Motor and Cognitive Performance in Patients with Liver Cirrhosis with Minimal Hepatic Encephalopathy

 ,
,  , ,
, ,  , ,
, ,  ,
,  ,
,
Abstract
:
1. Introduction
2. Materials and Methods
2.1. Study Design and Participants
2.2. Procedures
2.3. Cognitive-Functional Assessment and Outcomes
- Mini-Mental State Examination (MMSE), a series of tests to measure and grade cognitive impairment [20].
- Aprendizaje Verbal España-Complutense Test (TAVEC): to measure learning and memory, consisting of different subtests: immediate memory with possibility of learning, immediate memory without possibility of learning, short-term free memory, short-term memory-guided or with semantic keys, long-term free memory, long-term memory-guided or with semantic keys, and long-term recognition [25,26]. In addition, an overall score could also be obtained by combining the short-term free memory and short-term memory-guided, termed global short-term memory, and combining long-term memory and long-term memory-guided, which is called global long-term memory.
- Functioning Assessment Short Test (FAST): clinically assesses psychological functioning in the following areas, (a) autonomy, (b) work, (c) cognitive, (d) finances, (e) relationships and (f) leisure [30]. It also calculates a total score of functioning.
2.4. Biomechanical Gait Assessment and Outcomes
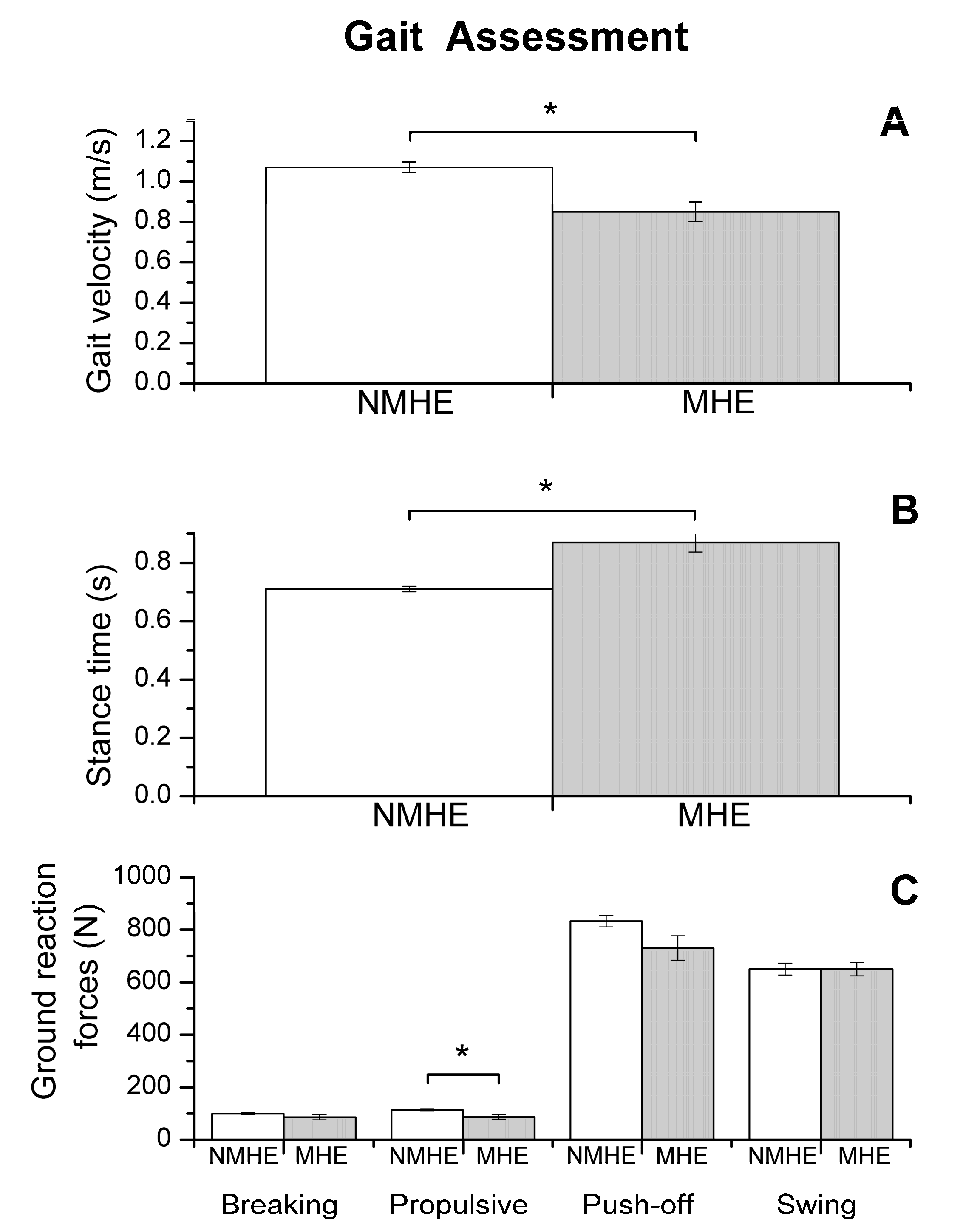
2.4.1. Gait
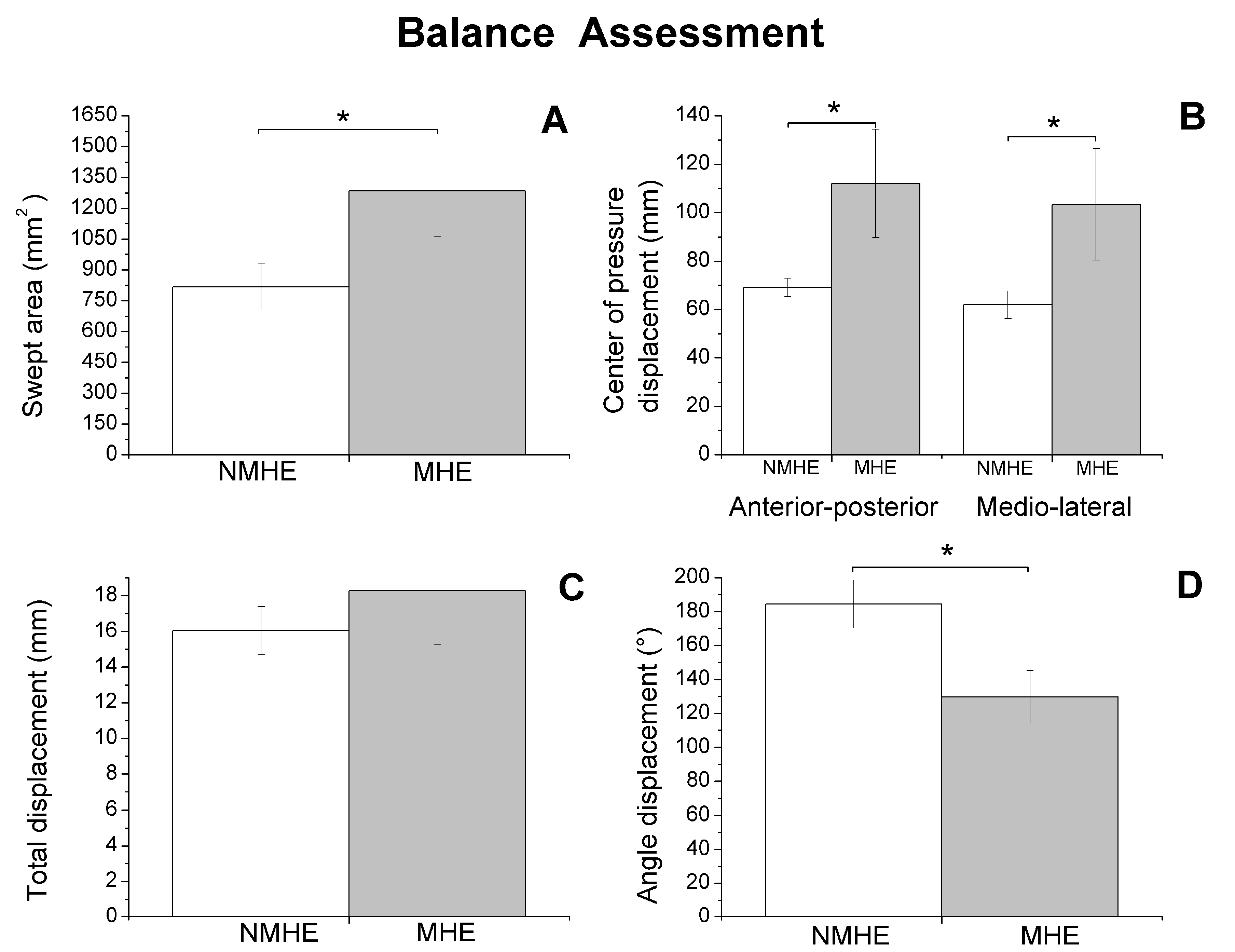
2.4.2. Balance
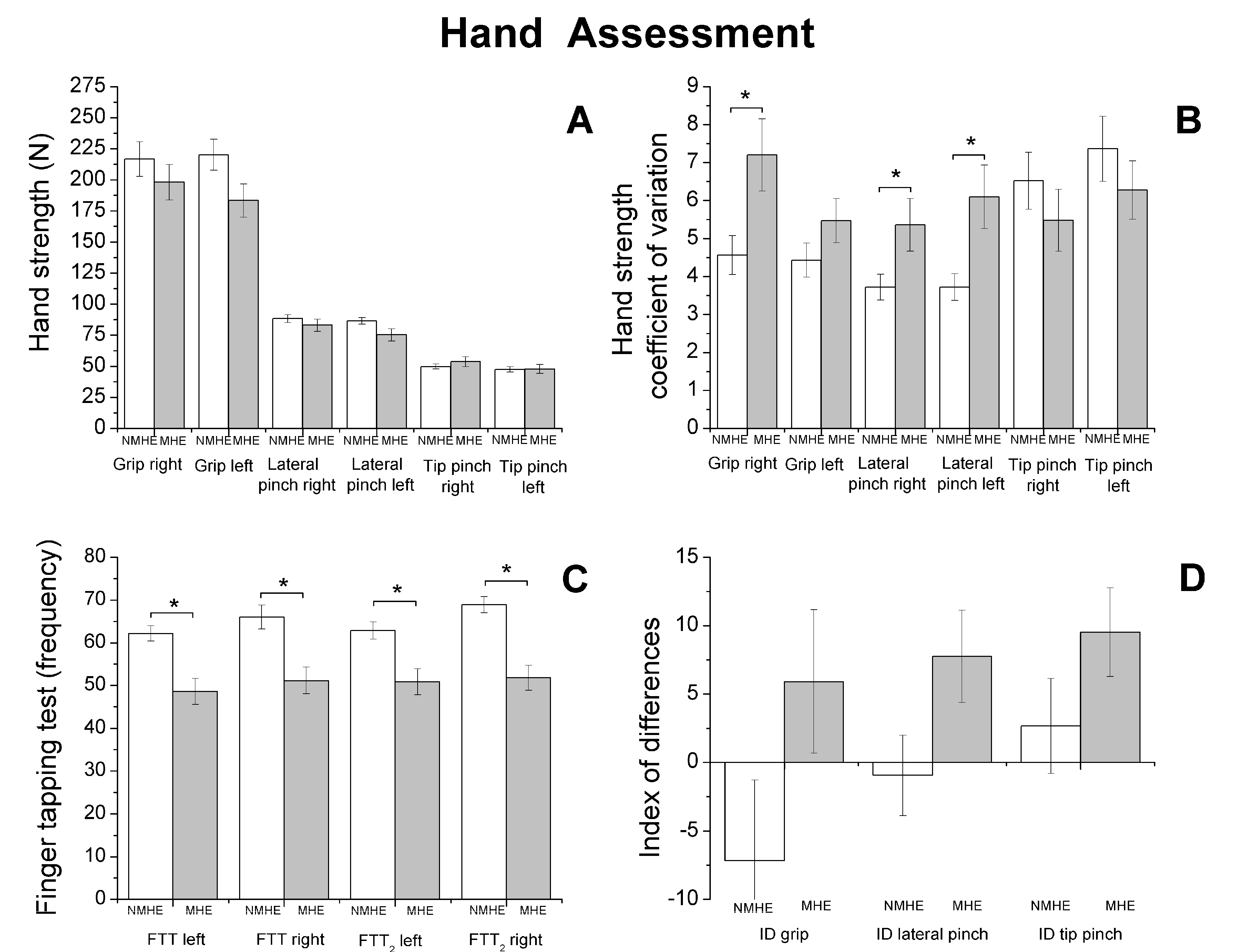
2.4.3. Hand Strength
2.4.4. Manual Motor Speed
2.5. Statistical Analysis
3. Results
3.1. Participants’ Characteristics
3.2. Cognition and Mental State
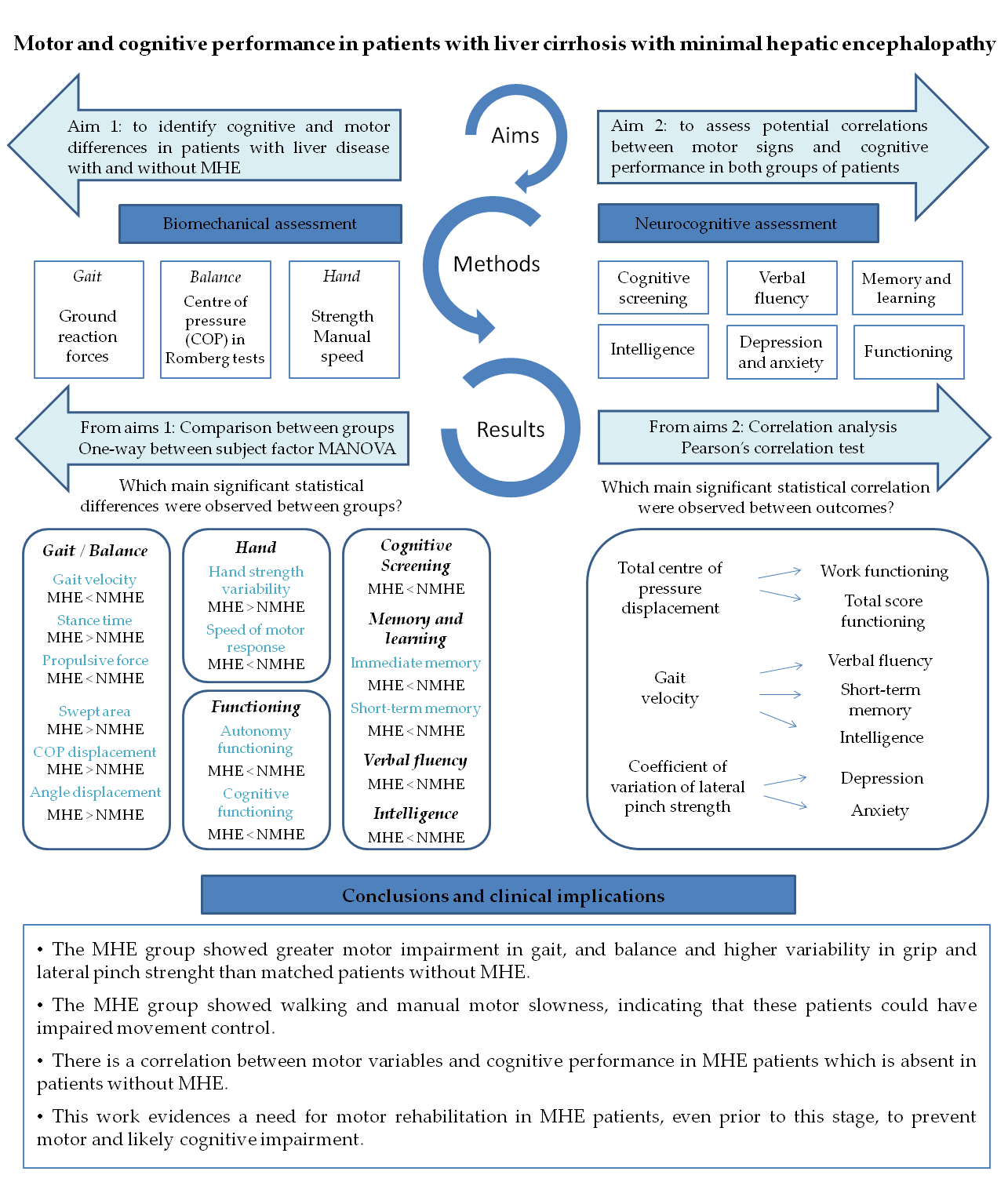
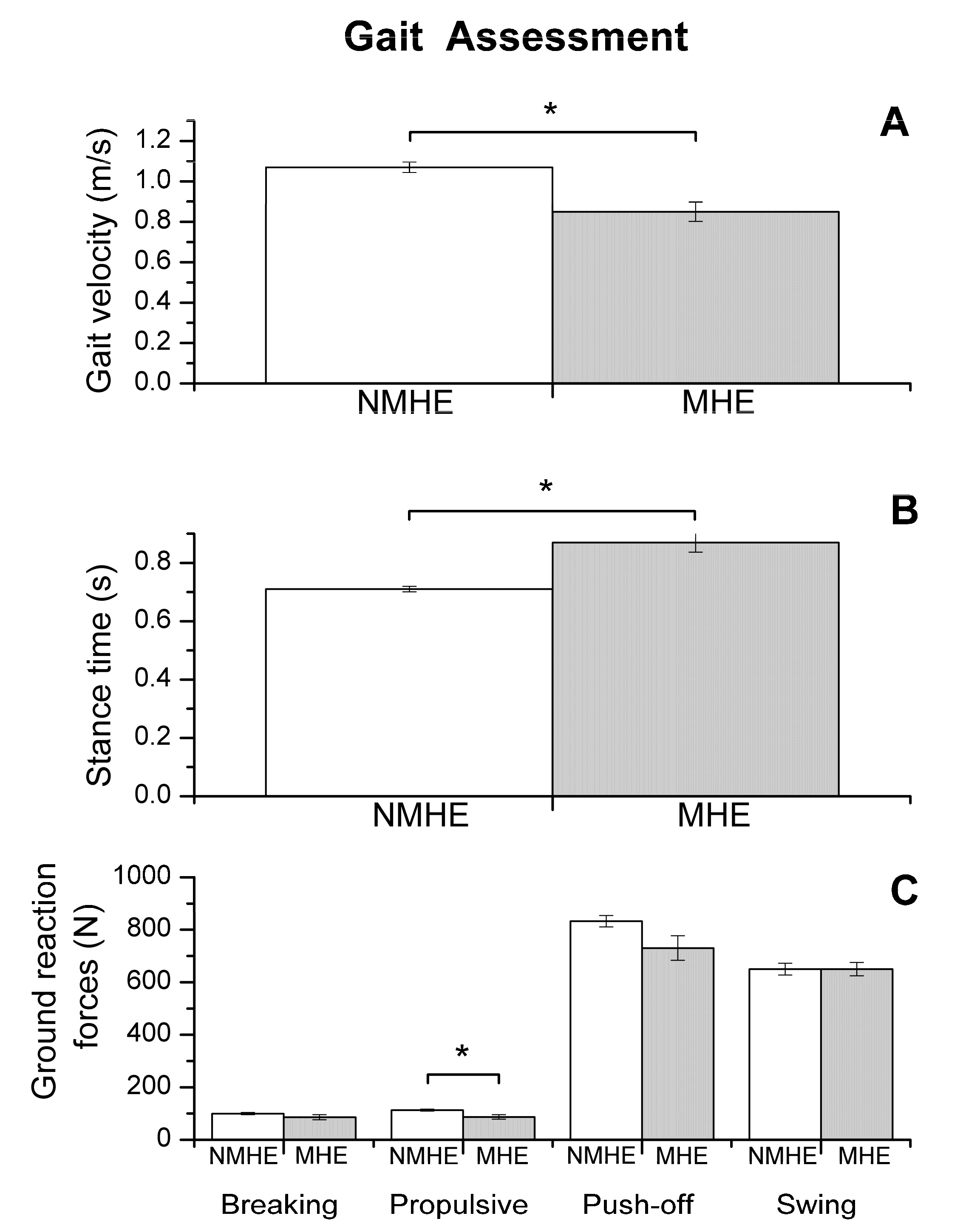
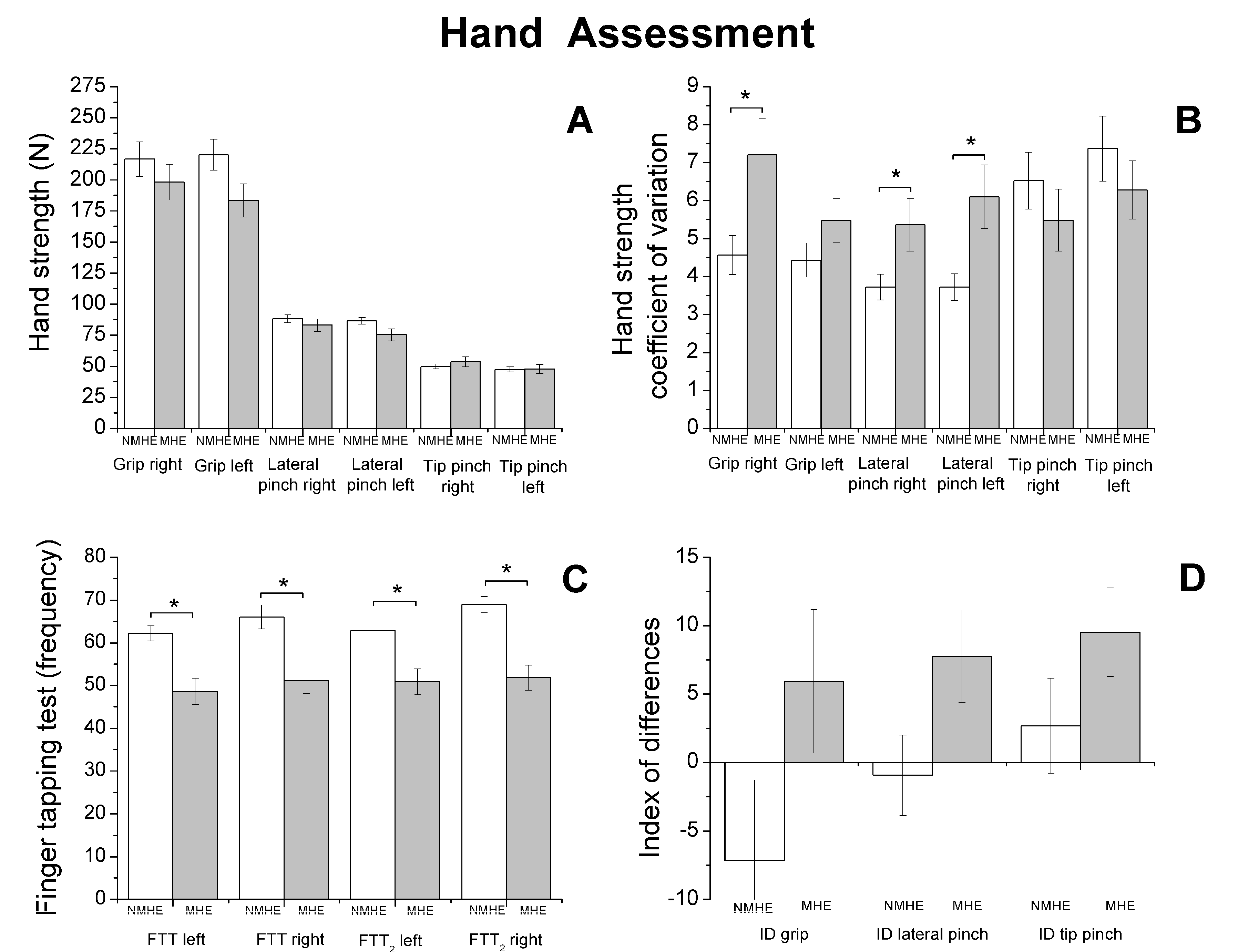
3.3. Motor Performance
3.4. Correlation between Motor and Cognitive/Mental Performance
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
Abbreviations
| COP | center of pressure |
| CV | coefficient of variation percentage |
| FAST | Functioning Assessment Short Test |
| FTT | Finger Tapping Test |
| GRF | Ground reaction force |
| HA | Hamilton Anxiety Rating Scale |
| HD | Hamilton Depression Rating Scale |
| HE | hepatic encephalopathy |
| ID | Index of Difference |
| MHE | minimal hepatic encephalopathy |
| MMSE | Mini-Mental State Examination |
| PHES | Psychometric Hepatic Encephalopathy Score |
| TAVEC | Aprendizaje Verbal España-Complutense Test |
| VFP | Verbal Fluency Phonemic |
| VFS | Verbal Fluency Semantic |
| WAIS | Wechsler Adult Intelligence Scale III |
References
