Chronic Gastritis Is Associated with a Decreased High-Density Lipid Level: Histological Features of Gastritis Based on the Updated Sydney System

 , , ,
, , ,  , , , , and
, , , , and
Abstract
1. Introduction
2. Materials and Methods
2.1. Patient Selection
2.2. Data Collection
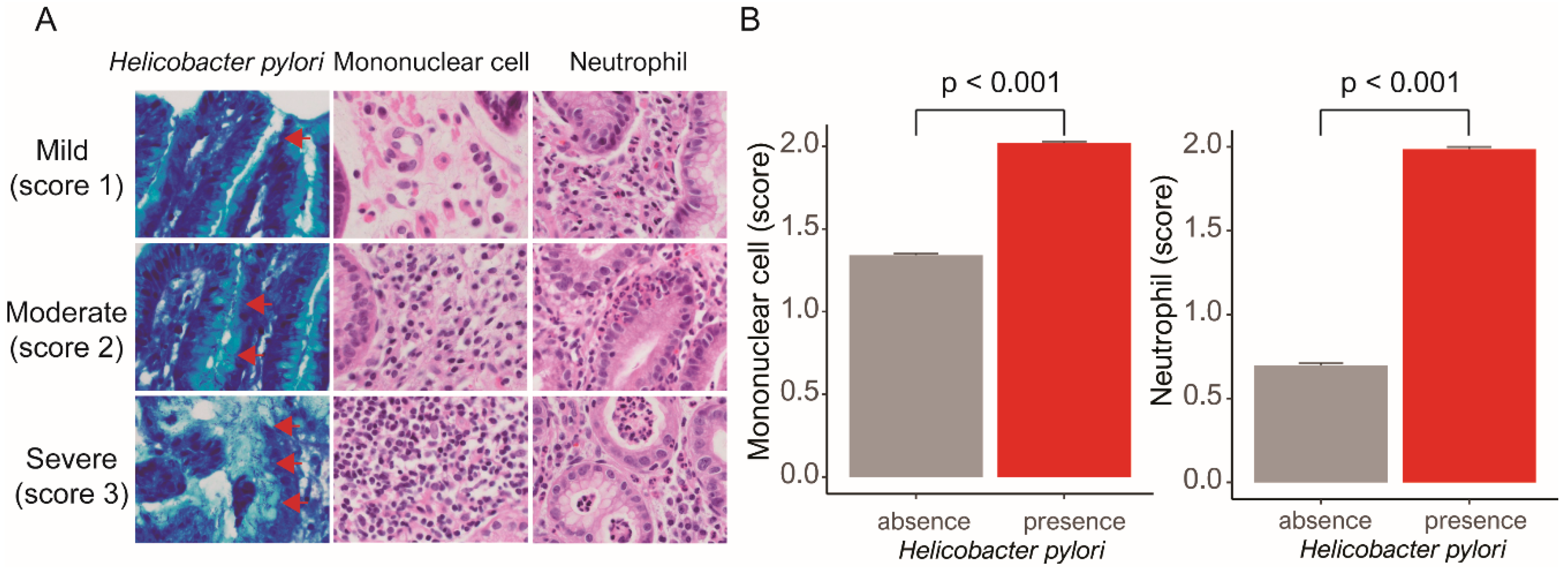
2.3. Microscopic Examination for Updated Sydney System Scoring
2.4. Statistical Analysis
3. Results
3.1. Clinical and Laboratory Parameters According to Helicobacter Pylori, Mononuclear Cells, and Neutrophils
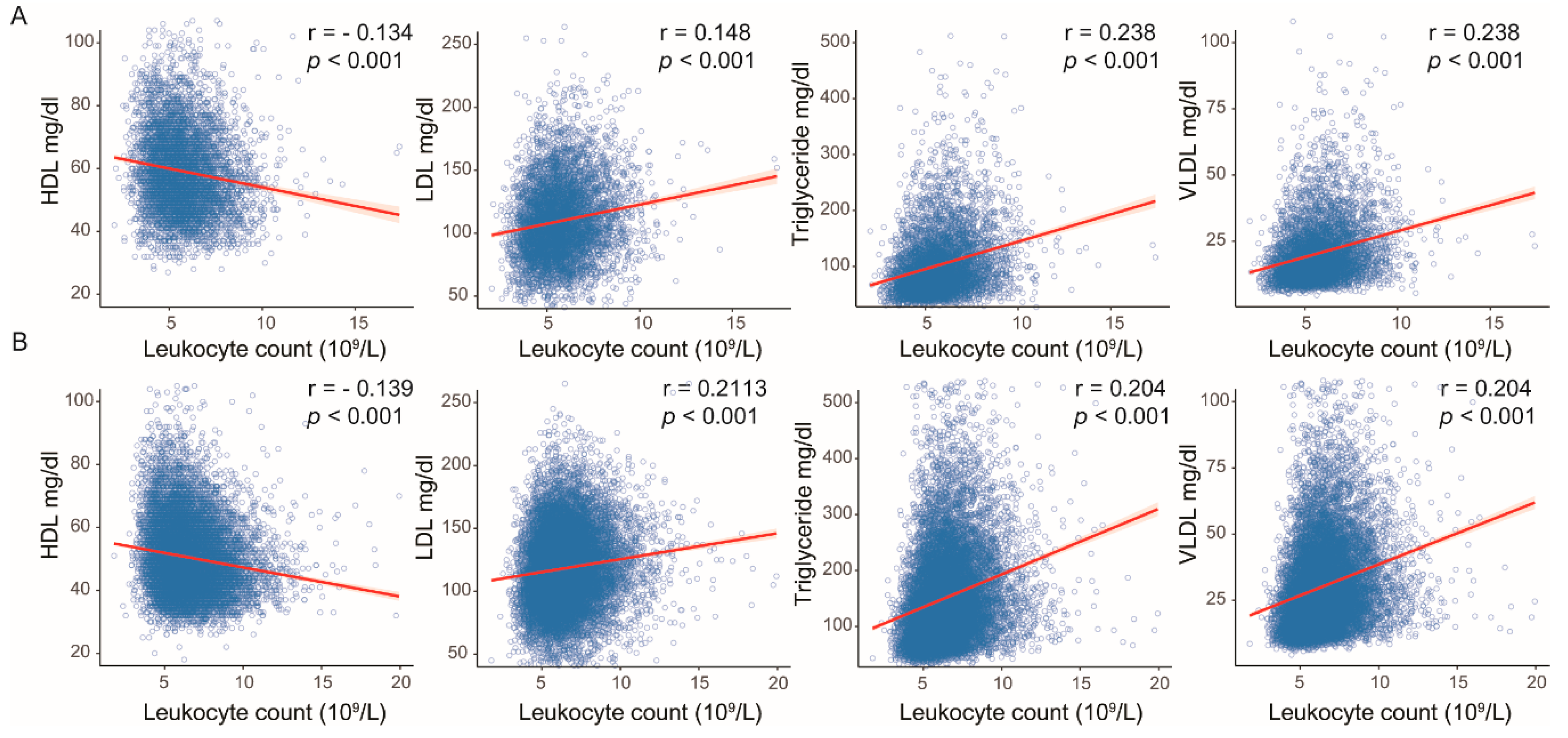
3.2. Associations among Helicobacter Pylori, Mononuclear Cells, Neutrophils, Serum Leukocyte Count and Lipid Profiles
4. Discussion
Author Contributions
Ethics Approval
Conflicts of Interest
Abbreviations
| KBSMC | Kangbuk Samsung Medical Center |
| HP | Helicobacter pylori |
| CVD | Cardiovascular disease |
| LDL | Low-density lipoprotein |
| VLDL | Very-low-density lipoprotein |
| TG | Triglyceride |
| HDL | High-density lipoprotein |
| USS | Updated Sydney system |
| SBP | Systolic blood pressure |
| DBP | Diastolic blood pressure |
| BMI | Body mass index |
References
- Takahashi, S.; Sakai, J.; Fujino, T.; Hattori, H.; Zenimaru, Y.; Suzuki, J.; Miyamori, I.; Yamamoto, T.T. The very low-density lipoprotein (VLDL) receptor: Characterization and functions as a peripheral lipoprotein receptor. J. Atheroscler. Thromb. 2004, 11, 200–208. [Google Scholar] [CrossRef] [PubMed]
- Chan, D.C.; Barrett, P.H.R.; Watts, G.F. The metabolic and pharmacologic bases for treating atherogenic dyslipidaemia. Best Pract Res. Clin. Endocrinol. Metab. 2014, 28, 369–385. [Google Scholar] [CrossRef] [PubMed]
- Zhou, X.; He, L.; Wan, D.; Yang, H.; Yao, K.; Wu, G.; Wu, X.; Yin, Y. Methionine restriction on lipid metabolism and its possible mechanisms. Amino Acids 2016, 48, 1533–1540. [Google Scholar] [CrossRef] [PubMed]
- Zhou, H.; Liu, R. ER stress and hepatic lipid metabolism. Front. Genet. 2014, 5, 112. [Google Scholar] [CrossRef] [PubMed]
- Steinberg, D. Atherogenesis in perspective: Hypercholesterolemia and inflammation as partners in crime. Nat. Med. 2002, 8, 1211–1217. [Google Scholar] [CrossRef] [PubMed]
- Cullen, T.W.; Giles, D.K.; Wolf, L.N.; Ecobichon, C.; Boneca, I.G.; Trent, M.S. Helicobacter pylori versus the host: Remodeling of the bacterial outer membrane is required for survival in the gastric mucosa. PLoS Pathog. 2011, 7, e1002454. [Google Scholar] [CrossRef]
- Figura, N. Helicobacter pylori factors involved in the development of gastroduodenal mucosal damage and ulceration. J. Clin. Gastroenterol. 1997, 25 (Suppl. S1), S149–S163. [Google Scholar] [CrossRef]
- Pece, S.; Giuliani, G.; Di Leo, A.; Fumarola, D.; Antonaci, S.; Jirillo, E. Role of lipopolysaccharide and related cytokines in Helicobacter pylori infection. Recenti Prog. Med. 1997, 88, 237–241. [Google Scholar]
- Gilroy, D.W.; Bishop-Bailey, D. Lipid Mediators in Immune Regulation and Resolution. Br. J. Pharmacol. 2019, 176, 1009–1023. [Google Scholar] [CrossRef]
- Chimienti, G.; Russo, F.; Lamanuzzi, B.L.; Nardulli, M.; Messa, C.; Di Leo, A.; Correale, M.; Giannuzzi, V.; Pepe, G. Helicobacter pylori is associated with modified lipid profile: Impact on Lipoprotein(a). Clin. Biochem. 2003, 36, 359–365. [Google Scholar] [CrossRef]
