Skin Phototype Could Be a Risk Factor for Multiple Sclerosis

 ,
,  ,
,
Abstract
1. Introduction
2. Experimental Section
2.1. Study Design and Subjects
2.2. Serum Concentration of 25-Hydroxy Vitamin D
2.3. Skin Phototype Classification
2.4. Exposure to Sun
2.5. Smoking Habit
2.6. HLA Typing
2.7. Statistical Analysis
3. Results
3.1. Vitamin D and Skin Tone
3.2. Smoking Habits
3.3. HLA Typing
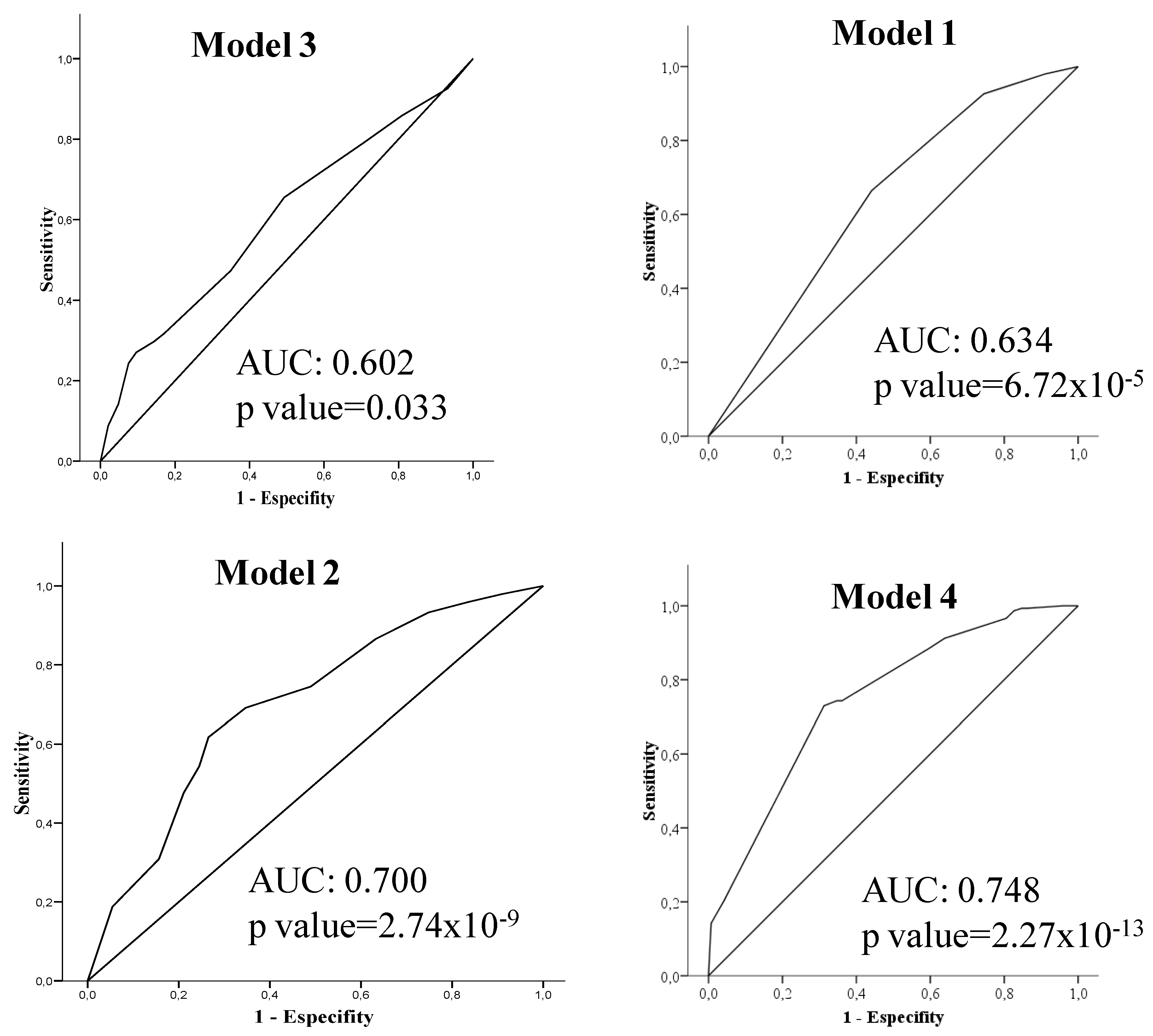
3.4. Multifactorial Model
3.5. Accumulative Risk Model
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Waubant, E.; Lucas, R.; Mowry, E.; Graves, J.; Olsson, T.; Alfredsson, L.; Langer-Gould, A. Environmental and genetic risk factors for MS: An integrated review. Ann. Clin. Transl. Neurol. 2019, 6, 1905–1922. [Google Scholar] [CrossRef] [PubMed]
- Moutsianas, L.; Jostins, L.; Beecham, A.H.; Dilthey, A.T.; Xifara, D.K.; Ban, M.; Shah, T.S.; Patsopoulos, N.A.; Alfredsson, L.; Anderson, C.A.; et al. Class II HLA interactions modulate genetic risk for multiple sclerosis. Nat. Genet. 2015, 47, 1107–1113. [Google Scholar] [PubMed]
- International Multiple Sclerosis Genetics Consortium. The Multiple Sclerosis Genomic Map: Role of peripheral immune cells and resident microglia in susceptibility. Science 2019, 465, eaav7188. [Google Scholar]
- Ramagopalan, S.V.; Maugeri, N.J.; Handunnetthi, L.; Lincoln, M.R.; Orton, S.M.; Dyment, D.A.; Deluca, G.C.; Herrera, B.M.; Chao, M.J.; Sadovnick, A.D.; et al. Expression of the multiple sclerosis-associated MHC class II Allele HLA-DRB1*1501 is regulated by vitamin D. PLoS Genet. 2009, 5, e1000369. [Google Scholar] [CrossRef] [PubMed]
- Smolders, J.; Moen, S.M.; Damoiseaux, J.; Huitinga, I.; Holmøy, T. Vitamin D in the healthy and inflamed central nervous system: Access and function. J. Neurol. Sci. 2011, 311, 37–43. [Google Scholar] [CrossRef] [PubMed]
- Bartosik-Psujek, H.; Psujek, M. Vitamin D as an immune modulator in multiple sclerosis. Neurol. Neurochir. Pol. 2019, 53, 113–122. [Google Scholar] [CrossRef] [PubMed]
- Behrens, J.R.; Rasche, L.; Gieß, R.M.; Pfuhl, C.; Wakonig, K.; Freitag, E.; Deuschle, K.; Bellmann-Strobl, J.; Paul, F.; Ruprecht, K.; et al. Low 25-hydroxyvitamin D, but not the bioavailable fraction of 25-hydroxyvitamin D, is a risk factor for multiple sclerosis. Eur. J. Neurol. 2016, 23, 62–67. [Google Scholar] [CrossRef]
