Relationship between Osteosarcopenia and Frailty in Patients with Chronic Liver Disease

 , ,
, , 
Abstract
1. Introduction
2. Materials and Methods
2.1. Statement of Ethics
2.2. Study Design and Patients
2.3. Diagnosis of Osteoporosis, Sarcopenia, and Frailty
2.4. Clinical and Laboratory Assessments
2.5. Statistical Analysis
3. Results
3.1. Patient Characteristics
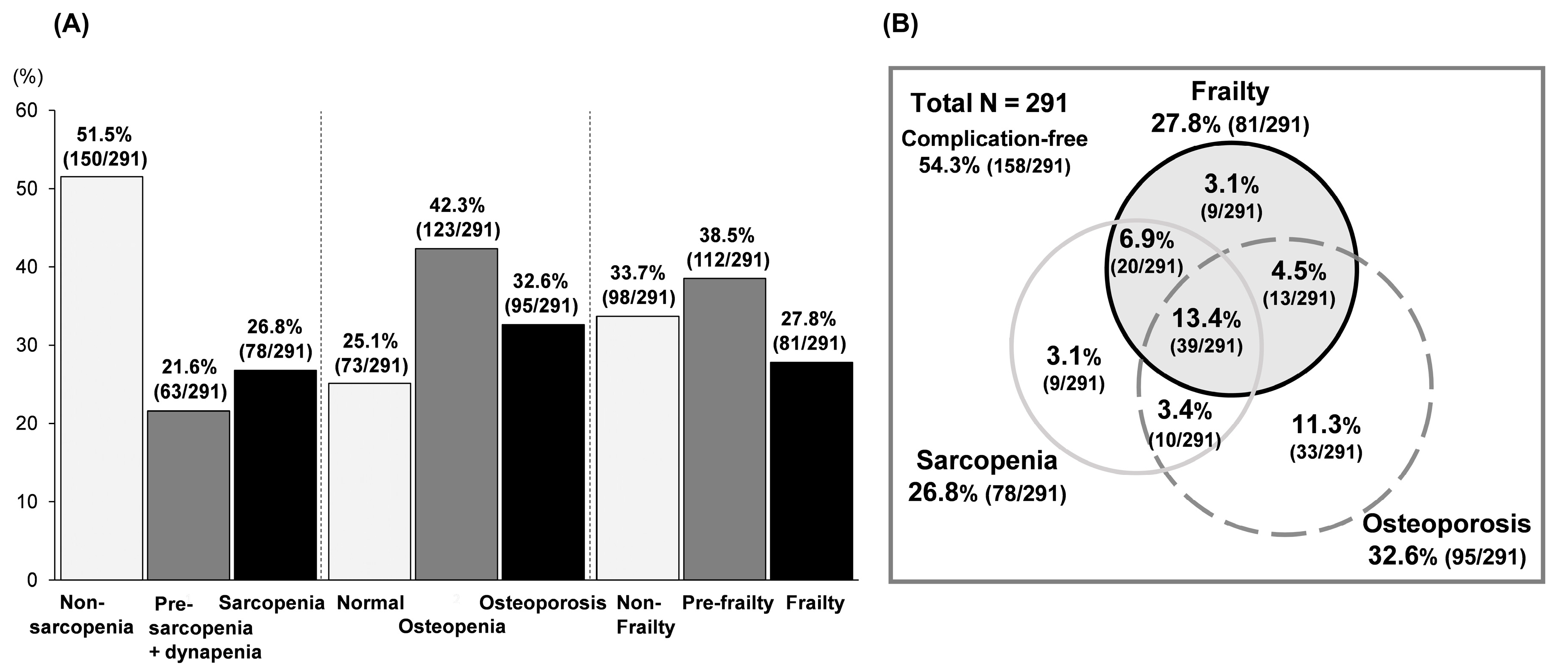
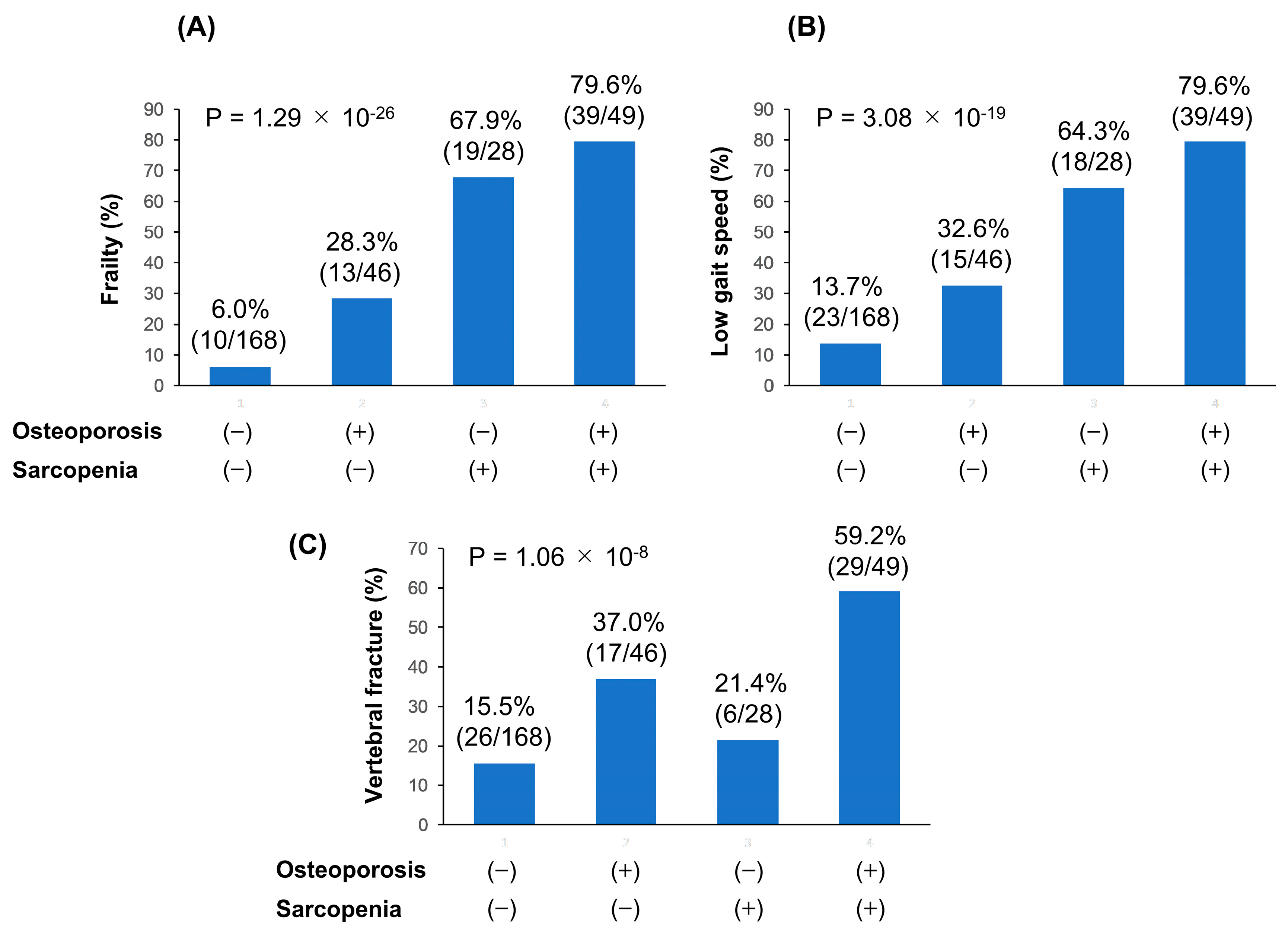
3.2. Prevalence of Osteoporosis, Sarcopenia, and Frailty
3.3. Comparison of Clinical Characteristics between Patients with and without Osteosarcopenia
3.4. Factors Associated with Osteosarcopenia in Patients with Chronic Liver Disease
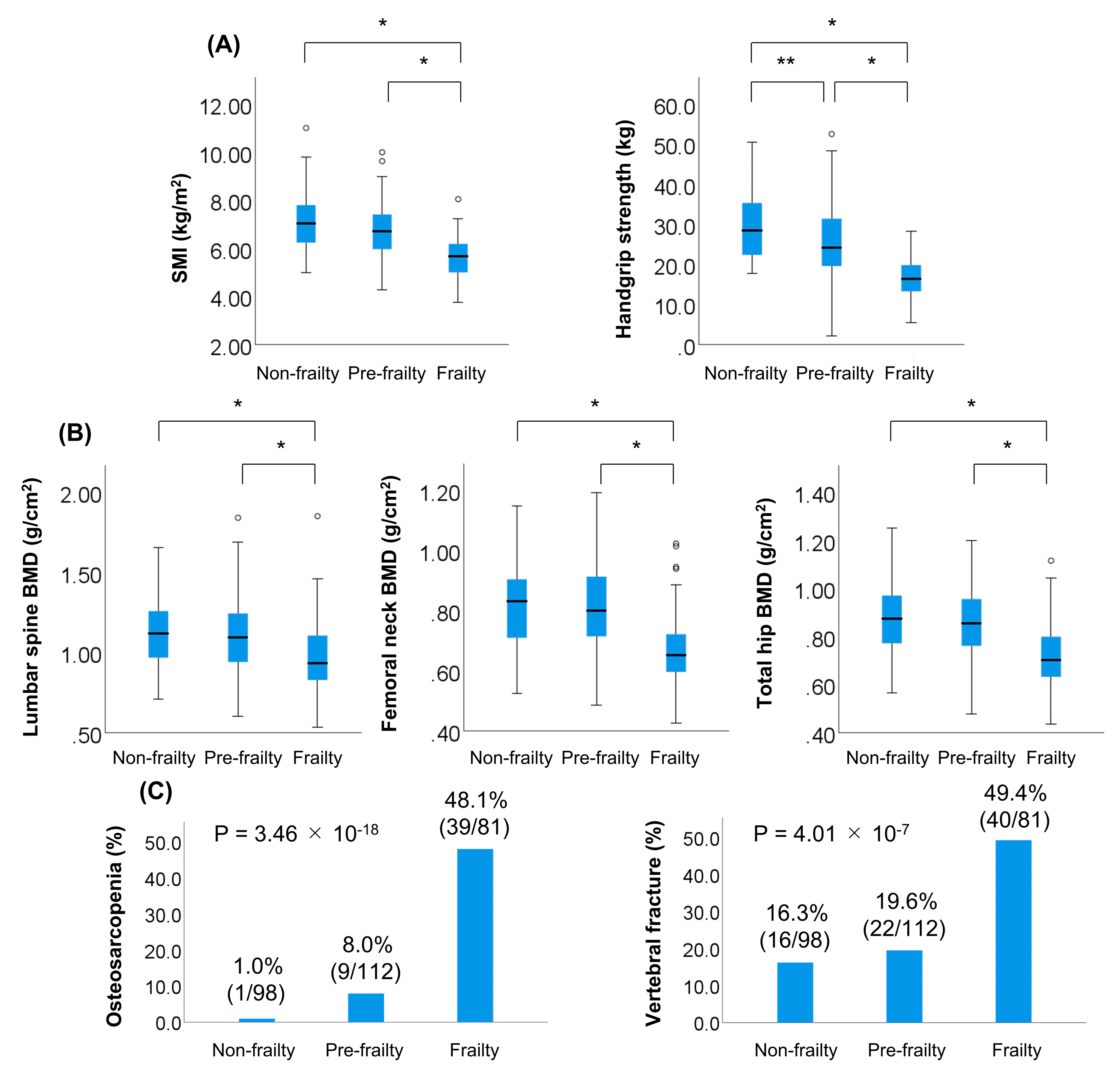
3.5. Comparison of Clinical Characteristics between Patients with and without Frailty
3.6. Factors Associated with Frailty in Patients with Chronic Liver Disease
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Binkley, N.; Buehring, B. Beyond FRAX: It’s time to consider “sarco-osteopenia”. J. Clin. Densitom. 2009, 12, 413–416. [Google Scholar] [CrossRef]
- Hassan, E.B.; Duque, G. Osteosarcopenia: A new geriatric syndrome. Aust. Fam. Phys. 2017, 46, 849–853. [Google Scholar] [PubMed]
- Hirschfeld, H.P.; Kinsella, R.; Duque, G. Osteosarcopenia: Where bone, muscle, and fat collide. Osteoporos Int. 2017, 28, 2781–2790. [Google Scholar] [CrossRef] [PubMed]
- Bani Hassan, E.; Phu, S.; Vogrin, S.; Escobedo Terrones, G.; Pérez, X.; Rodriguez-Sanchez, I.; Duque, G. Diagnostic Value of Mid-Thigh and Mid-Calf Bone, Muscle, and Fat Mass in Osteosarcopenia: A Pilot Study. Calcif. Tissue Int. 2019, 105, 392–402. [Google Scholar] [CrossRef] [PubMed]
- Cruz-Jentoft, A.J.; Bahat, G.; Bauer, J.; Boirie, Y.; Bruyère, O.; Cederholm, T.; Cooper, C.; Landi, F.; Rolland, Y.; Sayer, A.A.; et al. Writing Group for the European Working Group on Sarcopenia in Older People 2 (EWGSOP2), and the Extended Group for EWGSOP2; Sarcopenia: Revised European consensus on definition and diagnosis. Age Ageing 2019, 48, 16–31. [Google Scholar] [CrossRef] [PubMed]