- Rasmi, Y.; Zeynalzadeh, J.; Shirpoor, A.; Seyedmohammadzad, M.; Hajhosseini, R. Lipid Profile in Cardiac Syndrome X: Association with Helicobacter pylori. J. Clin. Diagn. Res. 2016, 10, BC07–BC09. [Google Scholar] [CrossRef]
- Dixon, M.F.; Genta, R.M.; Yardley, J.H.; Correa, P. Classification and grading of gastritis. The updated Sydney System. International Workshop on the Histopathology of Gastritis, Houston 1994. Am. J. Surg. Pathol. 1996, 20, 1161–1181. [Google Scholar] [CrossRef] [PubMed]
- Chen, T.-P.; Hung, H.-F.; Chen, M.-K.; Lai, H.-H.; Hsu, W.-F.; Huang, K.-C.; Yang, K.-C. Helicobacter pylori Infection is Positively Associated with Metabolic Syndrome in Taiwanese Adults: A Cross-Sectional Study. Helicobacter 2015, 20, 184–191. [Google Scholar] [CrossRef] [PubMed]
- Gunji, T.; Matsuhashi, N.; Sato, H.; Fujibayashi, K.; Okumura, M.; Sasabe, N.; Urabe, A. Helicobacter pylori infection is significantly associated with metabolic syndrome in the Japanese population. Am. J. Gastroenterol. 2008, 103, 3005–3010. [Google Scholar] [CrossRef]
- Ribaldone, D.G.; Fagoonee, S.; Hickman, I.; Altruda, F.; Saracco, G.M.; Pellicano, R. Helicobacter pylori infection and ischemic heart disease: Could experimental data lead to clinical studies? Minerva Cardioangiol. 2016, 64, 686–696. [Google Scholar]
- Shi, Y.; Duan, J.-Y.; Liu, D.-W.; Qiao, Y.-J.; Han, Q.-X.; Pan, S.-K.; Tang, L.; Cai, G.-Y.; Chen, X.-M.; Liu, Z.-S.; et al. Helicobacter pylori Infection is Associated with Occurrence of Proteinuria in Type 2 Diabetes Patients: A Systemic Review and Meta-Analysis. Chin. Med. J. 2018, 131, 2734–2740. [Google Scholar] [CrossRef] [PubMed]
- Hosseinzadeh, M.; Khosravi, A.; Saki, K.; Ranjbar, R. Evaluation of Helicobacter pylori infection in patients with common migraine headache. Arch. Med. Sci. 2011, 7, 844–849. [Google Scholar] [CrossRef] [PubMed]
- Shindler-Itskovitch, T.; Chodick, G.; Shalev, V.; Muhsen, K. Helicobacter pylori infection and prevalence of stroke. Helicobacter 2019, 24, e12553. [Google Scholar] [CrossRef]
- Ponzetto, A.; Holton, J. Extragastric diseases correlated with Helicobacter pylori. Helicobacter 2019, 24, e12549. [Google Scholar] [CrossRef]
- Franceschi, F.; Leo, D.; Fini, L.; Santoliquido, A.; Flore, R.; Tondi, P.; Roccarina, D.; Nista, E.C.; Cazzato, A.I.; Lupascu, A.; et al. Helicobacter pylori infection and ischaemic heart disease: An overview of the general literature. Dig. Liver Dis. 2005, 37, 301–308. [Google Scholar] [CrossRef]
- Yamaoka, Y.; Graham, D.Y. CagA status and gastric cancer unreliable serological tests produce unreliable data. Gastroenterology 1999, 117, 745. [Google Scholar] [CrossRef]
- Levitzky, Y.S.; Guo, C.-Y.; Rong, J.; Larson, M.G.; Walter, R.E.; Keaney, J.F.; Sutherland, P.A.; Vasan, A.; Lipinska, I.; Evans, J.C.; et al. Relation of smoking status to a panel of inflammatory markers: The framingham offspring. Atherosclerosis 2008, 201, 217–224. [Google Scholar] [CrossRef] [PubMed]
- Danesh, J.; Collins, R.; Appleby, P.; Peto, R. Association of fibrinogen, C-reactive protein, albumin, or leukocyte count with coronary heart disease: Meta-analyses of prospective studies. JAMA 1998, 279, 1477–1482. [Google Scholar] [CrossRef] [PubMed]
