Potential Risk of Other-Cause Mortality Due to Long-Term Androgen Deprivation Therapy in Elderly Patients with Clinically Localized Prostate Cancer Treated with Radiotherapy—A Confirmation Study

 ,
,  , ,
, , 
Abstract
1. Introduction
2. Methods
2.1. Patients
2.2. Treatment
2.3. Statistical Analysis
3. Results
3.1. Patients and Treatment Characteristics
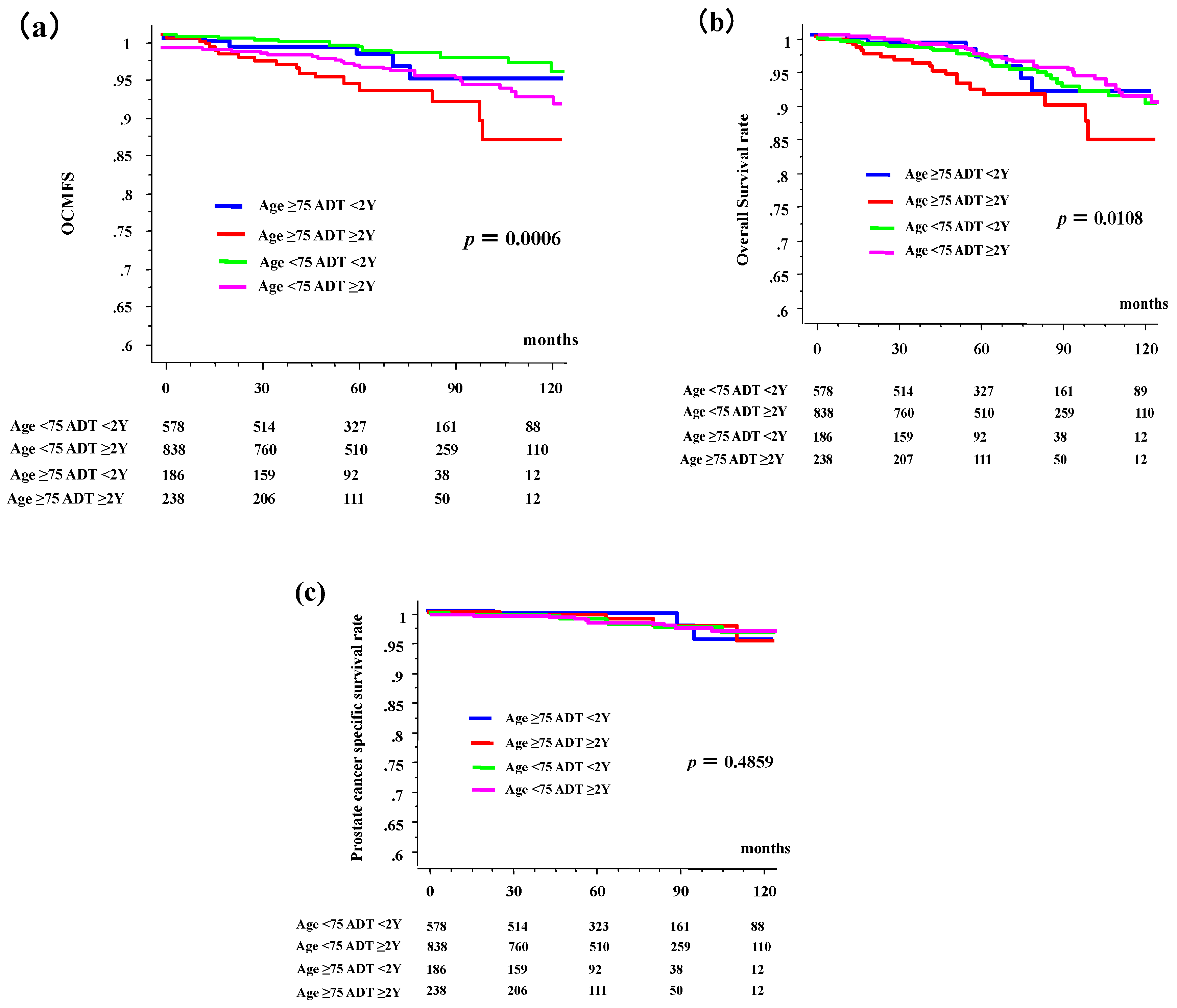
3.2. Other-Cause Mortality (OCM), Prostate Cancer-Related Death, and OS
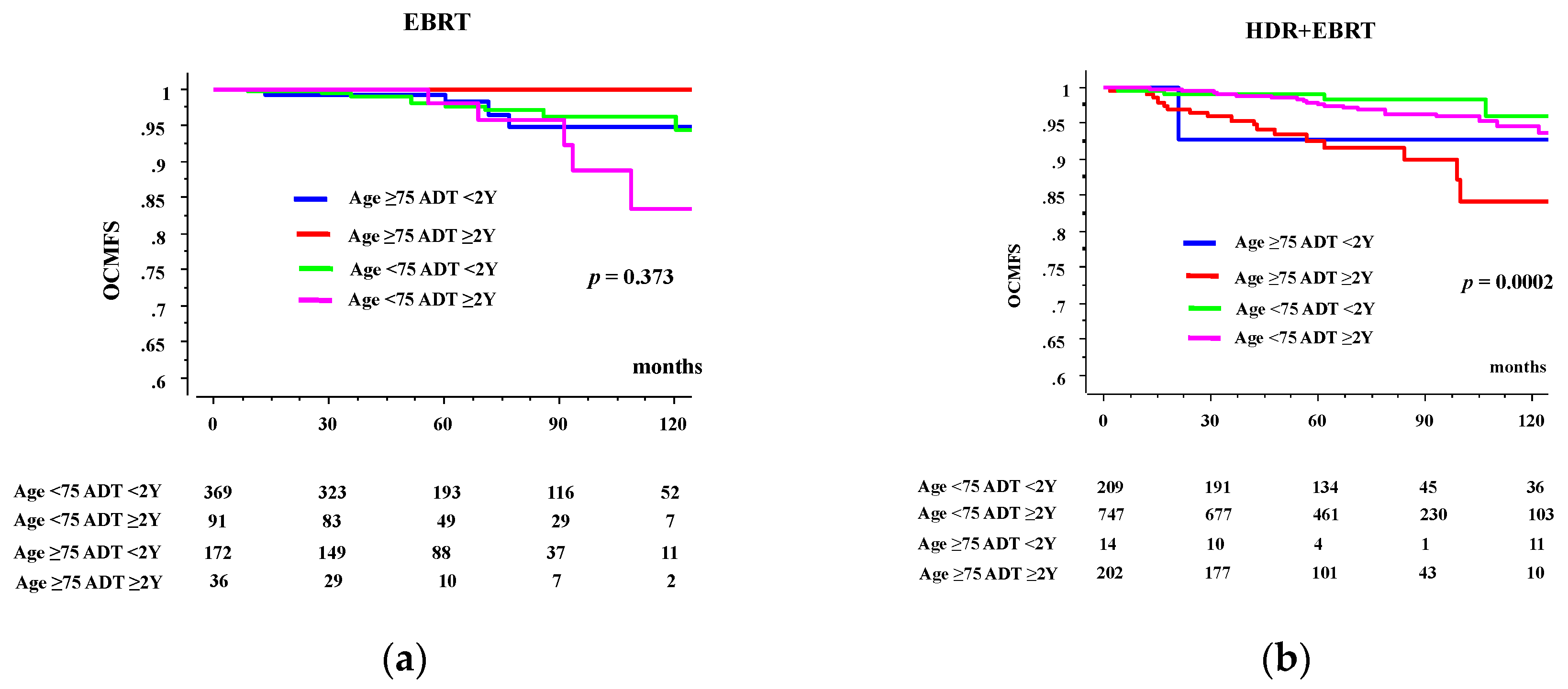
3.3. Comparison between EBRT and HDR + EBRT Group
3.4. Causes of OCM
4. Discussion
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Bray, F.; Ferlay, J.; Soerjomataram, I.; Siegel, R.L.; Torre, L.A.; Jemal, A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. Cancer J. Clin. 2018, 68, 394–424. [Google Scholar] [CrossRef]
- Bolla, M.; Gonzalez, D.; Warde, P.; Dubois, J.B.; Mirimanoff, R.-O.; Storme, G.; Bernier, J.; Kuten, A.; Sternberg, C.; Gil, T.; et al. Improved survival in patients with locally advanced prostate cancer treated with radiotherapy and goserelin. N. Engl. J. Med. 1997, 337, 295–300. [Google Scholar] [CrossRef]
- McGivney, W.T. The national comprehensive cancer network. Cancer 1998, 82, 2057–2060. [Google Scholar] [CrossRef]
- Sasse, A.D.; Sasse, E.; Carvalho, A.M.; Macedo, L.T. Androgenic suppression combined with radiotherapy for the treatment of prostate adenocarcinoma: A systematic review. BMC Cancer 2012, 12, 54. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, P.L.; Alibhai, S.M.; Basaria, S.; D’Amico, A.V.; Kantoff, P.W.; Keating, N.L.; Penson, D.; Rosario, D.J.; Tombal, B.; Smith, M.R. Adverse effects of androgen deprivation therapy and strategies to mitigate them. Eur. Urol. 2015, 67, 825–836. [Google Scholar] [CrossRef] [PubMed]
- Abdollah, F.; Sammon, J.; Reznor, G.; Sood, A.; Schmid, M.; Klett, D.; Sun, M.; Aizer, A.; Choueiri, T.; Hu, J.; et al. Medical androgen deprivation therapy and increased non-cancer mortality in non-metastatic prostate cancer patients aged ≥66 years. Eur. J. Surg. Oncol. 2015, 41, 1529–1539. [Google Scholar] [CrossRef]
