Bilateral Simultaneous Breast Reconstruction with DIEP- and TMG Flaps: Head to Head Comparison, Risk and Complication Analysis

 ,
,  ,
, 
Abstract
1. Introduction
2. Patients and Methods
2.1. Data Extraction
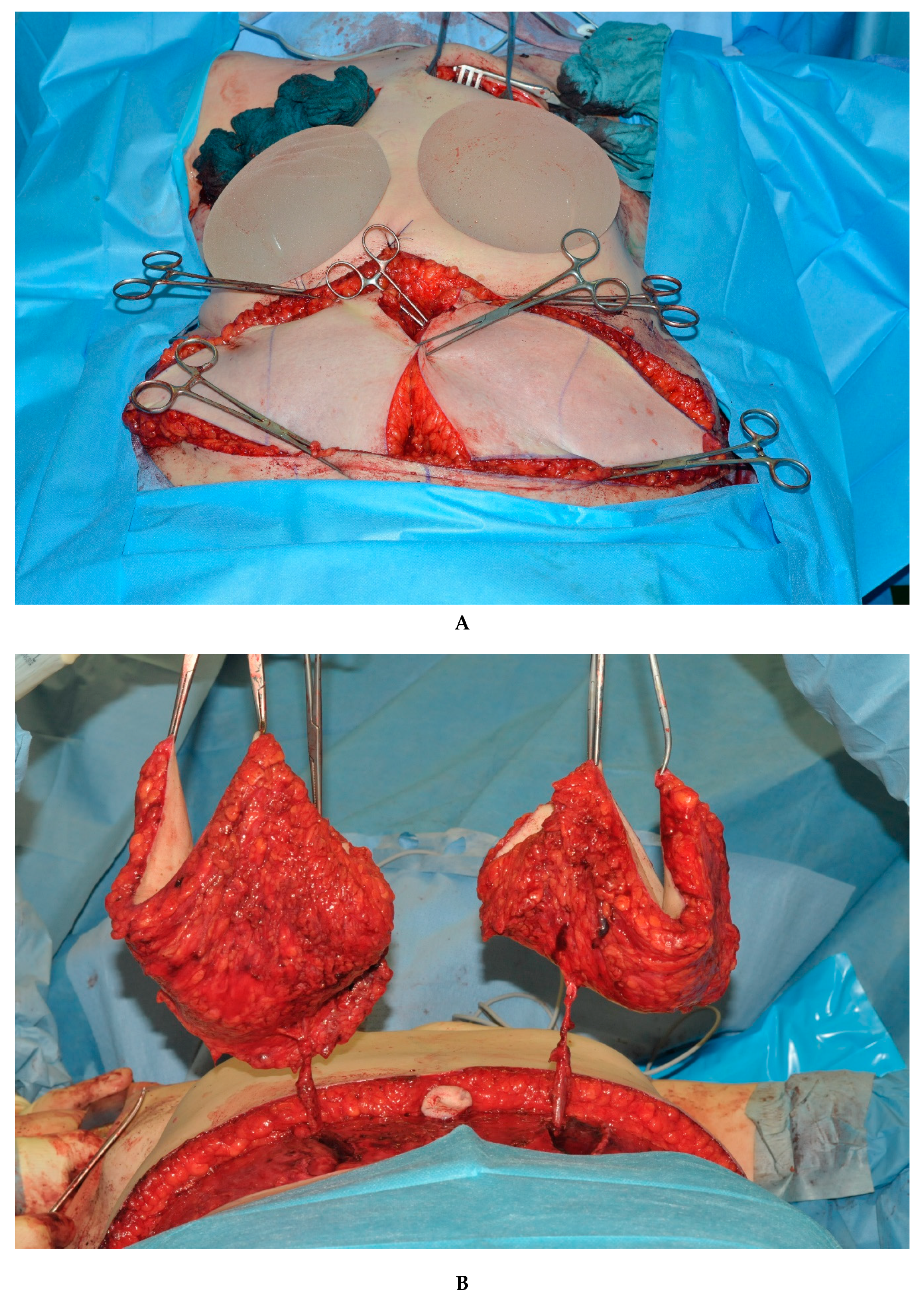
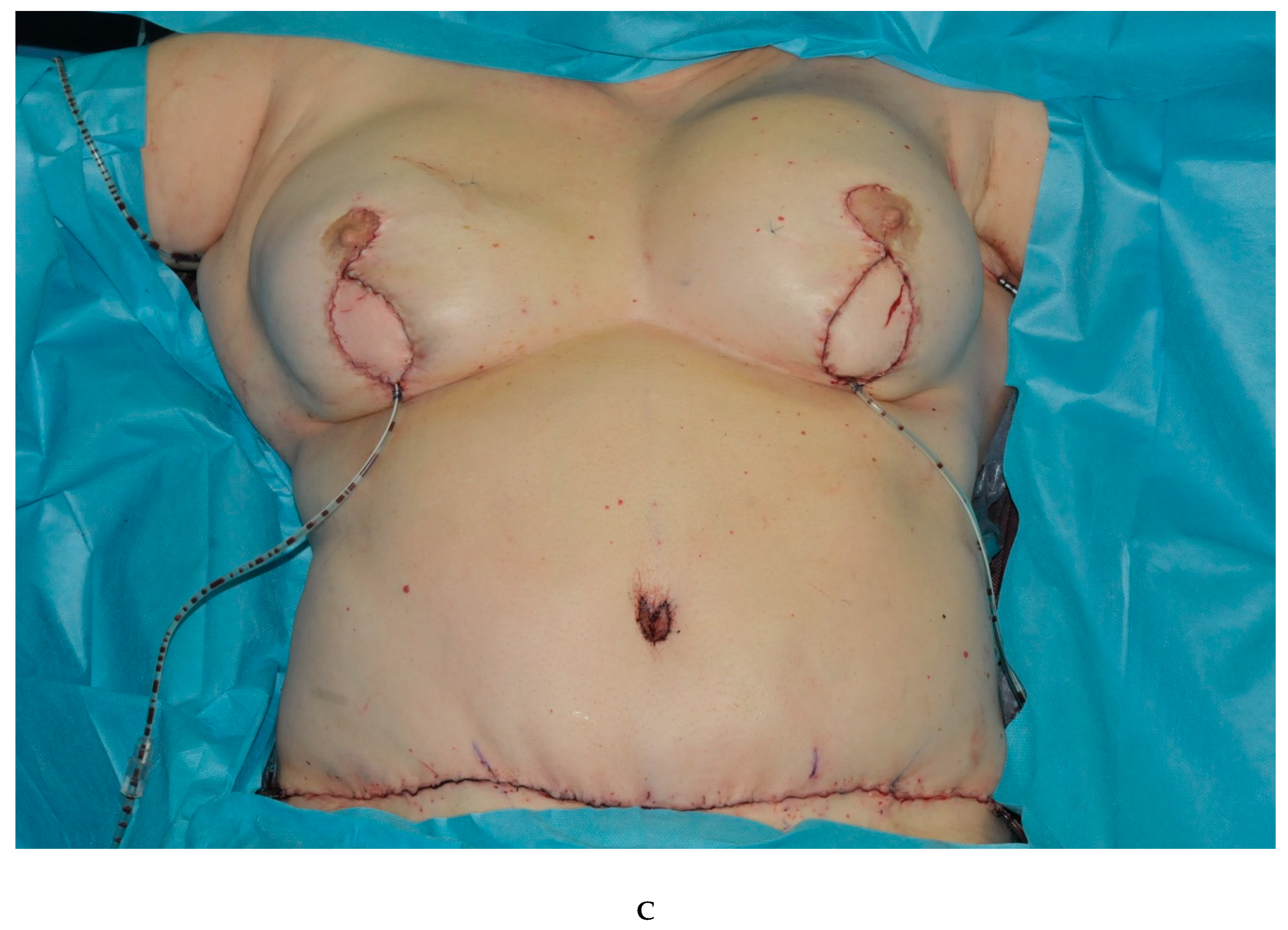
2.2. Surgical Approach
3. Statistics
4. Results
5. Discussion
6. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Hamdi, M.; Blondeel, P.; Van Landuyt, K.; Tondu, T.; Monstrey, S. Bilateral Autogenous Breast Reconstruction Using Perforator Free Flaps: A Single Center Experience. Plast. Reconstr. Surg. 2004, 114, 83–89. [Google Scholar] [CrossRef] [PubMed]
- Eisen, A.; Rebbeck, T.R.; Wood, W.C.; Weber, B.L. Prophylactic surgery in women with a hereditary to breast and ovarian cancer. J. Clin. Oncol. 2000, 18, 1980–1995. [Google Scholar] [CrossRef] [PubMed]
- Solomon, J.S.; Brunicardi, C.F.; Friedman, J.D. Evaluation and treatment of BRCA-positive patients. Plast. Reconstr. Surg. 2000, 105, 714–719. [Google Scholar] [CrossRef] [PubMed]
- Healy, C.; Allen, R.J. The evolution of perforator flap breast reconstruction: Twenty years after the first DIEP flap. J. Reconstr. Microsurg. 2014, 30, 121–126. [Google Scholar] [CrossRef]
- Baldwin, B.J.; Schusterman, M.A.; Miller, M.J.; Kroll, S.S.; Wang, B.G. Bilateral Breast Reconstruction—Conventional Versus Free Tram. Plast. Reconstr. Surg. 1994, 93, 1410–1416. [Google Scholar] [CrossRef]
- Bodin, F.; Schohn, T.; Dissaux, C.; Baratte, A.; Fiquet, C.; Bruant-Rodier, C. Bilateral simultaneous breast reconstruction with transverse musculocutaneous gracilis flaps. J. Plast. Reconstr. Aesthetic Surg. 2015, 68, e1–e6. [Google Scholar] [CrossRef] [PubMed]