- Tsang, K.W.; Lam, S.K. Helicobacter pylori and extra-digestive diseases. J. Gastroenterol. Hepatol. 1999, 14, 844–850. [Google Scholar] [CrossRef]
- Manolakis, A.; Kapsoritakis, A.N.; Potamianos, S.P. A review of the postulated mechanisms concerning the association of Helicobacter pylori with ischemic heart disease. Helicobacter 2007, 12, 287–297. [Google Scholar] [CrossRef]
- Fagoonee, S.; De Angelis, C.; Elia, C.; Silvano, S.; Oliaro, E.; Rizzetto, M.; Pellicano, R. Potential link between Helicobacter pylori and ischemic heart disease: Does the bacterium elicit thrombosis? Minerva Med. 2010, 101, 121–125. [Google Scholar]
- Kountouras, J.; Gavalas, E.; Zavos, C.; Stergiopoulos, C.; Chatzopoulos, D.; Kapetanakis, N.; Gisakis, D. Alzheimer’s disease and Helicobacter pylori infection: Defective immune regulation and apoptosis as proposed common links. Med. Hypotheses 2007, 68, 378–388. [Google Scholar] [CrossRef]
- Ross, R. Atherosclerosis--an inflammatory disease. N. Engl. J. Med. 1999, 340, 115–126. [Google Scholar] [CrossRef]
- Hansson, G.K. Inflammation, atherosclerosis, and coronary artery disease. N. Engl. J. Med. 2005, 352, 1685–1695. [Google Scholar] [CrossRef]
- Shah, P.K. Chronic infections and atherosclerosis/thrombosis. Curr. Atheroscler. Rep. 2002, 4, 113–119. [Google Scholar] [CrossRef]
- Low, J.E.; Metz, A.L.; Mertz, T.E.; Henry, S.P.; Knowlton, P.; Loewen, G.; Sommers, C.S.; Robertson, D.G.; Olszewski, B.J.; Schroeder, R.L. Cardiac hypertrophy in rats after intravenous administration of CI-959, a novel antiinflammatory compound: Morphologic features and pharmacokinetic and pharmacodynamic mechanisms. J. Cardiovasc. Pharmacol. 1995, 25, 930–939. [Google Scholar] [CrossRef] [PubMed]
- Takeshita, S.; Isshiki, T.; Ochiai, M.; Ishikawa, T.; Nishiyama, Y.; Fusano, T.; Toyoizumi, H.; Kondo, K.; Ono, Y.; Sato, T. Systemic inflammatory responses in acute coronary syndrome: Increased activity observed in polymorphonuclear leukocytes but not T lymphocytes. Atherosclerosis 1997, 135, 187–192. [Google Scholar] [CrossRef]
- Niebauer, J.; Maxwell, A.J.; Lin, P.S.; Wang, D.; Tsao, P.S.; Cooke, J.P. NOS inhibition accelerates atherogenesis: Reversal by exercise. Am. J. Physiol. Heart Circ. Physiol. 2003, 285, H535–H540. [Google Scholar] [CrossRef] [PubMed]
- Yang, Z.; Wang, J.M.; Chen, L.; Luo, C.F.; Tang, A.L.; Tao, J. Acute exercise-induced nitric oxide production contributes to upregulation of circulating endothelial progenitor cells in healthy subjects. J. Hum. Hypertens 2007, 21, 452–460. [Google Scholar] [CrossRef]
- Huang, Z.; Wu, X.; Stamler, J.; Rao, X.; Tao, S.; Friedewald, W.T.; Liao, Y.; Tsai, R.; Stamler, R.; He, H. A north-south comparison of blood pressure and factors related to blood pressure in the People’s Republic of China: A report from the PRC-USA Collaborative Study of Cardiovascular Epidemiology. J. Hypertens. 1994, 12, 1103–1112. [Google Scholar] [CrossRef]
- Pisinger, C.; Jorgensen, T. Waist circumference and weight following smoking cessation in a general population: The Inter99 study. Prev. Med. 2007, 44, 290–295. [Google Scholar] [CrossRef]
- Berlin, I. Smoking-induced metabolic disorders: A review. Diabetes Metab. 2008, 34, 307–314. [Google Scholar] [CrossRef]
