular complications of inflammatory bowel disease. Mayo Clin. Proc. 1986, 61, 140–145. [Google Scholar] [CrossRef]
- Kopylov, U.; Amitai, M.M.; Lubetsky, A.; Eliakim, R.; Chowers, Y.; Ben-Horin, S. Clinical and radiographic presentation of superior mesenteric vein thrombosis in Crohn’s disease: A single center experience. J. Crohn’s Colitis 2012, 6, 43–49. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bernstein, C.N.; Blanchard, J.F.; Houston, D.S.; Wajda, A. The incidence of deep venous thrombosis and pulmonary embolism among patients with inflammatory bowel disease: A population-based cohort study. Thromb. Haemost. 2001, 85, 430–434. [Google Scholar] [PubMed]
- Grainge, M.J.; West, J.; Card, T.R. Venous thromboembolism during active disease and remission in inflammatory bowel disease: A cohort study. Lancet 2010, 375, 657–663. [Google Scholar] [CrossRef]
- Nguyen, G.C.; Sam, J. Rising prevalence of venous thromboembolism and its impact on mortality among hospitalized inflammatory bowel disease patients. Am. J. Gastroenterol. 2008, 103, 2272–2280. [Google Scholar] [CrossRef]
- Kappelman, M.D.; Horvath-Puho, E.; Sandler, R.S.; Rubin, D.T.; Ullman, T.A.; Pedersen, L.; Baron, J.A.; Sørensen, H.T. Thromboembolic risk among Danish children and adults with inflammatory bowel diseases: A population-based nationwide study. Gut 2011, 60, 937–943. [Google Scholar] [CrossRef]
- Fumery, M.; Xiaocang, C.; Dauchet, L.; Gower-Rousseau, C.; Peyrin-Biroulet, L.; Colombel, J.F. Thromboembolic events and cardiovascular mortality in inflammatory bowel diseases: A meta-analysis of observational studies. J. Crohn’s Colitis 2014, 8, 469–479. [Google Scholar] [CrossRef]
- Yuhara, H.; Steinmaus, C.; Corley, D.; Koike, J.; Igarashi, M.; Suzuki, T.; Mine, T. Meta-analysis: The risk of venous thromboembolism in patients with inflammatory bowel disease. Aliment. Pharmacol. Ther. 2013, 37, 953–962. [Google Scholar] [CrossRef]
- Murthy, S.K.; Nguyen, G.C. Venous thromboembolism in inflammatory bowel disease: An epidemiological review. Am. J. Gastroenterol. 2011, 106, 713–718. [Google Scholar] [CrossRef]
- Papay, P.; Miehsler, W.; Tilg, H.; Petritsch, W.; Reinisch, W.; Mayer, A.; Haas, T.; Kaser, A. Clinical presentation of venous thromboembolism in inflammatory bowel disease. J. Crohn’s Colitis 2013, 7, 723–729. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Scoville, E.A.; Konijeti, G.G.; Nguyen, D.D.; Sauk, J.; Yajnik, V.; Ananthakrishnan, A.N. Venous thromboembolism in patients with inflammatory bowel diseases: A case-control study of risk factors. Inflamm. Bowel Dis. 2014, 20, 631–636. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Faye, A.S.; Wen, T.; Ananthakrishnan, A.N.; Lichtiger, S.; Kaplan, G.G.; Friedman, A.M.; Lawlor, G.; Wright, J.D.; Attenello, F.J.; Mack, W.J.; et al. Acute venous thromboembolism risk highest within 60 days after discharge from the hospital in patients with inflammatory bowel diseases. Clin. Gastroenterol. Hepatol. 2020, 18, 1133–1141. [Google Scholar] [CrossRef] [PubMed]
- Novacek, G.; Weltermann, A.; Sobala, A.; Tilg, H.; Petritsch, W.; Reinisch, W.; Mayer, A.; Haas, T.; Kaser, A.; Feichtenschlager, T.; et al. Inflammatory bowel disease is a risk factor for recurrent venous thromboembolism. Gastroenterology 2010, 39, 779–787. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wallaert, J.B.; De Martino, R.R.; Marsicovetere, P.S.; Goodney, P.P.; Finlayson, S.R.; Murray, J.J.; Holubar, S.D. Venous thromboembolism after surgery for inflammatory bowel disease: Are there modifiable risk factors? Data from ACS NSQIP. Dis. Colon Rectum 2012, 55, 1138. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Koutroumpakis, E.I.; Tsiolakidou, G.; Koutroubakis, I.E. Risk of venous thromboembolism in patients with inflammatory bowel disease. Semin. Thromb. Hemost. 2013, 39, 461–468. [Google Scholar] [CrossRef]
