Computerized Cognitive Rehabilitation Training for Ugandan Seniors Living with HIV: A Validation Study

 , , and
, , and
Abstract
1. Introduction
2. Experimental Section
2.1. Study Design
2.2. Setting
2.3. Recruitment and Enrolment Process
2.4. Eligibility and Exclusion Criteria
2.5. Intervention Allocation and Standard of Care (SOC)
2.6. Measurements
2.7. Study Outcomes
2.7.1. Feasibility/Acceptability
2.7.2. Cognitive Performance
- (a)
- Gross motor function—evaluated using Timed Gait test time to quantify amount of time (in seconds) taken to complete walking a 10-yard distance and back.
- (b)
- Fine motor function—evaluated using two tests: (i) Finger Tapping (number of taps within 10 s) and (ii) the Grooved Pegboard Test, which measures the amount of time (in seconds) it takes to place 25 slotted pegs into rows of randomly positioned slots on a board.
- (c)
- Executive function—measured using Color Trails2 test (time to completion of a complex task requiring attention to two aspects of problem solving simultaneously) and verbal (semantic) fluency (number correct animals named within 60 s) to quantify proficiency in completing tasks that require planning, organizing, prioritizing, focus/attention, multi-tasking, and inhibition of irrational impulses.
- (d)
- Speed of Processing—measures how long it takes individuals to complete a cognitive visual scanning and simple sequencing task using Color Trails 1 (time (in seconds) to task completion) and Digit Symbol test in which participants are asked to draw in small symbols in spaces under numbers corresponding to number/symbol pairs at the top of the test sheet (number correct matches within 90 s).
- (e)
- Attention/Short-term working memory—measured as number correct on Digit Span Forward and Digit Span Backward tests.
- (f)
- Verbal Learning/Memory—measures ability of individuals to acquire and retrieve components of memory using the WHO-UCLA Auditory Verbal Learning Test.
2.7.3. Quality of Life
2.7.4. Frailty Related Phenotype
2.8. Statistical Issues
2.9. Ethical Approval
3. Results
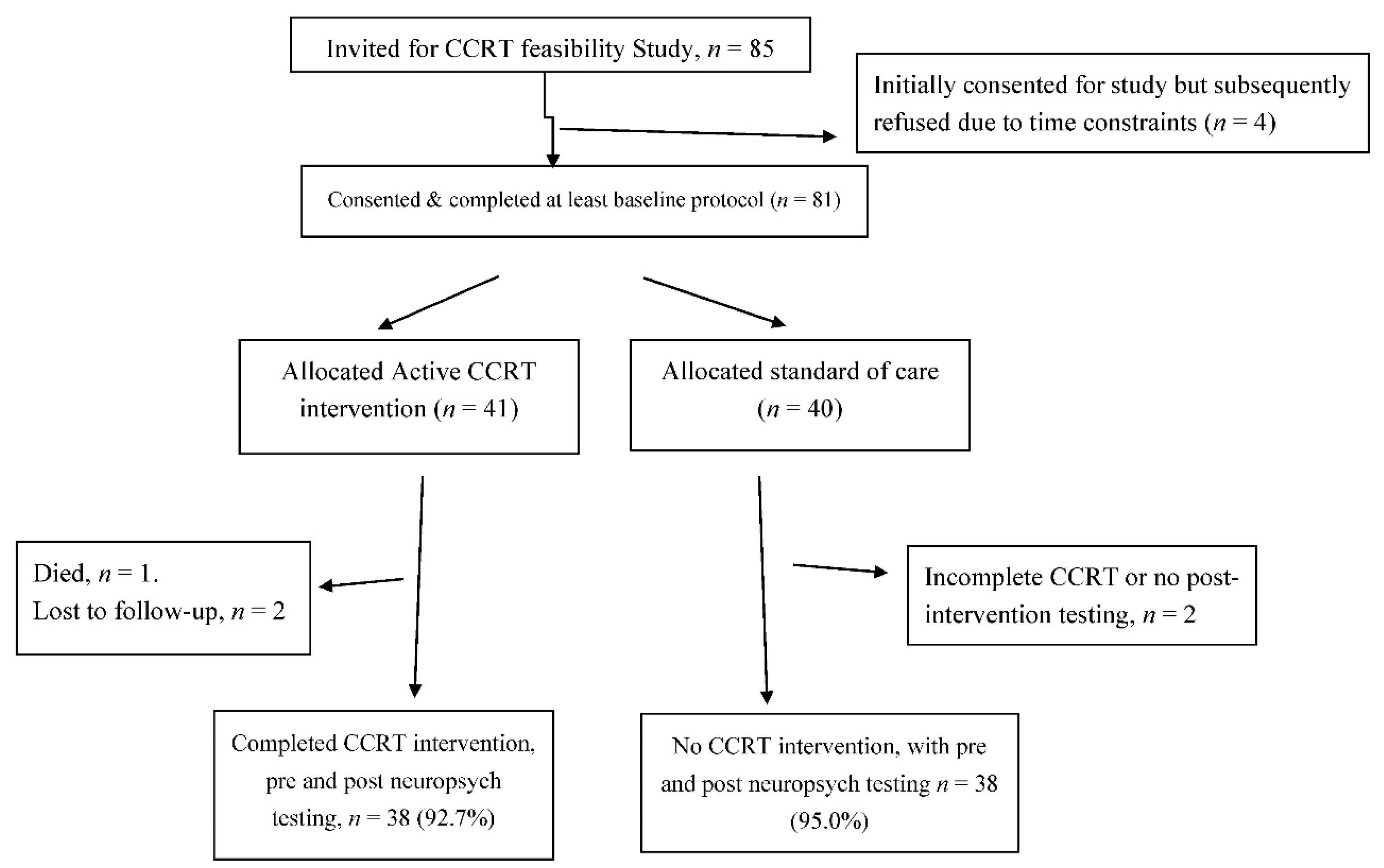
3.1. Description of Enrolled Participants
3.2. Feasibility/Acceptability of CCRT
3.3. Effect of CCRT on Neurocognitive Performance, QOL and Frailty according to HIV Status
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Hayutin, A.M. Graying of the Global Population. Public Policy Aging Rep. 2007, 17, 12–17. [Google Scholar] [CrossRef]
- Walker, J.M.; Harrison, F.E. Shared Neuropathological Characteristics of Obesity, Type 2 Diabetes and Alzheimer’s Disease: Impacts on Cognitive Decline. Nutrients 2015, 7, 7332–7357. [Google Scholar] [CrossRef] [PubMed]
- Glahn, D.C.; Kent, J.; Sprooten, E.; Diego, V.; Winkler, A.M.; Curran, J.E.; McKay, D.R.; Knowles, E.E.; Carless, M.A.; Göring, H.H.H.; et al. Genetic basis of neurocognitive decline and reduced white-matter integrity in normal human brain aging. Proc. Natl. Acad. Sci. USA 2013, 110, 19006–19011. [Google Scholar] [CrossRef] [PubMed]
- Chang, H.; Hawley, N.L.; Kalyesubula, R.; Siddharthan, T.; Checkley, W.; Knauf, F.; Rabin, T. Challenges to hypertension and diabetes management in rural Uganda: A qualitative study with patients, village health team members, and health care professionals. Int. J. Equity Health 2019, 18, 38. [Google Scholar] [CrossRef]