- Vilstrup, H.; Amodio, P.; Bajaj, J.; Cordoba, J.; Ferenci, P.; Mullen, K.D.; Weissenborn, K.; Wong, P. Hepatic encephalopathy in chronic liver disease: 2014 practice guideline by the american association for the study of liver diseases and the european association for the study of the liver. Hepatology 2014, 60, 715–735. [Google Scholar] [CrossRef]
- Felipo, V. Hepatic encephalopathy: Effects of liver failure on brain function. Nat. Rev. Neurosci. 2013, 14, 851–858. [Google Scholar] [CrossRef] [PubMed]
- Poordad, F.F. Review article: The burden of hepatic encephalopathy. Aliment. Pharmacol. Ther. 2007, 25, 3–9. [Google Scholar] [CrossRef] [PubMed]
- Trivedi, H.D.; Tapper, E.B. Interventions to improve physical function and prevent adverse events in cirrhosis. Gastroenterol. Rep. 2018, 6, 13–20. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kok, B.; Tandon, P. Frailty in patients with cirrhosis. Curr. Treat. Options Gastroenterol. 2018, 16, 215–225. [Google Scholar] [CrossRef]
- Ney, M.; Tangri, N.; Dobbs, B.; Bajaj, J.; Rolfson, D.; Ma, M.; Ferguson, T.; Bhardwaj, P.; Bailey, R.J.; Abraldes, J.; et al. Predicting hepatic encephalopathy-related hospitalizations using a composite assessment of cognitive impairment and frailty in 355 patients with cirrhosis. Am. J. Gastroenterol. 2018, 113, 1506–1515. [Google Scholar] [CrossRef]
- Román, E.; Córdoba, J.; Torrens, M.; Torras, X.; Villanueva, C.; Vargas, V.; Guarner, C.; Soriano, G. Minimal hepatic encephalopathy is associated with falls. Am. J. Gastroenterol. 2011, 106, 476–482. [Google Scholar] [CrossRef] [PubMed]
- Urios, A.; Mangas-Losada, A.; Gimenez-Garzó, C.; González-López, O.; Giner-Durán, R.; Serra, M.A.; Noe, E.; Felipo, V.; Montoliu, C. Altered postural control and stability in cirrhotic patients with minimal hepatic encephalopathy correlate with cognitive deficits. Liver Int. 2017, 37, 1013–1022. [Google Scholar] [CrossRef]
- Ridola, L.; Nardelli, S.; Gioia, S.; Riggio, O. Quality of life in patients with minimal hepatic encephalopathy. World J. Gastroenterol. 2018, 24, 5446–5453. [Google Scholar] [CrossRef]
- Nardone, R.; Taylor, A.C.; Höller, Y.; Brigo, F.; Lochner, P.; Trinka, E. Minimal hepatic encephalopathy: A review. Neurosci. Res. 2016, 111, 1–12. [Google Scholar] [CrossRef]
- Amodio, P.; Montagnese, S.; Gatta, A.; Morgan, M.Y. Characteristics of minimal hepatic encephalopathy. Metab. Brain Dis. 2004, 19, 253–267. [Google Scholar] [CrossRef] [PubMed]
- Weissenborn, K.; Heidenreich, S.; Ennen, J.; Rückert, N.; Hecker, H. Attention deficits in minimal hepatic encephalopathy. Metab. Brain Dis. 2001, 16, 13–19. [Google Scholar] [CrossRef] [PubMed]