- Weichman, K.E.; Tanna, N.; Broer, P.N.; Wilson, S.; Azhar, H.; Karp, N.S.; Choi, M.; Ahn, C.Y.; Levine, J.P.; Allen Sr, R.J. Microsurgical breast reconstruction in thin patients: The impact of low body mass indices. J. Reconstr. Microsurg. 2015, 31, 20–25. [Google Scholar] [CrossRef]
- Wechselberger, G.; Schoeller, T. The transverse myocutaneous gracilis free flap: A valuable tissue source breast reconstruction. Plast. Reconstr. Surg. 2004, 114, 69–73. [Google Scholar] [CrossRef]
- Pülzl, P.; Schoeller, T.; Kleewein, K.; Wechselberger, G. Donor-site morbidity of the transverse musculocutaneous gracilis flap in autologous breast reconstruction: Short-term and long-term results. Plast. Reconstr. Surg. 2011, 128, 233e–242e. [Google Scholar] [CrossRef]
- Alderman, A.K.; Wilkins, E.G.; Lowery, J.C.; Kim, M.; Davis, J.A. Determinants of patient satisfaction in postmastectomy breast reconstruction. Plast. Reconstr. Surg. 2000, 106, 769–776. [Google Scholar] [CrossRef]
- Hamdi, M.; Weiler-Mithoff, E.M.; Webster, M.H. Deep inferior epigastric perforator flap in breast reconstruction: Experience with the first 50 flaps. Plast. Reconstr. Surg. 1999, 103, 86–95. [Google Scholar] [CrossRef]
- Wade, R.G.; Razzano, S.; Sassoon, E.M.; Haywood, R.M.; Ali, R.S.; Figus, A. Complications in DIEP Flap Breast Reconstruction After Mastectomy for Breast Cancer: A Prospective Cohort Study Comparing Unilateral Versus Bilateral Reconstructions. Ann. Surg. Oncol. 2017, 24, 1465–1474. [Google Scholar] [CrossRef]
