1. Introduction
Colorectal cancer (CRC) is the third most commonly diagnosed cancer in men and the second most common cancer in women. In 2018, CRC accounted for an estimated 1,850,000 new cancer cases worldwide. At the same time, CRC was the second leading cause of cancer deaths, responsible for approximately 880,000 deaths [
1]. The incidence of CRC varies highly by region. The highest incidence rates are reported in Australia, New Zealand, Europe, and North America, and the lowest rates are found in Africa and South-Central Asia [
1,
2]. In recent years, CRC mortality has been steadily declining in developed countries. This may be attributed to advanced screening programs and more effective treatment methods [
3].
Early disease detection may determine the survival of a patient. Two main screening strategies, fecal tests for occult blood or endoscopy, are currently used in CRC clinics. Stool-based tests detect CRC with a sensitivity of 79% and specificity of 94% [
4]. However, despite their low costs, non-invasiveness, and demonstrated positive effect on lowering CRC-related mortality, the compliance of patients with stool-based methods is unsatisfactory [
4]. When positive, fecal tests are followed by colonoscopy, which is invasive and carries a risk of complications, and thus is tolerated poorly by patients. In addition, colonoscopy, the gold standard of CRC detection, is a costly procedure, with its success rate highly dependent on the endoscopist’s skills [
5,
6]. As a result, the adherence to screening in Europe is suboptimal and the average participation does not exceed 50% [
7]. Therefore, blood-based biomarkers—non-invasive and easily accessible—are sought after [
5].
Metabolic reprogramming has been recognized as one of eight cancer hallmarks [
8]. Changes in the metabolome can be both a cause and an effect of the disease. Consequently, metabolomics is gaining interest as a potential tool in biomarker and drug research [
6]. Mass spectrometry (MS) coupled with ultraperformance liquid chromatography (UPLC) is characterized by superior efficiency and reliability of metabolic profiling over other methods [
9]. A targeted approach to metabolomics allows for simultaneous quantification of a predetermined panel of metabolites present in a biological sample. Herein, the alterations in L-arginine/nitric oxide (NO) pathway metabolites and their potential utility as CRC diagnostic and prognostic biomarkers have been evaluated using liquid chromatography tandem mass spectrometry (LC-MS/MS).
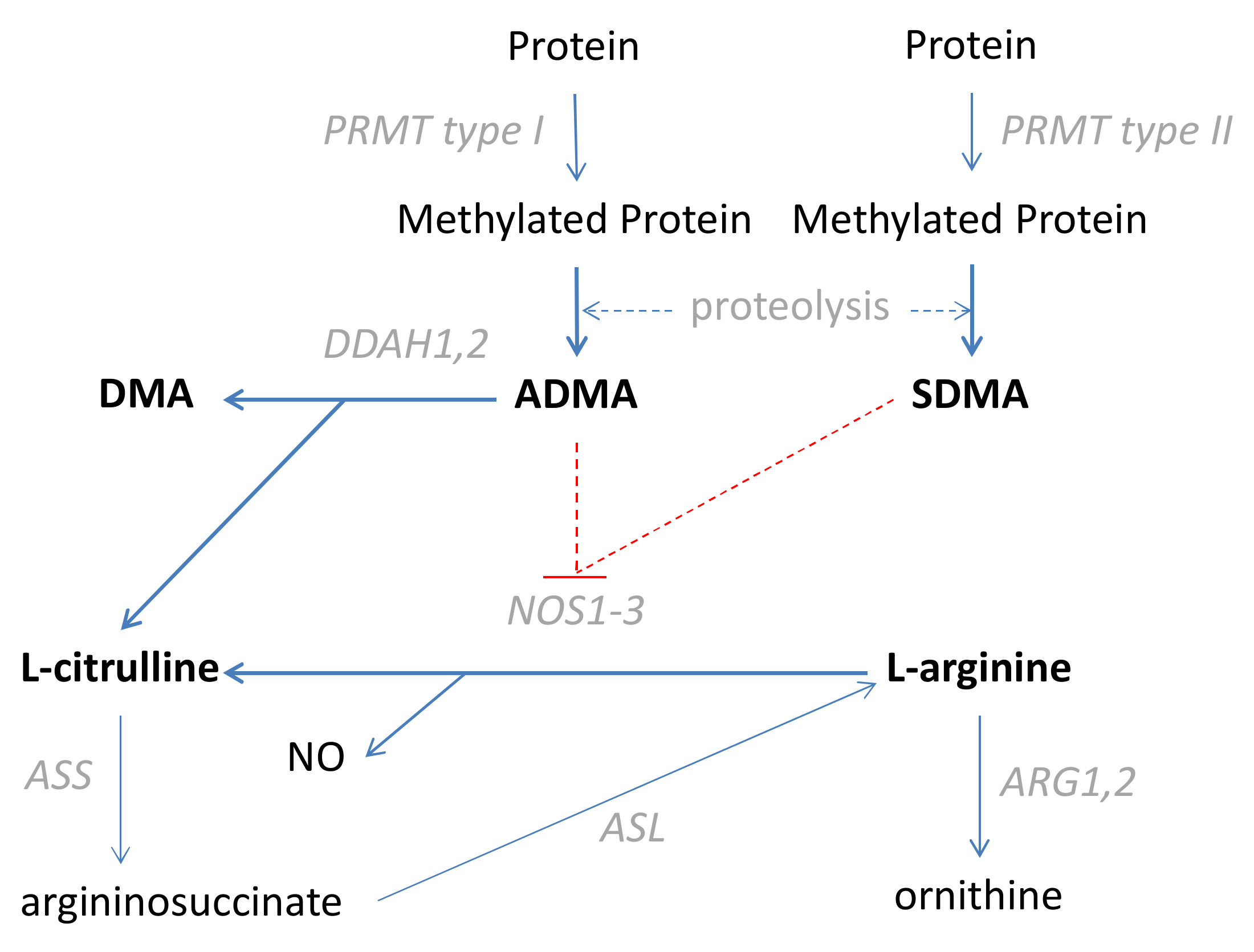
L-arginine, further referred to as arginine, is a conditionally essential amino acid used for NO synthesis by nitric oxide synthases (NOS), with citrulline as a co-product [
10]. The NO in the bowel, generated by endothelial (NOS3) and neuronal (NOS1) isoenzymes, contributes to the regulation of blood flow and bowel motility, respectively [
11]. In turn, its overproduction by the inducible NOS isoform (NOS2), during inflammation and oxidative stress, is associated with the synthesis of toxic peroxynitrite and neoplastic transformation [
11]. The activity of NOS enzymes, as well as arginine uptake, is inhibited by asymmetric and symmetric dimethylarginines (ADMA and SDMA, respectively). SDMA is excreted in the urine but ADMA is degraded into citrulline and dimethylamine (DMA) [
10]. A simplified scheme of the L-arginine/NO pathway is depicted in
Figure 1.
Previously, arginine and citrulline accumulation in colorectal cancer tissue, accompanied by the metabolite decrease at the systemic level, has been shown and attributed to the overexpression of
CAT-1, the cationic amino acid transporter [
12]. Others have demonstrated that ADMA and SDMA are elevated in both the tumor and adjacent tissue, which is accompanied by decreased nitrites and nitrates and interpreted as having a high angiogenic potential in the tumor microenvironment [
13]. Arginine has been repeatedly shown to facilitate tumor growth, also in CRC [
12]; hence, metabolite deprivation is viewed as an antineoplastic strategy [
14]. However, whether CRC is an arginine auxotrophic cancer remains controversial [
14,
15].
The aim of this study was to quantify systemic arginine, citrulline, ADMA, SDMA, and DMA, as well as to calculate the arginine/ADMA ratio in CRC patients. Its focus was on the suitability of metabolites as CRC biomarkers, individually and as a multi-metabolite panel. In addition, a group of patients was followed up for three days post-surgery and metabolite concentrations were examined to assess their suitability as predictors of adverse clinical events such as operational morbidity, anastomotic leakage, surgical site infections, and pathological postoperative ileus. Furthermore, the impact of patient- and surgery-related factors on metabolite concentration in the early perioperative period was evaluated.