- Clair, C.; Rigotti, N.A.; Porneala, B.; Fox, C.S.; D’Agostino, R.B.; Pencina, M.J.; Meigs, J.B. Association of smoking cessation and weight change with cardiovascular disease among adults with and without diabetes. JAMA 2013, 309, 1014–1021. [Google Scholar] [CrossRef]
- Fonseca, V.; McDuffie, R.; Calles, J.; Cohen, R.M.; Feeney, P.; Feinglos, M.; Gerstein, H.C.; Ismail-Beigi, F.; Morgan, T.M.; Pop-Busui, R.; et al. ACCORD Study Group Determinants of weight gain in the action to control cardiovascular risk in diabetes trial. Diabetes Care 2013, 36, 2162–2168. [Google Scholar] [CrossRef][Green Version]
- Puddey, I.B.; Beilin, L.J. Alcohol is bad for blood pressure. Clin. Exp. Pharmacol. Physiol. 2006, 33, 847–852. [Google Scholar] [CrossRef]
- Stewart, S.H.; Latham, P.K.; Miller, P.M.; Randall, P.; Anton, R.F. Blood pressure reduction during treatment for alcohol dependence: Results from the Combining Medications and Behavioral Interventions for Alcoholism (COMBINE) study. Addiction 2008, 103, 1622–1628. [Google Scholar] [CrossRef] [PubMed]
- Rehm, J.; Gmel, G.E.; Gmel, G.; Hasan, O.S.M.; Imtiaz, S.; Popova, S.; Probst, C.; Roerecke, M.; Room, R.; Samokhvalov, A.V.; et al. The relationship between different dimensions of alcohol use and the burden of disease-an update. Addiction 2017, 112, 968–1001. [Google Scholar] [CrossRef] [PubMed]
- Parl, F.F.; Lev, R.; Thomas, E.; Pitchumoni, C.S. Histologic and morphometric study of chronic gastritis in alcoholic patients. Hum. Pathol. 1979, 10, 45–56. [Google Scholar] [CrossRef]
- Becker, H.C. Influence of stress associated with chronic alcohol exposure on drinking. Neuropharmacology 2017, 122, 115–126. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Absence of Helicobacter pylori (N = 10,361) | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Parameters | Male (n = 15,322) | Female (n = 5929) | ||||||||||
| Mononuclear cell | Neutrophil | Mononuclear cell | Neutrophil | |||||||||
| Absence/ Mild (n = 4511) | Moderate/ Severe (n = 2671) | p | Absence (n = 3459) | Presence (n = 3723) | p | Absence/ Mild (n = 2087) | Moderate/ Severe (n = 1092) | p | Absence (n = 1610) | Presence (n = 1569) | p | |
| Clinical | ||||||||||||
| Age, years | 44.4 ± 9.8 | 44.7 ± 9.9 | 0.23 * | 44.2 ± 9.6 | 44.7 ± 10 | 0.041 * | 44.5 ± 10.5 | 46.8 ± 11.2 | <0.001 * | 44.5 ± 10.6 | 46.1 ± 11 | <0.001 * |
| Body mass index (kg/m2) | 24.6 ± 2.8 | 24.7 ± 2.8 | 0.009 * | 24.6 ± 2.8 | 24.7 ± 2.8 | 0.076 * | 22.8 ± 3 | 23.1 ± 3.3 | 0.007 * | 22.8 ± 3.1 | 23.1 ± 3.2 | 0.002 * |
| ‡ Regular exercise, % | 1259 (27.9) | 791 (29.6) | 0.129 † | 954 (27.6) | 1096 (29.4) | 0.086 † | 552 (26.4) | 297 (27.2) | 0.681 † | 422 (26.2) | 427 (27.2) | 0.549 † |
| Cigarette smoking, % | 3428 (76) | 2048 (76.7) | 0.529 † | 2621 (75.8) | 2855 (76.7) | 0.379 † | 256 (12.3) | 151 (13.8) | 0.232 † | 184 (11.4) | 223 (14.2) | 0.022 † |
| § Alcohol consumption, % | 3694 (81.9) | 2236 (83.7) | 0.05† | 2840 (82.1) | 3090 (83.0) | 0.334 † | 703 (33.7) | 379 (34.7) | 0.59 † | 563 (35) | 519 (33.1) | 0.277 † |
| Hypertension, % | 1111 (24.6) | 678 (25.4) | 0.492 † | 864 (25) | 925 (24.8) | 0.918 † | 355 (17) | 182 (16.7) | 0.845 † | 264 (16.4) | 273 (17.4) | 0.48 † |