- Felipo, V.; Ordoño, J.F.; Urios, A.; El Mlili, N.; Giménez-Garzó, C.; Aguado, C.; González-Lopez, O.; Giner-Duran, R.; Serra, M.A.; Wassel, A.; et al. Patients with minimal hepatic encephalopathy show impaired mismatch negativity correlating with reduced performance in attention tests. Hepatology 2012, 55, 530–539. [Google Scholar] [CrossRef] [PubMed]
- Ferenci, P.; Lockwood, A.; Mullen, K.; Tarter, R.; Weissenborn, K.; Blei, A.T. Hepatic encephalopathy—Definition, nomenclature, diagnosis, and quantification: Final report of the Working Party at the 11th World Congresses of Gastroenterology, Vienna, 1998. Hepatology 2002, 35, 716–721. [Google Scholar] [CrossRef] [PubMed]
- Weissenborn, K.; Ennen, J.C.; Schomerus, H.; Rückert, N.; Hecker, H. Neuropsychological characterization of hepatic encephalopathy. J. Hepatol. 2001, 34, 768–773. [Google Scholar] [CrossRef]
- Mechtcheriakov, S.; Graziadei, I.W.; Kugener, A.; Schuster, I.; Mueller, J.; Hinterhuber, H.; Vogel, W.; Marksteiner, J. Motor dysfunction in patients with liver cirrhosis: Impairment of handwriting. J. Neurol. 2006, 253, 349–356. [Google Scholar] [CrossRef]
- Montoliu, C.; Cauli, O.; Urios, A.; ElMlili, N.; Serra, M.A.; Giner-Duran, R.; González-Lopez, O.; Del Olmo, J.A.; Wassel, A.; Rodrigo, J.M.; et al. 3-nitro-tyrosine as a peripheral biomarker of minimal hepatic encephalopathy in patients with liver cirrhosis. Am. J. Gastroenterol. 2011, 106, 1629–1637. [Google Scholar] [CrossRef]
- Felipo, V.; Urios, A.; Giménez-Garzó, C.; Cauli, O.; Andrés-Costa, M.J.; González, O.; Serra, M.A.; Sánchez-González, J.; Aliaga, R.; Giner-Durán, R.; et al. Non invasive blood flow measurement in cerebellum detects minimal hepatic encephalopathy earlier than psychometric tests. World J. Gastroenterol. 2014, 20, 11815–11825. [Google Scholar] [CrossRef] [Green Version]
- Romero Gómez, M.; Córdoba, J.; Jover, R.; del Olmo, J.; Fernández, A.; Flavià, M.; Compañy, L.; Poveda, M.J.; Felipo, V. Normality tables in the Spanish population for psychometric tests used in the diagnosis of minimal hepatic encephalopathy. Med. Clin. (Barc.) 2006, 127, 246–249. [Google Scholar] [CrossRef]
- Folstein, M.F.; Folstein, S.E.; McHugh, P.R. “Mini-mental state”: A practical method for grading the cognitive state of patients for the clinician. J. Psychiatr. Res. 1975, 12, 189–198. [Google Scholar] [CrossRef]
- Shao, Z.; Janse, E.; Visser, K.; Meyer, A.S. What do verbal fluency tasks measure? Predictors of verbal fluency performance in older adults. Front. Psychol. 2014, 5, 772. [Google Scholar] [CrossRef] [PubMed]
- Ruff, R.M.; Light, R.H.; Parker, S.B.; Levin, H.S. Benton controlled oral word association test: Reliability and updated norms. Arch. Clin. Neuropsychol. 1996, 11, 329–338. [Google Scholar] [CrossRef] [PubMed]