4. Discussion
Metabolic reprogramming and avoiding destruction by the immune system have been recognized as emerging cancer hallmarks. Tumor-promoting inflammation, in turn, is known as its enabling characteristic [
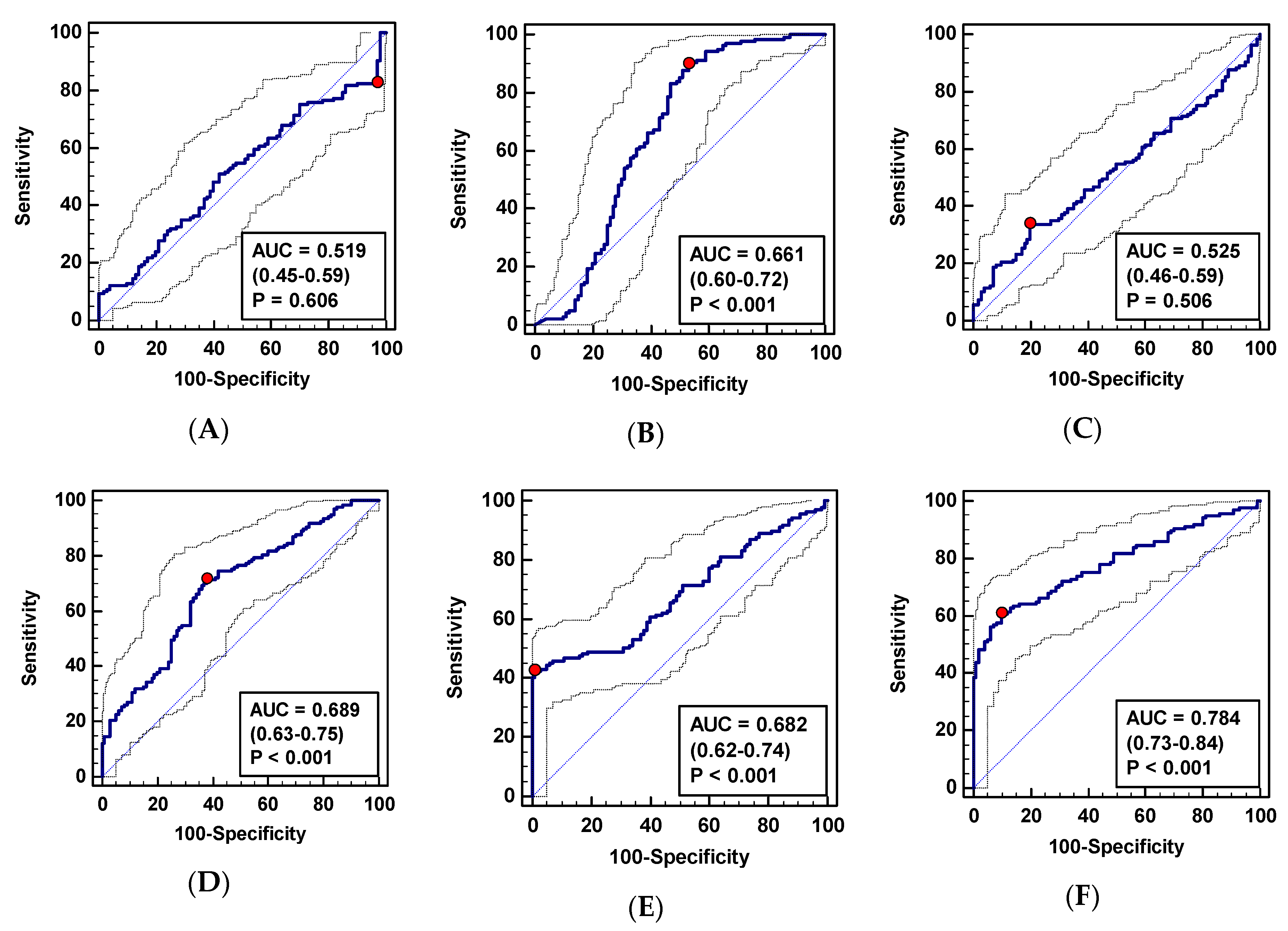
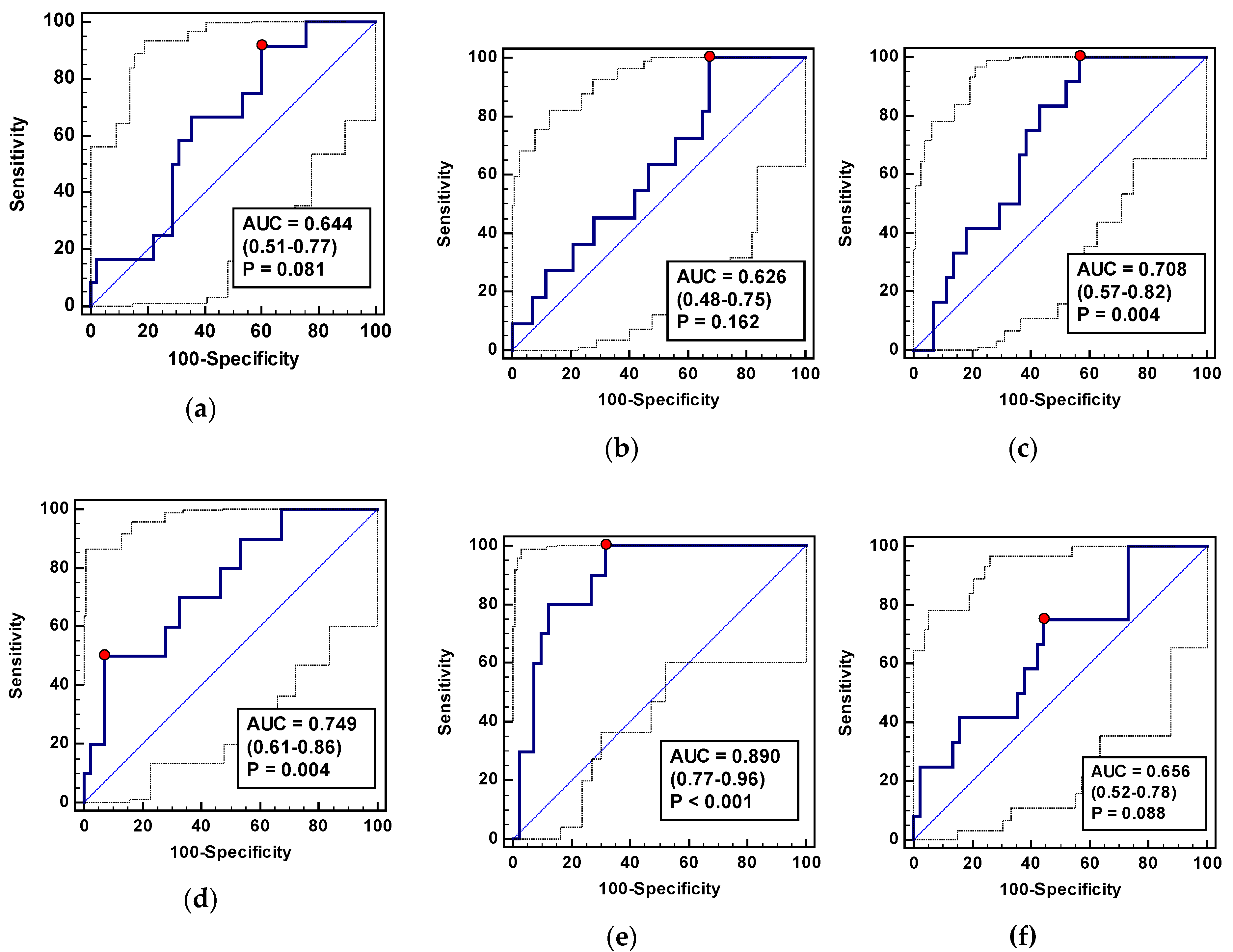
8]. The L-arginine/NO pathway is implicated in all three. Unsurprisingly, the pathway metabolite flux is affected by the disease and reflected at the systemic level by the altered pathway metabolite concentration, which might potentially be used for cancer detection. Targeted metabolomics enables simultaneous quantification of a set of metabolites allowing for the creation of multi-metabolite biomarker panels. The diagnostic accuracy of multi-analyte panels is potentially superior to the power of their individual components. This has been demonstrated previously, e.g., multi-marker diagnostic panels consisting of inflammatory mediators [
21,
22] or urine amino acid-related metabolites in mice CRC models [
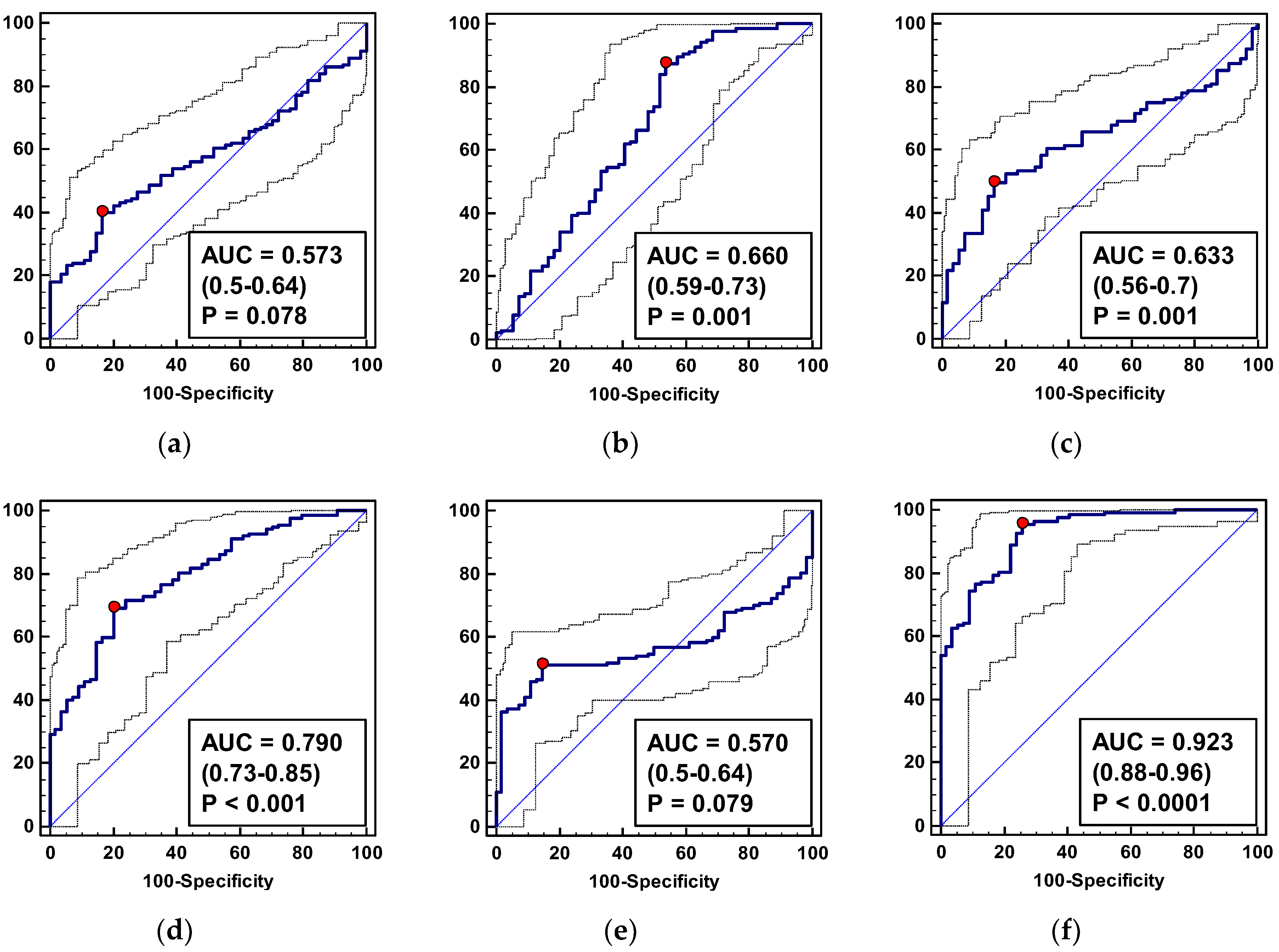
23]. Indeed, although CRC patients from our cohort differed significantly from healthy individuals in terms of citrulline (lower) and ADMA, SDMA, and DMA (higher), these metabolites individually possessed poor accuracy. The overall fair performance of SDMA was an exception but its individual impact was still outperformed by a panel consisting of SDMA, citrulline, and DMA. This panel displayed excellent accuracy as a potential CRC screening marker in the asymptomatic population. If positively validated, this finding is promising. Fecal-based assays, currently used for screening purposes, are comparable in cost and diagnostic power (characterized by lower sensitivity but higher specificity [
4]) and similarly non-invasive, but are currently underused due to poor compliance of patients [
7]. Blood-based metabolic panels might be better tolerated and have the advantage of being applicable in IBD patients.
In line with previous findings [
12], CRC patients had a decreased systemic arginine. Serum arginine depletion has been attributed to the upregulated amino acid uptake by tumors and linked with their accelerated growth, with concomitant obstruction of an anti-tumor immune response [
12]. The decrease in systemic arginine might be an early event in colonic carcinogenesis as it is also seen in active IBD [
16], a condition associated with an increased risk of CRC [