- Paintin, J.; Cooper, C.; Dennison, E. Osteosarcopenia. Br. J. Hosp. Med. (Lond.) 2018, 79, 253–258. [Google Scholar] [CrossRef]
- Saeki, C.; Takano, K.; Oikawa, T.; Aoki, Y.; Kanai, T.; Takakura, K.; Nakano, M.; Torisu, Y.; Sasaki, N.; Abo, M.; et al. Comparative assessment of sarcopenia using the JSH, AWGS, and EWGSOP2 criteria and the relationship between sarcopenia, osteoporosis, and osteosarcopenia in patients with liver cirrhosis. BMC Musculoskelet. Disord. 2019, 20, 615. [Google Scholar] [CrossRef]
- Clegg, A.; Young, J.; Iliffe, S.; Rikkert, M.O.; Rockwood, K. Frailty in elderly people. Lancet 2013, 38, 752–762. [Google Scholar] [CrossRef]
- Morley, J.E. Frailty and sarcopenia in elderly. Wien Klin Wochenschr. 2016, 128, 439–445. [Google Scholar] [CrossRef]
- Tandon, P.; Tangri, N.; Thomas, L.; Zenith, L.; Shaikh, T.; Carbonneau, M.; Ma, M.; Bailey, R.J.; Jayakumar, S.; Burak, K.W.; et al. A Rapid Bedside Screen to Predict Unplanned Hospitalization and Death in Outpatients with Cirrhosis: A Prospective Evaluation of the Clinical Frailty Scale. Am. J. Gastroenterol. 2016, 111, 1759–1767. [Google Scholar] [CrossRef]
- Lai, J.C.; Feng, S.; Terrault, N.A.; Lizaola, B.; Hayssen, H.; Covinsky, K. Frailty predicts waitlist mortality in liver transplant candidates. Am. J. Transplant. 2014, 14, 1870–1879. [Google Scholar] [CrossRef] [PubMed]
- Lai, J.C.; Rahimi, R.S.; Verna, E.C.; Kappus, M.R.; Dunn, M.A.; McAdams-DeMarco, M.; Haugen, C.E.; Volk, M.L.; Duarte-Rojo, A.; Ganger, D.R.; et al. Frailty Associated With Waitlist Mortality Independent of Ascites and Hepatic Encephalopathy in a Multicenter Study. Gastroenterology 2019, 156, 1675–1682. [Google Scholar] [CrossRef] [PubMed]
- Lai, J.C.; Covinsky, K.E.; Dodge, J.L.; Boscardin, W.J.; Segev, D.L.; Roberts, J.P.; Feng, S. Development of a novel frailty index to predict mortality in patients with end-stage liver disease. Hepatology 2017, 66, 564–574. [Google Scholar] [CrossRef] [PubMed]