- Webb, A.R.; Kazantzidis, A.; Kift, R.C.; Farrar, M.D.; Wilkinson, J.; Rhodes, L.E. Colour Counts: Sunlight and Skin Type as Drivers of Vitamin D Deficiency at UK Latitudes. Nutrients 2018, 10, 457. [Google Scholar] [CrossRef]
- Lucas, R.M.; Ponsonby, A.L.; Dear, K.; Valery, P.C.; Pender, M.P.; Taylor, B.V.; Kilpatrick, T.J.; Dwyer, T.; Coulthard, A.; Chapman, C.; et al. Sun exposure and vitamin D are independent risk factors for CNS demyelination. Neurology 2011, 76, 540–548. [Google Scholar] [CrossRef]
- Dwyer, T.; van der Mei, I.; Ponsonby, A.L.; Taylor, B.V.; Stankovich, J.; McKay, J.D.; Thomson, R.J.; Polanowski, A.M.; Dickinson, J.L. Melanocortin 1 receptor genotype, past environmental sun exposure, and risk of multiple sclerosis. Neurology 2008, 71, 583–589. [Google Scholar] [CrossRef]
- Van der Mei, I.A.; Ponsonby, A.L.; Dwyer, T.; Blizzard, L.; Simmons, R.; Taylor, B.V.; Butzkueven, H.; Kilpatrick, T. Past exposure to sun, skin phenotype, and risk of multiple sclerosis: Case-control study. BMJ 2003, 327, 316. [Google Scholar] [CrossRef] [PubMed]
- Dalmay, F.; Bhalla, D.; Nicoletti, A.; Cabrera-Gomez, J.A.; Cabre, P.; Ruiz, F.; Druet-Cabanac, M.; Dumas, M.; Preux, P.M. Multiple sclerosis and solar exposure before the age of 15 years: Case-control study in Cuba, Martinique and Sicily. Mult Scler. 2010, 16, 899–908. [Google Scholar] [CrossRef] [PubMed]
- Wang, Z.; Xie, J.; Wu, C.; Xiao, G. Correlation Between Smoking and Passive Smoking with Multiple Sclerosis and the Underlying Molecular Mechanisms. Med. Sci. Monit. 2019, 25, 893–902. [Google Scholar] [CrossRef] [PubMed]
- Hedström, A.K.; Sundqvist, E.; Bäärnhielm, M.; Nordin, N.; Hillert, J.; Kockum, I.; Olsson, T.; Alfredsson, L. Smoking and two human leukocyte antigen genes interact to increase the risk for multiple sclerosis. Brain 2011, 134, 653–664. [Google Scholar] [CrossRef]
- Hedström, A.K.; Hillert, J.; Olsson, T.; Alfredsson, L. Smoking and multiple sclerosis susceptibility. Eur. J. Epidemiol. 2013, 28, 867–874. [Google Scholar] [CrossRef]
