Heart Failure is Highly Prevalent and Difficult to Diagnose in Severe Exacerbations of COPD Presenting to the Emergency Department

 , , , , , ,
, , , , , ,
Abstract
1. Introduction
2. Methods
2.1. Study Design
2.2. Respiratory Ward Admission
2.3. Follow-Up after Discharge from Chart Review
2.4. Statistics
3. Results
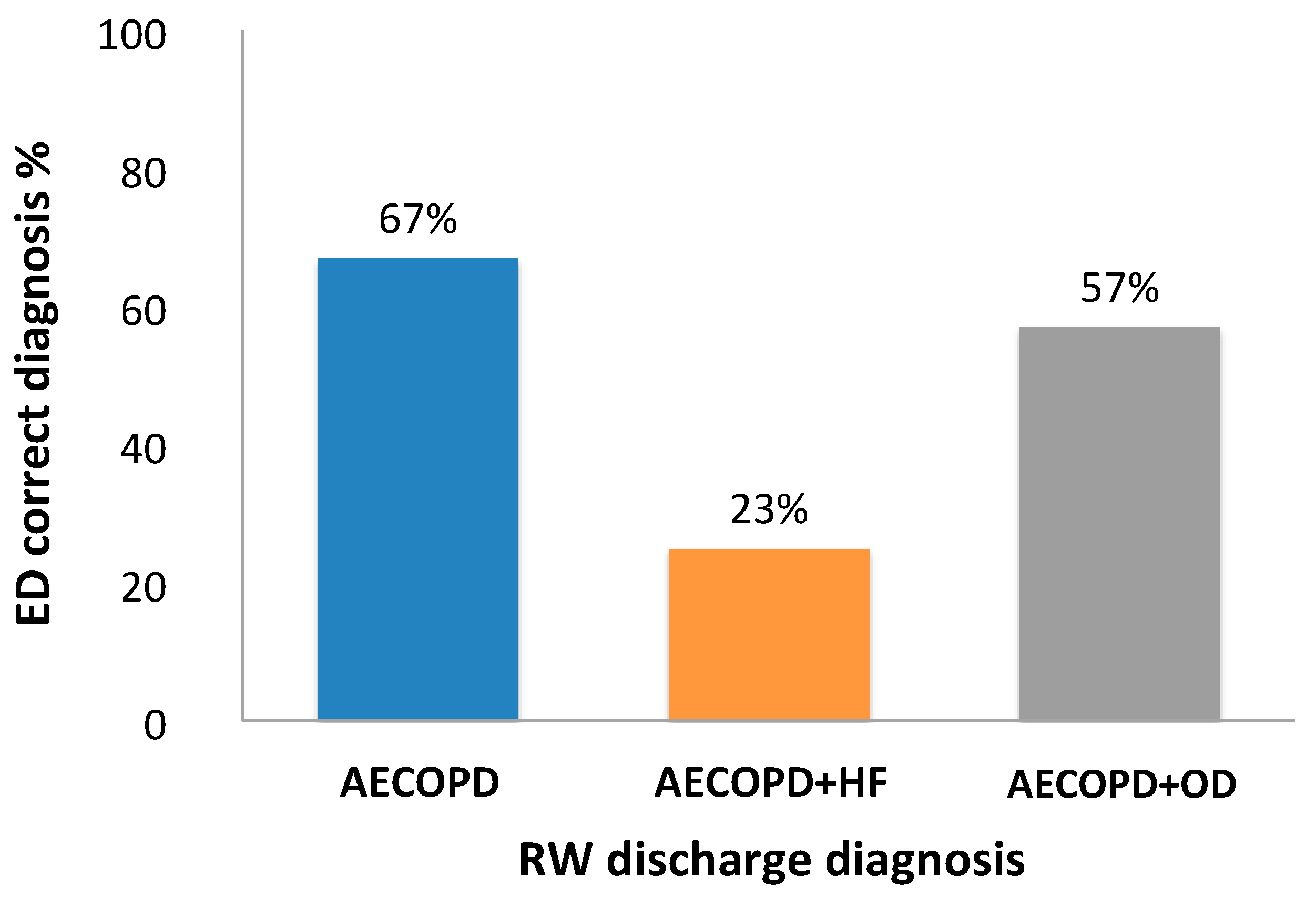
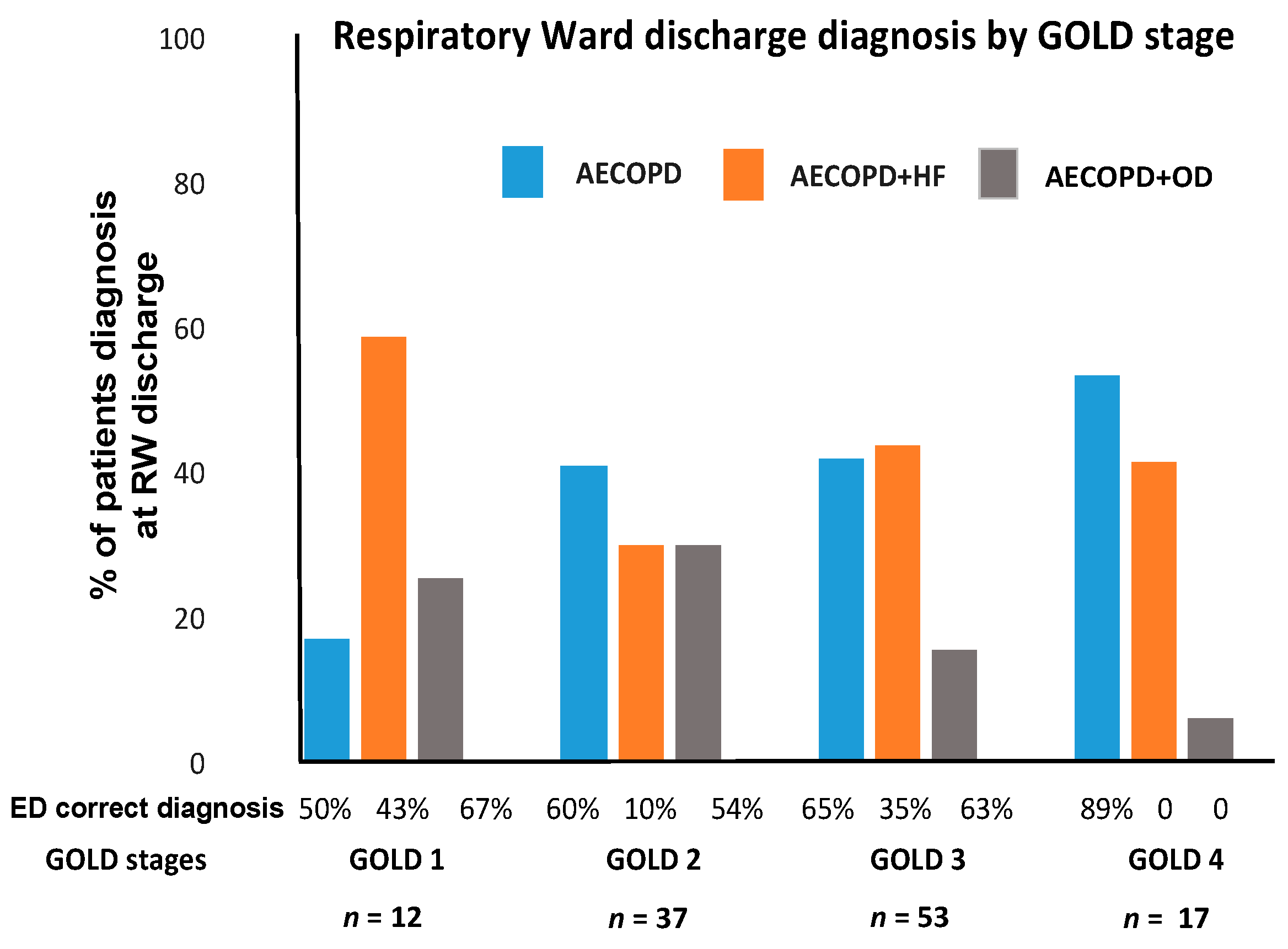
3.1. Diagnostic Comparison between ED and RW
3.2. Laboratory Results
3.3. Hospitalization
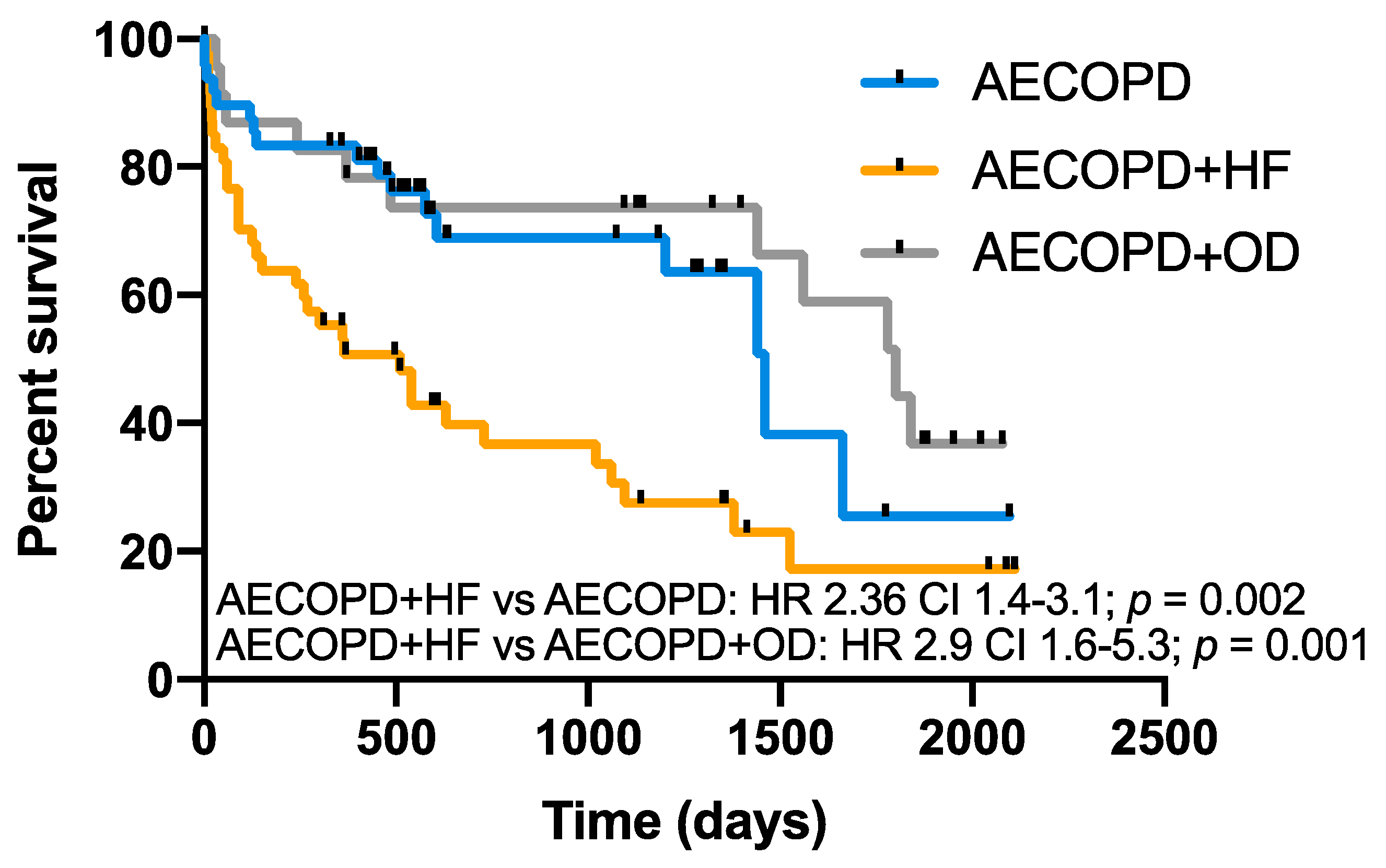
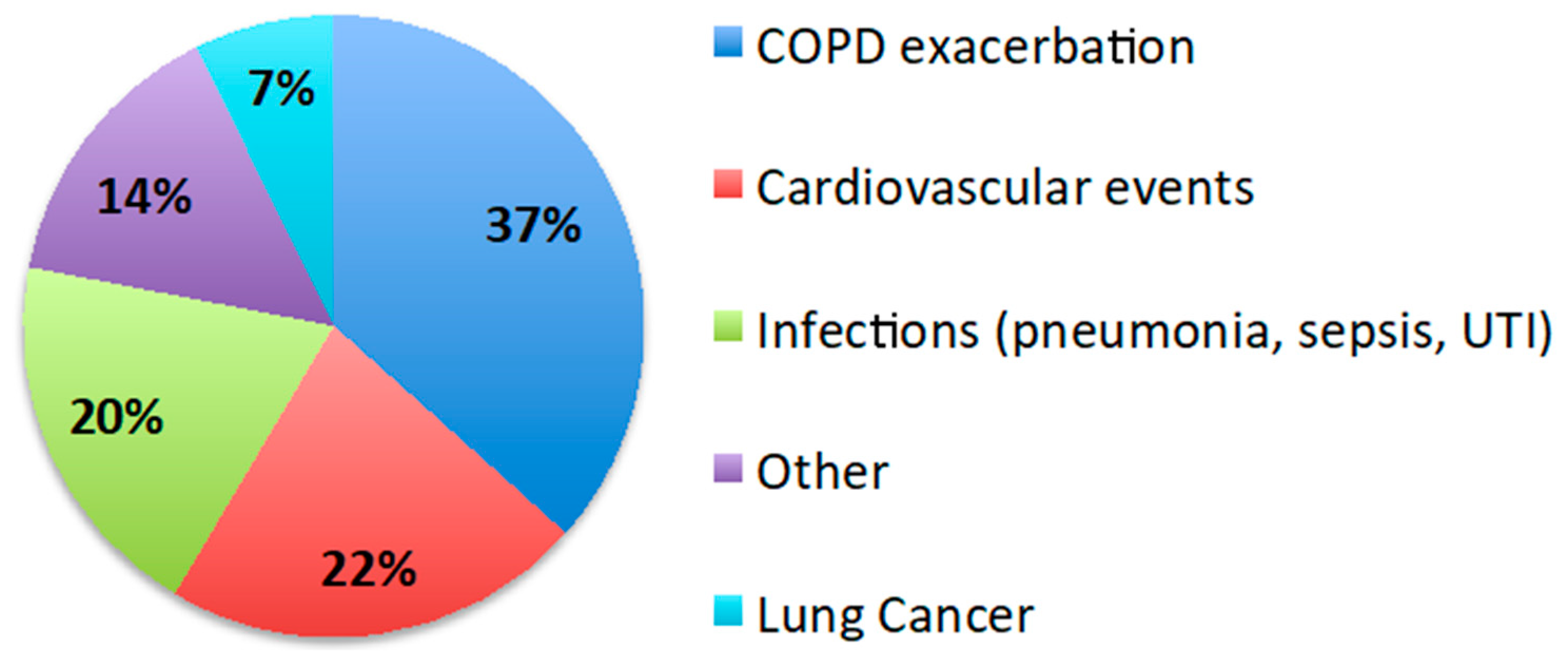
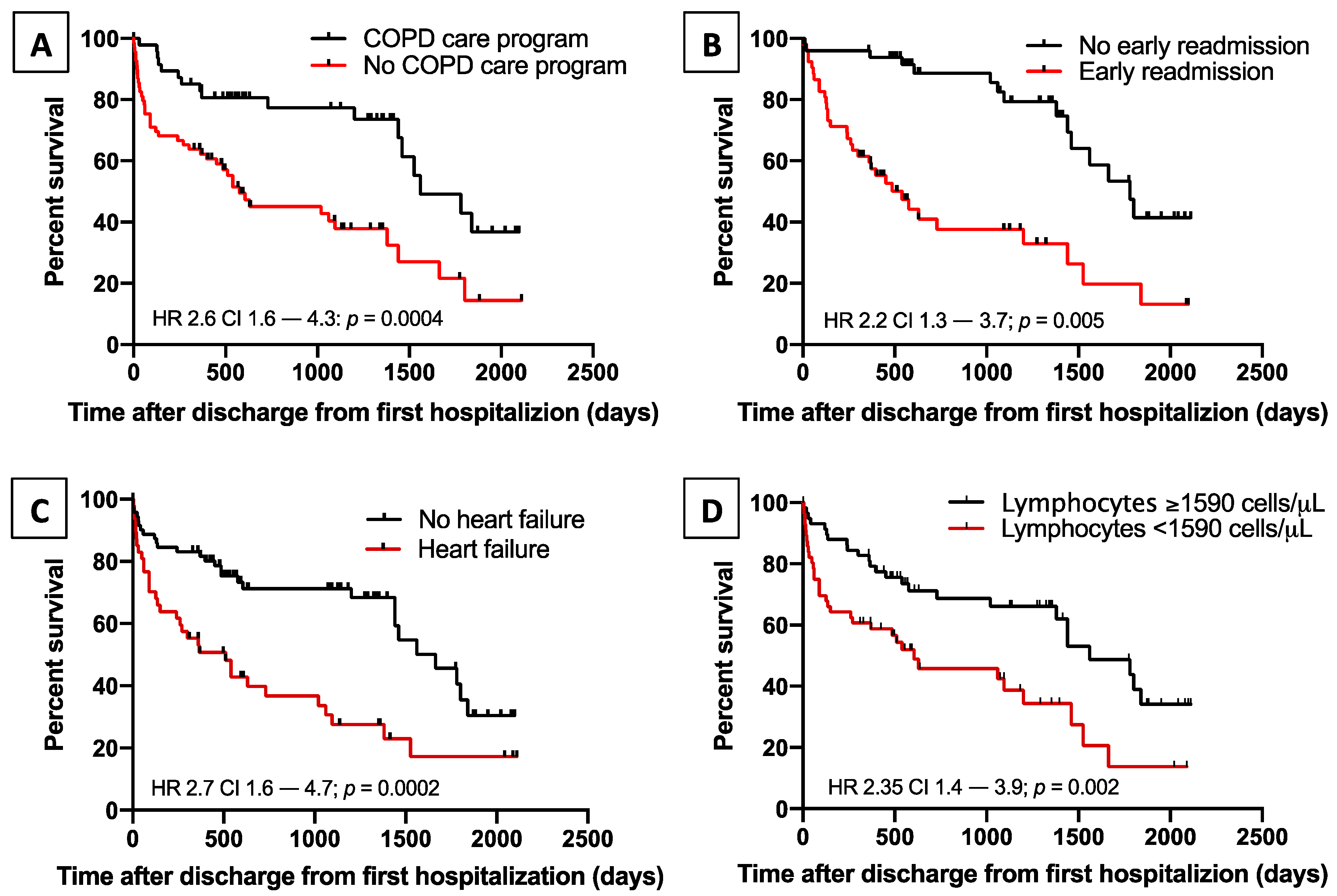
3.4. Post Discharge Follow-Up
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
Abbreviations
| AECOPD | acute exacerbations of COPD |
| AECOPD + HF | acute exacerbations of COPD and heart failure |
| AECOPD + OD | diagnosis other than AECOPD or AECOPD + HF |
| CRP | C-reactive protein |
| ED | emergency department |
| GOLD | Global initiative for Obstructive Lung Disease |
| HF | Heart failure |
| ICS | inhaled corticosteroids |
| LTOT | long-term oxygen therapy |
| NIV | non-invasive ventilation |
| NLR | neutrophil-to-lymphocyte ratio |
| NT-proBNP | N-terminal pro B-type natriuretic peptide |
| OCS | oral corticosteroids |
| RW | respiratory ward |
References
- Global Initiative for Chronic Obstructive Lung Disease. Global Initiative for Chronic Obstructive Lung Disease Global Strategy for the Diagnosis, Management and Prevention of Chronic Obstructive Pulmonary Disease, 2020 Report; Independently Published: Fontana, WI, USA, 2019. [Google Scholar]
- Baraldo, S.; Balestro, E.; Bazzan, E. Alpha-1 antitrypsin deficiency today: New insights in the immunological pathways. Respiration 2016, 91, 380–385. [Google Scholar] [CrossRef] [PubMed]