- Bhanji, R.A.; Narayanan, P.; Moynagh, M.R.; Takahashi, N.; Angirekula, M.; Kennedy, C.C. Differing Impact of Sarcopenia and Frailty in Nonalcoholic Steatohepatitis and Alcoholic Liver Disease. Liver Transpl. 2019, 25, 14–24. [Google Scholar] [CrossRef]
- Laube, R.; Wang, H.; Park, L.; Heyman, J.K.; Vidot, H.; Majumdar, A.; Strasser, S.I.; McCaughan, G.W.; Liu, K. Frailty in advanced liver disease. Liver Int. 2018, 38, 2117–2128. [Google Scholar] [CrossRef]
- Lai, J.C.; Covinsky, K.E.; McCulloch, C.E.; Feng, S. The Liver Frailty Index Improves Mortality Prediction of the Subjective Clinician Assessment in Patients With Cirrhosis. Am. J. Gastroenterol. 2018, 113, 235–242. [Google Scholar] [CrossRef]
- Yoshimura, N.; Muraki, S.; Oka, H.; Iidaka, T.; Kodama, R.; Horii, C.; Kawaguchi, H.; Nakamura, K.; Akune, T.; Tanaka, S. Do sarcopenia and/or osteoporosis increase the risk of frailty? A 4-year observation of the second and third ROAD study surveys. Osteoporos Int. 2018, 29, 2181–2190. [Google Scholar]
- Wang, Y.J.; Wang, Y.; Zhan, J.K.; Tang, Z.Y.; He, J.Y.; Tan, P.; Deng, H.-Q.; Huang, W.; Liu, Y.-S. Sarco-Osteoporosis: Prevalence and Association with Frailty in Chinese Community-Dwelling Older Adults. Int. J. Endocrinol. 2015, 2015, 482940. [Google Scholar] [CrossRef]
- Fried, L.P.; Tangen, C.M.; Walston, J.; Newman, A.B.; Hirsch, C.; Gottdiener, J.; Seeman, T.; Tracy, R.; Kop, W.J.; Burke, G.; et al. Frailty in older adults: Evidence for a phenotype. J. Gerontol. A Biol. Sci. Med. Sci. 2001, 5, M146–M156. [Google Scholar]
- WHO. Assessment of Fracture Risk and Its Application to Screening for Postmenopausal Osteoporosis; Technical Report Series; WHO Study Group: Geneva, Switzerland, 1994; pp. 1–129. [Google Scholar]
- Nishikawa, H.; Shiraki, M.; Hiramatsu, A.; Moriya, K.; Hino, K.; Nishiguchi, S. Japan Society of Hepatology guidelines for sarcopenia in liver disease (1 st edition): Recommendation from the working group for creation of sarcopenia assessment criteria. Hepatol. Res. 2016, 46, 951–963. [Google Scholar] [CrossRef] [PubMed]