24]. ADMA and SDMA have been shown to accumulate in tumor tissues as well [
13,
23], and are elevated in the urine of CRC-bearing mice, together with arginine and citrulline [
23]. In prostate cancer, however, the disease has been associated with increased arginine as compared to benign prostate hyperplasia [
25]. In our study, eight patients were verified as having colorectal adenomas, and despite a low number of observations, were characterized by a statistically higher SDMA concentration than healthy controls, as well as higher DMA than controls and CRC patients. While promising, the potential of SDMA and DMA quantification for differential diagnosis requires the analysis of a larger group of adenoma patients. In addition to large adenomas, active IBD and functional bowel disorders, such as irritable bowel syndrome, are present with a set of symptoms similar to CRC. We found that CRC is distinguished, among conditions presenting overlapping symptoms, by lower systemic citrulline and DMA, and higher SDMA. The analysis of pathway metabolites’ potential as differential markers and surveillance tools showed that the combination of ADMA, SDMA, and DMA allows for CRC detection in the symptomatic population with a fair accuracy, while citrulline alone is a fair surveillance marker.
SDMA and DMA are outside the mainstream research and data on their concentration in cancer are scant. A cancer-related elevation in systemic SDMA has been reported in hematological malignancies and found to be useful in predicting overall mortality [
18]. In CRC, the metabolite accumulated within a tumor-adjacent tissue as compared to normal tissue, and was associated with an increased risk of metastasis [
13]. In turn, metabolic profiling of CRC tissue samples has revealed that DMA accumulated in tumors with lymph node involvement, as compared to normal tissue [
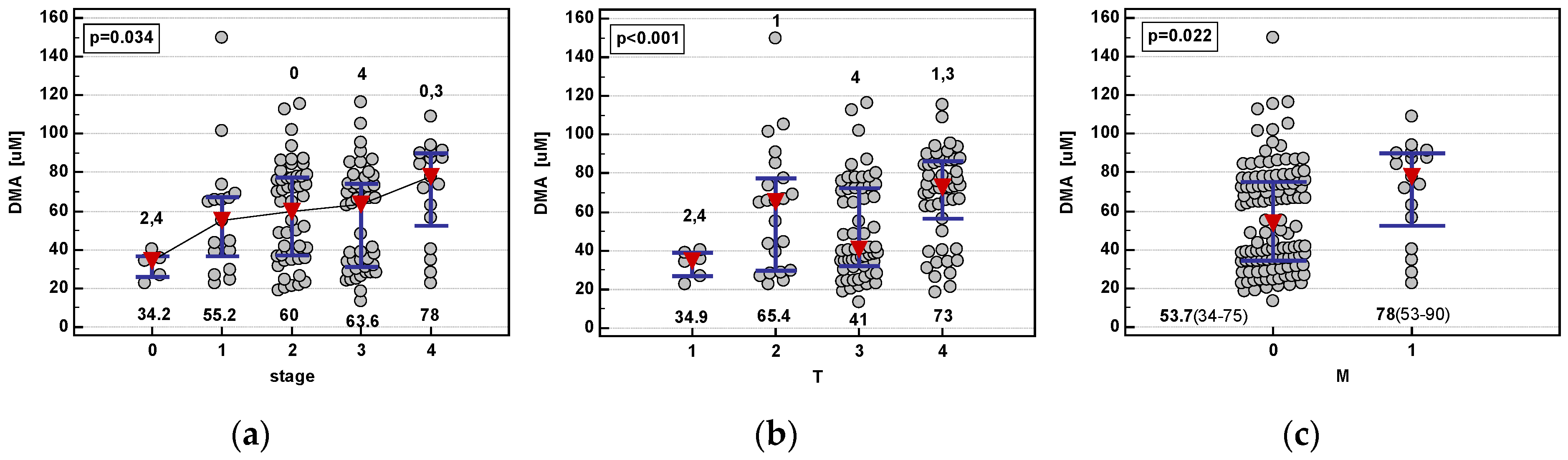
26]. A similar study in esophageal cancer has shown that DMA is associated with cancer progression but decreases in stage III tumors, and only its elevation in stage IV is significant as compared to normal tissue [
27]. Here, systemic DMA was the only pathway metabolite reflecting CRC advancement. It displayed an association pattern analogous to the local DMA concentration in esophageal cancer. A systemic elevation of DMA is also seen in IBD [
16], as demonstrated here, significantly more so than in CRC.