| Diabetes, % | 257 (5.7) | 150 (5.6) | 0.927 † | 181 (5.2) | 226 (6.1) | 0.138 † | 75 (3.6) | 39 (3.6) | 0.999 † | 59 (3.7) | 55 (3.5) | 0.884 † |
| Hepatitis, % | 681 (10.3) | 366 (9.7) | 0.351 † | 489 (9.6) | 558 (10.5) | 0.138 † | 187 (9) | 116 (10.6) | 0.146 † | 139 (8.6) | 164 (10.5) | 0.092 † |
| SBP, mmHg | 117.5 ± 12.5 | 118.2 ± 12.7 | 0.027 * | 117.8 ± 12.7 | 117.7 ± 12.5 | 0.675 * | 111.5 ± 13.6 | 112.9 ± 14.1 | 0.006 * | 111.1 ± 13.7 | 112.9 ± 13.9 | <0.001 * |
| DBP, mmHg | 76.2 ± 8.6 | 76.7 ± 8.7 | 0.013 * | 76.4 ± 8.6 | 76.3±8.7 | 0.677 * | 72.3 ± 9.4 | 73.0 ± 9.2 | 0.072 * | 72.2 ± 9.3 | 73.0 ± 9.4 | 0.018 * |
| Laboratory | ||||||||||||
| HDL, mg/dL | 50.9 ± 11.2 | 50.5 ± 11 | 0.129 * | 50.8 ± 11.3 | 50.7 ± 11.1 | 0.8 * | 59.5 ± 13.6 | 58.2 ± 12.8 | 0.008 * | 59.2 ± 13.4 | 58.8 ± 13.3 | 0.378 * |
| LDL, mg/dL | 117.8 ± 30.0 | 118.8 ± 29.6 | 0.183 * | 118.0 ± 29.6 | 118.4 ± 30.1 | 0.557 * | 108.6 ± 31.2 | 111.5 ± 30.6 | 0.012 * | 109.8 ± 31.1 | 109.4 ± 30.9 | 0.768 * |
| Triglycerides, mg/dL | 148.9 ± 0.9 | 152.9 ± 93.5 | 0.073 * | 148.8 ± 89.2 | 151.8 ± 94.3 | 0.176 * | 101.9 ± 61.5 | 104.9 ± 61.5 | 0.2 * | 102.4 ± 60.2 | 103.5 ± 62.8 | 0.606 * |
| VLDL, mg/dL | 29.8 ± 18.2 | 30.6 ± 18.7 | 0.073 * | 29.8 ± 17.8 | 30.4 ± 18.9 | 0.176 * | 20.4 ± 12.3 | 21.0 ± 12.3 | 0.2 * | 20.5 ± 12.0 | 20.7 ± 12.6 | 0.606 * |
| Leukocyte count (109/L) | 6.4 ± 1.7 | 6.5 ± 1.7 | <0.001 * | 6.4 ± 1.6 | 6.5 ± 1.7 | 0.001 * | 5.6 ± 1.5 | 5.7 ± 1.5 | 0.04 * | 5.6 ± 1.5 | 5.7 ± 1.5 | 0.254 * |
| Presence of Helicobacter pylori (N = 10,890) | ||||||||||||
| Parameters | Male (n = 15,322) | Female (n = 5929) | ||||||||||
| Mononuclear cell | Neutrophil | Mononuclear cell | Neutrophil | |||||||||
| Absence/ Mild (n = 740) | Moderate/ Severe (n = 7400) | p | Absence (n = 352) | Presence (n = 7788) | p | Absence/ Mild (n = 280) | Moderate/ Severe (n = 2470) | p | Absence (n = 135) | Presence (n = 2615) | p | |
| Clinical | ||||||||||||
| Age, years | 43.8 ± 9.2 | 42.2 ± 8.6 | <0.001 * | 44.3 ± 9.2 | 42.3 ± 8.6 | <0.001 * | 46.1 ± 10.2 | 44.3 ± 9.8 | 0.003 * | 46.1 ± 10.5 | 44.4 ± 9.8 | 0.042 * |
| Body mass index (kg/m2) | 24.8 ± 2.8 | 24.7 ± 2.8 | 0.076 * | 24.7 ± 2.7 | 24.7 ± 2.8 | 0.974 * | 22.8 ± 2.9 | 23.0 ± 3.1 | 0.461 * | 23.0 ± 2.8 | 23.0 ± 3.1 | 0.922 * |
| ‡Regular exercise, % | 202 (27.3) | 1877 (25.4) | 0.269 † | 89 (25.3) | 1990 (25.6) | 0.96 † | 76 (27.1) | 651 (26.4) | 0.833 † | 34 (25.2) | 693 (26.5) | 0.812 † |
| Cigarette smoking, % | 570 (77) | 5795 (78.3) | 0.447 † | 267 (75.9) | 6098 (78.3) | 0.307 † | 29 (10.4) | 358 (14.5) | 0.073 † | 14 (10.4) | 373 (14.3) | 0.254 † |
| §Alcohol consumption, % | 631 (85.3) | 6298 (85.1) | 0.949 † | 296 (84.1) | 6633 (85.2) | 0.631 † | 108 (38.6) | 922 (37.3) | 0.732 † | 59 (43.7) | 971 (37.1) | 0.148 † |
| Hypertension, % | 161 (21.8) | 1657 (22.4) | 0.727 † | 94 (26.7) | 1724 (22.1) | 0.05 † | 45 (16.1) | 395 (16) | 0.999 † | 28 (20.7) | 412 (15.8) | 0.155 † |
| Diabetes, % | 53 (7.2) | 365 (4.9) | 0.011 † | 22 (6.2) | 396 (5.1) | 0.398 † | 5 (1.8) | 84 (3.4) | 0.204 † | 3 (2.2) | 86 (3.3) | 0.665 † |
| Hepatitis, % | 89 (12) | 772 (10.4) | 0.2 † | 36 (10.2) | 825 (10.6) | 0.897 † | 27 (9.6) | 247 (10) | 0.933 † | 13 (9.6) | 261 (10) | 0.999 † |