- Benton, A.L. Differential behavioral effects in frontal lobe disease. Neuropsychologia 1968, 6, 53–60. [Google Scholar] [CrossRef]
- Hughes, B. Missile wounds of the brain. A Study of Psychological Deficits. J. Neurol. Neurosurg. Psychiatry. 1970, 33, 551. [Google Scholar] [CrossRef] [Green Version]
- Benedet, M.J.; Alejandre, M.Á. TAVEC: Test de aprendizaje verbal España-Complutense: Manual; Tea: Madrid, Spain, 2014. [Google Scholar]
- García-García, R.; Cruz-Gómez, Á.J.; Urios, A.; Mangas-Losada, A.; Forn, C.; Escudero-García, D.; Kosenko, E.; Torregrosa, I.; Tosca, J.; Giner-Durán, R.; et al. Learning and memory impairments in patients with minimal hepatic encephalopathy are associated with structural and functional connectivity alterations in hippocampus. Sci. Rep. 2018, 8, 9664. [Google Scholar] [CrossRef] [Green Version]
- Kharbanda, P.S.; Saraswat, V.A.; Dhiman, R.K. Minimal hepatic encephalopathy: Diagnosis by neuropsychological and neurophysiologic methods. Indian J. Gastroentero. J. Indian Soc. Gastroenterol. 2003, 22, S37–S41. [Google Scholar]
- Hassan, E.A.; Abd El-Rehim, A.S.; Seifeldein, G.S.; Shehata, G.A. Minimal hepatic encephalopathy in patients with liver cirrhosis: Magnetic resonance spectroscopic brain findings versus neuropsychological changes. Arab. J. Gastroenterol. 2014, 15, 108–113. [Google Scholar] [CrossRef]
- Ramos-Brieva, J.A.; Cordero Villafáfila, A. Validation of the Castillian version of the Hamilton Rating Scale for Depression. Actas Luso Esp. Neurol. Psiquiatr. Cienc. Afines. 1986, 14, 324–334. [Google Scholar]
- Knight, M.J.; Air, T.; Baune, B.T. The role of cognitive impairment in psychosocial functioning in remitted depression. J. Affect. Disord. 2018, 235, 129–134. [Google Scholar] [CrossRef] [PubMed]
- Tapper, E.B.; Konerman, M.; Murphy, S.; Sonnenday, C.J. Hepatic encephalopathy impacts the predictive value of the Fried Frailty Index. Am. J. Transplant. 2018, 18, 2566–2570. [Google Scholar] [CrossRef] [Green Version]
- Balaguer García, R.; Pitarch Corresa, S.; Baydal Bertomeu, J.M.; Morales Suárez-Varela, M.M. Static posturography with dynamic tests. Usefulness of biomechanical parameters in assessing vestibular patients. Acta Otorrinolaringol. Esp. 2012, 63, 332–338. [Google Scholar] [CrossRef] [PubMed]
- Peydro de Moya, F.; Montero Vilela, J.; Baydal Bertomeu, J.M.; Garrido Jaén, J.D.; Bermejo Bosch, I.; Page del Pozo, A.; Porcar Seder, R.; Morales Martín, I.; Barberà i Guillem, R. Objetivamos los gestos característicos de la mano. Rev. Biomecánica Inst. Biomecánica Valencia 2012, 58, 47–50. [Google Scholar]
