T Helper Cell Infiltration in Osteoarthritis-Related Knee Pain and Disability

 , , , ,
, , , ,  , and
, and
Abstract
1. Introduction
2. Experimental Section
2.1. Study Population
2.2. Clinical Assessment
2.3. Sample Collection
2.4. Tissue Processing
2.5. Flow Cytometry Analyses of Cell Surface Markers
2.6. Statistical Analyses
3. Results
3.1. Clinical Characteristics of the Study Population
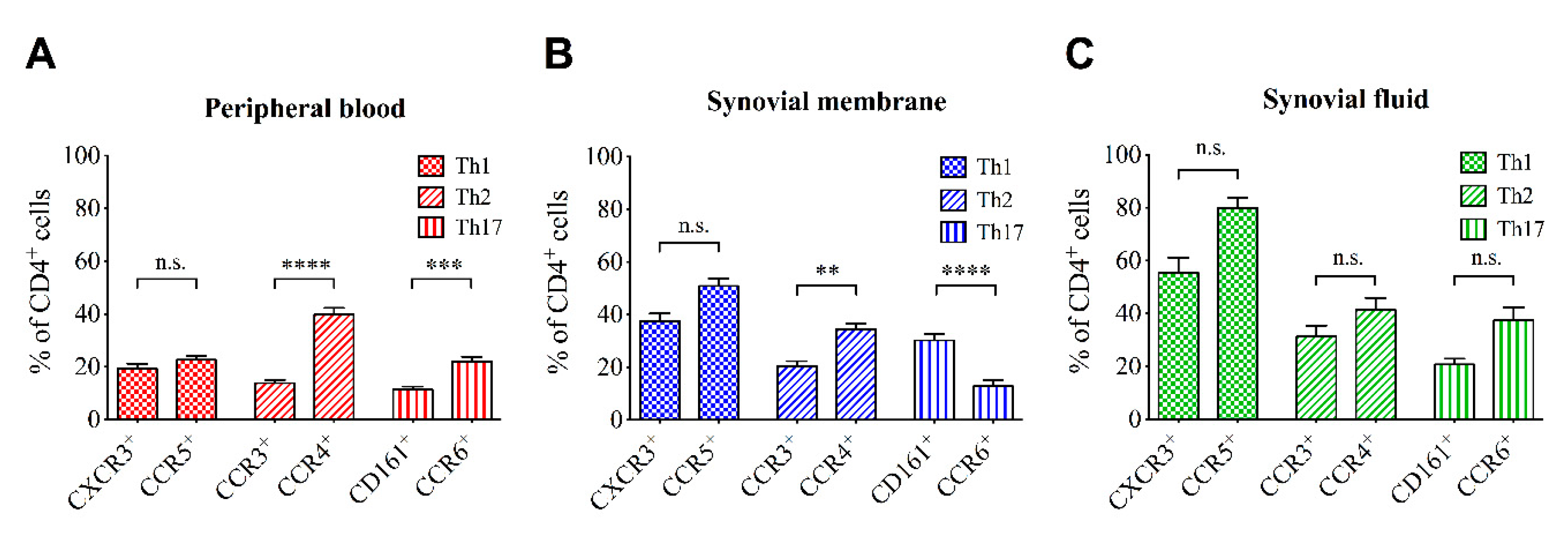
3.2. T Cell Profile in in OA Joints and Peripheral Blood
3.3. Correlation of Cell Infiltration and Clinical Parameters
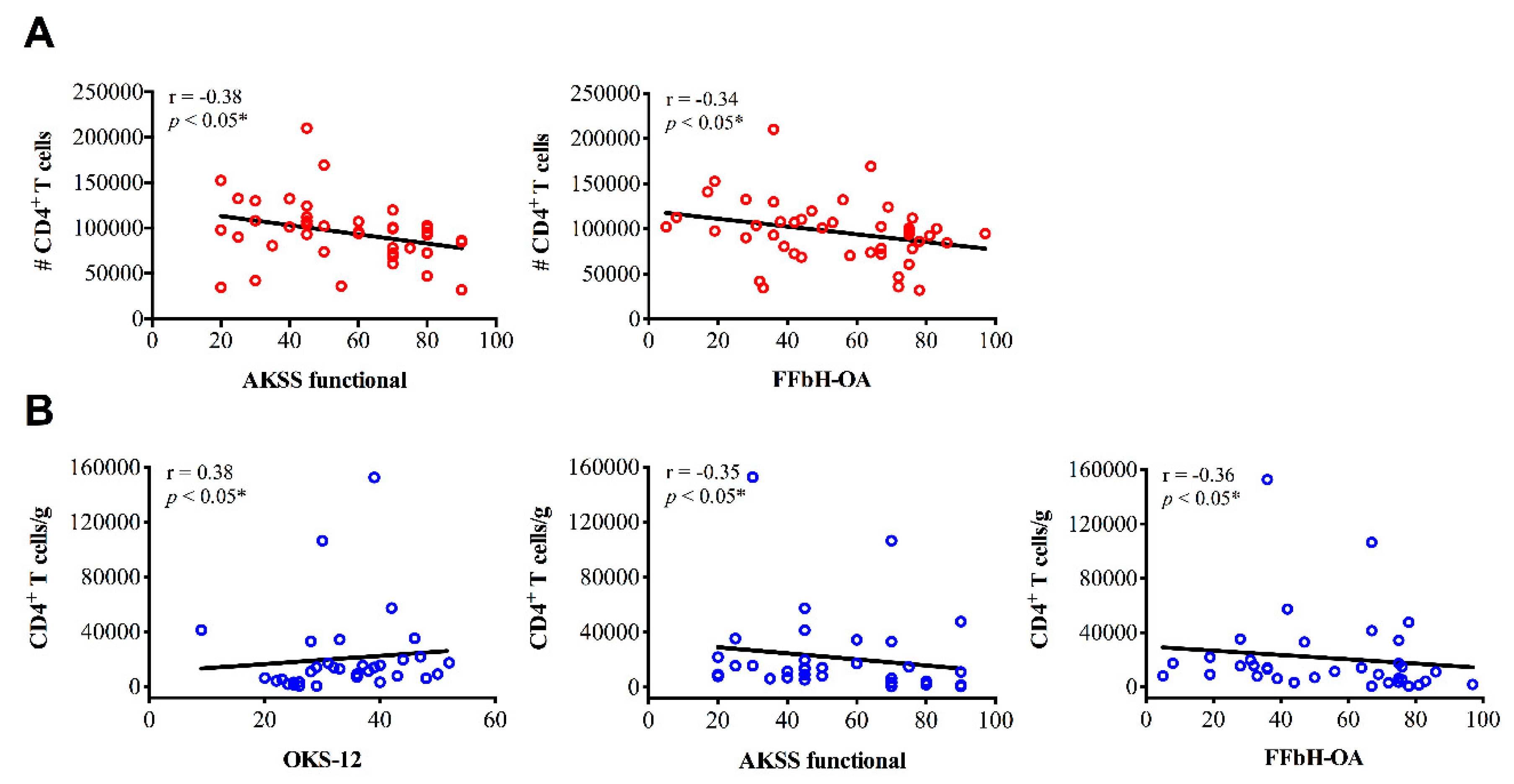
3.3.1. CD4+ Cell Infiltration and Clinical Parameters
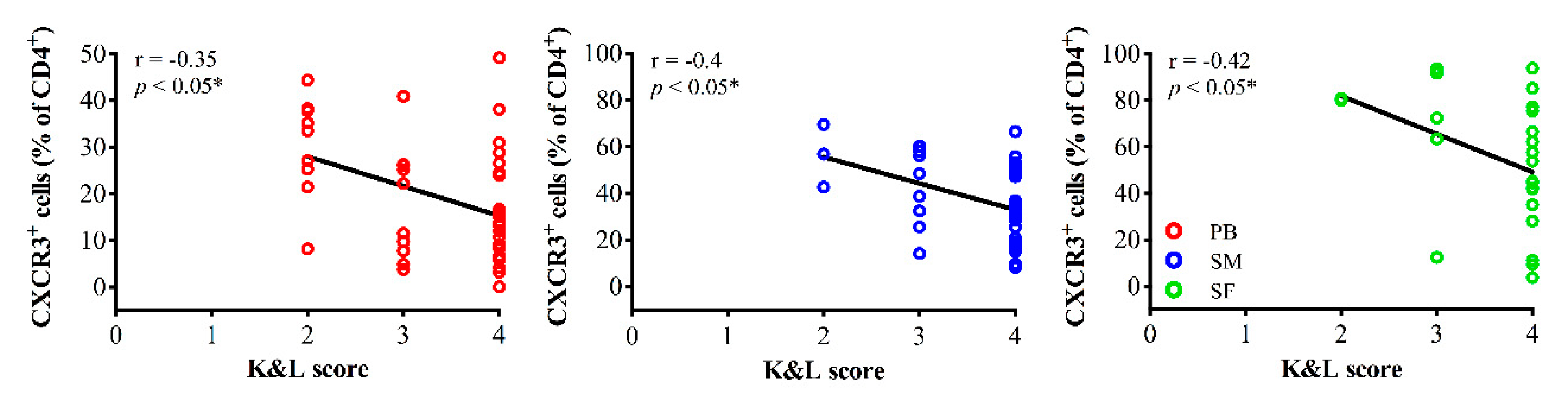
3.3.2. Th1 Cell Infiltration and Clinical Parameters
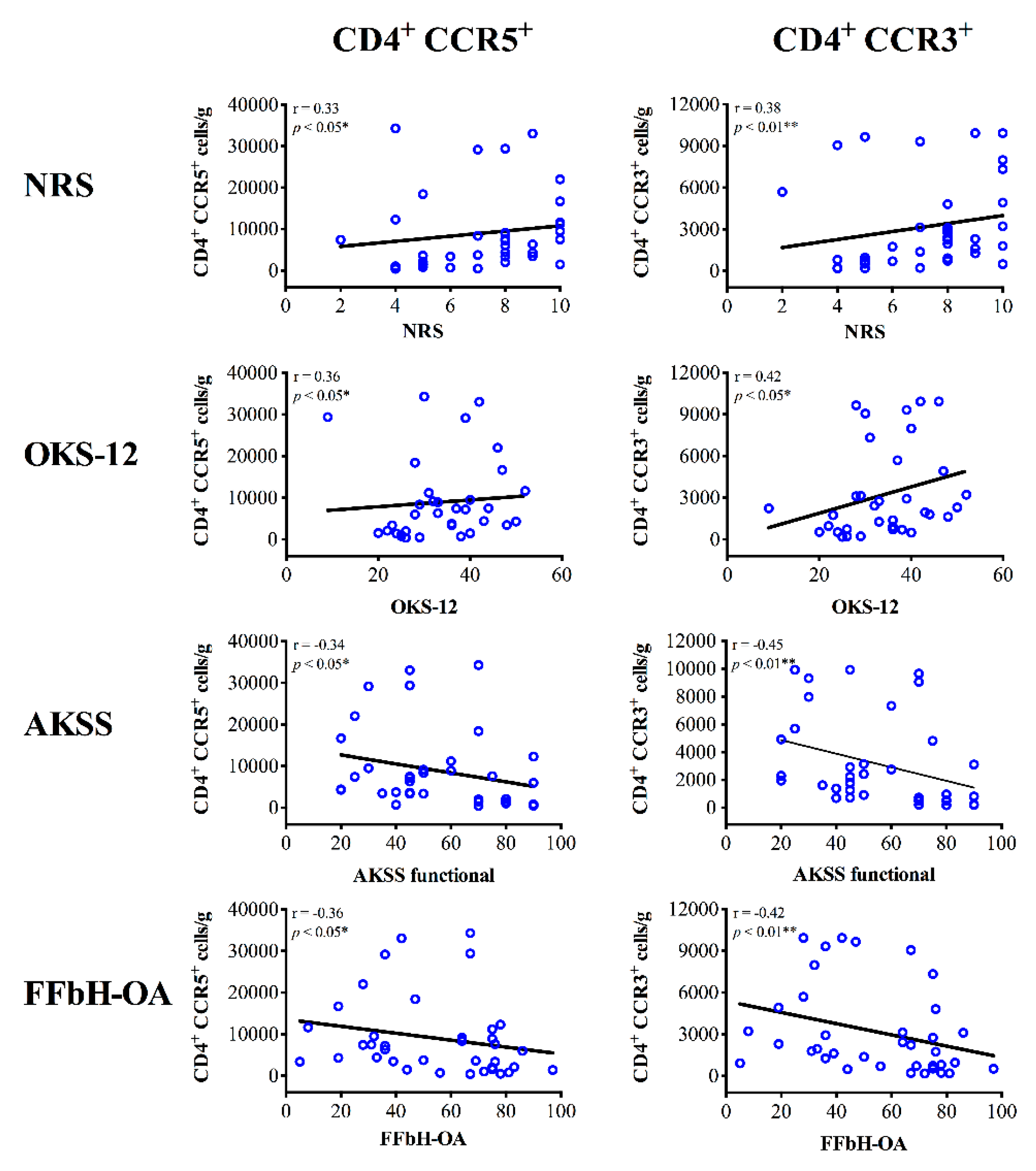
3.3.3. Th2 Cell Infiltration and Clinical Parameters
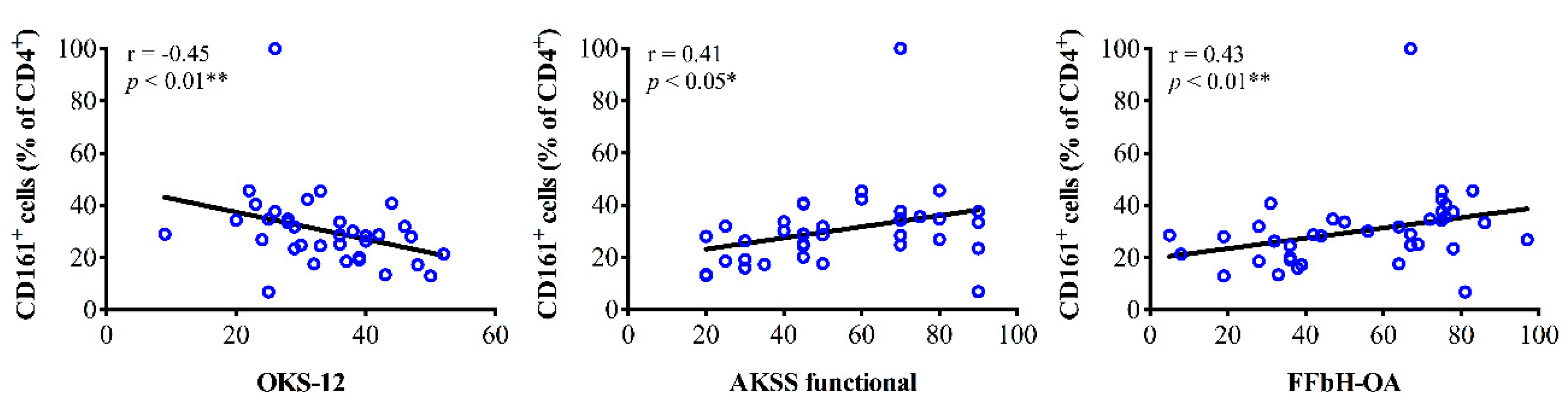
3.3.4. Th17 Cell Infiltration and Clinical Parameters
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Hay, S.I.; Abajobir, A.A.; Abate, K.H.; Abbafati, C.; Abbas, K.M.; Abd-Allah, F.; Abdulkader, R.S.; Abdulle, A.M.; Abebo, T.A.; Abera, S.F.; et al. Global, regional, and national disability-adjusted life-years (DALYs) for 333 diseases and injuries and healthy life expectancy (HALE) for 195 countries and territories, 1990–2016: A systematic analysis for the global burden of disease study 2016. Lancet 2017, 390, 1260–1344. [Google Scholar] [CrossRef]
- Robinson, W.H.; Lepus, C.M.; Wang, Q.; Raghu, H.; Mao, R.; Lindstrom, T.M.; Sokolove, J. Low-Grade inflammation as a key mediator of the pathogenesis of osteoarthritis. Nat. Rev. Rheumatol. 2016, 12, 580–592. [Google Scholar] [CrossRef]
- Bondeson, J.; Wainwright, S.D.; Lauder, S.; Amos, N.; Hughes, C.E. The role of synovial macrophages and macrophage-produced cytokines in driving aggrecanases, matrix metalloproteinases, and other destructive and inflammatory responses in osteoarthritis. Arthritis Res. 2006, 8, R187. [Google Scholar] [CrossRef]
- Roemer, F.W.; Guermazi, A.; Felson, D.T.; Niu, J.; Nevitt, M.C.; Crema, M.D.; Lynch, J.A.; Lewis, C.E.; Torner, J.; Zhang, Y. Presence of MRI-detected joint effusion and synovitis increases the risk of cartilage loss in knees without osteoarthritis at 30-month follow-up: The MOST study. Ann. Rheum. Dis. 2011, 70, 1804–1809. [Google Scholar] [CrossRef]
- Wang, Q.; Rozelle, A.L.; Lepus, C.M.; Scanzello, C.R.; Song, J.J.; Larsen, D.M.; Crish, J.F.; Bebek, G.; Ritter, S.Y.; Lindstrom, T.M.; et al. Identification of a central role for complement in osteoarthritis. Nat. Med. 2011, 17, 1674–1679. [Google Scholar] [CrossRef] [PubMed]
- Nees, T.A.; Rosshirt, N.; Zhang, J.A.; Reiner, T.; Sorbi, R.; Tripel, E.; Walker, T.; Schiltenwolf, M.; Hagmann, S.; Moradi, B. Synovial cytokines significantly correlate with osteoarthritis-related knee pain and disability: Inflammatory mediators of potential clinical relevance. J. Clin. Med. 2019, 8, 1343. [Google Scholar] [CrossRef]
- Leung, Y.Y.; Huebner, J.L.; Haaland, B.; Wong, S.B.S.; Kraus, V.B. Synovial fluid pro-inflammatory profile differs according to the characteristics of knee pain. Osteoarthr. Cartil. 2017, 25, 1420–1427. [Google Scholar] [CrossRef] [PubMed]