- Survival Statistics of Japanese Association of Clinical Cancer Centers Cancer Survival Rates at Japanese Association of Clinical Cancer Centers. Available online: http://www.zengankyo.ncc.go.jp/etc/seizonritsu/seizonritsu2007.html#10 (accessed on 10 April 2020).
- Yamazaki, H.; Masui, K.; Suzuki, G.; Nakamura, S.; Aibe, N.; Shimizu, D.; Yamada, K.; Okihara, K.; Shiraishi, T.; Kotsuma, T.; et al. Effect of androgen deprivation therapy on other-cause of mortality in elderly patients with clinically localized prostate cancer treated with modern radiotherapy: Is there a negative impact? J. Clin. Med. 2019, 8, 338. [Google Scholar] [CrossRef] [PubMed]
- Database: Retrospective Multi-Institutional Data Collection to Explore the Prognostic Prediction System with Machine Learning for Radiation Therapy after Prostate Cancer (B17-278). Available online: https://www.khp.kitasato-u.ac.jp/ska/radiotherapy/arcivements/#open-date (accessed on 19 January 2020).
- Ishiyama, H.; Kamitani, N.; Kawamura, H.; Kato, S.; Aoki, M.; Kariya, S.; Matsumura, T.; Kaidu, M.; Yoshida, K.; Hashimoto, Y.; et al. Nationwide multi-institutional retrospective analysis of high-dose-rate brachytherapy combined with external beam radiotherapy for localized prostate cancer: An asian prostate hdr-bt consortium. Brachytherapy 2017, 16, 503–510. [Google Scholar] [CrossRef] [PubMed]
- Huggins, C.; Hodges, C.V. Studies on prostatic cancer. I. The effect of castration, of estrogen and of androgen injection on serum phosphatases in metastatic carcinoma of the prostate. Cancer J. Clin. 1972, 22, 232–240. [Google Scholar] [CrossRef] [PubMed]
- Huggins, C.; Stevens, R.E.; Hodges, C.V. Studies on prostatic cancer. II. The effects of castration on advanced carcinoma of the prostate gland. Arch. Surg. 1941, 3, 209–223. [Google Scholar] [CrossRef]
- Zapatero, A.; Guerrero, A.; Maldonado, X.; Álvarez, A.; Segundo, C.G.S.; Rodríguez, M.A.C.; Macias, V.A.; Olive, A.P.; Casas, F.; Boladeras, A.; et al. High-dose radiotherapy with short-term or long-term androgen deprivation in localised prostate cancer (DART01/05 GICOR): A randomised, controlled, phase 3 trial. Lancet Oncol. 2015, 16, 320–327. [Google Scholar] [CrossRef]