- Rothnie, K.J.; Müllerová, H.; Smeeth, L.; Quint, J.K. Natural history of chronic obstructive pulmonary disease exacerbations in a general practice-based population with chronic obstructive pulmonary disease. Am. J. Respir. Crit. Care Med. 2018, 198, 464–471. [Google Scholar] [CrossRef] [PubMed]
- Overbeek, J.A.; Penning-van Beest, F.J.A.; Balp, M.M.; Dekhuijzen, R.P.N.; Herings, R.M.C. Burden of exacerbations in patients with moderate to very severe COPD in the Netherlands: A real-life study. COPD J. Chronic Obstr. Pulm. Dis. 2015, 12, 132–143. [Google Scholar] [CrossRef] [PubMed]
- Miravitlles, M.; Ferrer, M.; Pont, A. Effect of exacerbations on quality of life in patients with chronic obstructive pulmonary disease: A 2 year follow up study. Thorax 2004, 59, 387–395. [Google Scholar] [CrossRef] [PubMed]
- Vanasse, A.; Courteau, J.; Couillard, S.; Beauchesne, M.F.; Larivée, P. Predicting one-year mortality after a “first” hospitalization for chronic obstructive pulmonary disease: An eight-variable assessment score tool. COPD J. Chronic Obstr. Pulm. Dis. 2017, 14, 490–497. [Google Scholar] [CrossRef] [PubMed]
- Vanfleteren, L.E.; Spruit, M.A.; Franssen, F.M. Tailoring the approach to multimorbidity in adults with respiratory disease: The NICE guideline. Eur. Respir. J. 2017, 49, 1601696. [Google Scholar] [CrossRef]
- Vanfleteren, L.E.G.W.; Fabbri, L.M. Self-management interventions in COPD patients with multimorbidity. Eur. Respir. J. 2019, 54, 1901850. [Google Scholar] [CrossRef]
- Negewo, N.A.; Gibson, P.G.; McDonald, V.M. COPD and its comorbidities: Impact, measurement and mechanisms. Respirology 2015, 20, 1160–1171. [Google Scholar] [CrossRef]