- Orita, S.; Koshi, T.; Mitsuka, T.; Miyagi, M.; Inoue, G.; Arai, G.; Ishikawa, T.; Hanaoka, E.; Yamashita, K.; Yamashita, M.; et al. Associations between proinflammatory cytokines in the synovial fluid and radiographic grading and pain-related scores in 47 consecutive patients with osteoarthritis of the knee. BMC Musculoskelet. Disord. 2011, 12, 144. [Google Scholar] [CrossRef]
- Radojcic, M.R.; Thudium, C.S.; Henriksen, K.; Tan, K.; Karlsten, R.; Dudley, A.; Chessell, I.; Karsdal, M.A.; Bay-Jensen, A.C.; Crema, M.D.; et al. Biomarker of extracellular matrix remodelling C1M and proinflammatory cytokine interleukin 6 are related to synovitis and pain in end-stage knee osteoarthritis patients. Pain 2017, 158, 1254–1263. [Google Scholar] [CrossRef]
- Ren, G.; Lutz, I.; Railton, P.; Wiley, J.P.; McAllister, J.; Powell, J.; Krawetz, R.J. Serum and synovial fluid cytokine profiling in hip osteoarthritis: Distinct from knee osteoarthritis and correlated with pain. BMC Musculoskelet. Disord. 2018, 19, 39. [Google Scholar] [CrossRef] [PubMed]
- Bondeson, J.; Blom, A.B.; Wainwright, S.; Hughes, C.; Caterson, B.; van den Berg, W.B. The role of synovial macrophages and macrophage-produced mediators in driving inflammatory and destructive responses in osteoarthritis. Arthritis Rheum. 2010, 62, 647–657. [Google Scholar] [CrossRef] [PubMed]
- Moradi, B.; Rosshirt, N.; Tripel, E.; Kirsch, J.; Barie, A.; Zeifang, F.; Gotterbarm, T.; Hagmann, S. Unicompartmental and bicompartmental knee osteoarthritis show different patterns of mononuclear cell infiltration and cytokine release in the affected joints. Clin. Exp. Immunol. 2015, 180, 143–154. [Google Scholar] [CrossRef] [PubMed]
- Moradi, B.; Schnatzer, P.; Hagmann, S.; Rosshirt, N.; Gotterbarm, T.; Kretzer, J.P.; Thomsen, M.; Lorenz, H.M.; Zeifang, F.; Tretter, T. CD4(+)CD25(+)/highCD127low/(-) regulatory T cells are enriched in rheumatoid arthritis and osteoarthritis joints—Analysis of frequency and phenotype in synovial membrane, synovial fluid and peripheral blood. Arthritis Res. Ther. 2014, 16, R97. [Google Scholar] [CrossRef] [PubMed]
- Rosshirt, N.; Hagmann, S.; Tripel, E.; Gotterbarm, T.; Kirsch, J.; Zeifang, F.; Lorenz, H.M.; Tretter, T.; Moradi, B. A predominant Th1 polarization is present in synovial fluid of end-stage osteoarthritic knee joints: Analysis of peripheral blood, synovial fluid and synovial membrane. Clin. Exp. Immunol. 2019, 195, 395–406. [Google Scholar] [CrossRef]
- Haynes, M.K.; Hume, E.L.; Smith, J.B. Phenotypic characterization of inflammatory cells from osteoarthritic synovium and synovial fluids. Clin. Immunol. 2002, 105, 315–325. [Google Scholar] [CrossRef]
- Oehler, S.; Neureiter, D.; Meyer-Scholten, C.; Aigner, T. Subtyping of osteoarthritic synoviopathy. Clin. Exp. Rheumatol. 2002, 20, 633–640. [Google Scholar]
- Li, Y.S.; Luo, W.; Zhu, S.A.; Lei, G.H. T cells in osteoarthritis: Alterations and beyond. Front. Immunol. 2017, 8, 356. [Google Scholar] [CrossRef]
- Symons, J.A.; McCulloch, J.F.; Wood, N.C.; Duff, G.W. Soluble CD4 in patients with rheumatoid arthritis and osteoarthritis. Clin. Immunol. Immunopathol. 1991, 60, 72–82. [Google Scholar] [CrossRef]