- Chu, T.P.; Grainge, M.J.; Card, T.R. The risk of venous thromboembolism during and after hospitalisation in patients with inflammatory bowel disease activity. Aliment. Pharmacol. Ther. 2018, 48, 1099–1108. [Google Scholar] [CrossRef] [Green Version]
- Nguyen, G.C.; Bernstein, C.N.; Bitton, A.; Chan, A.K.; Griffiths, A.M.; Leontiadis, G.I.; Geerts, W.; Bressler, B.; Butzner, J.D.; Carrier, M.; et al. Consensus statements on the risk, prevention, and treatment of venous thromboembolism in inflammatory bowel disease: Canadian Association of Gastroenterology. Gastroenterology 2014, 146, 835–848. [Google Scholar] [CrossRef] [Green Version]
- Harbord, M.; Annese, V.; Vavricka, S.R.; Allez, M.; Barreiro-de Acosta, M.; Boberg, K.M.; Burisch, J.; De Vos, M.; De Vries, A.M.; Dick, A.D.; et al. The first European evidence-based consensus on extra-intestinal manifestations in inflammatory bowel disease. J. Crohn’s Colitis 2016, 10, 239–254. [Google Scholar] [CrossRef]
- Sam, J.J.; Bernstein, C.N.; Razik, R.; Thanabalan, R.; Nguyen, G.C. Physicians’ perceptions of risks and practices in venous thromboembolism prophylaxis in inflammatory bowel disease. Dig. Dis. Sci. 2013, 58, 46–52. [Google Scholar] [CrossRef]
- Razik, R.; Bernstein, C.N.; Sam, J.; Thanabalan, R.; Nguyen, G.C. Survey of perceptions and practices among Canadian gastroenterologists regarding the prevention of venous thromboembolism for hospitalized inflammatory bowel disease patients. Can. J. Gastroenterol. 2012, 26, 795–798. [Google Scholar] [CrossRef] [PubMed]
- Tinsley, A.; Naymagon, S.; Enomoto, L.M.; Hollenbeak, C.S.; Sands, B.E.; Ullman, T.A. Rates of pharmacologic venous thromboembolism prophylaxis in hospitalized patients with active ulcerative colitis: Results from a tertiary care center. J. Crohn’s Colitis 2013, 7, e635–e640. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Geerts, W.H.; Bergqvist, D.; Pineo, G.F.; Heit, J.A.; Samama, C.M.; Lassen, M.R.; Colwell, C.W. Prevention of venous thromboembolism: American College of Chest Physicians evidence-based clinical practice guidelines. Chest 2008, 133, 381S–453S. [Google Scholar] [CrossRef] [PubMed]
- Johannesdottir, S.A.; Horváth-Puhó, E.; Dekkers, O.M.; Cannegieter, S.C.; Jørgensen, J.O.L.; Ehrenstein, V.; Vandenbroucke, J.P.; Pedersen, L.; Sørensen, H.T. Use of glucocorticoids and risk of venous thromboembolism: A nationwide population-based case-control study. JAMA Intern. Med. 2013, 173, 743–752. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Anderson, F.A.; Spencer, F.A. Risk factors for venous thromboembolism. Circulation 2003, 107, I-9–I-16. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Solem, C.A.; Loftus, E.V., Jr.; Tremaine, W.J.; Sandborn, W.J. Venous thromboembolism in inflammatory bowel disease. Am. J. Gastroenterol. 2004, 99, 97–101. [Google Scholar] [CrossRef]
- Sbeit, W.; Kadah, A.; Shafrir, A.; Kalisky, I.; Mahamid, M.; Hazou, W.; Katz, L.; Mari, A.; Khoury, T. Unawareness of thromboprophylaxis is associated with low venous thromboembolism occurrence in hospitalized patients with acute inflammatory bowel disease flare. Minerva Med. 2020. [Google Scholar] [CrossRef]
- McCurdy, J.D.; Israel, A.; Hasan, M.; Weng, R.; Mallick, R.; Ramsay, T.; Carrier, M. A clinical predictive model for post-hospitalisation venous thromboembolism in patients with inflammatory bowel disease. Aliment. Pharmacol. Ther. 2019, 49, 1493–1501. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| ED Visits, n | 7009 |
| Total patients, n | 2405 |
| Visits per patient, average (SD) | 2.91 (± 5.3) |
| Male, n (% of total patients) Female, n (% of total patients) | 1216 (50.5) 1189 (49.5) |
| Crohn’s disease, n (% of total patients) | 1556 (64.7) |