- Peydro de Moya, F.; Rubio Hervás, M.; Bermejo Bosch, I.; Garrido Jaén, J.D.; Baydal Bertomeu, J.M.; Matey González, F.; Corté s Fabregat, A.; Ballester Fernández, A. ¿Cómo se miden la fuerza y la fatiga de la mano? Rev. Biomecánica 2011, 56, 49–51. [Google Scholar]
- Lorenzo-Agudo, M.A.; Santos-García, P.; Sánchez-Belizón, D. Determinación de los valores normales de fuerza muscular de puño y pinza en una población laboral. Rehabilitación 2007, 41, 220–227. [Google Scholar] [CrossRef]
- Su, C.-Y.; Lin, J.-H.; Chien, T.-H.; Cheng, K.-F.; Sung, Y.-T. Grip strength in different positions of elbow and shoulder. Arch. Phys. Med. Rehabil. 1994, 75, 812–815. [Google Scholar] [CrossRef]
- Mathiowetz, V.; Weber, K.; Volland, G.; Kashman, N. Reliability and validity of grip and pinch strength evaluations. J. Hand Surg. 1984, 9, 222–226. [Google Scholar] [CrossRef]
- Lin, C.-H.; Sung, W.-H.; Chiang, S.-L.; Lee, S.-C.; Lu, L.-H.; Wang, P.-C.; Wang, X.-M. Influence of aging and visual feedback on the stability of hand grip control in elderly adults. Exp. Gerontol. 2019, 119, 74–81. [Google Scholar] [CrossRef]
- Matuoka, J.Y.; Kurita, G.P.; Nordly, M.; Sjøgren, P.; de Mattos-Pimenta, C.A. Validation of a battery of neuropsychological tests for patients with metastatic cancer. Clin. Nurs. Res. 2019. [Google Scholar] [CrossRef]
- Lauridsen, M.M.; Thiele, M.; Kimer, N.; Vilstrup, H. The continuous reaction times method for diagnosing, grading, and monitoring minimal/covert hepatic encephalopathy. Metab. Brain Dis. 2013, 28, 231–234. [Google Scholar] [CrossRef]
- Fried, L.P.; Tangen, C.M.; Walston, J.; Newman, A.B.; Hirsch, C.; Gottdiener, J.; Seeman, T.; Tracy, R.; Kop, W.J.; Burke, G.; et al. Frailty in older adults: Evidence for a phenotype. J. Gerontol. A Biol. Sci. Med. Sci. 2001, 56, M146–M156. [Google Scholar] [CrossRef]
- Lamb, D.G.; Correa, L.N.; Seider, T.R.; Mosquera, D.M.; Rodriguez, J.A.; Salazar., L.; Schwartz, Z.J.; Cohen, R.A.; Falchook, A.D.; Heilman, K.M. The aging brain: Movement speed and spatial control. Brain Cogn. 2016, 109, 105–1111. [Google Scholar] [CrossRef]
- Guevara, M.; Baccaro, M.E.; Gómez-Ansón, B.; Frisoni, G.; Testa, C.; Torre, A.; Molinuevo, J.L.; Rami, L.; Pereira, G.; Urtasun Sotil, E.; et al. Cerebral magnetic resonance imaging reveals marked abnormalities of brain tissue density in patients with cirrhosis without overt hepatic encephalopathy. J. Hepatol. 2011, 55, 564–573. [Google Scholar] [CrossRef]
- Joebges, E.M.; Heidemann, M.; Schimke, N.; Hecker, H.; Ennen, J.C.; Weissenborn, K. Bradykinesia in minimal hepatic encephalopathy is due to disturbances in movement initiation. J. Hepatol. 2003, 38, 273–280. [Google Scholar] [CrossRef]