- van de Putte, L.B.; Meijer, C.J.; Lafeber, G.J.; Kleinjan, R.; Cats, A. Lymphocytes in rheumatoid and nonrheumatoid synovial fluids. Nonspecificity of high T-cell and low B-cell percentages. Ann. Rheum. Dis. 1975, 35, 451–455. [Google Scholar] [CrossRef]
- Kellgren, J.H.; Lawrence, J.S. Radiological assessment of osteo-arthrosis. Ann. Rheum. Dis. 1957, 16, 494–502. [Google Scholar] [CrossRef]
- Naal, F.D.; Impellizzeri, F.M.; Sieverding, M.; Loibl, M.; von Knoch, F.; Mannion, A.F.; Leunig, M.; Munzinger, U. The 12-item Oxford knee score: Cross-Cultural adaptation into German and assessment of its psychometric properties in patients with osteoarthritis of the knee. Osteoarthr. Cartil. 2009, 17, 49–52. [Google Scholar] [CrossRef] [PubMed]
- Insall, J.N.; Dorr, L.D.; Scott, R.D.; Scott, W.N. Rationale of the knee society clinical rating system. Clin. Orthop. Relat. Res. 1989, 13–14. [Google Scholar] [CrossRef]
- Kohlmann, T.; Richter, T.; Heinrichs, K.; Peschel, U.; Knahr, K.; Kryspin-Exner, I. Entwicklung und validierung des funktionsfragebogens hannover für patienten mit arthrosen der hüft-und kniegelenke (FFbH-OA). Drv-Schr. Bd 1999, 12, 40–42. [Google Scholar]
- Grieshaber-Bouyer, R.; Kammerer, T.; Rosshirt, N.; Nees, T.A.; Koniezke, P.; Tripel, E.; Schiltenwolf, M.; Kirsch, J.; Hagmann, S.; Moradi, B. Divergent mononuclear cell participation and cytokine release profiles define hip andknee osteoarthritis. J. Clin. Med. 2019, 8, 1631. [Google Scholar] [CrossRef]
- Nees, T.A.; Rosshirt, N.; Reiner, T.; Schiltenwolf, M.; Moradi, B. Inflammation and osteoarthritis-related pain. Schmerz 2019, 33, 4–12. [Google Scholar] [CrossRef]
- Chen, J.; Vistica, B.P.; Takase, H.; Ham, D.I.; Fariss, R.N.; Wawrousek, E.F.; Chan, C.C.; DeMartino, J.A.; Farber, J.M.; Gery, I. A unique pattern of up- and down-regulation of chemokine receptor CXCR3 on inflammation-inducing Th1 cells. Eur. J. Immunol. 2004, 34, 2885–2894. [Google Scholar] [CrossRef]
- Kim, C.H.; Rott, L.; Kunkel, E.J.; Genovese, M.C.; Andrew, D.P.; Wu, L.; Butcher, E.C. Rules of chemokine receptor association with T cell polarization in vivo. J. Clin. Investig. 2001, 108, 1331–1339. [Google Scholar] [CrossRef]
- Doodes, P.D.; Cao, Y.; Hamel, K.M.; Wang, Y.; Rodeghero, R.L.; Kobezda, T.; Finnegan, A. CCR5 is involved in resolution of inflammation in proteoglycan-induced arthritis. Arthritis Rheum. 2009, 60, 2945–2953. [Google Scholar] [CrossRef]
- Issekutz, A.C.; Quinn, P.J.; Lang, B.; Ramsey, S.; Huber, A.M.; Rowter, D.; Karkada, M.; Issekutz, T.B. Coexpression of chemokine receptors CCR5, CXCR3, and CCR4 and ligands for P- and E-selectin on T lymphocytes of patients with juvenile idiopathic arthritis. Arthritis Rheum. 2011, 63, 3467–3476. [Google Scholar] [CrossRef]
- Xie, J.H.; Nomura, N.; Lu, M.; Chen, S.L.; Koch, G.E.; Weng, Y.; Rosa, R.; Di Salvo, J.; Mudgett, J.; Peterson, L.B.; et al. Antibody-Mediated blockade of the CXCR3 chemokine receptor results in diminished recruitment of T helper 1 cells into sites of inflammation. J. Leukoc. Biol. 2003, 73, 771–780. [Google Scholar] [CrossRef]
- Wedderburn, L.R.; Robinson, N.; Patel, A.; Varsani, H.; Woo, P. Selective recruitment of polarized T cells expressing CCR5 and CXCR3 to the inflamed joints of children with juvenile idiopathic arthritis. Arthritis Rheum. 2000, 43, 765–774. [Google Scholar] [CrossRef]