- Keating, N.L.; O’Malley, A.J.; Freedland, S.J.; Smith, M.R. Diabetes and cardiovascular disease during androgen deprivation therapy: Observational study of veterans with prostate cancer. J. Natl. Cancer Inst. 2009, 102, 39–46. [Google Scholar] [CrossRef]
- Jespersen, C.G.; Nørgaard, M.; Borre, M. Androgen-deprivation therapy in treatment of prostate cancer and risk of myocardial infarction and stroke: A nationwide danish population-based cohort study. Eur. Urol. 2014, 65, 704–709. [Google Scholar] [CrossRef] [PubMed]
- Lapi, F.; Azoulay, L.; Niazi, M.T.; Yin, H.; Benayoun, S.; Suissa, S. Androgen deprivation therapy and risk of acute kidney injury in patients with prostate cancer. JAMA 2013, 310, 289–296. [Google Scholar] [CrossRef] [PubMed]
- Nead, K.T.; Sinha, S.; Nguyen, P.L. Androgen deprivation therapy for prostate cancer and dementia risk: A systematic review and meta-analysis. Prostate Cancer Prostatic Dis. 2017, 20, 259–264. [Google Scholar] [CrossRef]
- Hu, J.C.; Williams, S.B.; O’Malley, A.J.; Smith, M.R.; Nguyen, P.L.; Keating, N.L. Androgen-deprivation therapy for nonmetastatic prostate cancer is associated with an increased risk of peripheral arterial disease and venous thromboembolism. Eur. Urol. 2012, 61, 1119–1128. [Google Scholar] [CrossRef]
- Guo, Z.; Huang, Y.; Gong, L.; Gan, S.; Chan, F.L.; Gu, C.; Xiang, S.; Wang, S. Association of androgen deprivation therapy with thromboembolic events in patients with prostate cancer: A systematic review and meta-analysis. Prostate Cancer Prostatic Dis. 2018, 21, 451–460. [Google Scholar] [CrossRef]
- Morgans, A.K.; Fan, K.-H.; Koyama, T.; Albertsen, P.C.; Goodman, M.; Hamilton, A.S.; Hoffman, R.M.; Stanford, J.L.; Stroup, A.M.; Resnick, M.J.; et al. Influence of age on incident diabetes and cardiovascular disease in prostate cancer survivors receiving androgen deprivation therapy. J. Urol. 2014, 193, 1226–1231. [Google Scholar] [CrossRef]
- Beyer, D.C.; McKeough, T.; Thomas, T. Impact of short course hormonal therapy on overall and cancer specific survival after permanent prostate brachytherapy. Int. J. Radiat. Oncol. 2005, 61, 1299–1305. [Google Scholar] [CrossRef]