- Rutten, F.H.; Moons, K.G.; Cramer, M.J.; Grobbee, D.E.; Zuithoff, N.P.; Lammers, J.W.; Hoes, A.W. Recognising heart failure in elderly patients with stable chronic obstructive pulmonary disease in primary care: Cross sectional diagnostic study. BMJ 2005, 331, 1379. [Google Scholar] [CrossRef]
- MacDonald, M.I.; Shafuddin, E.; King, P.T.; Chang, C.L.; Bardin, P.G.; Hancox, R.J. Cardiac dysfunction during exacerbations of chronic obstructive pulmonary disease. Lancet Respir. Med. 2016, 4, 138–148. [Google Scholar] [CrossRef]
- Bafadhel, M.; Criner, G.; Dransfield, M.T.; Janssens, W.; McDonald, V.M.; Vogelmeier, C.F.; Russell, R.E.; Collis, P. Exacerbations of chronich obstructive pulmonary disease: Time to rename. Lancet Respir. Med. 2020, 8, 133–135. [Google Scholar] [CrossRef]
- Cosentino, E.R.; Landolfo, M.; Bentivenga, C.; Spinardi, L.; Esposti, D.D.; Cicero, A.F.; Miceli, R.; Bui, V.; Berardi, E.; Borghi, C. Morbidity and mortality in a population of patients affected by heart failure and chronic obstructive pulmonary disease: An observational study. BMC Cardiovasc. Disord. 2019, 19, 20. [Google Scholar] [CrossRef] [PubMed]
- Bhatt, S.P.; Dransfield, M.T. Chronic obstructive pulmonary disease and cardiovascular disease. Transl. Res. 2013, 162, 237–251. [Google Scholar] [CrossRef] [PubMed]
- Beghé, B.; Verduri, A.; Roca, M.; Fabbri, L.M. Exacerbation of respiratory symptoms in COPD patients may not be exacerbations of COPD. Eur. Respir. J. 2013, 41, 993–995. [Google Scholar] [CrossRef]
- Hangaard, S.; Helle, T.; Nielsen, C.; Hejlesen, O.K. Causes of misdiagnosis of chronic obstructive pulmonary disease: A systematic scoping review. Respir. Med. 2017, 129, 63–84. [Google Scholar] [CrossRef]