- Julià, E.; Edo, M.C.; Horga, A.; Montalban, X.; Comabella, M. Differential susceptibility to apoptosis of CD4+T cells expressing CCR5 and CXCR3 in patients with MS. Clin. Immunol. 2009, 133, 364–374. [Google Scholar] [CrossRef] [PubMed]
- Potestio, M.; D’Agostino, P.; Romano, G.C.; Milano, S.; Ferlazzo, V.; Aquino, A.; Di Bella, G.; Caruso, R.; Gambino, G.; Vitale, G.; et al. CD4+ CCR5+ and CD4+ CCR3+ lymphocyte subset and monocyte apoptosis in patients with acute visceral leishmaniasis. Immunology 2004, 113, 260–268. [Google Scholar] [CrossRef] [PubMed]
- Sallusto, F.; Mackay, C.R.; Lanzavecchia, A. Selective expression of the eotaxin receptor CCR3 by human T helper 2 cells. Science 1997, 277, 2005–2007. [Google Scholar] [CrossRef] [PubMed]
- Rivino, L.; Messi, M.; Jarrossay, D.; Lanzavecchia, A.; Sallusto, F.; Geginat, J. Chemokine receptor expression identifies Pre-T helper (Th)1, Pre-Th2, and nonpolarized cells among human CD4+ central memory T cells. J. Exp. Med. 2004, 200, 725–735. [Google Scholar] [CrossRef]
- Bonecchi, R.; Bianchi, G.; Bordignon, P.P.; D’Ambrosio, D.; Lang, R.; Borsatti, A.; Sozzani, S.; Allavena, P.; Gray, P.A.; Mantovani, A.; et al. Differential expression of chemokine receptors and chemotactic responsiveness of type 1 T helper cells (Th1s) and Th2s. J. Exp. Med. 1998, 187, 129–134. [Google Scholar] [CrossRef]
- Loetscher, P.; Uguccioni, M.; Bordoli, L.; Baggiolini, M.; Moser, B.; Chizzolini, C.; Dayer, J.M. CCR5 is characteristic of Th1 lymphocytes. Nature 1998, 391, 344–345. [Google Scholar] [CrossRef]
- Sebastiani, S.; Allavena, P.; Albanesi, C.; Nasorri, F.; Bianchi, G.; Traidl, C.; Sozzani, S.; Girolomoni, G.; Cavani, A. Chemokine receptor expression and function in CD4+ T lymphocytes with regulatory activity. J. Immunol. 2001, 166, 996–1002. [Google Scholar] [CrossRef]
- Chang, X.; Shen, J.; Yang, H.; Xu, Y.; Gao, W.; Wang, J.; Zhang, H.; He, S. Upregulated expression of CCR3 in osteoarthritis and CCR3 mediated activation of fibroblast-like synoviocytes. Cytokine 2016, 77, 211–219. [Google Scholar] [CrossRef]
- Haringman, J.J.; Smeets, T.J.; Reinders-Blankert, P.; Tak, P.P. Chemokine and chemokine receptor expression in paired peripheral blood mononuclear cells and synovial tissue of patients with rheumatoid arthritis, osteoarthritis, and reactive arthritis. Ann. Rheum. Dis. 2006, 65, 294–300. [Google Scholar] [CrossRef]
- Nissinen, R.; Leirisalo-Repo, M.; Tiittanen, M.; Julkunen, H.; Hirvonen, H.; Palosuo, T.; Vaarala, O. CCR3, CCR5, interleukin 4, and interferon-gamma expression on synovial and peripheral T cells and monocytes in patients with rheumatoid arthritis. J. Rheumatol. 2003, 30, 1928–1934. [Google Scholar] [PubMed]
- Katschke, K.J., Jr.; Rottman, J.B.; Ruth, J.H.; Qin, S.; Wu, L.; LaRosa, G.; Ponath, P.; Park, C.C.; Pope, R.M.; Koch, A.E. Differential expression of chemokine receptors on peripheral blood, synovial fluid, and synovial tissue monocytes/macrophages in rheumatoid arthritis. Arthritis Rheum. 2001, 44, 1022–1032. [Google Scholar] [CrossRef]