- Nanda, A.; Chen, M.-H.; Braccioforte, M.H.; Moran, B.J.; D’Amico, A.V. Hormonal therapy use for prostate cancer and mortality in men with coronary artery disease–induced congestive heart failure or myocardial infarction. JAMA 2009, 302, 866. [Google Scholar] [CrossRef]
- Pickles, T.; Tyldesley, S.; Hamm, J.; Virani, S.A.; Morris, W.J.; Keyes, M. Brachytherapy for intermediate-risk prostate cancer, androgen deprivation, and the risk of death. Int. J. Radiat. Oncol. 2018, 100, 45–52. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Variables | Strata | ADT ≥ 2 Years | ADT < 2 Years | p-Value | ||
|---|---|---|---|---|---|---|
| n = 1076 | n = 764 | |||||
| No. or Median (range) | (%) | No. or Median (range) | (%) | |||
| Age | 50 | 59 | (5%) | 43 | (6%) | 0.4271 |
| 60 | 434 | (40%) | 280 | (37%) | ||
| 70 | 345 | (32%) | 255 | (33%) | ||
| 75- | 238 | (22%) | 186 | (24%) | ||
| T category | 1 | 188 | (17%) | 190 | (25%) | <0.0001 |
| 2 | 340 | (32%) | 286 | (37%) | exc NA | |
| 3 | 529 | (49%) | 267 | (35%) | ||
| 4 | 11 | (1%) | 18 | (2%) | ||
| NA | 8 | (1%) | 3 | (0%) | ||
| Pretreatment PSA | ng/mL | 16.68 (2.682–1454) | 12.4 (2.286–399) | <0.0001 | ||
| Gleason score | −6 | 100 | (9%) | 70 | (9%) | <0.0001 |
| 7 | 462 | (43%) | 451 | (59%) | exc NA | |
| 8- | 510 | (47%) | 243 | (32%) | ||
| NA | 4 | (0.4%) | 0 | (0%) | ||
| NCCN risk classification | Low | 7 | (1%) | 26 | (3%) | <0.0001 |
| Intermediate | 139 | (13%) | 271 | (35%) | exc NA | |
| High | 927 | (86%) | 467 | (61%) | ||
| NA | 3 | (0.3%) | 0 | (0%) | ||
| Modality | EBRT | 127 | (12%) | 541 | (71%) | <0.0001 |
| HDR + EBRT | 949 | (88%) | 223 | (29%) | ||
| Follow-up | Months | 68 (2–177) | 63 (4–165) | 0.1135 |
| Variables | Strata | OCM (+) | OCM (-) | p-Value | |
|---|---|---|---|---|---|
| n = 63 | n = 1777 | ||||
| No. or Median (range) | OCM (+) % | No. or Median (range) | |||
| Age | −59 | 2 | (2%) | 100 | 0.0043 |
| 60–69 | 12 | (2%) | 702 | ||
| 70–74 | 27 | (5%) | 573 | ||
| 75– | 22 | (5%) | 402 | ||
| T category | 1 | 13 | (3%) | 365 | 0.1869 |
| 2 | 15 | (2%) | 611 | exc NA | |
| 3 | 34 | (4%) | 762 | ||
| 4 | 0 | (0%) | 29 | ||
| NA | 1 | (9%) | 10 | ||
| Pretreatment PSA | ng/mL | 19.45 (3.30–329) | 15.072 (2.286–1454) | 0.2069 | |
| Gleason | ≤6 | 4 | (2%) | 166 | 0.1075 |