- Brands, A.M.; Berg, E.V.D.; Manschot, S.M.; Biessels, G.J.; Kappelle, L.J.; De Haan, E.H.; Kessels, R.P.C. A detailed profile of cognitive dysfunction and its relation to psychological distress in patients with type 2 diabetes mellitus. J. Int. Neuropsychol. Soc. 2007, 13, 288–297. [Google Scholar] [CrossRef] [PubMed]
- Gottesman, R.F.; Schneider, A.L.; Albert, M.; Alonso, A.; Bandeen-Roche, K.; Coker, L.; Coresh, J.; Knopman, D.; Power, M.C.; Rawlings, A.M.; et al. Midlife hypertension and 20-year cognitive change: The atherosclerosis risk in communities neurocognitive study. JAMA Neurol. 2014, 71, 1218–1227. [Google Scholar] [CrossRef]
- De Roos, A.; Van Der Grond, J.; Mitchell, G.; Westenberg, J. Magnetic Resonance Imaging of Cardiovascular Function and the Brain: Is Dementia a Cardiovascular-Driven Disease? Circulation 2017, 135, 2178–2195. [Google Scholar] [CrossRef]
- Grady, C.L. The cognitive neuroscience of ageing. Nat. Rev. Neurosci. 2012, 13, 491–505. [Google Scholar] [CrossRef]
- Stern, A.L.; Ghura, S.; Gannon, P.J.; Akay-Espinoza, C.; Phan, J.; Yee, A.; Vassar, R.; Gelman, B.B.; Kolson, D.L.; Jordan-Sciutto, K.L. BACE1 Mediates HIV-Associated and Excitotoxic Neuronal Damage through an APP-Dependent Mechanism. J. Neurosci. 2018, 38, 4288–4300. [Google Scholar] [CrossRef]
- Becker, J.T.; Dew, M.A.; Aizenstein, H.J.; Lopez, O.L.; Morrow, L.; Saxton, J.; Tárraga, L. A pilot study of the effects of internet-based cognitive stimulation on neuropsychological function in HIV disease. Disabil. Rehabilit. 2012, 34, 1848–1852. [Google Scholar] [CrossRef]
- Vance, D.E.; Fazeli, P.L.; Gakumo, C.A. The impact of neuropsychological performance on everyday functioning between older and younger adults with and without HIV. J. Assoc. Nurses AIDS Care 2012, 24, 112–125. [Google Scholar] [CrossRef] [PubMed]
- Malkasian, D.R.; Diamond, M.C. The Effects of Environmental Manipulation On The Morphology of The Neonate Rat Brain. Int. J. Neurosci. 1971, 2, 161–169. [Google Scholar] [CrossRef]
- Marusic, U.; Giordani, B.; Moffat, S.D.; Petrič, M.; Dolenc, P.; Pišot, R.; Kavcic, V. Computerized cognitive training during physical inactivity improves executive functioning in older adults. Aging Neuropsychol. Cogn. 2016, 25, 49–69. [Google Scholar] [CrossRef]
- Marusic, U.; Kavcic, V.; Giordani, B.; Gerževič, M.; Meeusen, R.; Pišot, R. Computerized spatial navigation training during 14 days of bed rest in healthy older adult men: Effect on gait performance. Psychol. Aging 2015, 30, 334–340. [Google Scholar] [CrossRef] [PubMed]
- Hempel, A.; Schröder, J.; Caraballo, N.M.G.; Giesel, F.L.; Amann, M.; Meyer, H.; Wüstenberg, T.; Essig, M. Plasticity of Cortical Activation Related to Working Memory during Training. Am. J. Psychiatry 2004, 161, 745–747. [Google Scholar] [CrossRef] [PubMed]
- Klingberg, T. Training and plasticity of working memory. Trends Cogn. Sci. 2010, 14, 317–324. [Google Scholar] [CrossRef]
- Nikolaidis, A.; Voss, M.W.; Lee, H.; Vo, L.T.K.; Kramer, A.F. Parietal plasticity after training with a complex video game is associated with individual differences in improvements in an untrained working memory task. Front. Hum. Neurosci. 2014, 8, 169. [Google Scholar] [CrossRef] [PubMed]