- Berger, A. Th1 and Th2 responses: What are they? BMJ (Clin. Res. Ed.) 2000, 321, 424. [Google Scholar] [CrossRef] [PubMed]
- Sakkas, L.I.; Scanzello, C.; Johanson, N.; Burkholder, J.; Mitra, A.; Salgame, P.; Katsetos, C.D.; Platsoucas, C.D. T cells and T-cell cytokine transcripts in the synovial membrane in patients with osteoarthritis. Clin. Diagn. Lab. Immunol. 1998, 5, 430–437. [Google Scholar] [CrossRef] [PubMed]
- Dolhain, R.J.; ter Haar, N.T.; Hoefakker, S.; Tak, P.P.; de Ley, M.; Claassen, E.; Breedveld, F.C.; Miltenburg, A.M. Increased expression of interferon (IFN)-gamma together with IFN-gamma receptor in the rheumatoid synovial membrane compared with synovium of patients with osteoarthritis. Br. J. Rheumatol. 1996, 35, 24–32. [Google Scholar] [CrossRef] [PubMed]
- Yamada, H.; Nakashima, Y.; Okazaki, K.; Mawatari, T.; Fukushi, J.-I.; Oyamada, A.; Fujimura, K.; Iwamoto, Y.; Yoshikai, Y. Preferential accumulation of activated Th1 cells not only in rheumatoid arthritis but also in osteoarthritis joints. J. Rheumatol. 2011, 38, 1569–1575. [Google Scholar] [CrossRef]
- Ishii, H.; Tanaka, H.; Katoh, K.; Nakamura, H.; Nagashima, M.; Yoshino, S. Characterization of infiltrating T cells and Th1/Th2-type cytokines in the synovium of patients with osteoarthritis. Osteoarthr. Cartil. 2002, 10, 277–281. [Google Scholar] [CrossRef]
- Hussein, M.R.; Fathi, N.A.; El-Din, A.M.; Hassan, H.I.; Abdullah, F.; Al-Hakeem, E.; Backer, E.A. Alterations of the CD4(+), CD8 (+) T cell subsets, interleukins-1beta, IL-10, IL-17, tumor necrosis factor-alpha and soluble intercellular adhesion molecule-1 in rheumatoid arthritis and osteoarthritis: Preliminary observations. Pathol. Oncol. Res. Por. 2008, 14, 321–328. [Google Scholar] [CrossRef]
- Wojdasiewicz, P.; Poniatowski, L.A.; Szukiewicz, D. The role of inflammatory and anti-inflammatory cytokines in the pathogenesis of osteoarthritis. Mediat. Inflamm. 2014, 2014, 19. [Google Scholar] [CrossRef]
- Schaible, H.G. Mechanisms of chronic pain in osteoarthritis. Curr. Rheumatol. Rep. 2012, 14, 549–556. [Google Scholar] [CrossRef]
- Schaible, H.G.; von Banchet, G.S.; Boettger, M.K.; Brauer, R.; Gajda, M.; Richter, F.; Hensellek, S.; Brenn, D.; Natura, G. The role of proinflammatory cytokines in the generation and maintenance of joint pain. Ann. N. Y. Acad. Sci. 2010, 1193, 60–69. [Google Scholar] [CrossRef] [PubMed]
- Schaible, H.G. Nociceptive neurons detect cytokines in arthritis. Arthritis Res. Ther. 2014, 16, 470. [Google Scholar] [CrossRef] [PubMed]
- Imamura, M.; Ezquerro, F.; Marcon Alfieri, F.; Vilas Boas, L.; Tozetto-Mendoza, T.R.; Chen, J.; Ozcakar, L.; Arendt-Nielsen, L.; Rizzo Battistella, L. Serum levels of proinflammatory cytokines in painful knee osteoarthritis and sensitization. Int. J. Inflamm. 2015, 2015, 329792. [Google Scholar] [CrossRef] [PubMed]
- Borzi, R.M.; Mazzetti, I.; Marcu, K.B.; Facchini, A. Chemokines in cartilage degradation. Clin. Orthop. Relat. Res. 2004, 427, 53–61. [Google Scholar] [CrossRef]
- Weiss, I.D.; Shoham, H.; Wald, O.; Wald, H.; Beider, K.; Abraham, M.; Barashi, N.; Galun, E.; Nagler, A.; Peled, A. Ccr5 deficiency regulates the proliferation and trafficking of natural killer cells under physiological conditions. Cytokine 2011, 54, 249–257. [Google Scholar] [CrossRef]