- Giménez-Garzó, C.; Garcés, J.J.; Urios, A.; Mangas-Losada, A.; García-García, R.; González-López, O.; Giner-Durán, R.; Escudero-García, D.; Serra, M.A.; Soria, E.; et al. The PHES battery does not detect all cirrhotic patients with early neurological deficits, which are different in different patients. PLoS ONE 2017, 12, e0171211. [Google Scholar] [CrossRef]
- Groeneweg, M.; Quero, J.; De Bruijn, I.; Hartmann, I.J.; Essink-bot, M.L.; Hop, W.C.; Schalm, S.W. Subclinical hepatic encephalopathy impairs daily functioning. Hepatology 1998, 28, 45–49. [Google Scholar] [CrossRef] [PubMed]
- Åberg, F. From prolonging life to prolonging working life: Tackling unemployment among liver-transplant recipients. World J. Gastroenterol. 2016, 22, 3701–3711. [Google Scholar] [CrossRef] [PubMed]
- Murphy, S.L.; Richardson, J.K.; Blackwood, J.; Martinez, B.; Tapper, E.B. Neurocognitive and muscular capacities are associated with frailty in adults with cirrhosis. Dig. Dis. Sci. 2020. [Google Scholar] [CrossRef]
- Rao, A.K.; Uddin, J.; Gillam, A.; Louis, E.D. Cognitive motor interference during dual-task gait in essential tremor. Gait Posture 2013, 38, 403–409. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Holtzer, R.; Verghese, J.; Xue, X.; Lipton, R.B. Cognitive processes related to gait velocity: Results from the einstein aging study. Neuropsychology 2006, 20, 215–223. [Google Scholar] [CrossRef] [PubMed]
- Alvarez, J.; Emory, E. Executive function and the frontal lobes: A meta-analytic review. Neuropsychol. Rev. 2006, 16, 17–42. [Google Scholar] [CrossRef] [PubMed]
- García-García, R.; Cruz-Gómez, A.J.; Mangas-Losada, A.; Urios, A.; Forn, C.; Escudero-García, D.; Kosenko, E.; Ordoño, J.F.; Tosca, J.; Giner-Durán, R.; et al. Reduced resting state connectivity and gray matter volume correlate with cognitive impairment in minimal hepatic encephalopathy. PLoS ONE 2017, 12, e0186463. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lai, J.C.; Volk, M.L.; Strasburg, D.; Alexander, N. Performance-based measures associate with frailty in patients with end-stage liver disease. Transplantation 2016, 100, 2656–2660. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lai, J.C.; Covinsky, K.E.; Dodge, J.L.; Boscardin, W.J.; Segev, D.L.; Roberts, J.P.; Feng, S. Development of a novel frailty index to predict mortality in patients with end-stage liver disease. Hepatology 2017, 66, 564–574. [Google Scholar] [CrossRef] [PubMed]
- Rochester, L.; Baker, K.; Hetherington, V.; Jones, D.; Willems, A.-M.; Kwakkel, G.; Van Wegen, E.; Lim, I.; Nieuwboer, A. Evidence for motor learning in Parkinson’s disease: Acquisition, automaticity and retention of cued gait performance after training with external rhythmical cues. Brain Res. 2010, 1319, 103–111. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Demographical and Clinical Variables | Patients with MHE (n = 28) | Patients without MHE (n = 38) | Between Groups |