- Boivin, M.J.; Nakasujja, N.; Sikorskii, A.; Opoka, R.O.; Giordani, B. A Randomized Controlled Trial to Evaluate if Computerized Cognitive Rehabilitation Improves Neurocognition in Ugandan Children with HIV. AIDS Res. Hum. Retrovir. 2016, 32, 743–755. [Google Scholar] [CrossRef] [PubMed]
- Boivin, M.J.; Busman, R.A.; Parikh, S.M.; Bangirana, P.; Page, C.; Opoka, R.O.; Giordani, B. A pilot study of the neuropsychological benefits of computerized cognitive rehabilitation in Ugandan children with HIV. Neuropsychology 2010, 24, 667–673. [Google Scholar] [CrossRef]
- Bangirana, P.; Giordani, B.; John, C.C.; Page, C.; Opoka, R.O.; Boivin, M.J. Immediate Neuropsychological and Behavioral Benefits of Computerized Cognitive Rehabilitation in Ugandan Pediatric Cerebral Malaria Survivors. J. Dev. Behav. Pediatr. 2009, 30, 310–318. [Google Scholar] [CrossRef]
- Bangirana, P.; Allebeck, P.; Boivin, M.J.; John, C.C.; Page, C.; Ehnvall, A.; Musisi, S. Cognition, behaviour and academic skills after cognitive rehabilitation in Ugandan children surviving severe malaria: A randomised trial. BMC Neurol. 2011, 11, 96. [Google Scholar] [CrossRef] [PubMed]
- Willis, S.L.; Tennstedt, S.L.; Marsiske, M.; Ball, K.; Elias, J.; Koepke, K.M.; Morris, J.N.; Rebok, G.W.; Unverzagt, F.W.; Stoddard, A.M.; et al. Long-term Effects of Cognitive Training on Everyday Functional Outcomes in Older Adults. JAMA 2006, 296, 2805–2814. [Google Scholar] [CrossRef] [PubMed]
- Pressler, S.J.; Titler, M.; Koelling, T.M.; Riley, P.L.; Jung, M.; Hoyland-Domenico, L.; Ronis, D.L.; Smith, D.G.; Bleske, B.E.; Dorsey, S.G.; et al. Nurse-Enhanced Computerized Cognitive Training Increases Serum Brain-Derived Neurotropic Factor Levels and Improves Working Memory in Heart Failure. J. Card. Fail. 2015, 21, 630–641. [Google Scholar] [CrossRef] [PubMed]
- Pressler, S.J.; Therrien, B.; Riley, P.L.; Chou, C.-C.; Ronis, D.L.; Koelling, T.M.; Smith, D.G.; Sullivan, B.J.; Frankini, A.-M.; Giordani, B. Nurse-Enhanced Memory Intervention in Heart Failure: The MEMOIR Study. J. Card. Fail. 2011, 17, 832–843. [Google Scholar] [CrossRef]
- Schein, R.L.; Koenig, H.G. The Center for Epidemiological Studies-Depression (CES-D) Scale: Assessment of depression in the medically ill elderly. Int. J. Geriatr. Psychiatry 1997, 12, 436–446. [Google Scholar] [CrossRef]
- Glover, D.A.; Garcia-Aracena, E.F.; Lester, P.; Rice, E.; Rothram-Borus, M.J. Stress Biomarkers as Outcomes for HIV+ Prevention: Participation, Feasibility and Findings among HIV+ Latina and African American Mothers. AIDS Behav. 2009, 14, 339–350. [Google Scholar] [CrossRef]
- Nakasujja, N.; Skolasky, R.L.; Musisi, S.; Allebeck, P.; Robertson, K.R.; Ronald, A.R.; Katabira, E.; Clifford, D.B.; Sacktor, N. Depression symptoms and cognitive function among individuals with advanced HIV infection initiating HAART in Uganda. BMC Psychiatry 2010, 10, 44. [Google Scholar] [CrossRef]
- Norman, G.; Sloan, J.A.; Wyrwich, K.W. Interpretation of Changes in Health-related Quality of Life. Med. Care 2003, 41, 582–592. [Google Scholar] [CrossRef]
- Erder, M.H.; Santanello, N.; Hays, R.D. Assessing the clinical significance of patient-reported outcomes: Examples drawn from a recent meeting of the drug information association (DIA). Clin. Ther. 2003, 25, D12–D13. [Google Scholar] [CrossRef]