An interesting observation is that the baseline systemic metabolite concentration differs depending on the tumor anatomical subsite, with a higher concentration of arginine, ADMA, and SDMA in left-sided colonic tumors. There is a growing awareness of the molecular heterogeneity of cancers arising in different segments of the colorectum [
28,
29,
30,
31] that may also be reflected at the systemic level [
22,
32,
33]. Proximal tumors are reportedly more advanced upon diagnosis, larger, and less differentiated [
34], displaying poor responsiveness to chemotherapy and, consequently, associated with a worse prognosis [
35]. Lower systemic arginine in right-sided cancers may indicate accelerated amino acid uptake by tumor cells and contribute to higher aggressiveness of cancers in this location. Owing to the association of arginine with immunity [
36], it would also translate into the induction of immunosuppression in patients with right-sided CRC. As demonstrated here, the dependence of a potential biomarker on the primary tumor location should be taken into consideration as it might affect its diagnostic power.
The ADMA and arginine-to-ADMA ratio are considered sensitive indicators of endothelial dysfunction and therefore risk markers in cardiovascular medicine [
37]. In cancer, arginine and ADMA have demonstrated potential as markers of cardiac dysfunction related to cancer therapeutics [
38]. Moreover, previous studies on critically ill patients or those undergoing cardiac surgery have shown that ADMA may be a novel biomarker indicative of increased perioperative risk [