- Offodile, A.C., II; Aherrera, A.; Wenger, J.; Rajab, T.K.; Guo, L. Impact of increasing operative time on the incidence of early failure and complications following free tissue transfer? A risk factor analysis of 2,008 patients from the ACS-NSQIP database. Microsurgery 2017, 37, 12–20. [Google Scholar] [CrossRef] [PubMed]
- Craft, R.O.; Colakoglu, S.; Curtis, M.S.; Yueh, J.H.; Lee, B.S.; Tobias, A.M.; Lee, B.T. Patient satisfaction in unilateral and bilateral breast reconstruction [outcomes article]. Plast. Reconstr. Surg. 2011, 127, 1417–1424. [Google Scholar] [CrossRef]
- Schaverien, M.V.; Butler, C.E. Complications in DIEP Flap Breast Reconstruction after Mastectomy for Breast Cancer: A Prospective Cohort Study Comparing Unilateral and Bilateral Reconstructions. Ann. Surg. Oncol. 2017, 24, 1451–1453. [Google Scholar] [CrossRef]
- Tomouk, T.; Mohan, A.T.; Azizi, A.; Conci, E.; Brickley, E.B.; Malata, C.M. Donor site morbidity in DIEP free flap breast reconstructions: A comparison of unilateral, bilateral, and bipedicled surgical procedure types. J. Plast. Reconstr. Aesthet. Surg. 2017, 70, 1505–1513. [Google Scholar] [CrossRef] [PubMed]
- Werdin, F.; Peek, A.; Martin, N.C.; Baumeister, S. Superior gluteal artery perforator flap in bilateral breast reconstruction. Ann. Plast. Surg. 2010, 64, 17–21. [Google Scholar] [CrossRef] [PubMed]
- De Frene, B.; Van Landuyt, K.O.E.N.R.A.A.D.; Hamdi, M.O.U.S.T.A.P.H.A.; Blondeel, P.; Roche, N.; Voet, D.; Monstrey, S. Free DIEAP and SGAP flap breast reconstruction after abdominal/gluteal liposuction. J. Plast. Reconstr. Aesthetic Surg. 2006, 59, 1031–1036. [Google Scholar] [CrossRef] [PubMed]
- Schoeller, T.; Huemer, G.M.; Wechselberger, G. The transverse musculocutaneous gracilis flap for breast reconstruction: Guidelines for flap and patient selection. Plast. Reconstr. Surg. 2008, 122, 29–38. [Google Scholar] [CrossRef]