- Norman, G.R.; Sloan, J.A.; Wyrwich, K.W. Interpretation of changes in health-related quality of life—The remarkable universality of half a standard deviation. Med. Care 2003, 41, 582–592. [Google Scholar] [CrossRef]
- Rothrock, N.E.; Hays, R.D.; Spritzer, K.; Yount, S.E.; Riley, W.; Cella, D. Relative to the general US population, chronic diseases are associated with poorer health-related quality of life as measured by the Patient-Reported Outcomes Measurement Information System (PROMIS). J. Clin. Epidemiol. 2010, 63, 1195–1204. [Google Scholar] [CrossRef] [PubMed]
- Cella, D.; Eton, D.; Fairclough, D.; Bonomi, P.; Heyes, A.; Silberman, C.; Wolf, M.; Johnson, D. What is a clinically meaningful change on the Functional Assessment of Cancer Therapy–Lung (FACT-L) Questionnaire? Results from Eastern Cooperative Oncology Group (ECOG) Study 5592. J. Clin. Epidemiol. 2002, 55, 285–295. [Google Scholar] [CrossRef]
- Cavallo, M.; Hunter, E.M.; van der Hiele, K.; Angilletta, C. Computerized Structured Cognitive Training in Patients Affected by Early-Stage Alzheimer’s Disease is Feasible and Effective: A Randomized Controlled Study. Arch. Clin. Neuropsychol. 2016, 31, 868–876. [Google Scholar] [CrossRef] [PubMed]
- Strenziok, M.; Parasuraman, R.; Clarke, E.; Cisler, D.S.; Thompson, J.C.; Greenwood, P.M. Neurocognitive enhancement in older adults: Comparison of three cognitive training tasks to test a hypothesis of training transfer in brain connectivity. NeuroImage 2014, 85, 1027–1039. [Google Scholar] [CrossRef]
- Cody, S.L.; Fazeli, P.L.; Vance, D.E. Feasibility of a Home-Based Speed of Processing Training Program in Middle-Aged and Older Adults with HIV. J. Neurosci. Nurs. 2015, 47, 247–254. [Google Scholar] [CrossRef]
- Ownby, R.; Acevedo, A. A pilot study of cognitive training with and without transcranial direct current stimulation to improve cognition in older persons with HIV-related cognitive impairment. Neuropsychiatr. Dis. Treat. 2016, 12, 2745–2754. [Google Scholar] [CrossRef]
- Towe, S.L.; Patel, P.; Meade, C.S. The Acceptability and Potential Utility of Cognitive Training to Improve Working Memory in Persons Living with HIV: A Preliminary Randomized Trial. J. Assoc. Nurses AIDS Care 2017, 28, 633–643. [Google Scholar] [CrossRef] [PubMed]
- Vance, D.E.; Jensen, M.; Tende, F.; Raper, J.L.; Morrison, S.; Fazeli, P.L. Individualized-Targeted Computerized Cognitive Training to Treat HIV-Associated Neurocognitive Disorder: An Interim Descriptive Analysis. J. Assoc. Nurses AIDS Care 2018, 29, 604–611. [Google Scholar] [CrossRef]
- Herrera, C.; Chambon, C.; Michel, B.F.; Paban, V.; Alescio-Lautier, B. Positive effects of computer-based cognitive training in adults with mild cognitive impairment. Neuropsychologia 2012, 50, 1871–1881. [Google Scholar] [CrossRef]
- Hu, M.; Wu, X.; Shu, X.; Hu, H.; Chen, Q.; Peng, L.; Feng, H. Effects of computerised cognitive training on cognitive impairment: A meta-analysis. J. Neurol. 2019, 1–9. [Google Scholar] [CrossRef]
- Hardy, D.J.; Vance, D.E. The Neuropsychology of HIV/AIDS in Older Adults. Neuropsychol. Rev. 2009, 19, 263–272. [Google Scholar] [CrossRef] [PubMed]