- Diab, N.; Gershon, A.S.; Sin, D.D. Underdiagnosis and overdiagnosis of chronic obstructive pulmonary disease. Am. J. Respir. Crit. Care Med. 2018, 198, 1130–1139. [Google Scholar] [CrossRef]
- Gershon, A.S.; Thiruchelvam, D.; Chapman, K.R. Health services burden of undiagnosed and overdiagnosed COPD. Chest 2018, 153, 1336–1346. [Google Scholar] [CrossRef]
- Agusti, A.; Calverley, P.M.; Celli, B.; Coxson, H.O.; Edwards, L.D.; Lomas, D.A.; MacNee, W.; Miller, B.E.; Rennard, S.; Silverman, E.K.; et al. Evaluation of COPD longitudinally to identify predictive surrogate endpoints (ECLIPSE) investigators. Respir. Res. 2010, 11, 122. [Google Scholar] [CrossRef]
- Vanfleteren, L.E.; Spruit, M.A.; Groenen, M.; Gaffron, S.; van Empel, V.P.; Bruijnzeel, P.L.; Rutten, E.P.; Roodt, J.O.; Wouters, E.F.; Franssen, F.M. Clusters of comorbidities based on validated objective measurements and systemic inflammation in patients with chronic obstructive pulmonary disease. Am. J. Respir. Crit. Care Med. 2013, 187, 728–735. [Google Scholar] [CrossRef]
- Chen, W.; Thomas, J.; Sadatsafavi, M.; FitzGerald, J.M. Risk of cardiovascular comorbidity in patients with chronic obstructive pulmonary disease: A systematic review and meta-analysis. Lancet Respir. Med. 2015, 3, 631–639. [Google Scholar] [CrossRef]
- Matamis, D. Targeting occult heart failure in intensive care unit patients with acute chronic obstructive pulmonary disease exacerbation: Effect on outcome and quality of life. J. Crit. Care 2014, 29, 315.e7-14. [Google Scholar] [CrossRef]
- MacIntyre, N.; Huang, Y.C. Acute exacerbations and respiratory failure in chronic obstructive pulmonary disease. Proc. Am. Thorac. Soc. 2008, 5, 530–535. [Google Scholar] [CrossRef] [PubMed]