- Fansa, H.; Schirmer, S.; Warnecke, I.C.; Cervelli, A.; Frerichs, O. The transverse myocutaneous gracilis muscle flap: A fast and reliable method for breast reconstruction. Plast. Reconstr. Surg. 2008, 122, 1326–1333. [Google Scholar] [CrossRef]
- Buntic, R.F.; Horton, K.M.; Brooks, D.; Althubaiti, G.A. Transverse Upper Gracilis Flap as an Alternative to Abdominal Tissue Breast Reconstruction. Plast. Reconstr. Surg. 2011, 128, 607e–613e. [Google Scholar] [CrossRef] [PubMed]
- Vega, S.J.; Sandeen, S.N.; Bossert, R.P.; Perrone, A.; Ortiz, L.; Herrera, H. Gracilis myocutaneous free flap in autologous breast reconstruction. Plast. Reconstr. Surg. 2009, 124, 1400–1409. [Google Scholar] [CrossRef]
- Fattah, A.; Figus, A.; Mathur, B.; Ramakrishnan, V.V. The transverse myocutaneous gracilis flap: Technical refinements. J. Plast. Reconstr. Aesthetic Surg. 2010, 63, 305–313. [Google Scholar] [CrossRef] [PubMed]
- Gill, P.S.; Hunt, J.P.; Guerra, A.B.; Dellacroce, F.J.; Sullivan, S.K.; Boraski, J.; Metzinger, S.E.; Dupin, C.L.; Allen, R.J. A 10-Year Retrospective Review of 758 DIEP Flaps for Breast Reconstruction. Plast. Reconstr. Surg. 2004, 113, 1153–1160. [Google Scholar] [CrossRef] [PubMed]
- Rao, S.S.; Parikh, P.M.; Goldstein, J.A.; Nahabedian, M.Y. Unilateral failures in bilateral microvascular breast reconstruction. Plast. Reconstr. Surg. 2010, 126, 17–25. [Google Scholar] [CrossRef] [PubMed]
- Chang, E.I.; Chang, E.I.; Soto-Miranda, M.A.; Zhang, H.; Nosrati, N.; Crosby, M.A.; Reece, G.P.; Robb, G.L.; Chang, D.W. Comprehensive Evaluation of Risk Factors and Management of Impending Flap Loss in 2138 Breast Free Flaps. Ann. Plast. Surg. 2016, 77, 67–71. [Google Scholar] [CrossRef] [PubMed]