| SBP, mmHg | 116.4 ± 12.6 | 117.6 ± 12.1 | 0.01 * | 117.1 ± 13.3 | 117.5 ± 12.1 | 0.584 * | 111.3 ± 13.9 | 111.7 ± 13.8 | 0.647 * | 111.9 ± 15.7 | 111.7 ± 13.7 | 0.908 * |
| DBP, mmHg | 76.3 ± 8.2 | 76.4 ± 8.6 | 0.814 * | 77.0 ± 9.1 | 76.4 ± 8.5 | 0.191 * | 72.1 ± 9.6 | 72.0 ± 9.4 | 0.955 * | 72.0 ± 10.2 | 72.0 ± 9.4 | 0.954 * |
| Laboratory | ||||||||||||
| HDL, mg/dL | 51.0 ± 11.1 | 50.3 ± 10.7 | 0.084 * | 50.0 ± 11.0 | 50.3 ± 10.8 | 0.598 * | 61.2 ± 14.5 | 58.9 ± 12.9 | 0.012 * | 61.0 ± 13.4 | 59.0 ± 13 | 0.076 * |
| LDL, mg/dL | 118.2 ± 29.9 | 118.6 ± 29.8 | 0.72 * | 116.6 ± 27.3 | 118.7 ± 29.9 | 0.172 * | 110.7 ± 29.2 | 110.0 ± 30.6 | 1.726 * | 111.8 ± 29.7 | 110.0 ± 30.5 | 1.499 * |
| Triglycerides, mg/dL | 154.9 ± 101.8 | 153.1 ± 96.4 | 0.66 * | 152.8 ± 102.3 | 153.3 ± 96.6 | 0.918 * | 103.0 ± 70.9 | 102.5 ± 60 | 0.914 * | 100.5 ± 63.4 | 102.7 ± 61.1 | 0.692 * |
| VLDL, mg/dL | 31.0 ± 20.4 | 30.6 ± 19.3 | 0.66 * | 30.6 ± 20.5 | 30.7 ± 19.3 | 0.918 * | 20.6 ± 14.2 | 20.5 ± 12.0 | 0.914 * | 20.1 ± 12.7 | 20.5 ± 12.2 | 0.692 * |
| Leukocyte count (109/L) | 51.0 ± 11.1 | 50.3 ± 10.7 | 0.084 * | 50.0 ± 11.0 | 50.3 ± 10.8 | 0.598 * | 5.8 ± 1.4 | 5.9 ± 1.5 | 0.206 * | 5.8 ± 1.5 | 5.9 ± 1.5 | 0.278 * |
| Male (n = 15,322) | |||||||||
|---|---|---|---|---|---|---|---|---|---|
| Parameters | Helicobacter pylori | Mononuclear Cell | Neutrophil | ||||||
| Absence (n = 7182) | Presence (n = 8140) | p | Absence/Mild (n = 5251) | Moderate/Severe (n = 10,071) | p | Absence (n = 3811) | Presence (n = 11,511) | p | |
| Clinical | |||||||||
| Age, years | 44.5 ± 9.8 | 42.4 ± 8.7 | <0.001 * | 44.3 ± 9.7 | 42.9 ± 9 | <0.001 * | 44.3 ± 9.6 | 43.1 ± 9.2 | <0.001 * |
| Body mass index (kg/m2) | 24.6 ± 2.8 | 24.7 ± 2.8 | 0.337 * | 24.6 ± 2.8 | 24.7 ± 2.8 | 0.112 * | 24.6 ± 2.8 | 24.7 ± 2.8 | 0.056 * |
| ‡ Regular exercise | 1905 (26.5) | 1893 (23.3) | <0.001† | 1374 (26.2) | 2424 (24.1) | 0.005† | 985 (25.8) | 2813 (24.4) | 0.085 † |
| Cigarette smoking | 5476 (76.2) | 6365 (78.2) | 0.004† | 3998 (76.1) | 7843 (77.9) | 0.016† | 2888 (75.8) | 8953 (77.8) | 0.011† |
| § Alcohol consumption | 5930 (82.6) | 6929 (85.1) | <0.001† | 4325 (82.4) | 8534 (84.7) | <0.001† | 3136 (82.3) | 9723 (84.5) | 0.002 † |
| Hypertension | 1789 (24.9) | 1818 (22.3) | <0.001† | 1272 (24.2) | 2335 (23.2) | 0.156 † | 958 (25.1) | 2649 (23) | 0.008 † |
| Diabetes | 407 (5.7) | 418 (5.1) | 0.156 † | 310 (5.9) | 515 (5.1) | 0.044† | 203 (5.3) | 622 (5.4) | 0.888 † |
| Hepatitis | 744 (10.4) | 861 (10.6) | 0.679 † | 583 (11.1) | 1022 (10.1) | 0.071 † | 386 (10.1) | 1219 (10.6) | 0.438 † |
| SBP, mmHg | 117.7 ± 12.6 | 117.5 ± 12.2 | 0.205 * | 117.3 ± 12.5 | 117.7 ± 12.3 | 0.049 * | 117.7 ± 12.8 | 117.6 ± 12.3 | 0.446 * |
| DBP, mmHg | 76.3 ± 8.6 | 76.4 ± 8.6 | 0.695 * | 76.2 ± 8.6 | 76.5 ± 8.6 | 0.039 * | 76.4 ± 8.6 | 76.4 ± 8.6 | 0.563 * |
| Laboratory | |||||||||
| HDL, mg/dL | 50.7 ± 11.2 | 50.3 ± 10.8 | 0.02 * | 50.9 ± 11.2 | 50.3 ± 10.8 | 0.002 * | 50.7 ± 11.2 | 50.5 ± 10.9 | 0.234 * |
| LDL, mg/dL | 118.2 ± 29.8 | 118.6 ± 29.8 | 0.408 * | 117.9 ± 30 | 118.6 ± 29.7 | 0.12 * | 117.8 ± 29.4 | 118.6 ± 30 | 0.189 * |
| Triglycerides, mg/dL | 150.4 ± 91.9 | 153.3 ± 96.9 | 0.054 * | 149.7 ± 92.5 | 153.1 ± 95.6 | 0.035 * | 149.2 ± 90.5 | 152.8 ± 95.9 | 0.035 * |