| Ulcerative colitis, n (% of total patients) | 849 (35.3) |
| Age of admission, median years (IQR) | 42 (28–65) |
| IBD-related complaints, n (% of ED visits) | 3305 (47.2) |
| Total hospitalizations, n (% of ED visits) | 3967 (56.6) |
| Hospitalization unit, n (% of total hospitalizations) | |
| General surgery | 1510 (38.1) |
| Internal medicine and geriatrics | 1505 (37.9) |
| Short-term hospitalization unit | 297 (7.5) |
| Pediatrics | 226 (5.7) |
| Cardiology | 76 (1.9) |
| Others (Orthopedics, Urology, Oncology, Gynecology) | 353 (8.9) |
| Hospitalization length in days, median (IQR) | 4 (2–7) |
| Return to ED in 30 days (% of ED visits) | 1303 (18.6) |
| VTE prophylaxis, n (% of total hospitalizations) | 463 (11.7) |
| Patients with Newly Diagnosed VTE | 36 |
| ED diagnosis, n (% of VTE) | 19 (52.8) |
| Hospitalization diagnosis, n (% of VTE) | 17 (47.2) |
| Male, n (%) | 18 (50) |
| Female, n (%) | 18 (50) |
| Single VTE, n (% of patients) | 30 (83.3) |
| Double VTE, n (% of patients) | 6 (16.6) |
| DVT, n (%) | 34 (94.4) |
| PE, n (%) | 8 (22.2) |
| DVT location, n (% of DVTs) | |
| Proximal | 28 (82.4) |
| Distal | 9 (26.5) |
| Age at onset of VTE, median (IQR) | 64.5 (48.25–79.25) |
| Additional thrombosis-related risk factors, n (%) | |
| Malignancy | 6 (16.7) |
| Post-operative period | 6 (16.7) |
| Bedridden | 4 (12.5) |
| Central venous access | 2 (5.5) |
| No risk factors | 21 (58.3) |
| CD, n (%) | 18 (50) |
| UC, n (%) | 18 (50) |
| CD extent, n (% of CD patients) | |
| L1 (ileal) | 3 (16.6) |
| L2 (colonic) | 2 (11.1) |
| L3 (ileo-colonic) | 10 (55.6) |
| CD behavior, n (% of patients with CD) | |
| B1 (non-stricturing and non-penetrating) | 7 (38.9) |
| B2 (stricturing) | 5 (27.8) |
| B3 (penetrating) | 4 (22.2) |
| UC extent, n (% of patients with UC) | |
| E1 (proctitis) | 1 (33.3) |
| E2 (left sided colitis) | 2 (66.7) |
| E3 (right sided colitis) | 0 (0) |
| Additional extra-intestinal manifestations | 8 (22.2) |
| Current IBD therapy, n (%) | |
| 5-ASA derivatives | 18 (50) |
| Steroids | 8 (22.2) |
| Biologics | 7 (19.4) |
| Immunomodulators | 11 (30.6) |
| IBD-Related Diagnosis, n (% of hospitalization VTE) | 6 (35.3) |
| Hospitalization length, median (IQR) | 21 (7–42.5) |
| Hospitalization unit, n (%) | |
| Internal medicine and geriatrics | 11 (64.7) |
| General surgery | 5 (29.4) |
| Orthopedics | 1 (5.9) |
| Mortality, n (% of hospitalization VTE) | |
| In-hospitalization | 1 (5.9) |
| 30 days post-discharge | 1 (5.9) |
| 90 days post-discharge | 1 (5.9) |
| Anticoagulation, n (% of hospitalization VTE) | |
| Prophylaxis | 5 (29.4) |
| Therapeutic | 4 (23.5) |
| None | 8 (47.1) |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Levartovsky, A.; Barash, Y.; Ben-Horin, S.; Ungar, B.; Klang, E.; Soffer, S.; Kopylov, U. Thromboprophylaxis for Hospitalized Patients with Inflammatory Bowel Disease—Are We There Yet? J. Clin. Med. 2020, 9, 2753. https://doi.org/10.3390/jcm9092753
Levartovsky A, Barash Y, Ben-Horin S, Ungar B, Klang E, Soffer S, Kopylov U. Thromboprophylaxis for Hospitalized Patients with Inflammatory Bowel Disease—Are We There Yet? Journal of Clinical Medicine. 2020; 9(9):2753. https://doi.org/10.3390/jcm9092753
Chicago/Turabian StyleLevartovsky, Asaf, Yiftach Barash, Shomron Ben-Horin, Bella Ungar, Eyal Klang, Shelly Soffer, and Uri Kopylov. 2020. "Thromboprophylaxis for Hospitalized Patients with Inflammatory Bowel Disease—Are We There Yet?" Journal of Clinical Medicine 9, no. 9: 2753. https://doi.org/10.3390/jcm9092753
APA StyleLevartovsky, A., Barash, Y., Ben-Horin, S., Ungar, B., Klang, E., Soffer, S., & Kopylov, U. (2020). Thromboprophylaxis for Hospitalized Patients with Inflammatory Bowel Disease—Are We There Yet? Journal of Clinical Medicine, 9(9), 2753. https://doi.org/10.3390/jcm9092753