- Li, H.; Zeng, Z.; Cheng, J. Prognostic role of NT-proBNP for in-hospital and 1-year mortality in patients with acute exacerbations of COPD. Int. J. Chron. Obstruct. Pulmon. Dis. 2020, 15, 57–67. [Google Scholar] [CrossRef]
- Boussuges, A.; Pinet, C.; Molenat, F.; Burnet, H.; Ambrosi, P.; Badier, M.; Sainty, J.M.; Orehek, J. Left atrial and ventricular filling in chronic obstructive pulmonary disease: An echocardiographic and doppler study. Am. J. Respir. Crit. Care Med. 2000, 162, 670–675. [Google Scholar] [CrossRef] [PubMed]
- Jörgensen, K.; Müller, M.F.; Nel, J.; Upton, R.N.; Houltz, E.; Ricksten, S.E. Reduced intrathoracic blood volume and left and right ventricular dimensions in patients with severe emphysema: An MRI study. Chest 2007, 131, 1050–1057. [Google Scholar] [CrossRef] [PubMed]
- Hohlfeld, J.M.; Vogel-Claussen, J.; Biller, H.; Berliner, D.; Berschneider, K.; Tillmann, H.C.; Hiltl, S.; Bauersachs, J.; Welte, T. Effect of lung deflation with indacaterol plus glycopyrronium on ventricular filling in patients with hyperinflation and COPD (CLAIM): A double-blind, randomised, crossover, placebo-controlled, single-centre trial. Lancet Respir. Med. 2018, 6, 368–378. [Google Scholar] [CrossRef]
- Donaldson, G.C.; Hurst, J.R.; Smith, C.J.; Hubbard, R.B.; Wedzicha, J.A. Increased risk of myocardial infarction and stroke following exacerbation of COPD. Chest 2010, 137, 1091–1097. [Google Scholar] [CrossRef] [PubMed]
- Au, D.H.; Udris, E.M.; Fan, V.S.; Curtis, J.R.; McDonell, M.B.; Fihn, S.D. Risk of mortality and heart failure exacerbations associated with inhaled beta-adrenoceptor agonists among patients with known left ventricular systolic dysfunction. Chest 2003, 123, 1964–1969. [Google Scholar] [CrossRef] [PubMed]