|---|---|---|---|
| Age (years) a | 63.42 (9.17) | 61.12 (8.34) | 0.52 |
| Weight (kg) a | 79.56 (13.35) | 79.36 (13.14) | 0.83 |
| Height (m) a | 1.66 (0.07) | 1.66 (0.07) | 0.98 |
| BMI a | 28.68 (3.90) | 28.82 (4.81) | 0.75 |
| Child–Pugh score (A/B/C) b | 20/7/1 | 28/9/1 | 0.76 |
| MELD score a | 9.7 (2.6) | 9.4 (3) | 0.66 |
| Gender | M:21/F:7 | M:30/F:8 | 0.70 |
| Etiology of cirrhosis | 0.05 | ||
| Alcohol b | 14 | 20 | |
| HCV/HBV/HCV + alcohol b | 4/1/1 | 13/0/1 | |
| NASH b | 5 | 4 | |
| Primary biliary cirrhosis b | 2 | 0 | |
| Autoimmune | 1 | 0 | |
| Ascites b | 12 | 8 | 0.08 |
| Esophageal varices b | 19 | 18 | 0.20 |
| Outcomes | Patients with MHE | Patients without MHE | Post-Hoc p-Value | ||
|---|---|---|---|---|---|
| Mean | SD | Mean | SD | ||
| Functioning Assessment Short Test (FAST) | |||||
| Autonomy functioning | 4.43 | 3.17 | 2.74 | 1.98 | 0.03 * |
| Work functioning | 13.18 | 4.78 | 12.76 | 4.90 | 0.16 |
| Cognitive functioning | 6.14 | 3.96 | 3.16 | 2.11 | 0.00 * |
| Finances functioning | 1.14 | 1.63 | 0.55 | 1.03 | 0.40 |
| Relationships functioning | 4.93 | 3.87 | 5.13 | 2.88 | 0.35 |
| Leisure functioning | 3.00 | 2.34 | 1.89 | 1.81 | 0.10 |
| Total functioning | 32.82 | 12.80 | 26.24 | 9.77 | 0.19 |
| Hamilton depression and anxiety rating scale | |||||
| Depression | 6.71 | 6.33 | 6.71 | 4.77 | 0.76 |
| Anxiety | 8.86 | 9.66 | 8.32 | 5.23 | 0.83 |
| Mini-Mental State Examination Test (MMSE) | |||||
| Cognitive state | 26.35 | 2.88 | 28.13 | 1.42 | 0.03 * |
| Aprendizaje Verbal España-Complutense Test (TAVEC) | |||||
| Immediate memory and learning | 34.26 | 9.65 | 39.39 | 9.85 | 0.02 * |
| Immediate memory | 3.19 | 1.27 | 3.95 | 1.39 | 0.02 * |
| Short-term memory | 5.52 | 3.27 | 8.26 | 2.70 | 0.01 * |
| Short-term memory-guided | 7.26 | 2.89 | 9.24 | 2.82 | 0.09 |
| Global short-term memory | 12.78 | 5.32 | 17.24 | 5.30 | 0.05 |
| Long-term memory | 6.78 | 2.91 | 8.53 | 2.81 | 0.05 |
| Long-term memory-guided | 7.56 | 2.89 | 9.16 | 3.03 | 0.14 |
| Global long-term memory | 14.33 | 5.28 | 17.53 | 5.60 | 0.10 |
| Long-term recognition | 13 | 2.44 | 13.61 | 1.94 | 0.04 * |
| Verbal Fluency Test | |||||
| Semantic verbal fluency | 13.96 | 4.04 | 20.38 | 5.46 | 0.00 * |
| Phonemic verbal fluency | 19.93 | 9.41 | 33.81 | 10.94 | 0.00 * |
| Total verbal fluency | 33.89 | 12.30 | 54.19 | 14.43 | 0.00 * |
| Wechsler Adult Intelligence Scale III (WAIS) | |||||
| Intelligence | 33.19 | 12.39 | 43.37 | 7.17 | 0.00 * |
| Cognitive Outcomes | Patients with MHE | Patients without MHE |