- Link, J.; Kockum, I.; Lorentzen, A.R.; Lie, B.A.; Celius, E.G.; Westerlind, H.; Schaffer, M.; Alfredsson, L.; Olsson, T.; Brynedal, B.; et al. Importance of human leukocyte antigen (HLA) class I and II alleles on the risk of multiple sclerosis. PLoS ONE 2012, 7, e36779. [Google Scholar] [CrossRef]
- Polman, C.H.; Reingold, S.C.; Banwell, B.; Clanet, M.; Cohen, J.A.; Filippi, M.; Fujihara, K.; Havrdova, E.; Hutchinson, M.; Kappos, L.; et al. Diagnostic criteria for multiple sclerosis: 2010 revisions to the McDonald criteria. Ann. Neurol. 2011, 69, 292–302. [Google Scholar] [CrossRef]
- Fitzpatrick, T.B. The validity and practicality of sun-reactive skin types I through VI. Arch. Dermatol. 1988, 124, 869–871. [Google Scholar] [CrossRef]
- Institute of Medicine (US) Committee to Review Dietary Reference Intakes for Vitamin D and Calcium; Ross, A.C.; Taylor, C.L.; Yaktine, A.L.; Del Valle, H.B. (Eds.) Dietary Reference Intakes for Calcium and Vitamin D; National Academies Press: Washington, DC, USA, 2011. [Google Scholar]
- Munger, K.L.; Levin, L.I.; Hollis, B.W.; Howard, N.S.; Ascherio, A. Serum 25-hydroxyvitamin D levels and risk of multiple sclerosis. JAMA 2006, 296, 2832–2838. [Google Scholar] [CrossRef]
- Bates, D.; Maechler, M.; Bolker, B.; Walker, S. Fitting Linear Mixed-Effects Models Using lme4. J. Stat. Softw. 2015, 67, 1–48. [Google Scholar] [CrossRef]
- R Core Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2019; Available online: https://www.R-project.org/ (accessed on 1 July 2020).
- Robin, X.; Turck, N.; Hainard, A.; Tiberti, N.; Lisacek, F.; Sanchez, J.C.; Müller, M. pROC: An open-source package for R and S+ to analyze and compare ROC curves. BMC Bioinform. 2011, 12, 77. [Google Scholar] [CrossRef] [PubMed]
- Canty, A.; Ripley, B. Boot: Bootstrap R (S-Plus) Functions; R Package Version 1; Cambridge University Press: Cambridge, UK, 2019; pp. 3–23. [Google Scholar]
- Coraddu, F.; Reyes-Yanez, M.P.; Parra, A.; Gray, J.; Smith, S.I.; Taylor, C.J.; Compston, D.A. HLA associations with multiple sclerosis in the Canary Islands. J. Neuroimmunol. 1998, 87, 130–135. [Google Scholar] [CrossRef]
- Atlas Nacional de España, Instituto Geográfico Nacional, Ministerio de Transporte, Movilidad y Agenda urbana. Available online: http://atlasnacional.ign.es/wane/P%C3%A1gina_principal (accessed on 1 June 2020).