- Park, J.E.; Alkureishi, L.W.; Song, D.H. TUGs into VUGs and Friendly BUGs: Transforming the Gracilis Territory into the Best Secondary Breast Reconstructive Option. Plast. Reconstr. Surg. 2015, 136, 447–454. [Google Scholar] [CrossRef] [PubMed]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Table 1 | Total | Double DIEP | Double TMG |
|---|---|---|---|
| n = 119 | n = 76 | n = 43 | |
| Age-years | |||
| mean | 53 | 54.0 | 52.4 |
| standard deviation | 10 | 9.3 | 11.2 |
| BMI kg/m² | |||
| mean | 26.4 | 28.8 | 22.2 |
| standard deviation | 5.5 | 5.0 | 3.6 |
| Table 2 | Total | Double DIEP | Double TMG |
|---|---|---|---|
| Cut to suture time | |||
| mean | 473.5 | 476.4 | 468.5 |
| standard deviation | 106.7 | 103.4 | 113.2 |
| p = 0.698 |
| Table 3 | Total | Double DIEP | Double TMG | p-Value |
|---|---|---|---|---|
| vascular insufficiency | 15/238 (6.3 %) | 6/152 (3.9 %) | 9/86 (10.5 %) | 0.0468 |
| Relative Risk double TMG vs. double DIEP: | 2.65 | |||
| partial flap necrosis | 13/238 (5.5 %) | 6/152 (3.9 %) | 7/86 (8.1 %) | 0.1716 |
| Relative Risk double TMG vs. double DIEP: | 2.06 | |||
| flap loss | 7/238 (2.9 %) | 4/152 (2.6 %) | 3/86 (3.5 %) | 0.7071 |
| Relative Risk double TMG vs. double DIEP: | 1.33 | |||
| late fat necrosis | 6/238 (2.5 %) | 6/152 (3.9 %) | 0/86 (0.0 %) | 0.0898 |
| Relative Risk double TMG vs. double DIEP: | 0.00 | |||
| donor site complication | 25/119 (21.0 %) | 18/76 (23.7 %) | 7/43 (16.3 %) | 0.9075 |
| Relative Risk double DIEP vs. double TMG: | 1.45 | |||
| erythrocyte concentrate substitution | 21/119 (17.6 %) | 7/76 (9.2 %) | 14/43 (32.6 %) | 0.0013 |