| score | 7 | 24 | (3%) | 889 | exc NA |
| 8≤ | 33 | (4%) | 720 | ||
| NA | 2 | 2 | |||
| NCCN risk | Low | 0 | (0%) | 33 | 0.0209 |
| classification | Intermediate | 12 | (3%) | 398 | excl. NA |
| High | 50 | (4%) | 1344 | ||
| NA | 1 | 2 | |||
| PSA failure | Yes | 12 | (5%) | 231 | 0.1835 |
| No | 51 | (3%) | 1550 | ||
| NA | 1 | ||||
| ADT | No | 1 | (1%) | 145 | 0.0979 |
| Yes | 62 | (4%) | 1637 | ||
| ADT <2-y | 17 | (3%) | 606 | ||
| ADT ≥2-y | 45 | (4%) | 1031 | ||
| Duration | 40 (0–113) | 35.5 (0–49) | 0.0096 | ||
| Neoadjuvant | (yes) | 62 | 1625 | ||
| (duration) | Months | 10 (4–55) | 9 (1–92) | ||
| Adjuvant | (yes) | 50 | 1209 | ||
| (duration) | Months | 36 (10–50) | 36 (1–134) | ||
| Modality | EBRT | 18 | (3%) | 655 | 0.1847 |
| HDR + EBRT | 45 | (4%) | 1127 |
| Variables | Strata | Elder ≥ 75 | Young < 75 | p-Value | ||
|---|---|---|---|---|---|---|
| n = 424 | n = 1416 | |||||
| No. or Median (range) | (%) | No. or Median (range) | (%) | |||
| T category | 1 | 87 | (21%) | 291 | (21%) | 0.3333 |
| 2 | 149 | (35%) | 477 | (34%) | ||
| 3 | 183 | (43%) | 613 | (43%) | ||
| 4 | 2 | (0.5%) | 27 | (2%) | ||
| NA | 3 | (0.7%) | 8 | (1%) | ||
| Pretreatment PSA | ng/mL | 15.039 (2.682–500) | 15.155 (2.286–1454) | 0.5979 | ||
| Gleason score | ≤6 | 39 | (9%) | 131 | (9%) | 0.5485 |
| 7 | 204 | (48%) | 709 | (50%) | ||
| 8≤ | 179 | (42%) | 574 | (41%) | ||
| NA | 2 | (0.5%) | 2 | (0.1%) | ||
| NCCN risk | Low | 6 | (1%) | 27 | (2%) | 0.0028 |
| classification | Intermediate | 80 | (19%) | 330 | (23%) | |
| High | 335 | (79%) | 1059 | (75%) | ||
| NA | 3 | (1%) | 0 | (0%) | ||
| ADT | Yes | 399 | (94%) | 1296 | (92%) | 0.0839 |
| No | 25 | (6%) | 120 | (9%) | ||
| Duration | 36 (0–102) | 33 (0–140) | 0.7073 | |||
| Neoadjuvant | (yes) | 62 | 1625 | |||
| (duration) | Months | 10 (4–55) | 9 (1–92) | |||
| Adjuvant | (yes) | 50 | 1209 | |||
| (duration) | Months | 36 (10–50) | 36 (1–134) | |||
| Follow-up | Months | 58.5 (2–155) | 68 (4–177) | <0.0001 | ||
| Modality | EBRT | 208 | (49%) | 460 | (33%) | <0.0001 |
| HDR + EBRT | 216 | (51%) | 956 | (68%) |
| Variables | Strata | ADT Duration | OCM (+) | OCM (-) | p-Value | |
|---|---|---|---|---|---|---|