- Bozoki, A.C.; Radovanović, M.; Winn, B.; Heeter, C.; Anthony, J.C. Effects of a computer-based cognitive exercise program on age-related cognitive decline. Arch. Gerontol. Geriatr. 2013, 57, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Ciccarelli, N.; Fabbiani, M.; Baldonero, E.; Fanti, I.; Cauda, R.; Di Giambenedetto, S.; Silveri, M.C. Effect of Aging and Human Immunodeficiency Virus Infection on Cognitive Abilities. J. Am. Geriatr. Soc. 2012, 60, 2048–2055. [Google Scholar] [CrossRef] [PubMed]
- Vance, D.E.; Fazeli, P.L.; Ross, L.A.; Wadley, V.G.; Ball, K. Speed of Processing Training with Middle-Age and Older Adults with HIV: A Pilot Study. J. Assoc. Nurses AIDS Care 2012, 23, 500–510. [Google Scholar] [CrossRef]
- Kaur, J.; Dodson, J.E.; Steadman, L.; Vance, D.E. Predictors of Improvement Following Speed of Processing Training in Middle-Aged and Older Adults with HIV. J. Neurosci. Nurs. 2014, 46, 23–33. [Google Scholar] [CrossRef][Green Version]
- Li, H.; Li, J.; Li, N.; Li, B.; Wang, P.; Zhou, T. Cognitive intervention for persons with mild cognitive impairment: A meta-analysis. Ageing Res. Rev. 2011, 10, 285–296. [Google Scholar] [CrossRef]


{kind=link}
| CCRT, n = 41 | No CCRT, n = 40 | p-Value | |
|---|---|---|---|
| Age (years) | 59.7 (8.2) | 60.0 (6.6) | 0.894 |
| n (%) | n (%) | ||
| Female Sex | 24 (58.5) | 20 (50.0) | 0.441 |
| HIV Status | |||
| HIV+ | 19 (47.5) | 20 (50.0) | 0.823 |
| Mean (SD) Years on HAART (if HIV+) | 8.8 (5.6) | 9.7 (3.8) | 0.564 |
| Years of Education | |||
| ≤Primary | 21 (55.3) | 17 (44.7) | 0.539 |
| Some/Completed Ordinary Levels | 10 (26.3) | 14 (36.8) | |
| Some Advanced Levels or Higher | 6 (15.8) | 6 (15.8) | |
| Number of non-HIV comorbid diagnoses | |||
| 0 | 11 (27.5) | 13 (33.3) | 0.838 |
| 1 | 18 (45.0) | 16 (41.0) | |
| 2 | 6 (15.0) | 7 (18.0) | |
| 3+ | 5 (12.5) | 3 (7.7) | |
| Lipid Profile Tests | Mean (SD) | Mean (SD) | |
| High Cholesterol | 16 (40.0) | 14 (35.0) | 0.559 |
| Low HDL | 16 (40.0) | 14 (35.0) | 0.559 |
| High LDL | 19 (47.5) | 15 (37.5) | 0.534 |
| High Triglycerides | 10 (25.0) | 8 (20.0) | 0.556 |
| High CRP | 2 (5.0) | 7 (17.5) | 0.127 |
| CESD Score | 16.7 (11.0) | 16.1 (9.5) | 0.816 |
| Frailty Score | 3.1 (1.9) | 2.7 (1.5) | 0.273 |
| Quality of Life Score | 72.1 (11.1) | 71.0 (9.4) | 0.621 |
| Body Mass Index | 24.4 (4.7) | 23.6 (6.0) | 0.562 |
| Hemoglobin | 14.3 (2.4) | 14.2 (1.9) | 0.746 |
| Stress Scores | mean (SD) | mean (SD) | |
| Acute Stress | 20.5 (6.2) | 18.9 (7.0) | 0.311 |
| Recent Life Stress (within 5 years) | 11.8 (5.6) | 11.3 (4.9) | 0.678 |
| Number of Lifetime Adversity | 5.5 (3.8) | 5.6 (3.3) | 0.963 |
| Immune Measures | n = 34, mean (SD) | n = 34, mean (SD) | |
| Absolute CD4 cell count | 612.8 (323) | 663 (320) | 0.516 |
| CD4/CD8 Ratio | 1.2 (0.6) | 1.3 (0.9) | 0.418 |
| Neuropsychological Test Battery | Mean (SD) | Mean (SD) | |
| 1. Timed Gait (time, s) | 12.8 (7.6) | 12.4 (4.2) | 0.819 |
| 2. Verbal Fluency (Total Correct) | 12.5 (2.9) | 12.3 (3.4) | 0.779 |
| 3. Symbol Digit Modality (number correct) | 23.3 (12.3) | 22.8 (11.7) | 0.868 |
| 4. Finger Tapping (number of taps) | 32.9 (7.4) | 33.6 (9.3) | 0.707 |
| 5. Overall (Forward + Backward) | 8.5 (3.3) | 7.3 (2.8) | 0.108 |
| 6. Color Trails [100 × (T2−T1)/t1] | 52.5 (54.4) | 51.8 (46.6) | 0.949 |