39,
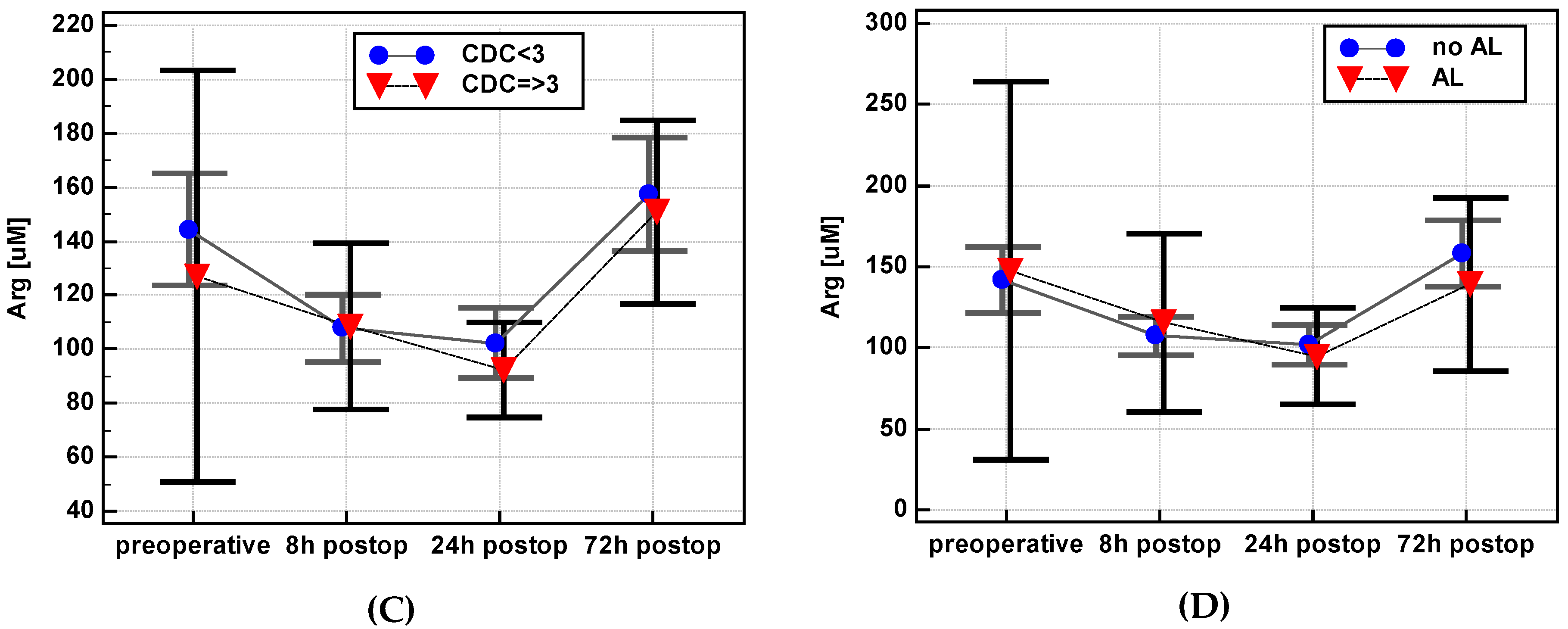
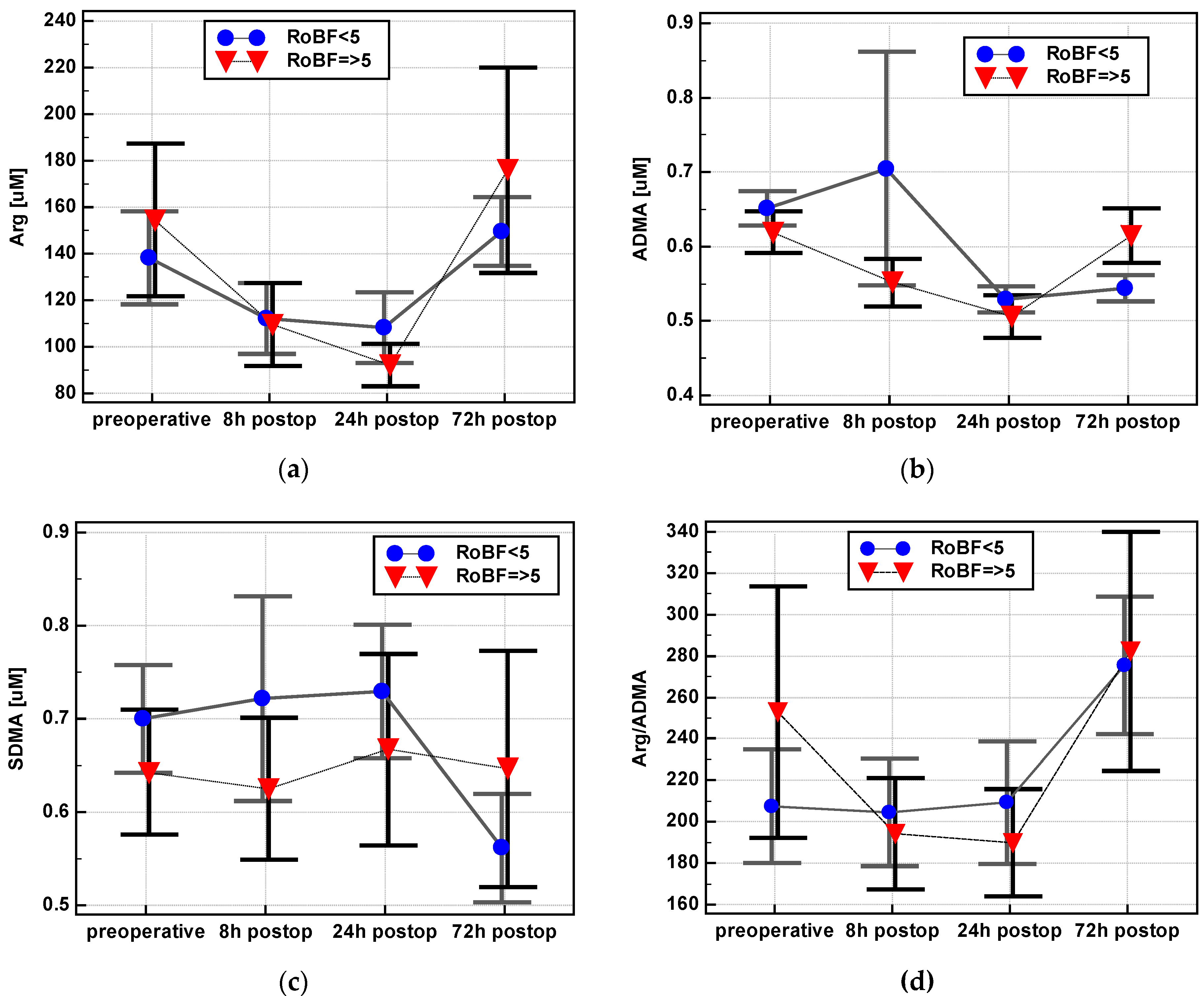
40]. Corroborating this notion, the dynamics in ADMA concentration in our cohort differed depending on the Clavien-Dindo score, which, in turn, is inversely related to the five-year overall survival, disease-free survival, and cancer-specific survival and directly correlated with overall recurrence rates [
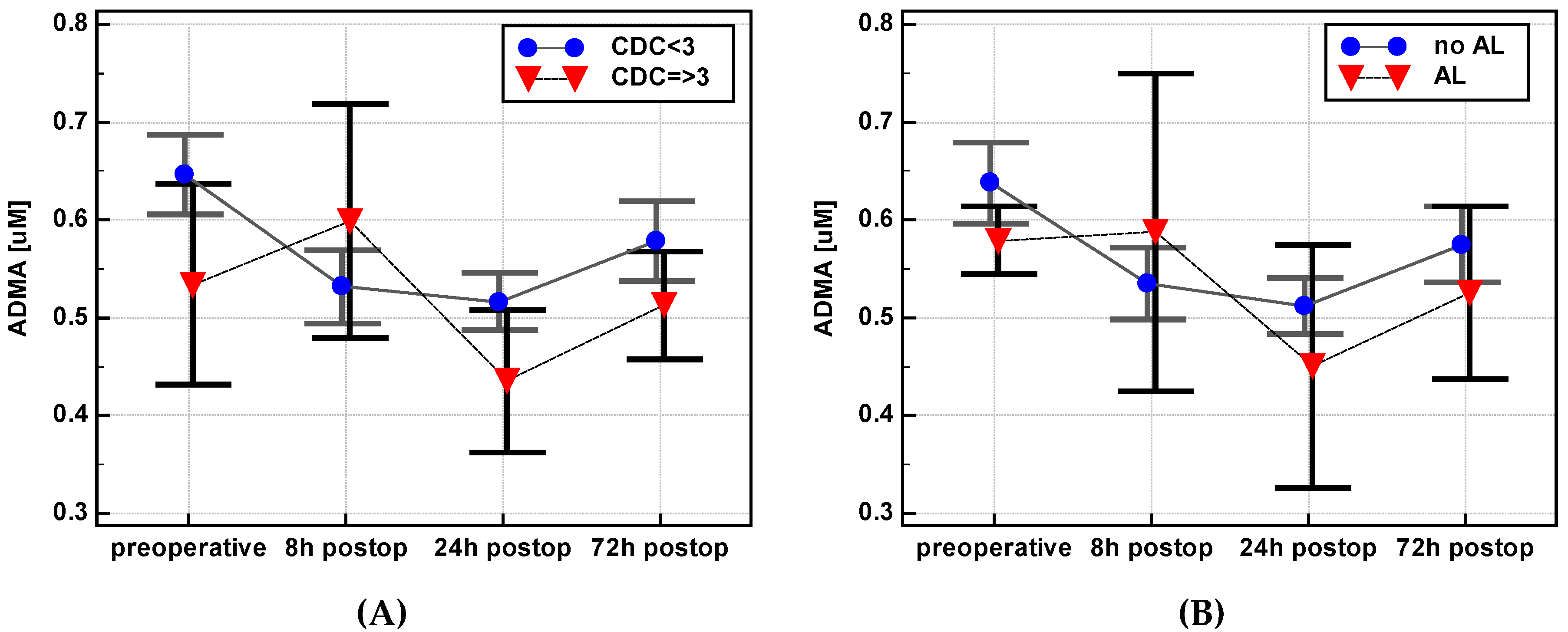
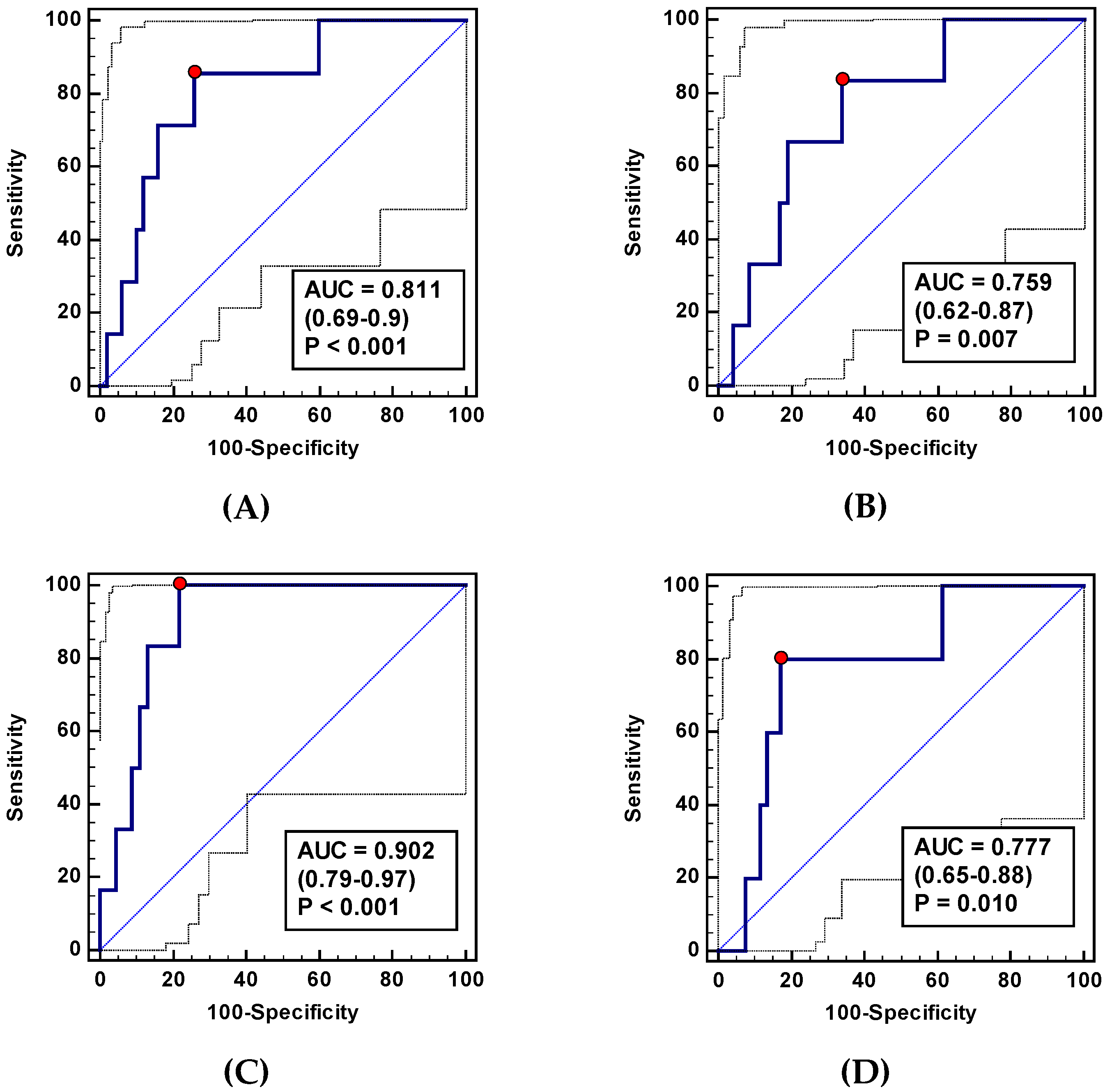
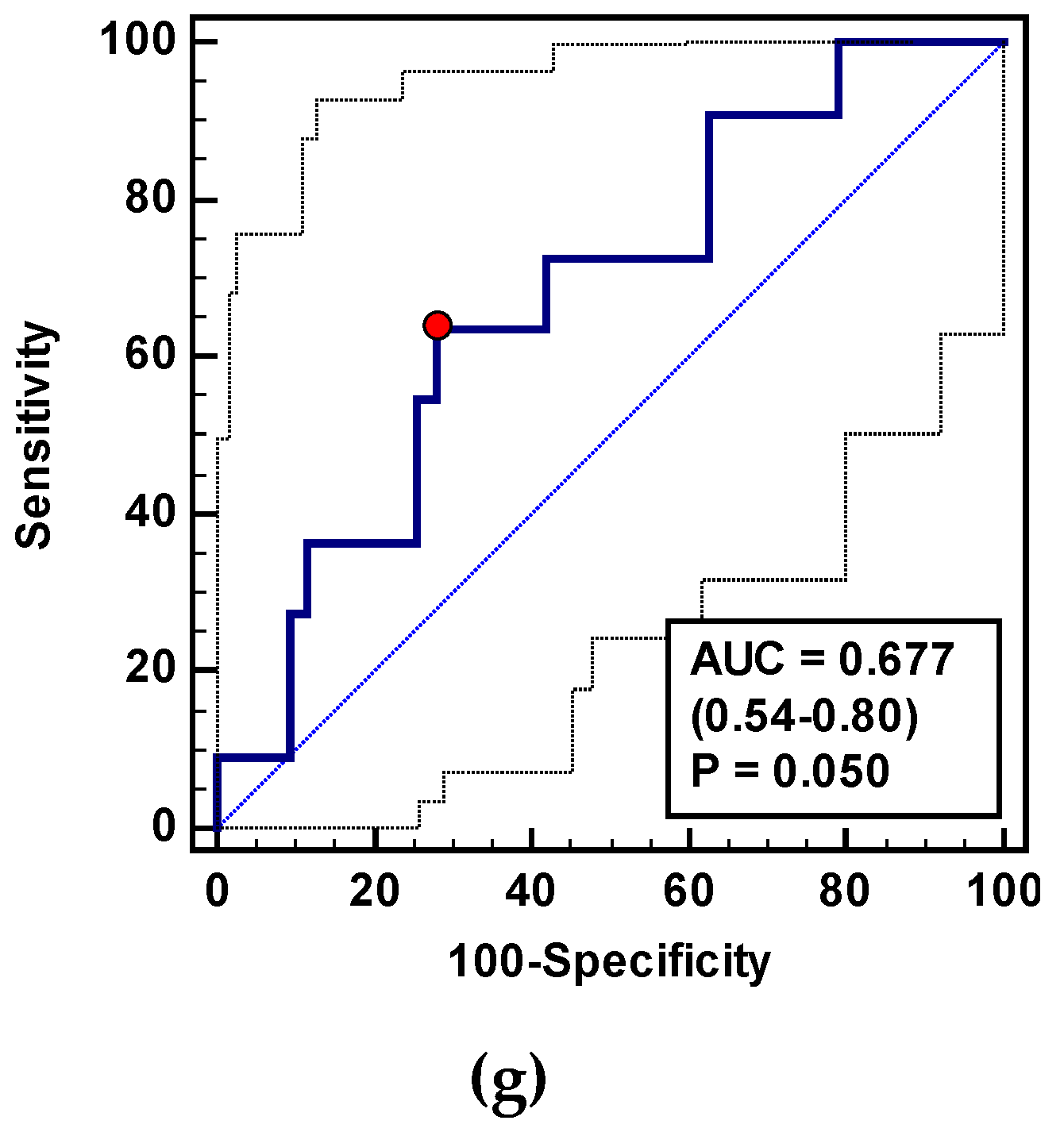
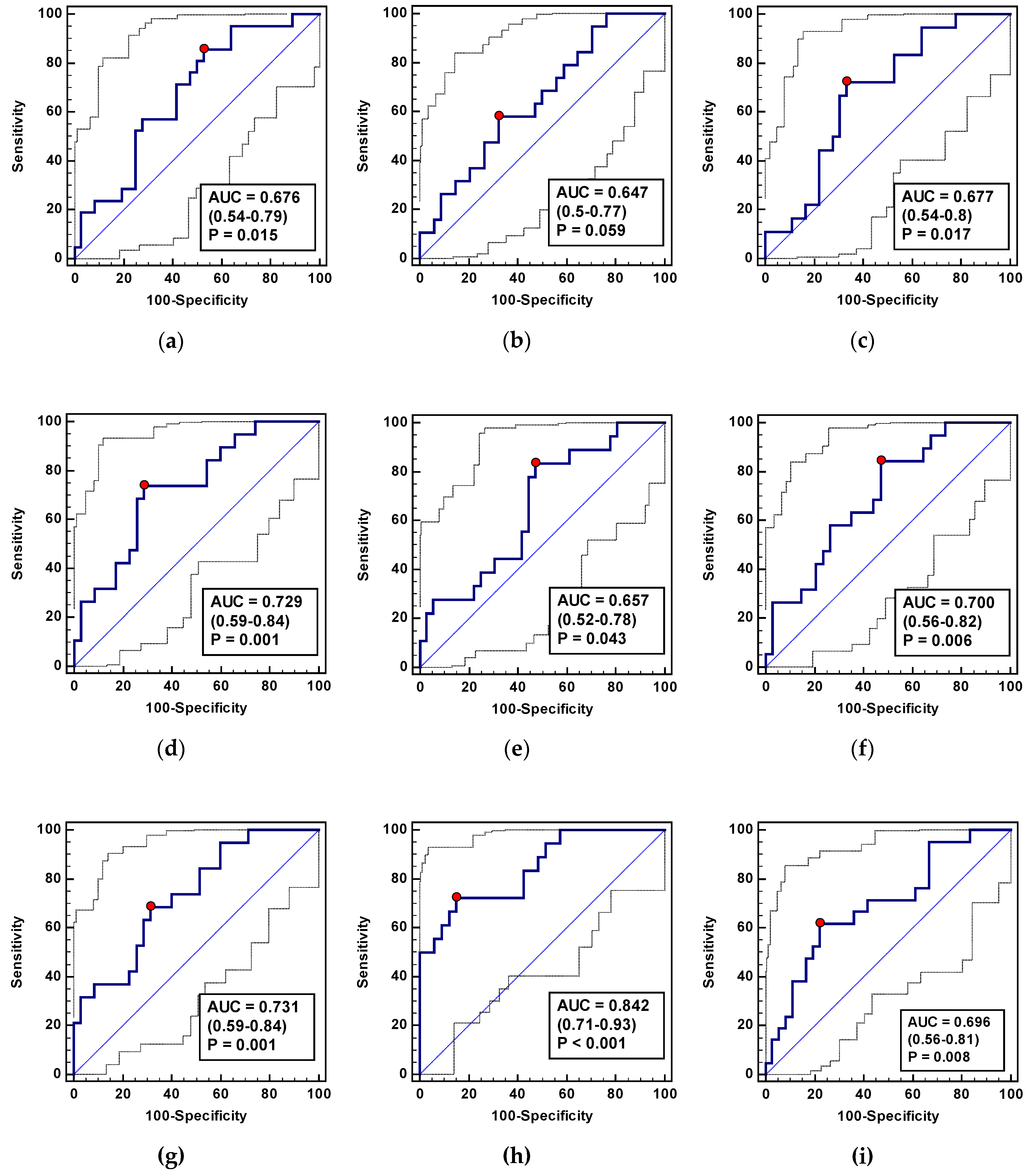
41]. Indices based on ADMA dynamics might predict an increased risk for severe postoperative complications (CDC ≥ 3), with very good accuracy and excellent sensitivity prior to their clinical manifestation.