- Tsutsumimoto, K.; Doi, T.; Makizako, H.; Hotta, R.; Nakakubo, S.; Makino, K.; Suzuki, T.; Shimada, H. Aging-related anorexia and its association with disability and frailty. J. Cachexia Sarcopenia Muscle 2018, 9, 834–843. [Google Scholar] [CrossRef] [PubMed]
- Kawao, N.; Kaji, H. Interactions between muscle tissues and bone metabolism. J. Cell Biochem. 2015, 116, 687–695. [Google Scholar] [CrossRef] [PubMed]
- George, J.; Ganesh, H.K.; Acharya, S.; Bandgar, T.R.; Shivane, V.; Karvat, A.; Bhatia, S.J.; Shah, S.; Menon, P.S.; Shah, N. Bone mineral density and disorders of mineral metabolism in chronic liver disease. World J. Gastroenterol. 2009, 15, 3516–3522. [Google Scholar] [CrossRef]
- Tajiri, K.; Shimizu, Y. Branched-chain amino acids in liver diseases. Transl. Gastroenterol. Hepatol. 2018, 3, 47. [Google Scholar] [CrossRef] [PubMed]
- Moriwaki, H. Branched-chain amino acids as a protein- and energy-source in liver cirrhosis. Biochem. Biophys. Res. Commun. 2004, 313, 405–409. [Google Scholar] [CrossRef]
- Ottestad, I.; Ulven, S.M.; Øyri, L.K.L.; Sandvei, K.S.; Gjevestad, G.O.; Bye, A.; Sheikh, N.A.; Biong, A.S.; Andersen, L.F.; Holven, K.B. Reduced plasma concentration of branched-chain amino acids in sarcopenic older subjects: A cross-sectional study. Br. J. Nutr. 2018, 120, 445–453. [Google Scholar] [CrossRef]
- Coelho-Júnior, H.J.; Calvani, R.; Picca, A.; Gonçalves, I.O.; Landi, F.; Bernabei, R.; Cesari, M.; Uchida, M.C.; Marzetti, E. Protein-Related Dietary Parameters and Frailty Status in Older Community-Dwellers across Different Frailty Instruments. Nutrients 2020, 12, 508. [Google Scholar] [CrossRef]
- Sepúlveda-Loyola, W.; Phu, S.; Bani Hassan, E.; Brennan-Olsen, S.L.; Zanker, J.; Vogrin, S.; Conzade, R.; Kirk, B.; Saedi, A.A.; Probst, V. The Joint Occurrence of Osteoporosis and Sarcopenia (Osteosarcopenia): Definitions and Characteristics. J. Am. Med. Dir. Assoc. 2020, 21, 220–225. [Google Scholar] [CrossRef]
- Drey, M.; Sieber, C.C.; Bertsch, T.; Bauer, J.M.; Schmidmaier, R.; FiAT Intervention Group. Osteosarcopenia is more than sarcopenia and osteopenia alone. Aging Clin. Exp. Res. 2016, 28, 895–899. [Google Scholar]