- Buchanan, R.J.; Zuniga, M.A.; Carrillo-Zuniga, G.; Chakravorty, B.J.; Tyry, T.; Moreau, R.L.; Huang, C.; Vollmer, T. Comparisons of Latinos, African Americans, and Caucasians with multiple sclerosis. Ethn. Dis. 2010, 20, 451–457. [Google Scholar] [PubMed]
- Rivas-Rodríguez, E.; Amezcua, L. Ethnic Considerations and Multiple Sclerosis Disease Variability in the United States. Neurol. Clin. 2018, 36, 151–162. [Google Scholar] [CrossRef] [PubMed]
- Khan, O.; Williams, M.J.; Amezcua, L.; Javed, A.; Larsen, K.E.; Smrtka, J.M. Multiple sclerosis in US minority populations: Clinical practice insights. Neurol. Clin. Pract. 2015, 5, 132–142. [Google Scholar] [CrossRef] [PubMed]
- Langer-Gould, A.; Brara, S.M.; Beaber, B.E.; Zhang, J.L. Incidence of multiple sclerosis in multiple racial and ethnic groups. Neurology 2013, 80, 1734–1739. [Google Scholar] [CrossRef]
- Langer-Gould, A.; Zhang, J.L.; Chung, J.; Yeung, Y.; Waubant, E.; Yao, J. Incidence of acquired CNS demyelinating syndromes in a multiethnic cohort of children. Neurology 2011, 77, 1143–1148. [Google Scholar] [CrossRef]
- Yao, S.; Hong, C.C.; Bandera, E.V.; Zhu, Q.; Liu, S.; Cheng, T.-Y.D.; Zirpoli, G.; Haddad, S.A.; Lunetta, K.L.; Ruiz-Narvaez, E.A.; et al. Demographic, lifestyle, and genetic determinants of circulating concentrations of 25-hydroxyvitamin D and vitamin D-binding protein in African American and European American women. Am. J. Clin. Nutr. 2017, 105, 1362–1371. [Google Scholar] [CrossRef]
- Looker, A.C.; Dawson-Hughes, B.; Calvo, M.S.; Gunter, E.W.; Sahyoun, N.R. Serum 25-hydroxyvitamin D status of adolescents and adults in two seasonal subpopulations from NHANES III. Bone 2002, 30, 771–777. [Google Scholar] [CrossRef]
- Martinelli, V.; Dalla Costa, G.; Colombo, B.; Dalla Libera, D.; Rubinacci, A.; Filippi, M.; Furlan, R.; Comi, G. Vitamin D levels and risk of multiple sclerosis in patients with clinically isolated syndromes. Mult. Scler. 2014, 20, 147–155. [Google Scholar] [CrossRef]
- Pierrot-Deseilligny, C.; Souberbielle, J.C. Contribution of vitamin D insufficiency to the pathogenesis of multiple sclerosis. Ther. Adv. Neurol. Disord. 2013, 6, 81–116. [Google Scholar] [CrossRef] [PubMed]
- Smolders, J.; Damoiseaux, J.; Menheere, P.; Hupperts, R. Vitamin D as an immune modulator in multiple sclerosis, a review. J. Neuroimmunol. 2008, 194, 7–17. [Google Scholar] [CrossRef] [PubMed]
- Bhargava, P.; Steele, S.U.; Waubant, E.; Revirajan, N.R.; Marcus, J.; Dembele, M.; Cassard, S.D.; Hollis, B.W.; Crainiceanu, C.; Mowry, E.M. Multiple sclerosis patients have a diminished serologic response to vitamin D supplementation compared to healthy controls. Mult. Scler. 2016, 22, 753–760. [Google Scholar] [CrossRef] [PubMed]