Likewise, biomarkers predictive of perioperative complications following colorectal resection are being extensively investigated [
42]. To promote a complication-free recovery, the modern model of perioperative care, the “fast track”, has been introduced and popularized worldwide [
43]. This package of perioperative modifications results in fewer complications, reduction of cost, shortening of hospital stay, and quicker overall recovery. Patients undergoing colorectal surgery with such perioperative care are routinely discharged home as early as the 3rd–5th postoperative day. Unfortunately, this early discharge carries the risk of developing postoperative complications such as SSI, bowel obstruction or anastomotic leakage at home, where access to medical expertise is limited. Reliable markers of perioperative complications would help determine which patients are eligible for a safe early discharge. Therefore, we explored whether the changes in L-arginine/NO pathway metabolites in the early perioperative period may be useful as indicators of the most typical adverse clinical events such as anastomotic leakage, surgical site infections, and delayed restoration of bowel function. To the best of our knowledge, there is only one preliminary study, conducted on a mixed cohort (benign diseases included) of 16 patients undergoing laparoscopic colorectal surgery, in which arginine, ADMA, and citrulline concentration had been followed [
44]. Corroborating the results of Ragina et al. [
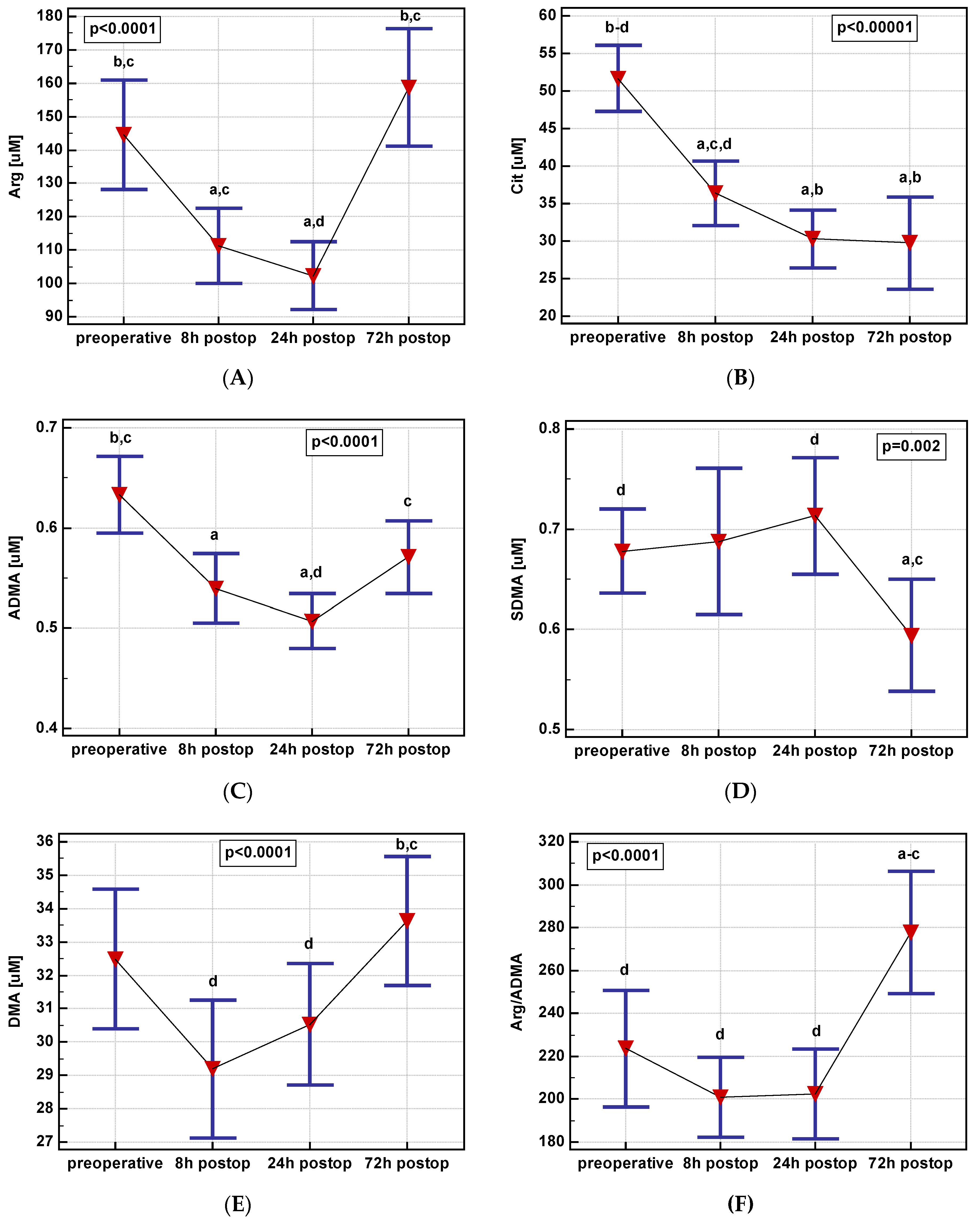
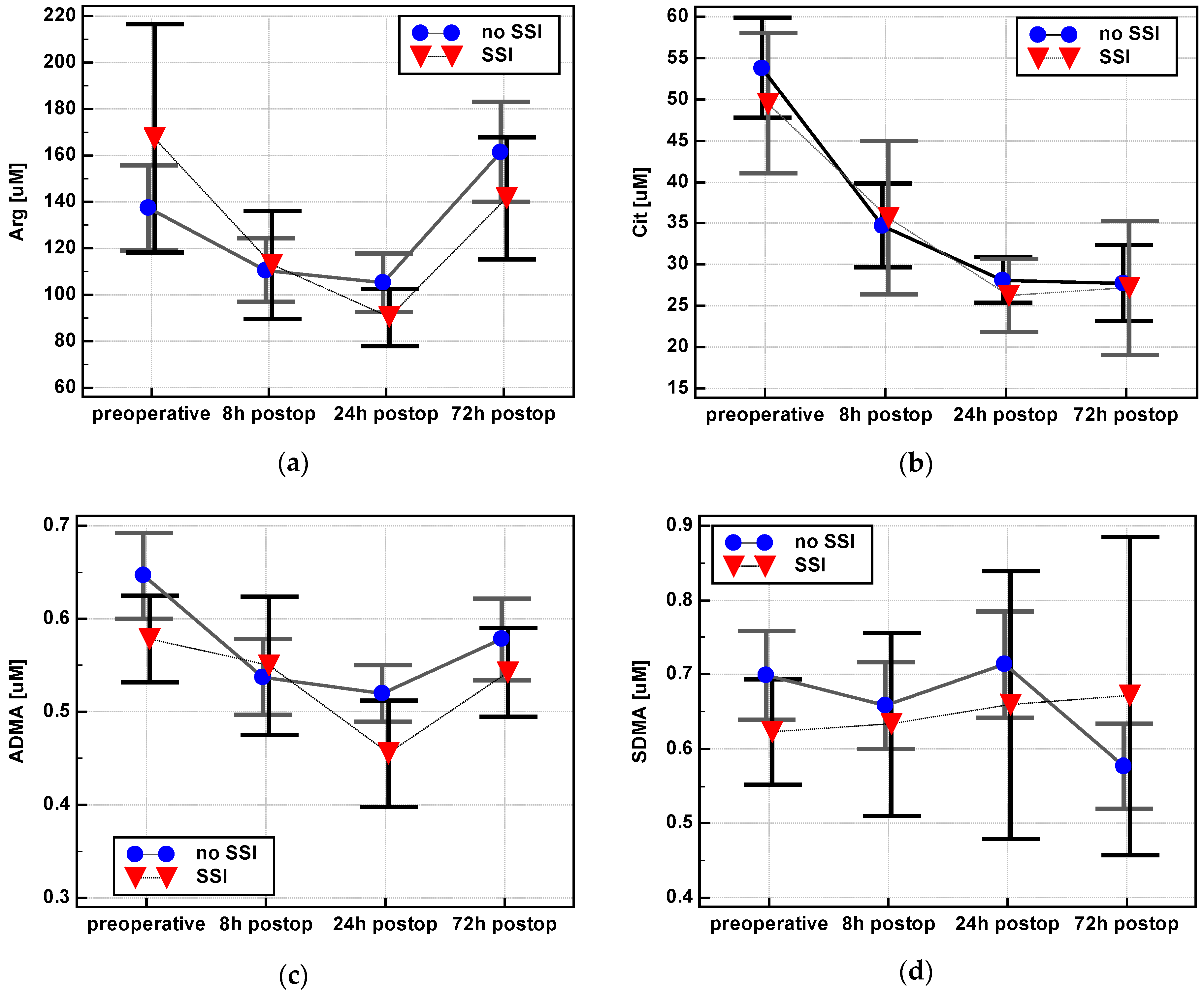
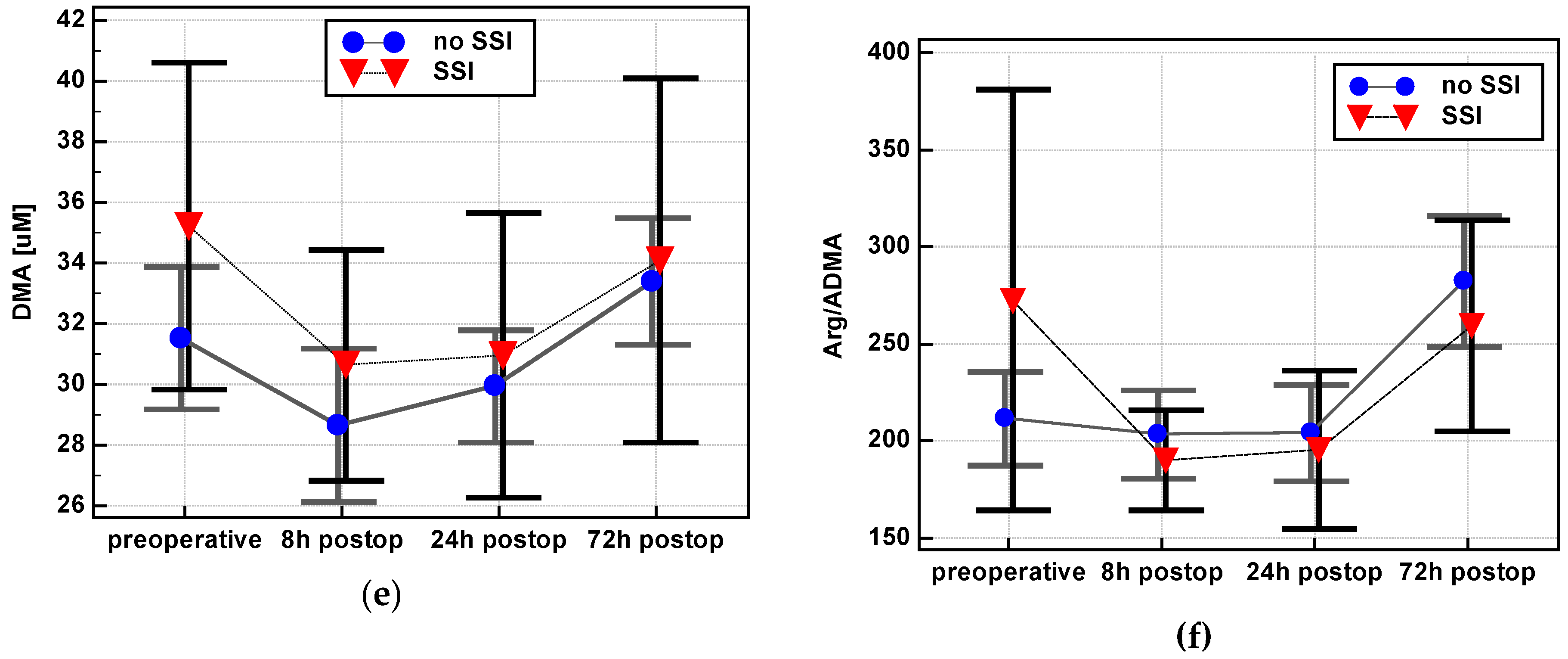
44], arginine in our study dropped directly after surgery but increased on postoperative day three. In our cohort, although ADMA displayed a similar trend to arginine, citrulline was decreasing during the whole observation period. As citrulline is considered a marker of gut functionality [
45,
46], its depletion in the early postoperative period, likely resulting from bowel manipulation and ileus, is to be expected. An interesting observation is that SDMA displayed an inverse pattern to ADMA. Both dimethylarginines are derived from proteins methylated by a group of protein arginine methyltransferases (PRMTs), of which type I enzymes yield ADMA and type II enzymes SDMA [
47]. The pool of dimethylarginines is regulated by the rate of their synthesis as well as degradation, which includes renal excretion and enzymatic degradation to citrulline and DMA in the case of ADMA but solely renal excretion in the case of SDMA [
11]. The anesthesia during surgery, blood loss, surgery-induced increase in aldosterone and antidiuretic hormone, and electrolyte imbalance associated with bowel manipulation and postoperative ileus may impair the renal function [