- Yuan, G.H.; Masuko-Hongo, K.; Sakata, M.; Tsuruha, J.; Onuma, H.; Nakamura, H.; Aoki, H.; Kato, T.; Nishioka, K. The role of C-C chemokines and their receptors in osteoarthritis. Arthritis Rheum. 2001, 44, 1056–1070. [Google Scholar] [CrossRef]
- Qin, S.; Rottman, J.B.; Myers, P.; Kassam, N.; Weinblatt, M.; Loetscher, M.; Koch, A.E.; Moser, B.; Mackay, C.R. The chemokine receptors CXCR3 and CCR5 mark subsets of T cells associated with certain inflammatory reactions. J. Clin. Investig. 1998, 101, 746–754. [Google Scholar] [CrossRef]
- Haas, C.S.; Martinez, R.J.; Attia, N.; Haines, G.K., 3rd; Campbell, P.L.; Koch, A.E. Chemokine receptor expression in rat adjuvant-induced arthritis. Arthritis Rheum. 2005, 52, 3718–3730. [Google Scholar] [CrossRef]
- Okamoto, H.; Kamatani, N. A CCR-5 antagonist inhibits the development of adjuvant arthritis in rats. Rheumatology (Oxf. Engl.) 2006, 45, 230–232. [Google Scholar] [CrossRef]
- Shahrara, S.; Proudfoot, A.E.; Woods, J.M.; Ruth, J.H.; Amin, M.A.; Park, C.C.; Haas, C.S.; Pope, R.M.; Haines, G.K.; Zha, Y.Y.; et al. Amelioration of rat adjuvant-induced arthritis by Met-RANTES. Arthritis Rheum. 2005, 52, 1907–1919. [Google Scholar] [CrossRef]
- Suzuki, N.; Nakajima, A.; Yoshino, S.; Matsushima, K.; Yagita, H.; Okumura, K. Selective accumulation of CCR5+ T lymphocytes into inflamed joints of rheumatoid arthritis. Int. Immunol. 1999, 11, 553–559. [Google Scholar] [CrossRef]
- Szabo, I.; Chen, X.H.; Xin, L.; Adler, M.W.; Howard, O.M.; Oppenheim, J.J.; Rogers, T.J. Heterologous desensitization of opioid receptors by chemokines inhibits chemotaxis and enhances the perception of pain. Proc. Natl. Acad. Sci. USA 2002, 99, 10276–10281. [Google Scholar] [CrossRef] [PubMed]
- Sun, S.; Chen, D.; Lin, F.; Chen, M.; Yu, H.; Hou, L.; Li, C. Role of interleukin-4, the chemokine CCL3 and its receptor CCR5 in neuropathic pain. Mol. Immunol. 2016, 77, 184–192. [Google Scholar] [CrossRef] [PubMed]
- Richter, F.; Natura, G.; Loser, S.; Schmidt, K.; Viisanen, H.; Schaible, H.G. Tumor necrosis factor causes persistent sensitization of joint nociceptors to mechanical stimuli in rats. Arthritis Rheum. 2010, 62, 3806–3814. [Google Scholar] [CrossRef]
- Brenn, D.; Richter, F.; Schaible, H.G. Sensitization of unmyelinated sensory fibers of the joint nerve to mechanical stimuli by interleukin-6 in the rat: An inflammatory mechanism of joint pain. Arthritis Rheum. 2007, 56, 351–359. [Google Scholar] [CrossRef] [PubMed]
- Tang, C.H.; Hsu, C.J.; Fong, Y.C. The CCL5/CCR5 axis promotes interleukin-6 production in human synovial fibroblasts. Arthritis Rheum. 2010, 62, 3615–3624. [Google Scholar] [CrossRef] [PubMed]
- Benigni, G.; Dimitrova, P.; Antonangeli, F.; Sanseviero, E.; Milanova, V.; Blom, A.; van Lent, P.; Morrone, S.; Santoni, A.; Bernardini, G. CXCR3/CXCL10 axis regulates neutrophil-NK cell cross-talk determining the severity of experimental osteoarthritis. J. Immunol. 2017, 198, 2115–2124. [Google Scholar] [CrossRef]
- Qi, C.; Shan, Y.; Wang, J.; Ding, F.; Zhao, D.; Yang, T.; Jiang, Y. Circulating T helper 9 cells and increased serum interleukin-9 levels in patients with knee osteoarthritis. Clin. Exp. Pharmacol. Physiol. 2016, 43, 528–534. [Google Scholar] [CrossRef]