- Oleksik, A.M.; Ewing, S.; Shen, W.; van Schoor, N.M.; Lips, P. Impact of incident vertebral fractures on health related quality of life (HRQOL) in postmenopausal women with prevalent vertebral fractures. Osteoporos Int. 2005, 16, 861–870. [Google Scholar] [CrossRef] [PubMed]
- JafariNasabian, P.; Inglis, J.E.; Kelly, O.J.; Ilich, J.Z. Osteosarcopenic obesity in women: Impact, prevalence, and management challenges. Int. J. Womens Health 2017, 9, 33–42. [Google Scholar] [CrossRef] [PubMed]
- Jadczak, A.D.; Makwana, N.; Luscombe-Marsh, N.; Visvanathan, R.; Schultz, T.J. Effectiveness of exercise interventions on physical function in community-dwelling frail older people: An umbrella review of systematic reviews. JBI Database Syst. Rev. Implement Rep. 2018, 16, 752–775. [Google Scholar] [CrossRef] [PubMed]
- Stanghelle, B.; Bentzen, H.; Giangregorio, L.; Pripp, A.H.; Skelton, D.A.; Bergland, A. Effects of a resistance and balance exercise programme on physical fitness, health-related quality of life and fear of falling in older women with osteoporosis and vertebral fracture: A randomized controlled trial. Osteoporos Int. 2020. Epub ahead of print. [Google Scholar] [CrossRef]
- Bonnet, N.; Bourgoin, L.; Biver, E.; Douni, E.; Ferrari, S. RANKL inhibition improves muscle strength and insulin sensitivity and restores bone mass. J. Clin. Investig. 2019, 129, 3214–3223. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Variable | All patients | Osteosarcopenia | Non-Osteosarcopenia | p-Value |
|---|---|---|---|---|
| Patients, n (%) | 291 | 49 (16.8) | 242 (83.2) | |
| Male, n (%) | 137 (47.1) | 16 (32.7) | 121 (50.0) | 0.027 |
| Age (years) | 70.0 (59.0–76.0) | 76.0 (72.5–81.0) | 68.0 (57.8–74.0) | <0.001 |
| BMI (kg/m2) | 23.1 (20.8–26.0) | 20.4 (19.0–22.2) | 23.7 (21.4–26.1) | <0.001 |
| Liver cirrhosis, n (%) | 151 (51.9) | 31 (63.3) | 120 (49.6) | 0.081 |
| Etiology | ||||
| HBV/HCV/alcohol/PBC/other, n | 41/92/52/59/47 | 5/21/5/14/4 | 36/71/47/45/43 | 0.061 |
| Total bilirubin (mg/dL) | 0.7 (0.5–1.0) | 0.6 (0.4–0.8) | 0.8 (0.5–1.0) | 0.006 |