- Buajordet, I.; Ebbesen, J.; Erikssen, J.; Brors, O.; Hilberg, T. Fatal adverse drug events: The paradox of drug treatment. J. Intern. Med. 2001, 250, 327–341. [Google Scholar] [CrossRef] [PubMed]
- Han, M.K.; Quibrera, P.M.; Carretta, E.E.; Barr, R.G.; Bleecker, E.R.; Bowler, R.P.; Cooper, C.B.; Comellas, A.; Couper, D.J.; Curtis, J.L.; et al. Frequency of exacerbations in patients with chronic obstructive pulmonary disease: An analysis of the SPIROMICS cohort. Lancet Respir. Med. 2017, 5, 619–626. [Google Scholar] [CrossRef]
- Zhou, M.; Chen, C.; Peng, J.; Luo, C.H.; Feng, D.Y.; Yang, H.; Xie, X.; Zhou, Y. Fast Prediction of Deterioration and Death Risk in Patients With Acute Exacerbation of Chronic Obstructive Pulmonary Disease Using Vital Signs and Admission History: Retrospective Cohort Study. JMIR Med. Inform. 2019, 7, e13085. [Google Scholar] [CrossRef] [PubMed]
- Serra-Picamal, X.; Roman, R.; Escarrabill, J.; Garcia-Altes, A.; Argimon, J.M.; Soler, N. Hospitalization due to exacerbations of COPD, a big data perspective. Respir. Med. 2018, 145, 219–225. [Google Scholar] [CrossRef] [PubMed]
- Acanfora, D.; Gheorghiade, M.; Trojano, L.; Furgi, G.; Pasini, E.; Picone, C.; Papa, A.; Iannuzzi, G.L.; Bonow, R.O.; Rengo, F. Relative lymphocyte count: A prognostic indicator of mortality in elderly patients with congestive heart failure. Am. Heart J. 2001, 142, 167–173. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Respiratory Ward Diagnostic Groups | |||||
|---|---|---|---|---|---|
| Whole Population | AECOPD (n = 48) | AECOPD + HF (n = 48) | AECOPD + OD (n = 23) | p | |
| Subjects, n (%) | 119 (100) | 48 (40.3) | 48 (40.3) | 23 (19.4) | - |
| Age, years | 74 ± 10 | 72 ± 10 | 76 ± 9 | 76 ± 11 | n.s. |
| Male sex, n (%) | 66 (55) | 30 (63) | 22 (46) | 14 (61) | n.s. |