- Gianfrancesco, M.A.; Stridh, P.; Rhead, B.; Shao, X.; Xu, E.; Graves, J.S.; Chitnis, T.; Waldman, A.; Lotze, T.; Schreiner, T.; et al. Network of Pediatric Multiple Sclerosis Centers. Evidence for a causal relationship between low vitamin D, high BMI, and pediatric-onset MS. Neurology 2017, 88, 1623–1629. [Google Scholar] [CrossRef]
- Qiu, F.; Liang, C.L.; Liu, H.; Zeng, Y.Q.; Hou, S.; Huang, S.; Lai, X.; Dai, Z. Impacts of cigarette smoking on immune responsiveness: Up and down or upside down? Oncotarget 2017, 8, 268–284. [Google Scholar] [CrossRef]
- Gonçalves, R.B.; Coletta, R.D.; Silverio, K.G.; Benevides, L.; Casati, M.Z.; da Silva, J.S.; Nociti, F.H., Jr. Impact of smoking on inflammation: Overview of molecular mechanisms. Inflamm. Res. 2011, 60, 409–424. [Google Scholar] [CrossRef]
- Perricone, C.; Versini, M.; Ben-Ami, D.; Gertel, S.; Watad, A.; Segel, M.J.; Ceccarelli, F.; Conti, F.; Cantarini, L.; Bogdanos, D.P.; et al. Smoke and autoimmunity: The fire behind the disease. Autoimmun. Rev. 2016, 15, 354–374. [Google Scholar] [CrossRef]
- Hernan, M.A.; Jick, S.S.; Logroscino, G.; Ole-k, M.J.; Ascherio, A.; Jick, H. Cigarette smoking and the progression of multiple sclerosis. Brain 2005, 128, 1461–1465. [Google Scholar] [CrossRef]
- Seo, S.B.; Choe, E.S.; Kim, K.S.; Shim, S.M. The effect of tobacco smoke exposure on the generation of reactive oxygen species and cellular membrane damage using co-culture model of blood brain barrier with astrocytes. Toxicol. Ind. Health 2017, 33, 530–536. [Google Scholar] [CrossRef]
- Jersild, C.; Svejgaard, A.; Fog, T. HL-A antigens and multiple sclerosis. Lancet 1972, 299, 1240–1241. [Google Scholar] [CrossRef]
- Greer, J.M. The Role of HLA in MS Susceptibility and Phenotype. Curr. Top. Behav. Neurosci. 2015, 26, 1–27. [Google Scholar]
- Zahoor, I.; Haq, E. Multiple sclerosis in India: Iceberg or volcano. J. Neuroimmunol. 2017, 307, 27–30. [Google Scholar] [CrossRef] [PubMed]
- Patti, F.; Caserta, C.; Colandonio, S.; Iudica, M.L.; Maimone, D.; Lo Fermo, S.; D’Amico, E.; Chisari, C.; Mayer, F.; Vanacore, N. Prevalence and Incidence of Multiple Sclerosis in the City of Biancavilla. Neuroepidemiology 2019, 53, 108–114. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Women% (n) | Men% (n) | p Value | Patients% (n) | Controls% (n) | p Value | |
|---|---|---|---|---|---|---|
| 25(OH)D deficient | 33.0% (65) | 26.3% (26) | n.s. | 40.3% (60) | 21.1% (31) | 3.50 × 10−4 |
| Light brown skin | 83.6% (163) | 83.8% (83) | n.s. | 92.6% (138) | 74.5% (108) | 2.60 × 10−5 |
| Smokers | 51.0% (100) | 54.5% (54) | n.s. | 69.1% (103) | 34.9% (51) | 4.13 × 10−9 |
| Smokers in Tenerife | 53.3% (32) | 56.4% (22) | n.s. | 73.5% (36) | 36.0% (18) | 1.81 × 10−4 |
| Smokers in Málaga | 45.8% (33) | 64.3% (18) | n.s. | 58.0% (29) | 44.0% (22) | n.s. |
| Smokers in Madrid | 54.7% (35) | 43.8% (14) | n.s. | 76.0% (38) | 23.9% (11) | 3.39 × 10−6 |
| Present HLA-DRB1*15:01 | 24.1% (47) | 25.3% (25) | n.s. | 31.8% (47) | 17.1% (25) | 0.004 |