| Albumin (g/dL) | 4.0 (3.7–4.3) | 4.0 (3.6–4.3) | 4.1 (3.7–4.3) | 0.332 |
| Prothrombin time INR | 1.05 (0.97–1.15) | 1.06 (0.97–1.11) | 1.05 (0.97–1.15) | 0.466 |
| M2BPGi (C.O.I) | 1.56 (0.86–3.58) | 1.99 (1.37–2.96) | 1.44 (0.78–3.75) | 0.030 |
| IGF-1 (ng/mL) | 65 (47–90) | 49 (41–64) | 68 (50–95) | <0.001 |
| Zinc (μg/dL) | 68 (59–78) | 66 (56–76) | 68 (59–78) | 0.378 |
| BCAA (μmol/L) | 405 (344–465) | 333 (293–401) | 417 (367–476) | <0.001 |
| TRACP-5b (mU/dL) | 415 (312–563) | 463 (311–596) | 410 (312–528) | 0.273 |
| P1NP (ng/mL) | 49 (34–72) | 46 (34–76) | 49 (34–70) | 0.714 |
| PTH-intact (pg/mL) | 47 (35–59) | 51 (38–85) | 44 (34–57) | 0.010 |
| SMI (kg/m2) | ||||
| All patients | 6.48 (5.74–7.26) | 5.12 (4.74–5.52) | 6.75 (5.99–7.44) | <0.001 |
| Male | 7.19 (6.65–7.99) | 5.93 (5.15–6.43) | 7.34 (6.94–8.09) | <0.001 |
| Female | 5.88 (5.27–6.48) | 4.94 (4.61–5.25) | 6.04 (5.75–6.57) | <0.001 |
| Handgrip strength (kg) | ||||
| All patients | 23.4 (17.9–31.4) | 15.1 (13.1–17.8) | 24.8 (19.7–32.6) | <0.001 |
| Male | 31.0 (24.9–37.4) | 21.8 (13.3–23.9) | 32.4 (27.4–38.2) | <0.001 |
| Female | 18.9 (15.3–22.4) | 14.9 (12.6–17.0) | 21.0 (17.5–23.5) | <0.001 |
| Lumbar spine BMD (g/cm2) | 1.07 (0.90–1.22) | 0.85 (0.75–0.95) | 1.10 (0.95–1.24) | <0.001 |
| Femoral neck BMD (g/cm2) | 0.76 (0.67–0.89) | 0.62 (0.56–0.65) | 0.81 (0.71–0.90) | <0.001 |
| Total hip BMD (g/cm2) | 0.83 (0.71–0.94) | 0.66 (0.58–0.71) | 0.86 (0.76–0.96) | <0.001 |
| Frailty, n (%) | 81 (27.8) | 39 (79.6) | 42 (17.4) | <0.001 |
| Low gait speed (m/s), n (%) | 95 (32.6) | 39 (79.6) | 56 (23.1) | <0.001 |
| Vertebral fracture, n (%) | 78 (26.8) | 29 (59.2) | 49 (20.2) | <0.001 |
| Variable | Univariate | Multivariate | ||
|---|---|---|---|---|
| OR (95%CI) | p-Value | OR (95% CI) | p-Value | |
| Male | 0.485 (0.254–0.927) | 0.029 | ||
| Age (years) | 1.094 (1.053–1.136) | <0.001 | ||
| BMI (kg/m2) | 0.767 (0.687–0.857) | <0.001 | 0.821 (0.726–0.929) | 0.002 |
| IGF-1 (ng/mL) | 0.974 (0.961–0.987) | <0.001 | 0.980 (0.964–0.996) | 0.014 |