| Smoking History, pack-years | 40 ± 24 | 42 ± 30 | 40 ± 19 | 39 ± 20 | n.s. |
| FEV1, L | 1.08 ± 0.4 | 1.09 ± 0.5 | 1.08 ± 0.4 | 1.12 ± 0.33 | n.s. |
| FEV1, % predicted | 51 ± 18 | 48 ± 19 | 54 ± 21 | 54 ± 12 | n.s. |
| Presence of | |||||
| emphysema, n (%) | 54 (45) | 25 (52) | 19 (40) | 10 (43) | n.s. |
| GOLD stage, n (%) | |||||
| 1 | 12 (10) | 2 (4) | 7 (14) | 3 (13) | n.s. |
| 2 | 37 (31) | 15 (31) | 11 (23) | 11 (48) | n.s. |
| 3 | 53 (45) | 22 (46) | 23 (48) | 8 (35) | n.s. |
| 4 | 17 (14) | 9 (19) | 7 (15) | 1 (4) | n.s |
| Comorbidities, n | 3.5 ± 1.8 | 3 ± 1.7 * | 4 ± 1.9 | 3.5 ± 1.8 | 0.04 |
| NIV at home, n (%) | 16 (15) | 6 (13) | 9 (19) | 1 (4) | n.s. |
| LTOT at home, n (%) | 66 (55) | 24 (50) | 34 (70) | 8 (35) * | 0.01 |
| ED Diagnosis | Sensitivity (%) | Specificity (%) | PPV (%) | NPV (%) | LR+ | LR− |
|---|---|---|---|---|---|---|
| AECOPD | 27.0 | 56.0 | 51.0 | 7.0 | 0.5 | 1.6 |
| AECOPD + HF | 23.0 | 99.0 | 92.0 | 65.0 | 23.0 | 0.8 |
| AECOPD + OD | 52.0 | 69.0 | 28.0 | 85.0 | 1.7 | 0.9 |
| Whole Population | AECOPD (n = 48) | AECOPD + HF (n = 48) | AECOPD + OD (n = 23) | p | ||
|---|---|---|---|---|---|---|
| Drawn at ED | NT-proBNP, ng/L | 1596 ± 2558 | 144 ± 113 * | 2567 ± 2826 | 1747 ± 2987 | 0.01 |
| CRP, mg/L | 82.3 ± 99.4 | 28.6 ± 58.5 *,§ | 93 ± 98.3 | 132 ± 116.3 | 0.01 | |
| Drawn at RW | NT-proBNP, ng/L | 960 ± 2168 | 140 ± 207 *,§ | 1629 ± 2941 | 779 ± 895 | <0.0001 |
| CRP, mg/L | 60.3 ± 76.2 | 38.2 ± 58.7 *,§ | 68.3 ± 78.5 | 89.7 ± 92.3 | 0.01 | |
| Risk Factor | Univariate Analysis | Cox Regression | ||
|---|---|---|---|---|
| p Value | HR | 95% CI | p Value | |
| Lack of inclusion in a COPD care program | 0.001 | 2.56 | 1.31–4.99 | 0.006 |
| Heart failure | 0.0003 | 2.19 | 1.26–3.79 | 0.005 |