| 7. Grooved Pegboard Test (time, s) | |||
| Non-Dominant Hand | 150.9 (55.7) | 146.0 (49.7) | 0.677 |
| Dominant Hand | 123.2 (47.8) | 119.5 (48.3) | 0.739 |
| 8. WHO UCLA Verbal Learning Test (number correct) | |||
| Sum of Immediate Recalls (Trials 1–5) | 8.4 (1.7) | 7.9 (1.8) | 0.291 |
| Interference List Recall (Trial 6) | 5.0 (1.9) | 4.6 (2.2) | 0.335 |
| Post Interference List Recall (Trial 7) | 8.0 (2.5) | 7.7 (2.5) | 0.563 |
| Delayed Recall of First list (Trial 8) | 7.8 (2.6) | 7.9 (2.7) | 0.864 |
| Delayed Recall & Recognition (Trial 9) | 12.9 (2.1) | 12.6 (2.7) | 0.530 |
| HIV+, n = 40 | HIV−, n = 41 | p-Value | |
|---|---|---|---|
| Age (years) | 58.1 (7.3) | 61.6 (7.3) | 0.033 |
| n (%) | n (%) | ||
| Female Sex | 24 (58.5) | 20 (50.0) | 0.823 |
| median (range) Years on HAART (if HIV+) | 10 (1 to 18) | n/a | |
| Years of Education | |||
| ≤Primary | 21 (55.3) | 21 (52.5) | 0.501 |
| Some/Completed O’Levels | 10 (26.3) | 14 (35.0) | |
| Some A-Levels or Higher | 8 (20) | 5 (12.5) | |
| Number of non-HIV comorbid diagnoses | 1.05 (1.5) | 1.15 (1.6) | 0.658 |
| Lipid Profile Tests | Mean (SD) | Mean (SD) | |
| Cholesterol | 5.0(1.13) | 4.90 (0.99) | |
| HDL | 1.40 (0.40) | 1.40 (0.50) | 0.929 |
| LDL | 2.92 (1.01) | 3.12 (1.04) | 0.403 |
| Triglycerides | 1.66 (1.3) | 1.35 (0.46) | 0.192 |
| CRP | 6562 (16464) | 3310 (5068) | 0.267 |
| CESD Score | 15.1 (11.5) | 17.7 (8.8) | 0.430 |
| Frailty Score | 3.1 (1.9) | 2.9 (1.5) | 0.501 |
| Quality of Life Score | 74 (11.0) | 69.0 (9.3) | 0.045 |
| Body Mass Index | 23.5 (5.1) | 24.6 (5.7) | 0.379 |
| Hemoglobin | 13.8 (1.6) | 14.8 (2.5) | 0.0376 |
| Stress Scores | Mean (SD) | Mean (SD) | |
| Acute Stress | 18.1 (6.4) | 21.2 (6.6) | 0.039 |
| Recent Life Stress (within 5 years) | 11.7 (6.2) | 11.3 (4.1) | 0.794 |
| Number of Lifetime Adversity | 5.5 (3.6) | 5.6 (3.6) | 0.963 |
| Immune Measures | n = 34, | n = 34, | |
| Mean (SD) | Mean (SD) | ||
| Absolute CD4 cell count | 564 (319) | 722 (304) | 0.042 |
| CD4/CD8 Ratio | 0.85 (0.38) | 1.75 (0.80) | <0.001 |
| Neuropsychological Test Battery | Mean (SD) | Mean (SD) | |
| 1. Timed Gait (time, s) | 13.9 (7.8) | 11.4 (3.3) | 0.075 |
| 2. Verbal Fluency (Total Correct) | 12.2(3.1) | 12.9 (2.5) | 0.365 |
| 3. Symbol Digit Modality (number correct) | 22.8 (11.6) | 23.2 (12.4) | 0.867 |
| 4. Finger Tapping (number of taps) | 30.7 (9.2) | 35.7 (6.3) | 0.005 |
| 5a. Score digit forward (simple attention) | 3.7 (1.8) | 4.5 (1.9) | 0.054 |
| 5b. Score digit backward (short term verbal memory) | 3.4 (1.4) | 4.1 (1.9) | 0.064 |
| 5. Overall (Forward + Backward) | 7.1 (2.9) | 8.6 (3.2) | 0.034 |
| 6. Color Trails [100 × (T2 − T1)/t1] | 107.3 (68.5) | 84.0 (56) | 0.100 |
| 7. Grooved Pegboard Test (time, s) | |||
| Non-Dominant Hand | 0.17 (1.04) | −0.17 (0.94) | 0.128 |
| Dominant Hand | 0.21 (1.1) | −0.21 (0.85) | 0.060 |
| 8. WHO UCLA Verbal Learning Test (Number Correct) | |||
| Sum of Immediate Recalls (Trials 1–5) | 8.0 (1.7) | 8.3 (2.5) | 0.438 |
| Interference List Recall (Trial 6) | 5.0 (1.9) | 5.0 (1.7) | 0.438 |
| Post Interference List Recall (Trial 7) | 7.4 (2.3) | 8.1 (2.4) | 0.158 |
| Delayed Recall of First list (Trial 8) | 7.5 (2.4) | 8.3 (2.4) | 0.198 |
| Delayed Recall & Recognition (Trial 9) | 12.7 (2.4) | 12.9 (2.5) | 0.689 |