- Pesenacker, A.M.; Bending, D.; Ursu, S.; Wu, Q.; Nistala, K.; Wedderburn, L.R. CD161 defines the subset of FoxP3+ T cells capable of producing proinflammatory cytokines. Blood 2013, 121, 2647–2658. [Google Scholar] [CrossRef]
- Fergusson, J.R.; Fleming, V.M.; Klenerman, P. CD161-expressing human T cells. Front. Immunol. 2011, 2, 36. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Total Study Population | UC OA | BC OA | |
|---|---|---|---|
| Number of patients, n | 47 | 17 | 30 |
| Gender, n (%) | |||
| Male | 12 (25.5%) | 3 (17.6%) | 9 (30.0%) |
| Female | 35 (74.5%) | 14 (82.4%) | 21 (70.0%) |
| Age, years | 67.5 ± 8.7 (47–83) | 65.4 ± 8.1 (49–76) | 68.7 ± 9 (47–83) |
| BMI (kg/m2) | 29.8 ± 6.2 (20.3–50.1) | 30.0 ± 7.1 (20.8–46.1) | 29.7 ± 5.8 (20.3–50.1) |
| K&L score, n (%) | |||
| 2 | 9 (19.1%) | 8 (47.1%) | 1 (3.3%) |
| 3 | 10 (21.3%) | 7 (41.2%) | 3 (10.0%) |
| 4 | 28 (59.6%) | 2 (11.8%) | 26 (86.7%) |
| Knee pain, NRS (0–10) | 7.2 ± 2.1 (2.0–10.0) | 6.9 ± 1.6 (4.0–10.0) | 7.3 ± 2.3 (2.0–10.0) |
| OKS-12 (Pt.) | 33.8 ± 9.0 (9.0–52.00) | 34.5 ± 4.5 (26.0–43.0) | 34.6 ± 10 (9.0–52.00) |
| AKSS | |||
| Knee score (Pt.) | 42.8 ± 15.2 (14.0–73.0) | 48.5 ± 14.5 (18.0–73.0) | 39.4 ± 14.9 (14.0–70.0) |
| Functional score (Pt.) | 56.6 ± 21.5 (20.0–90.0) | 62.8 ± 22.9 (20.0–90.0) | 53.0 ± 20.2 (20.0–90.0) |
| FFbH-OA (%) | 54.5 ± 23.0 (5.0–97.0) | 60.9 ± 19.0 (28.0–86.0) | 50.8 ± 24.6 (5.0–97.0) |
| T Cells | PB | SM | SF | p-Value | ||
|---|---|---|---|---|---|---|
| Mean ± SEM | Mean ± SEM | Mean ± SEM | PB:SM | PB:SF | SM:SF | |
| CD3+ | ||||||
| Cell count | 122,996 ± 5907 | 76,883 ± 16,445 | 15,553 ± 4448 | **** <0.0001 | **** <0.0001 | ** <0.01 |
| Cells/mL (g) | 15,249 ± 960.1 | 28,243 ± 6052 | 2026 ± 450.1 | n.s. | **** <0.0001 | **** <0.0001 |
| CD4+ | ||||||
| Cell count | 96,798 ± 5141 | 58,010 ± 13,322 | 7453 ± 2626 | **** <0.0001 | **** <0.0001 | *** <0.001 |
| Cells/mL (g) | 12,034 ± 832.7 | 21,301 ± 4935 | 820.7 ± 218.3 | n.s. | **** <0.0001 | **** <0.0001 |
| % of CD3+ cells | 78.45 ± 1.39 | 71.64 ± 1.66 | 42.03± 3.3 | * <0.05 | **** <0.0001 | **** <0.0001 |
| Th1 | ||||||
| CD4+ CXCR3+ | ||||||
| Cell count | 18,562 ± 2153 | 19,372 ± 3846 | 3879 ± 1499 | n.s. | **** <0.0001 | **** <0.0001 |
| Cells/mL (g) | 2449 ± 336.8 | 7253 ± 1484 | 442.6 ± 147.7 | * <0.05 | **** <0.0001 | **** <0.0001 |
| % of CD4+ cells | 19.26 ± 1.88 | 37.57 ± 2.93 | 55.34 ± 5.73 | *** <0.001 | **** <0.0001 | n.s. |
| CD4+ CCR5+ | ||||||
| Cell count | 21,256 ± 1603 | 25,224 ± 4756 | 6757 ± 2499 | n.s. | **** <0.0001 | *** <0.001 |
| Cells/mL (g) | 2624 ± 220.0 | 9041 ± 1553 | 709.9 ± 202.6 | ** <0.01 | **** <0.0001 | **** <0.0001 |
| % of CD4+ cells | 22.67 ± 1.5 | 50.90 ± 2.81 | 79.77 ± 4.03 | **** <0.0001 | **** <0.0001 | ** <0.01 |
| CD4+ CXCR3+ CCR5+ | ||||||
| Cell count | 1683 ± 317.0 | 2055 ± 552.5 | 92.68 ± 18.15 | n.s. | **** <0.0001 | **** <0.0001 |
| Cells/mL (g) | 199.8 ± 37.7 | 836.2 ± 276.3 | 12.50 ± 3.4 | * <0.05 | **** <0.0001 | **** <0.0001 |
| % of CD4+ cells | 1.61 ± 0.27 | 5.11 ± 1.43 | 4.76 ± 1.50 | **** <0.0001 | n.s. | n.s. |
| Th2 | ||||||
| CD4+ CCR3+ | ||||||