| Early readmission for AECOPD | 0.006 | 2.05 | 1.11–3.79 | 0.02 |
| Lymphocytes * (cells/µL) | 0.0003 | 0.57 | 0.37–0.87 | 0.01 |
| Neutrophil-to-lymphocytes ratio | 0.02 | - | - | - |
| GOLD stage 3–4 | 0.036 | - | - | - |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tinè, M.; Bazzan, E.; Semenzato, U.; Biondini, D.; Cocconcelli, E.; Balestro, E.; Casara, A.; Baraldo, S.; Turato, G.; Cosio, M.G.; et al. Heart Failure is Highly Prevalent and Difficult to Diagnose in Severe Exacerbations of COPD Presenting to the Emergency Department. J. Clin. Med. 2020, 9, 2644. https://doi.org/10.3390/jcm9082644
Tinè M, Bazzan E, Semenzato U, Biondini D, Cocconcelli E, Balestro E, Casara A, Baraldo S, Turato G, Cosio MG, et al. Heart Failure is Highly Prevalent and Difficult to Diagnose in Severe Exacerbations of COPD Presenting to the Emergency Department. Journal of Clinical Medicine. 2020; 9(8):2644. https://doi.org/10.3390/jcm9082644
Chicago/Turabian StyleTinè, Mariaenrica, Erica Bazzan, Umberto Semenzato, Davide Biondini, Elisabetta Cocconcelli, Elisabetta Balestro, Alvise Casara, Simonetta Baraldo, Graziella Turato, Manuel G. Cosio, and et al. 2020. "Heart Failure is Highly Prevalent and Difficult to Diagnose in Severe Exacerbations of COPD Presenting to the Emergency Department" Journal of Clinical Medicine 9, no. 8: 2644. https://doi.org/10.3390/jcm9082644
APA StyleTinè, M., Bazzan, E., Semenzato, U., Biondini, D., Cocconcelli, E., Balestro, E., Casara, A., Baraldo, S., Turato, G., Cosio, M. G., & Saetta, M. (2020). Heart Failure is Highly Prevalent and Difficult to Diagnose in Severe Exacerbations of COPD Presenting to the Emergency Department. Journal of Clinical Medicine, 9(8), 2644. https://doi.org/10.3390/jcm9082644