| n = 63 | n = 1777 | |||||
| No. | OCM (+) % | No. | ||||
| Total | ADT < 2-y | 18 | (3%) | 602 | 0.0338 | |
| ADT ≥ 2-y | 45 | (4%) | 1031 | |||
| NCCN risk classification | Low | ADT < 2-y | 0 | (0%) | 26 | NA |
| ADT ≥ 2-y | 0 | (0%) | 7 | |||
| Intermediate | ADT < 2-y | 4 | (1%) | 267 | 0.0337 | |
| ADT ≥ 2-y | 8 | (6%) | 131 | |||
| High | ADT < 2-y | 14 | (3%) | 453 | 0.4013 | |
| ADT ≥ 2-y | 36 | (4%) | 891 | |||
| Age | Elder ≥ 75 | ADT < 2-y | 5 | (3%) | 181 | 0.0401 |
| ADT ≥ 2-y | 17 | (7%) | 221 | |||
| Young < 75 | ADT < 2-y | 13 | (2%) | 565 | 0.2283 | |
| ADT ≥ 2-y | 28 | (3%) | 810 |
| Variables | Strata | EBRT | HDR + EBRT | p-Value | ||
|---|---|---|---|---|---|---|
| n = 668 | n = 1172 | |||||
| No. or Median (range) | (%) | No. or Median (range) | (%) | |||
| Age | 50 | 25 | (4%) | 77 | (7%) | <0.0001 |
| 60 | 213 | (32%) | 501 | (43%) | ||
| 70 | 222 | (33%) | 378 | (32%) | ||
| 75- | 208 | (31%) | 216 | (18%) | ||
| T category | 1 | 140 | (21%) | 238 | (20%) | 0.0257 |
| 2 | 225 | (33%) | 401 | (34%) | exc NA | |
| 3 | 279 | (41%) | 517 | (44%) | ||
| 4 | 19 | (3%) | 19 | (2%) | ||
| NA | 5 | (1%) | 5 | (0%) | ||
| Pretreatment PSA | ng/mL | 16.2 (2.28–1454) | 14.7 (2.68–500) | <0.0001 | ||
| Gleason score | ≤6 | 68 | (10%) | 102 | (9%) | 0.0222 |
| 7 | 357 | (53%) | 556 | (47%) | exc NA | |
| 8≤ | 242 | (36%) | 511 | (44%) | ||
| NA | 1 | (0%) | 3 | (0%) | ||
| NCCN risk classification | Low | 22 | (3%) | 11 | (1%) | <0.0001 |
| Intermediate | 174 | (26%) | 236 | (20%) | exc NA | |
| High | 472 | (70%) | 922 | (79%) | ||
| NA | 0 | (0%) | 3 | (0%) | ||
| PSA failure | Yes | 148 | (22%) | 95 | (8%) | <0.0001 |
| No | 520 | (77%) | 1076 | (92%) | exc NA | |
| NA | 0 | (0%) | 1 | (0%) | ||
| ADT | Yes | 578 | (86%) | 1117 | (95%) | <0.0001 |
| No | 90 | (13%) | 55 | (5%) | ||
| Duration | 9 (0–140) | 43 (0–128) | 0.0274 | |||
| OCM | Yes | 18 | (3%) | 45 | (4%) | 0.194 |
| No | 650 | (97%) | 1127 | (96%) | ||
| Follow-up | Months | 61.0 (9–145) | 69 (9–177) | 0.0033 |
| Total | ADT ≥ 2Y | ADT < 2Y | ||
|---|---|---|---|---|
| n = 1076 | n = 764 | |||
| Cardiovascular | 2 | (0.2%) | 0 | (0.0%) |
| Pulmonary | 4 | (0.4%) | 2 | (0.3%) |