| Cell count | 13,223 ± 1253 | 8880 ± 1586 | 2052 ± 862.6 | * <0.05 | **** <0.0001 | *** <0.001 |
| Cells/mL (g) | 1655 ± 182.3 | 3181 ± 523.5 | 208.1 ± 59.13 | n.s. | **** <0.0001 | **** <0.0001 |
| % of CD4+ cells | 13.88 ± 1.07 | 20.37 ± 1.96 | 31.34 ± 4.10 | * <0.05 | **** <0.0001 | n.s. |
| CD4+ CCR4+ | ||||||
| Cell count | 37,538 ± 3002 | 17,255 ± 3635 | 2080 ± 633 | *** <0.001 | **** <0.0001 | *** <0.001 |
| Cells/mL (g) | 4738 ± 503.8 | 6310 ± 1371 | 239.8 ± 53.83 | n.s. | **** <0.0001 | **** <0.0001 |
| % of CD4+ cells | 39.80 ± 2.54 | 34.35 ± 2.25 | 41.40 ± 4.49 | n.s. | n.s. | n.s. |
| CD4+ CCR3+ CCR4+ | ||||||
| Cell count | 1635 ± 146.6 | 1206 ± 303.1 | 182.8 ± 38.4 | *** <0.001 | **** <0.0001 | *** <0.001 |
| Cells/mL (g) | 204.5 ± 21.1 | 425.3 ± 101.7 | 25.07 ± 6.02 | n.s. | **** <0.0001 | **** <0.0001 |
| % of CD4+ cells | 1.74 ± 0.14 | 2.27 ± 0.38 | 8.62 ± 2.46 | n.s. | *** <0.001 | ** <0.01 |
| Th17 | ||||||
| CD4+ CD161+ | ||||||
| Cell count | 9008 ± 708.4 | 5479 ± 1529 | 1132 ± 468.2 | *** <0.001 | **** <0.0001 | ** <0.01 |
| Cells/mL (g) | 1288 ± 128.6 | 882.7 ± 248.7 | 131 ± 93.14 | ** <0.01 | **** <0.0001 | ** <0.01 |
| % of CD4+ cells | 11.42 ± 1.13 | 30.22 ± 2.41 | 20.73 ± 2.22 | **** <0.0001 | *** <0.001 | n.s. |
| CD4+ CCR6+ | ||||||
| Cell count | 20,035 ± 2189 | 1937 ± 574.5 | 3203 ± 1757 | **** <0.0001 | **** <0.0001 | n.s. |
| Cells/mL (g) | 2844 ± 385.7 | 334.9 ± 112.6 | 211.8 ± 134.9 | **** <0.0001 | **** <0.0001 | n.s. |
| % of CD4+ cells | 21.98 ± 1.83 | 12.79 ± 2.36 | 37.49 ± 4.86 | ** <0.01 | n.s. | **** <0.0001 |
| CD4+ CD161+ CCR6+ | ||||||
| Cell count | 8128 ± 840.7 | 2253 ± 723.1 | 761.5 ± 353.3 | **** <0.0001 | **** <0.0001 | n.s. |
| Cells/mL (g) | 1200 ± 161.4 | 329.3 ± 89.58 | 91.90 ± 71.78 | *** <0.001 | **** <0.0001 | n.s. |
| % of CD4+ cells | 8.49 ± 0.68 | 11.16 ± 0.7551 | 10.92 ± 1.49 | n.s. | n.s. | n.s. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nees, T.A.; Rosshirt, N.; Zhang, J.A.; Platzer, H.; Sorbi, R.; Tripel, E.; Reiner, T.; Walker, T.; Schiltenwolf, M.; Lorenz, H.-M.; et al. T Helper Cell Infiltration in Osteoarthritis-Related Knee Pain and Disability. J. Clin. Med. 2020, 9, 2423. https://doi.org/10.3390/jcm9082423
Nees TA, Rosshirt N, Zhang JA, Platzer H, Sorbi R, Tripel E, Reiner T, Walker T, Schiltenwolf M, Lorenz H-M, et al. T Helper Cell Infiltration in Osteoarthritis-Related Knee Pain and Disability. Journal of Clinical Medicine. 2020; 9(8):2423. https://doi.org/10.3390/jcm9082423
Chicago/Turabian StyleNees, Timo Albert, Nils Rosshirt, Jiji Alexander Zhang, Hadrian Platzer, Reza Sorbi, Elena Tripel, Tobias Reiner, Tilman Walker, Marcus Schiltenwolf, Hanns-Martin Lorenz, and et al. 2020. "T Helper Cell Infiltration in Osteoarthritis-Related Knee Pain and Disability" Journal of Clinical Medicine 9, no. 8: 2423. https://doi.org/10.3390/jcm9082423
APA StyleNees, T. A., Rosshirt, N., Zhang, J. A., Platzer, H., Sorbi, R., Tripel, E., Reiner, T., Walker, T., Schiltenwolf, M., Lorenz, H.-M., Tretter, T., Moradi, B., & Hagmann, S. (2020). T Helper Cell Infiltration in Osteoarthritis-Related Knee Pain and Disability. Journal of Clinical Medicine, 9(8), 2423. https://doi.org/10.3390/jcm9082423