|---|---|---|
| Gait Velocity | ||
| Short-term memory (TAVEC test) | 0.51 (0.02) * | 0.27 (0.11) |
| Semantic verbal fluency (Verbal Fluency Test) | 0.66 (0.00) * | 0.41 (0.01) * |
| Phonemic verbal fluency (Verbal Fluency Test) | 0.61 (0.00) * | 0.41 (0.01) * |
| Intelligence (WAIS test) | 0.50 (0.05) * | 0.03 (0.87) |
| Total center of pressure displacement | ||
| Work functioning (FAST test) | −0.81 (0.00) * | −0.12 (0.49) |
| Total functioning (FAST test) | −0.74 (0.01) * | 0.07 (0.69) |
| Right lateral pinch coefficient of variation | ||
| Depression (Hamilton test) | 0.54 (0.01) * | 0.27 (0.11) |
| Anxiety (Hamilton test) | 0.52 (0.02) * | 0.21 (0.22) |
| Right hand motor speed (bilateral performance) | ||
| Finances functioning (FAST test) | 0.50 (0.04) * | 0.31 (0.06) |
| Left hand motor speed (bilateral performance) | ||
| Short-term memory (TAVEC test) | 0.53 (0.02) * | 0.12 (0.49) |
| Total score of memory and learning (TAVEC test) | 0.48 (0.04) * | 0.21 (0.23) |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
San Martín-Valenzuela, C.; Borras-Barrachina, A.; Gallego, J.-J.; Urios, A.; Mestre-Salvador, V.; Correa-Ghisays, P.; Ballester, M.-P.; Escudero-García, D.; Tosca, J.; Montón, C.; et al. Motor and Cognitive Performance in Patients with Liver Cirrhosis with Minimal Hepatic Encephalopathy. J. Clin. Med. 2020, 9, 2154. https://doi.org/10.3390/jcm9072154
San Martín-Valenzuela C, Borras-Barrachina A, Gallego J-J, Urios A, Mestre-Salvador V, Correa-Ghisays P, Ballester M-P, Escudero-García D, Tosca J, Montón C, et al. Motor and Cognitive Performance in Patients with Liver Cirrhosis with Minimal Hepatic Encephalopathy. Journal of Clinical Medicine. 2020; 9(7):2154. https://doi.org/10.3390/jcm9072154
Chicago/Turabian StyleSan Martín-Valenzuela, Constanza, Aroa Borras-Barrachina, Juan-José Gallego, Amparo Urios, Víctor Mestre-Salvador, Patricia Correa-Ghisays, María-Pilar Ballester, Desamparados Escudero-García, Joan Tosca, Cristina Montón, and et al. 2020. "Motor and Cognitive Performance in Patients with Liver Cirrhosis with Minimal Hepatic Encephalopathy" Journal of Clinical Medicine 9, no. 7: 2154. https://doi.org/10.3390/jcm9072154
APA StyleSan Martín-Valenzuela, C., Borras-Barrachina, A., Gallego, J.-J., Urios, A., Mestre-Salvador, V., Correa-Ghisays, P., Ballester, M.-P., Escudero-García, D., Tosca, J., Montón, C., Ríos, M.-P., Kosenko, E., Felipo, V., Tabares-Seisdedos, R., Selva-Vera, G., & Montoliu, C. (2020). Motor and Cognitive Performance in Patients with Liver Cirrhosis with Minimal Hepatic Encephalopathy. Journal of Clinical Medicine, 9(7), 2154. https://doi.org/10.3390/jcm9072154