| Relative Risk double TMG vs. double DIEP: | 3.53 |
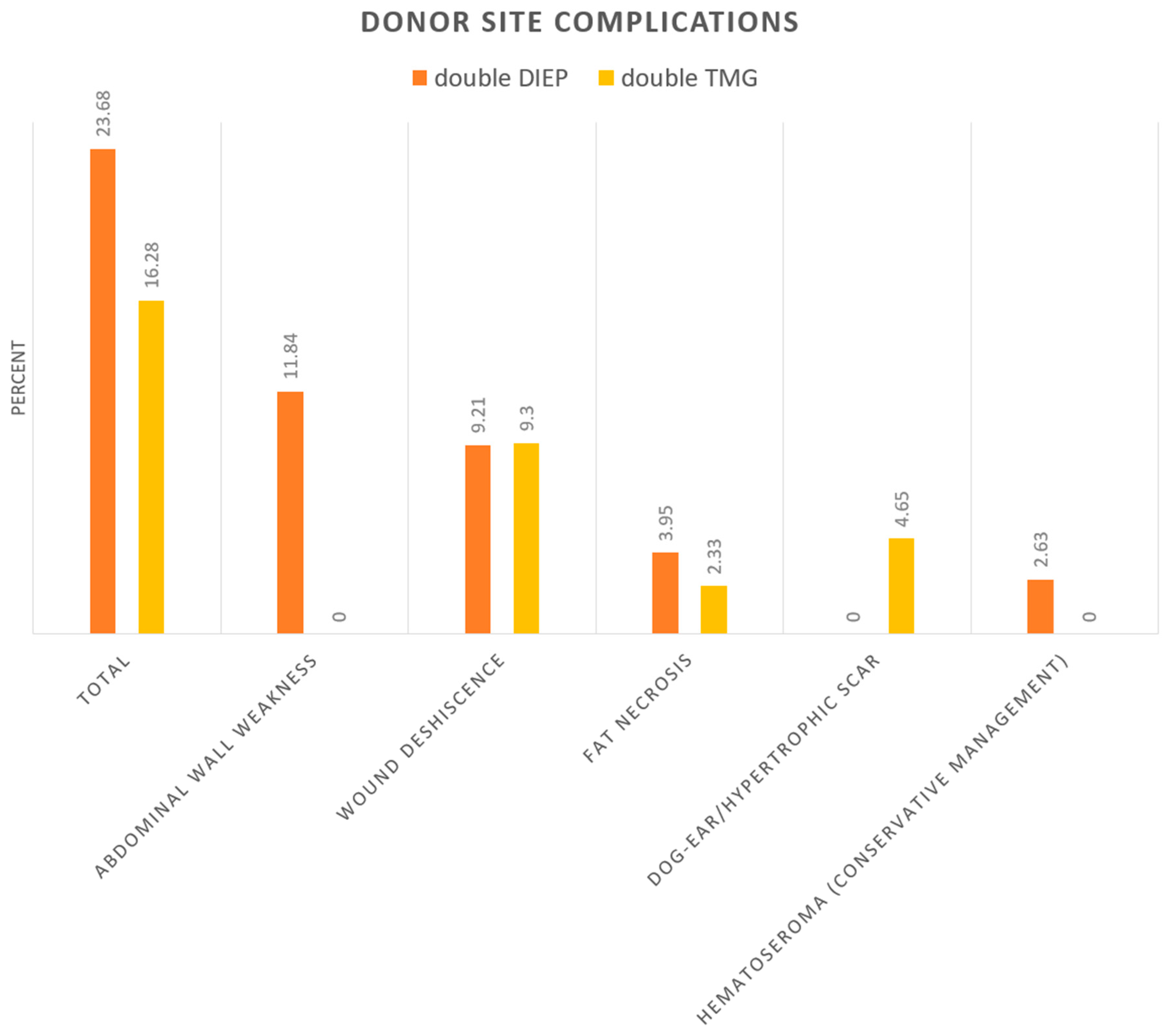
| Table 4 | Double DIEP (%) | Double TMG (%) |
|---|---|---|
| Total | 23.68 | 16.28 |
| abdominal wall weakness/Hernias | 11.84 | 0 |
| wound deshiscence | 9.21 | 9.3 |
| fat necrosis | 3.95 | 2.33 |
| dog-ear/hypertrophic scar | 0 | 4.65 |
| Hematoseroma (conservative management) | 2.63 | 0 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Weitgasser, L.; Schwaiger, K.; Medved, F.; Hamler, F.; Wechselberger, G.; Schoeller, T. Bilateral Simultaneous Breast Reconstruction with DIEP- and TMG Flaps: Head to Head Comparison, Risk and Complication Analysis. J. Clin. Med. 2020, 9, 2031. https://doi.org/10.3390/jcm9072031
Weitgasser L, Schwaiger K, Medved F, Hamler F, Wechselberger G, Schoeller T. Bilateral Simultaneous Breast Reconstruction with DIEP- and TMG Flaps: Head to Head Comparison, Risk and Complication Analysis. Journal of Clinical Medicine. 2020; 9(7):2031. https://doi.org/10.3390/jcm9072031
Chicago/Turabian StyleWeitgasser, Laurenz, Karl Schwaiger, Fabian Medved, Felix Hamler, Gottfried Wechselberger, and Thomas Schoeller. 2020. "Bilateral Simultaneous Breast Reconstruction with DIEP- and TMG Flaps: Head to Head Comparison, Risk and Complication Analysis" Journal of Clinical Medicine 9, no. 7: 2031. https://doi.org/10.3390/jcm9072031
APA StyleWeitgasser, L., Schwaiger, K., Medved, F., Hamler, F., Wechselberger, G., & Schoeller, T. (2020). Bilateral Simultaneous Breast Reconstruction with DIEP- and TMG Flaps: Head to Head Comparison, Risk and Complication Analysis. Journal of Clinical Medicine, 9(7), 2031. https://doi.org/10.3390/jcm9072031