| VLDL, mg/dL | 30.1 ± 18.4 | 30.7 ± 19.4 | 0.054 * | 29.9 ± 18.5 | 30.6 ± 19.1 | 0.035 * | 29.8 ± 18.1 | 30.6 ± 19.2 | 0.035 * |
| Leukocyte count (109/L) | 6.4 ± 1.7 | 6.6 ± 1.6 | <0.001 * | 6.4 ± 1.7 | 6.6 ± 1.6 | <0.001 * | 6.4 ± 1.7 | 6.5 ± 1.6 | <0.001 * |
| Female (n = 5929) | |||||||||
| Parameters | Helicobactor pylori | Mononuclear cell | Neutrophil | ||||||
| Absence (n = 3179) | Presence (n = 2750) | p | Absence/Mild (n = 2367) | Moderate/Severe (n = 3562) | p | Absence (n = 1745) | Presence (n = 4184) | p | |
| Clinical | |||||||||
| Age, years | 45.3 ± 10.8 | 44.5 ± 9.8 | 0.002 * | 44.7 ± 10.5 | 45.0 ± 10.3 | 0.207 * | 44.6 ± 10.6 | 45.0 ± 10.3 | 0.229 * |
| Body mass index (kg/m2) | 22.9 ± 3.1 | 23.0 ± 3.1 | 0.704 * | 22.8 ± 3 | 23.0 ± 3.2 | 0.012 * | 22.8 ± 3 | 23.0 ± 3.1 | 0.007 * |
| ‡ Regular exercise | 807 (25.4) | 694 (25.2) | 0.919 † | 603 (25.5) | 898 (25.2) | 0.842 † | 436 (25) | 1065 (25.5) | 0.73 † |
| Cigarette smoking | 407 (12.8) | 387 (14.1) | 0.163 † | 285 (12.0) | 509 (14.3) | 0.014† | 198 (11.3) | 596 (14.2) | 0.003† |
| § Alcohol consumption | 1082 (34.0) | 1030 (37.5) | 0.007† | 811 (34.3) | 1301 (36.5) | 0.08 † | 622 (35.6) | 1490 (35.6) | 0.999 † |
| Hypertension | 537 (16.9) | 440 (16) | 0.374 † | 400 (16.9) | 577 (16.2) | 0.499 † | 292 (16.7) | 685 (16.4) | 0.761 † |
| Diabetes | 114 (3.6) | 89 (3.2) | 0.505 † | 80 (3.4) | 123 (3.5) | 0.937 † | 62 (3.6) | 141 (3.4) | 0.783 † |
| Hepatitis | 303 (9.5) | 274 (10) | 0.606 † | 214 (9.0) | 363 (10.2) | 0.156 † | 152 (8.7) | 425 (10.2) | 0.096 † |
| SBP, mmHg | 112.0 ± 13.8 | 111.7 ± 13.8 | 0.401 * | 111.5 ± 13.7 | 112.1 ± 13.9 | 0.095 * | 111.2 ± 13.8 | 112.2 ± 13.8 | 0.014 * |
| DBP, mmHg | 72.6 ± 9.3 | 72.0 ± 9.4 | 0.033 * | 72.3 ± 9.4 | 72.3 ± 9.3 | 0.961 * | 72.2 ± 9.3 | 72.4 ± 9.4 | 0.395 * |
| Laboratory | |||||||||
| HDL, mg/dL | 59.0 ± 13.3 | 59.1 ± 13.1 | 0.856 * | 59.7 ± 13.7 | 58.7 ± 12.8 | 0.004 * | 59.4 ± 13.4 | 58.9 ± 13.1 | 0.233 * |
| LDL, mg/dL | 109.6 ± 31 | 110.1 ± 30.4 | 0.531 * | 108.9 ± 30.9 | 110.5 ± 30.6 | 0.044 * | 109.9 ± 31.0 | 109.8 ± 30.6 | 0.888 * |
| Triglycerides, mg/dL | 102.9 ± 61.5 | 102.6 ± 61.2 | 0.815 * | 102.0 ± 62.6 | 103.2 ± 60.5 | 0.466 * | 102.2 ± 60.5 | 103.0 ± 61.7 | 0.67 * |
| VLDL, mg/dL | 20.6 ± 12.3 | 20.5 ± 12.2 | 0.815 * | 20.4 ± 12.5 | 20.6 ± 12.1 | 0.466 * | 20.4 ± 12.1 | 20.6 ± 12.3 | 0.67 * |
| Leukocyte count (109/L) | 5.7 ± 1.5 | 5.9 ± 1.5 | <0.001 * | 5.7 ± 1.5 | 5.9 ± 1.5 | <0.001 * | 5.6 ± 1.5 | 5.8 ± 1.5 | <0.001 * |
| Parameters | Male (n = 15,322) | Female (n = 5929) | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Odds Ratio | 95% CI | p | Odds Ratio | 95% CI | p | ||||
| Low | High | Low | High | ||||||
| HDL (<60 mg/dL) | HP | ||||||||
| Crude | 0.892 | 0.822 | 0.968 | 0.006 | 0.966 | 0.871 | 1.07 | 0.505 | |
| *Adjusted | 0.898 | 0.826 | 0.977 | 0.012 | 0.926 | 0.832 | 1.029 | 0.154 | |
| Mononuclear cell | |||||||||
| Crude | 0.904 | 0.83 | 0.984 | 0.02 | 0.891 | 0.802 | 0.989 | 0.03 | |
| *Adjusted | 0.913 | 0.837 | 0.997 | 0.042 | 0.888 | 0.798 | 0.99 | 0.032 | |
| Neutrophil | |||||||||
| Crude | 0.942 | 0.858 | 1.034 | 0.21 | 0.93 | 0.831 | 1.041 | 0.206 | |