| BCAA (μmol/L) | 0.993 (0.989–0.996) | <0.001 | ||
| PTH-intact (pg/mL) | 1.019 (1.009–1.029) | <0.001 | 1.017 (1.005–1.030) | 0.006 |
| Frailty | 15.545 (7.370–32.789) | <0.001 | 9.837 (4.199–23.043) | <0.001 |
| Vertebral fracture | 5.711 (2.981–10.943) | <0.001 | 3.306 (1.439–7.596) | 0.005 |
| Variable | Frailty | Non-Frailty and Pre-Frailty | p-Value |
|---|---|---|---|
| Patients, n (%) | 81 (27.8) | 210 (72.2) | |
| Male, n (%) | 31 (38.3) | 106 (50.5) | 0.062 |
| Age (years) | 76.0 (69.5–80.0) | 67.0 (56.0–73.0) | <0.001 |
| BMI (kg/m2) | 21.5 (19.8–24.5) | 23.8 (21.3–26.2) | <0.001 |
| Liver cirrhosis, n (%) | 56 (69.1) | 95 (45.2) | <0.001 |
| Etiology | |||
| HBV/HCV/alcohol/PBC/other, n | 7/36/9/16/13 | 34/56/43/43/34 | 0.015 |
| Total bilirubin (mg/dL) | 0.7 (0.5–1.0) | 0.7 (0.5–1.0) | 0.140 |
| Albumin (g/dL) | 3.9 (3.4–4.3) | 4.1 (3.8–4.4) | 0.001 |
| Prothrombin time INR | 1.07 (0.99–1.17) | 1.04 (0.97–1.14) | 0.356 |
| M2BPGi (C.O.I) | 2.33 (1.29–4.70) | 1.37 (0.72–2.71) | <0.001 |
| IGF-1 (ng/mL) | 54 (41–69) | 72 (51–97) | <0.001 |
| Zinc (μg/dL) | 63 (51–75) | 70 (60–78) | 0.001 |
| BCAA (μmol/L) | 370 (308–412) | 427 (370–485) | <0.001 |
| TRACP-5b (mU/dL) | 458 (323–592) | 394 (311–528) | 0.084 |
| P1NP (ng/mL) | 49 (33–79) | 49 (36–67) | 0.801 |
| PTH-intact (pg/mL) | 48 (33–68) | 46 (35–57) | 0.411 |
| SMI (kg/m2) | |||
| All patients | 5.65 (4.97–6.24) | 6.87 (6.05–7.59) | <0.001 |
| Male | 6.18 (5.65–6.94) | 7.45 (7.03–8.16) | <0.001 |
| Female | 5.24 (4.81–5.75) | 6.08 (5.71–6.57) | <0.001 |
| Handgrip strength (kg) | |||
| All patients | 16.4 (13.2–20.2) | 27.0 (21.2–34.3) | <0.001 |
| Male | 22.8 (18.3–24.7) | 33.9 (29.4–38.8) | <0.001 |
| Female | 14.5 (12.3–17.0) | 21.5 (18.5–23.9) | <0.001 |
| Lumbar spine BMD (g/cm2) | 0.93 (0.82–1.11) | 1.11 (0.94–1.25) | <0.001 |
| Femoral neck BMD (g/cm2) | 0.65 (0.60–0.72) | 0.82 (0.71–0.91) | <0.001 |
| Total hip BMD (g/cm2) | 0.70 (0.63–0.80) | 0.86 (0.76–0.97) | <0.001 |
| Low gait speed (m/s), n (%) | 75 (92.6) | 20 (9.5) | <0.001 |