| LS Means (SE) | β (95% CI) | Effect Size | p-Value | Adj.R2 | ||
|---|---|---|---|---|---|---|
| CCRT | No CCRT | |||||
| WHO UCLA Learning Tests (# Correct) | ||||||
| Immediate Recall (trials 1–5) | 9.94 (0.20) | 9.60 (0.20) | 0.33 (−0.29, 0.86) | 0.25 | 0.243 | 0.46 |
| Interference List Recall (trial 6) | 5.44 (0.28) | 5.72 (0.27) | −0.28 (−1.02, 0.46) | −0.16 | 0.407 | 0.25 |
| Post Interference List Recall (trial 7) | 10.1 (0.35) | 9.1 (0.35) | 1.00 (0.02, 1.98) | 0.43 | 0.046 | 0.30 |
| Delayed Recall (trial 8) | 10.2 (0.36) | 9.2 (0.35) | 1.04 (0.06, 2.02) | 0.47 | 0.038 | 0.41 |
| Word Recognition (trial 9) | 13.7 (0.32) | 13.6 (0.32) | 0.09 (−0.50, 0.99) | 0.04 | 0.841 | 0.12 |
| Digit Span Test (# correct) | ||||||
| Short term auditory memory/simple attention | 4.5 (0.19) | 4.8 (0.19) | −0.36 (−0.88, 0.17) | −0.29 | 0.186 | 0.34 |
| Short-term verbal memory | 4.4 (0.24) | 4.01 (0.25) | 0.45 (−0.21, 1.12) | 0.29 | 0.116 | 0.18 |
| Overall score | 8.76 (0.35) | 8.72 (0.34) | 0.03 (−0.91, 0.97) | 0.01 | 0.949 | 0.34 |
| Color Trails (time, s) | 99.5 (9.7) | 112.9 (9.7) | −13.4 (−39.8, 14.0) | −0.21 | 0.327 | 0.05 |
| Finger Tapping Test (time, s) | 38.1 (0.85) | 37.3 (0.87) | 0.83 (−1.6, 3.2) | 0.15 | 0.498 | 0.05 |
| Grooved Peg Board (time, s) | ||||||
| Grooved Pegboard NDH | 0.06 (0.11) | −0.12 (0.12) | 0.18 (−0.16, 0.51) | 0.24 | 0.296 | 0.45 |
| Grooved Pegboard DH | 0.07 (0.10) | −0.14 (0.11) | 0.21 (−0.07, 0.50) | 0.32 | 0.143 | 0.51 |
| Verbal Fluency | ||||||
| Verbal Fluency (Tot. Correct) | 13.4 (0.85) | 12.2 (0.91) | 1.25 (−0.09, 2.58) | 0.38 | 0.068 | 0.21 |
| Timed Gait (time, s) | 11.4 (0.52) | 12.1 (0.52) | −0.65 (−2.1, 0.83) | −0.20 | 0.401 | 0.15 |
| Symbol Digit Modality (# correct) | 24.5 (1.9) | 26.3 2.0) | −1.78 (−4.74, 1.19) | −0.25 | 0.239 | 0.63 |
| Frailty score | 1.98 (0.35) | 2.09 (0.38) | −0.12 (−0.74, 0.50) | −0.09 | 0.714 | 0.22 |
| Quality of Life Score | 72.1 (2.6) | 74.7 (2.8) | −2.64 (−6.7, 1.4) | −0.28 | 0.206 | 0.50 |
| Among HIV-Positive Older Ugandans | Among HIV-Negative Older Ugandans | |||||||
|---|---|---|---|---|---|---|---|---|
| CCRT | No CCRT | Estimated Effect | CCRT | No CCRT | Estimated Effect | |||
| LS Means (SE) | LS Means (SE) | β (95% CI) | Effect Size (p-Value) | LS Means (SE) | LS Means (SE) | β (95% CI) | Effect Size (p-Value) | |
| WHO UCLA Learning Tests (# Correct) | ||||||||
| Immediate Recall (trials 1–5) | 10.1 (0.39) | 9.2 (0.43) | 0.91 (0.08, 1.73) | 0.69 (0.032) | 9.83 (0.42) | 9.9 (0.43) | −0.19 (−0.96, 0.57) | −0.14 (0.620) |
| Interference List Recall (trial 6) | 5.3 (0.52) | 5.3 (0.59) | 0.01 (−1.12, 1.13) | 0.02 (0.992) | 5.6 (0.57) | 6.1 (0.59) | −0.50 (−1.52, 0.52) | −0.29 (0.334) |
| Post Interference List Recall (trial 7) | 10.5 (0.70) | 9.5 (0.77) | 1.03 (−0.43, 2.49) | 0.44 (0.168) | 10.1 (0.75) | 9.1 (0.76) | 1.05 (−0.31, 2.41) | 0.45 (0.129) |
| Delayed Recall (trial 8) | 11.5 (0.68) | 10.6 (0.75) | 0.91 (−0.49, 2.30) | 0.41 (0.202) | 11.6 (0.73) | 10.6 (0.39) | 1.00 (−0.31, 2.32) | 0.45 (0.135) |
| Word Recognition (trial 9) | 13.4 (0.60) | 13.7 (0.26) | −0.34 (−1.6, 0.92) | −0.15 (0.602) | 14.0 (0.66) | 13.6 (0.66) | 0.46 (−0.74, 1.65) | 0.20 (0.451) |
| Digit Span Test (# correct) | ||||||||