| *Adjusted | 0.95 | 0.864 | 1.045 | 0.295 | 0.946 | 0.843 | 1.063 | 0.35 | |
| LDL (>130 mg/dL) | HP | ||||||||
| Crude | 1.027 | 0.96 | 1.098 | 0.44 | 1.07 | 0.949 | 1.207 | 0.267 | |
| *Adjusted | 1.026 | 0.958 | 1.098 | 0.462 | 1.141 | 1.007 | 1.292 | 0.038 | |
| Mononuclear cell | |||||||||
| Crude | 1.043 | 0.972 | 1.12 | 0.238 | 1.088 | 0.962 | 1.23 | 0.179 | |
| *Adjusted | 1.037 | 0.966 | 1.114 | 0.314 | 1.072 | 0.944 | 1.217 | 0.283 | |
| Neutrophil | |||||||||
| Crude | 1.05 | 0.971 | 1.135 | 0.22 | 0.999 | 0.876 | 1.139 | 0.987 | |
| *Adjusted | 1.044 | 0.965 | 1.129 | 0.28 | 0.973 | 0.849 | 1.115 | 0.692 | |
| Triglycerides (>150 mg/dL) | HP | ||||||||
| Crude | 1.06 | 0.993 | 1.131 | 0.081 | 1.043 | 0.905 | 1.203 | 0.56 | |
| *Adjusted | 1.039 | 0.971 | 1.112 | 0.265 | 1.134 | 0.977 | 1.317 | 0.098 | |
| Mononuclear cell | |||||||||
| Crude | 1.058 | 0.988 | 1.133 | 0.108 | 1.11 | 0.959 | 1.284 | 0.162 | |
| *Adjusted | 1.032 | 0.961 | 1.108 | 0.391 | 1.084 | 0.931 | 1.263 | 0.3 | |
| Neutrophil | |||||||||
| Crude | 1.004 | 0.859 | 1.173 | 0.963 | 1.078 | 1.000 | 1.163 | 0.05 | |
| *Adjusted | 1.054 | 0.975 | 1.140 | 0.185 | 0.961 | 0.816 | 1.132 | 0.636 | |
| VLDL (>30 mg/dL) | HP | ||||||||
| Crude | 1.060 | 0.993 | 1.131 | 0.081 | 1.043 | 0.905 | 1.203 | 0.56 | |
| *Adjusted | 1.039 | 0.971 | 1.112 | 0.265 | 1.134 | 0.977 | 1.317 | 0.098 | |
| Mononuclear cell | |||||||||
| Crude | 1.058 | 0.988 | 1.133 | 0.108 | 1.11 | 0.959 | 1.284 | 0.162 | |
| *Adjusted | 1.032 | 0.961 | 1.108 | 0.391 | 1.084 | 0.931 | 1.263 | 0.3 | |
| Neutrophil | |||||||||
| Crude | 1.078 | 1.000 | 1.163 | 0.05 | 1.004 | 0.859 | 1.173 | 0.963 | |
| *Adjusted | 1.054 | 0.975 | 1.14 | 0.185 | 0.961 | 0.816 | 1.132 | 0.636 | |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, D.-H.; Son, B.K.; Min, K.-W.; Han, S.K.; Na, J.U.; Choi, P.C.; Kim, H.-L.; Kwon, M.J.; Oh, Y.H.; Jung, W.Y.; et al. Chronic Gastritis Is Associated with a Decreased High-Density Lipid Level: Histological Features of Gastritis Based on the Updated Sydney System. J. Clin. Med. 2020, 9, 1856. https://doi.org/10.3390/jcm9061856
Kim D-H, Son BK, Min K-W, Han SK, Na JU, Choi PC, Kim H-L, Kwon MJ, Oh YH, Jung WY, et al. Chronic Gastritis Is Associated with a Decreased High-Density Lipid Level: Histological Features of Gastritis Based on the Updated Sydney System. Journal of Clinical Medicine. 2020; 9(6):1856. https://doi.org/10.3390/jcm9061856
Chicago/Turabian StyleKim, Dong-Hoon, Byoung Kwan Son, Kyueng-Whan Min, Sang Kuk Han, Ji Ung Na, Pil Cho Choi, Hack-Lyoung Kim, Mi Jung Kwon, Young Ha Oh, Woon Yong Jung, and et al. 2020. "Chronic Gastritis Is Associated with a Decreased High-Density Lipid Level: Histological Features of Gastritis Based on the Updated Sydney System" Journal of Clinical Medicine 9, no. 6: 1856. https://doi.org/10.3390/jcm9061856
APA StyleKim, D.-H., Son, B. K., Min, K.-W., Han, S. K., Na, J. U., Choi, P. C., Kim, H.-L., Kwon, M. J., Oh, Y. H., Jung, W. Y., Moon, J.-Y., Hong, S., Oh, K.-W., & Kim, Y. S. (2020). Chronic Gastritis Is Associated with a Decreased High-Density Lipid Level: Histological Features of Gastritis Based on the Updated Sydney System. Journal of Clinical Medicine, 9(6), 1856. https://doi.org/10.3390/jcm9061856