| OR | IC 95% | p Value | |
|---|---|---|---|
| Model 1 | |||
| Skin tone (Light brown skin vs. pale skin) | 4.40 | 2.13–9.06 | 5.34 × 10−5 |
| Sex (female vs. male) | 1.71 | 1.03–2.83 | 0.037 |
| Model 2 | |||
| Smoking habits (Smoker vs. non−smoker) | 4.39 | 2.67–7.21 | 4.96 × 10−9 |
| Sex (female vs. male) | 1.85 | 1.09–3.12 | 0.023 |
| Province of residence | |||
| Tenerife vs. Madrid | 0.87 | 0.47–1.60 | 0.66 |
| Málaga vs. Madrid | 0.88 | 0.48–1.61 | 0.68 |
| Model 3 | |||
| HLA−DRB1*15:01 (Presence vs. absence) | 2.30 | 1.32–4.02 | 0.003 |
| Sex (female vs. male) | 1.66 | 1.01–2.74 | 0.045 |
| Province of residence | |||
| Tenerife vs. Madrid | 0.95 | 0.54–1.69 | 0.95 |
| Málaga vs. Madrid | 0.89 | 0.50–1.59 | 0.70 |
| Model 4 | |||
| Skin tone (Light brown skin vs. pale skin) | 5.90 | 2.39–15.45 | 1.72 × 10−4 |
| Smoking habits (Smoker vs. non−smoker) | 4.52 | 2.69–7.72 | 1.89 × 10−8 |
| HLA−DRB1*15:01 (Presence vs. absence) | 2.39 | 1.30–4.50 | 0.006 |
| Sex (female vs. male) | 1.88 | 1.08–3.30 | 0.025 |
| OR | IC 95% | p Value | |
|---|---|---|---|
| Number of factors | |||
| Light brown skin vs. 0 factor | 10.51 | 1.34–82.65 | 0.25 |
| Light brown skin + Presence HLA−DRB1*15:01 vs. 0 factor | 26.33 | 3.02–229.35 | 0.003 |
| Light brown skin + Smoker vs. 0 factor | 42.68 | 5.45–334.43 | 3.52 × 10−4 |
| Light brown skin + Smoker + Presence HLA−DRB1*15:01 vs. 0 factor | 114.16 | 12.60–1034.12 | 2.51 × 10−5 |
| Sex (female vs. male) | 1.89 | 1.06–3.37 | 0.031 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Urbaneja, P.; Hurtado-Guerrero, I.; Hernández, M.Á.; Oliver-Martos, B.; Oreja-Guevara, C.; Ortega-Pinazo, J.; Alonso, A.; Barón-López, F.J.; Leyva, L.; Fernández, Ó.; et al. Skin Phototype Could Be a Risk Factor for Multiple Sclerosis. J. Clin. Med. 2020, 9, 2384. https://doi.org/10.3390/jcm9082384
Urbaneja P, Hurtado-Guerrero I, Hernández MÁ, Oliver-Martos B, Oreja-Guevara C, Ortega-Pinazo J, Alonso A, Barón-López FJ, Leyva L, Fernández Ó, et al. Skin Phototype Could Be a Risk Factor for Multiple Sclerosis. Journal of Clinical Medicine. 2020; 9(8):2384. https://doi.org/10.3390/jcm9082384
Chicago/Turabian StyleUrbaneja, Patricia, Isaac Hurtado-Guerrero, Miguel Ángel Hernández, Begoña Oliver-Martos, Celia Oreja-Guevara, Jesús Ortega-Pinazo, Ana Alonso, Francisco J Barón-López, Laura Leyva, Óscar Fernández, and et al. 2020. "Skin Phototype Could Be a Risk Factor for Multiple Sclerosis" Journal of Clinical Medicine 9, no. 8: 2384. https://doi.org/10.3390/jcm9082384
APA StyleUrbaneja, P., Hurtado-Guerrero, I., Hernández, M. Á., Oliver-Martos, B., Oreja-Guevara, C., Ortega-Pinazo, J., Alonso, A., Barón-López, F. J., Leyva, L., Fernández, Ó., & Pinto-Medel, M. J. (2020). Skin Phototype Could Be a Risk Factor for Multiple Sclerosis. Journal of Clinical Medicine, 9(8), 2384. https://doi.org/10.3390/jcm9082384