| Short term auditory memory/simple attention | 5.05 (0.37) | 5.3 (0.41) | −0.21 (−0.97, 0.56) | −0.17 (0.560) | 4.7 (0.40) | 5.3 (0.40) | −0.54 (−1.26, 0.19) | −0.44 (0.147) |
| Short-term verbal memory | 4.35 (0.47) | 3.56 (0.52) | 0.79 (−0.18, 1.77) | 0.51 (0.112) | 4.47 (0.50) | 4.26 (0.51) | 0.20 (−0.72, 1.12) | 0.13 (0.666) |
| Overall score | 9.57 (0.65) | 8.63 (0.73) | 0.95 (−0.42, 2.32) | 0.32 (0.174) | 9.02 (0.71) | 9.63 (0.71) | −0.62 (−1.92, 0.68) | −0.21(0.351) |
| Color Trails (time, s) | 96.6 (19.0) | 117 (21) | −20.9 (−60.8, 19.1) | −0.32 (0.306) | 125 (20.4) | 128 (20.7) | −3.2 (−40.1, 33.7) | −0.05 (0.867) |
| Finger Tapping Test (# taps) | 38.2 (1.6) | 36.2 (1.7) | 2.1 (−1.4, 5.6) | 0.38 (0.233) | 37.7 (1.82) | 37.5 (1.79) | 0.2 (−3.1, 3.5) | 0.04 (0.903) |
| Grooved Peg Board (time, s) | ||||||||
| Grooved Pegboard NDH | 126.5 (10.7) | 125 (11.6) | 2.0 (−20.0, 24.0) | 0.06 (0.860) | 136(11.5) | 129 (11.5) | 6.6 (−14.2, 27.4) | 0.20 (0.535) |
| Grooved Pegboard DH | 97.9 (8.6) | 92.5 (9.5) | 5.5 (−12.2, 23.2) | 0.20 (0.542) | 102.9 (9.1) | 91.6 (9.2) | 11.4 (−5.0, 27.7) | 0.41 (0.172) |
| Verbal Fluency | ||||||||
| Verbal Fluency (Tot. Correct) | 13.2 (1.0) | 11.5 (1.03) | 1.68 (−0.32, 3.67) | 0.51 (0.099) | 13.5 (1.04) | 12.7 (1.05) | 0.87 (−0.99, 2.72) | 0.26 (0.358) |
| Timed Gait (time, s) | 9.5 (0.97) | 10.9 (1.06) | −1.43 (−3.5, 0.60) | −0.44 (0.167) | 9.9 (1.06) | 9.8 (1.09) | 0.12 (−1.8, 2.0) | 0.04 (0.904) |
| Symbol Digit Modality(# correct) | 23.6 (2.1) | 26.0 (2.3) | −2.4 (−6.8, 2.0) | −0.34 (0.286) | 25.5 (2.29) | 26.7 (2.31) | −1.24 (−5.4, 2.9) | −0.17 (0.556) |
| Frailty score | 2.24 (0.23) | 2.22 (0.26) | 0.02 (−0.47, 0.51) | 0.03 (0.931) | 2.29 (0.26) | 2.83 (0.26) | −0.54 (−1.00, −0.08) | −0.71 (0.023) |
| Quality of Life Score | 72.9 (3.2) | 74.8 (3.2 | −1.9 (−7.8, 4.1) | −0.20 (0.533) | 71.1 (3.2) | 73.2 (3.1) | −2.1 (−8.0, 3.9) | −0.22 (0.490) |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ezeamama, A.E.; Sikorskii, A.; Sankar, P.R.; Nakasujja, N.; Ssonko, M.; Kaminski, N.E.; Guwatudde, D.; Boivin, M.J.; Giordani, B. Computerized Cognitive Rehabilitation Training for Ugandan Seniors Living with HIV: A Validation Study. J. Clin. Med. 2020, 9, 2137. https://doi.org/10.3390/jcm9072137
Ezeamama AE, Sikorskii A, Sankar PR, Nakasujja N, Ssonko M, Kaminski NE, Guwatudde D, Boivin MJ, Giordani B. Computerized Cognitive Rehabilitation Training for Ugandan Seniors Living with HIV: A Validation Study. Journal of Clinical Medicine. 2020; 9(7):2137. https://doi.org/10.3390/jcm9072137
Chicago/Turabian StyleEzeamama, Amara E., Alla Sikorskii, Parvathy R. Sankar, Noeline Nakasujja, Michael Ssonko, Norbert E. Kaminski, David Guwatudde, Michael J. Boivin, and Bruno Giordani. 2020. "Computerized Cognitive Rehabilitation Training for Ugandan Seniors Living with HIV: A Validation Study" Journal of Clinical Medicine 9, no. 7: 2137. https://doi.org/10.3390/jcm9072137
APA StyleEzeamama, A. E., Sikorskii, A., Sankar, P. R., Nakasujja, N., Ssonko, M., Kaminski, N. E., Guwatudde, D., Boivin, M. J., & Giordani, B. (2020). Computerized Cognitive Rehabilitation Training for Ugandan Seniors Living with HIV: A Validation Study. Journal of Clinical Medicine, 9(7), 2137. https://doi.org/10.3390/jcm9072137