| Other malignancies | 15 | (1.4%) | 2 | (0.3%) |
| Other | 6 | (0.6%) | 4 | (0.5%) |
| Unknown | 18 | (1.7%) | 10 | (1.3%) |
| Elder ≥ 75 | n = 238 | n = 186 | ||
| Cardiovascular | 0 | (0.0%) | 0 | (0.0%) |
| Pulmonary | 2 | (0.8%) | 0 | (0.0%) |
| Other malignancies | 8 | (3.4%) | 1 | (0.5%) |
| Other | 1 | (0.4%) | 1 | (0.5%) |
| Unknown | 6 | (2.5%) | 3 | (1.6%) |
| Young < 75 | n = 838 | n = 578 | ||
| Cardiovascular | 2 | (0.2%) | 0 | (0.0%) |
| Pulmonary | 2 | (0.2%) | 2 | (0.3%) |
| Other malignancies | 7 | (0.8%) | 1 | (0.2%) |
| Other | 5 | (0.6%) | 3 | (0.5%) |
| Unknown | 12 | (1.4%) | 7 | (1.2%) |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yamazaki, H.; Masui, K.; Suzuki, G.; Aibe, N.; Shimizu, D.; Kimoto, T.; Yoshida, K.; Nakamura, S. Potential Risk of Other-Cause Mortality Due to Long-Term Androgen Deprivation Therapy in Elderly Patients with Clinically Localized Prostate Cancer Treated with Radiotherapy—A Confirmation Study. J. Clin. Med. 2020, 9, 2296. https://doi.org/10.3390/jcm9072296
Yamazaki H, Masui K, Suzuki G, Aibe N, Shimizu D, Kimoto T, Yoshida K, Nakamura S. Potential Risk of Other-Cause Mortality Due to Long-Term Androgen Deprivation Therapy in Elderly Patients with Clinically Localized Prostate Cancer Treated with Radiotherapy—A Confirmation Study. Journal of Clinical Medicine. 2020; 9(7):2296. https://doi.org/10.3390/jcm9072296
Chicago/Turabian StyleYamazaki, Hideya, Koji Masui, Gen Suzuki, Norihiro Aibe, Daisuke Shimizu, Takuya Kimoto, Ken Yoshida, and Satoaki Nakamura. 2020. "Potential Risk of Other-Cause Mortality Due to Long-Term Androgen Deprivation Therapy in Elderly Patients with Clinically Localized Prostate Cancer Treated with Radiotherapy—A Confirmation Study" Journal of Clinical Medicine 9, no. 7: 2296. https://doi.org/10.3390/jcm9072296
APA StyleYamazaki, H., Masui, K., Suzuki, G., Aibe, N., Shimizu, D., Kimoto, T., Yoshida, K., & Nakamura, S. (2020). Potential Risk of Other-Cause Mortality Due to Long-Term Androgen Deprivation Therapy in Elderly Patients with Clinically Localized Prostate Cancer Treated with Radiotherapy—A Confirmation Study. Journal of Clinical Medicine, 9(7), 2296. https://doi.org/10.3390/jcm9072296