| Osteosarcopenia, n (%) | 39 (48.1) | 10 (4.8) | <0.001 |
| Vertebral fracture, n (%) | 40 (49.4) | 38 (18.1) | <0.001 |
| Variable | Univariate | Multivariate | ||
|---|---|---|---|---|
| OR (95%CI) | p-Value | OR (95%CI) | p-Value | |
| Age (years) | 1.089 (1.056–1.123) | <0.001 | 1.090 (1.050–1.130) | <0.001 |
| BMI (kg/m2) | 0.875 (0.811–0.943) | <0.001 | ||
| Liver cirrhosis | 2.712 (1.574–4.672) | <0.001 | ||
| Albumin (g/dL) | 0.375 (0.227–0.621) | <0.001 | ||
| M2BPGi (C.O.I) | 1.124 (1.041–1.214) | 0.003 | 1.149 (1.039–1.271) | 0.007 |
| IGF-1 (ng/mL) | 0.980 (0.970–0.989) | <0.001 | ||
| Zinc (μg/dL) | 0.974 (0.956–0.992) | 0.006 | ||
| BCAA (μmol/L) | 0.993 (0.989–0.996) | <0.001 | 0.994 (0.990–0.997) | 0.001 |
| PTH-intact (pg/mL) | 1.009 (1.001–1.018) | 0.006 | ||
| Osteosarcopenia | 18.571 (8.596–40.121) | <0.001 | 10.069 (4.282–23.680) | <0.001 |
| Vertebral fracture | 4.416 (2.523–7.728) | <0.001 | ||
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Saeki, C.; Kanai, T.; Nakano, M.; Oikawa, T.; Torisu, Y.; Abo, M.; Saruta, M.; Tsubota, A. Relationship between Osteosarcopenia and Frailty in Patients with Chronic Liver Disease. J. Clin. Med. 2020, 9, 2381. https://doi.org/10.3390/jcm9082381
Saeki C, Kanai T, Nakano M, Oikawa T, Torisu Y, Abo M, Saruta M, Tsubota A. Relationship between Osteosarcopenia and Frailty in Patients with Chronic Liver Disease. Journal of Clinical Medicine. 2020; 9(8):2381. https://doi.org/10.3390/jcm9082381
Chicago/Turabian StyleSaeki, Chisato, Tomoya Kanai, Masanori Nakano, Tsunekazu Oikawa, Yuichi Torisu, Masahiro Abo, Masayuki Saruta, and Akihito Tsubota. 2020. "Relationship between Osteosarcopenia and Frailty in Patients with Chronic Liver Disease" Journal of Clinical Medicine 9, no. 8: 2381. https://doi.org/10.3390/jcm9082381
APA StyleSaeki, C., Kanai, T., Nakano, M., Oikawa, T., Torisu, Y., Abo, M., Saruta, M., & Tsubota, A. (2020). Relationship between Osteosarcopenia and Frailty in Patients with Chronic Liver Disease. Journal of Clinical Medicine, 9(8), 2381. https://doi.org/10.3390/jcm9082381