48,
49]. It is possible that such altered filtration in the early postoperative period hampers SDMA excretion, leading to metabolite accumulation in the blood. Acute kidney injury (AKI) is a relatively common complication after colorectal surgery [
49], more so in males and patients with transfusions [
48], with which, as shown here, the SDMA increase at 24 h post incision was positively correlated. In fact, SDMA has been proposed as a marker of renal function in children with nephrotic syndrome [
50] and adults with chronic kidney disease [
51]. As demonstrated in this study, quantifying perioperative SDMA concentrations might potentially be useful in monitoring patients recovering from CRC for AKI.
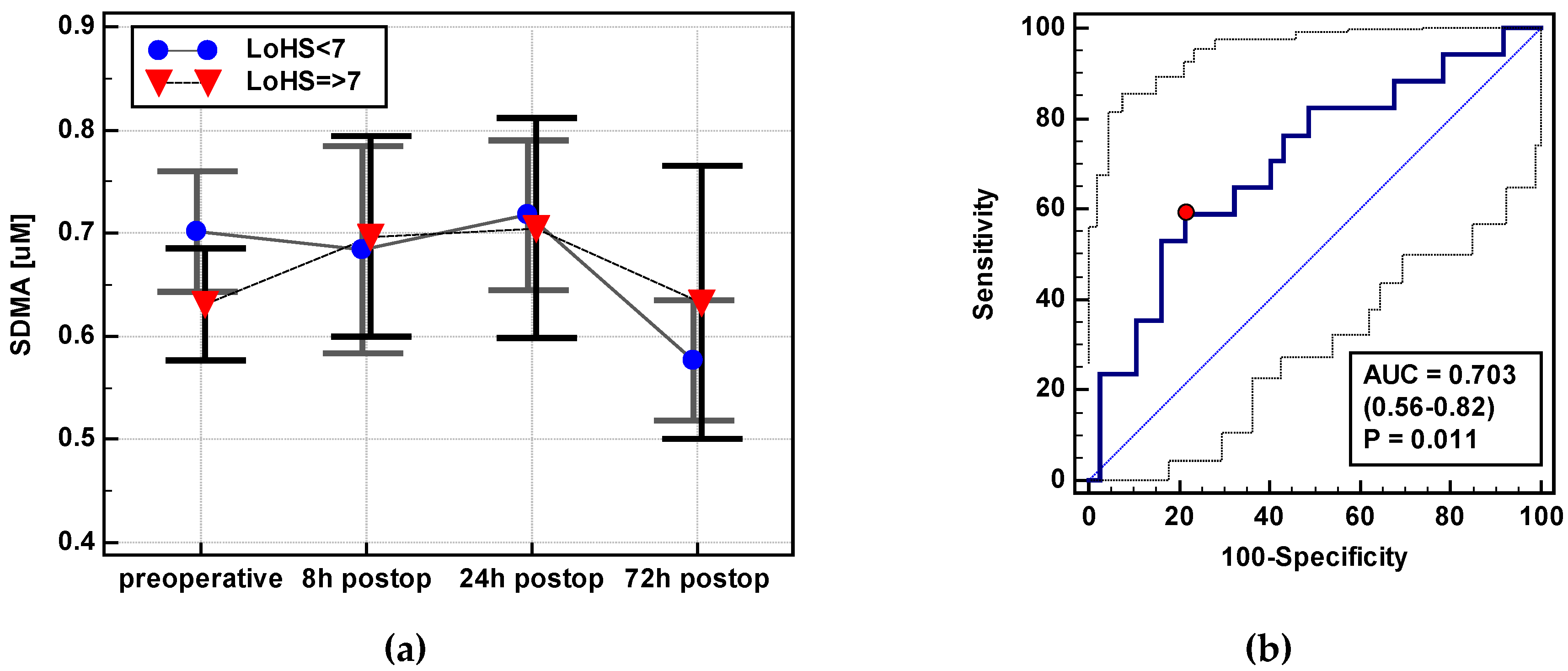
Colorectal surgery is followed by a temporary gut dysmotility, referred to as postoperative ileus. While some degree of postoperative ileus is an expected and physiological response to surgical trauma, its persistence is considered as one of the most common complications [
52]. However, there is no consensus concerning its clinical definition and timeframe. Therefore, for the purpose of this study, a restoration of bowel function was defined as tolerance of solid diet and passage of first stool. The median value in the examined cohort was calculated and median + 1 day (thus 5th postoperative day) was established as a cutoff to define the prolonged (pathological) postoperative ileus, which is in agreement with the criteria proposed by Vather et al. [
52]. The rationale behind seeking an association between perioperative alterations in the L-arginine/NO pathway and postoperative ileus is that NO synthesized by neuronal NOS is considered a main non-cholinergic and non-adrenergic inhibitory neurotransmitter in the gut, and NOS inhibitors have been shown to alleviate postoperative ileus in animal models [
53]. Correspondingly, as demonstrated here, the most potent NOS inhibitor, ADMA, was more pronouncedly decreased in the early postoperative period in patients with a delayed restoration of bowel function. The NO synthesized by inducible NOS during the inflammatory response to surgical trauma and bowel manipulation further aggravates postoperative bowel dysfunction. In line with the role attributed to inflammation in hampering bowel motility, we have previously shown the ability of early postoperative concentrations of chemokines monocyte chemoattractant protein 1 (MCP-1/CCL2) and “regulated on activation, normal T cell expressed and secreted” (RANTES/CCL5) to predict postoperative ileus [
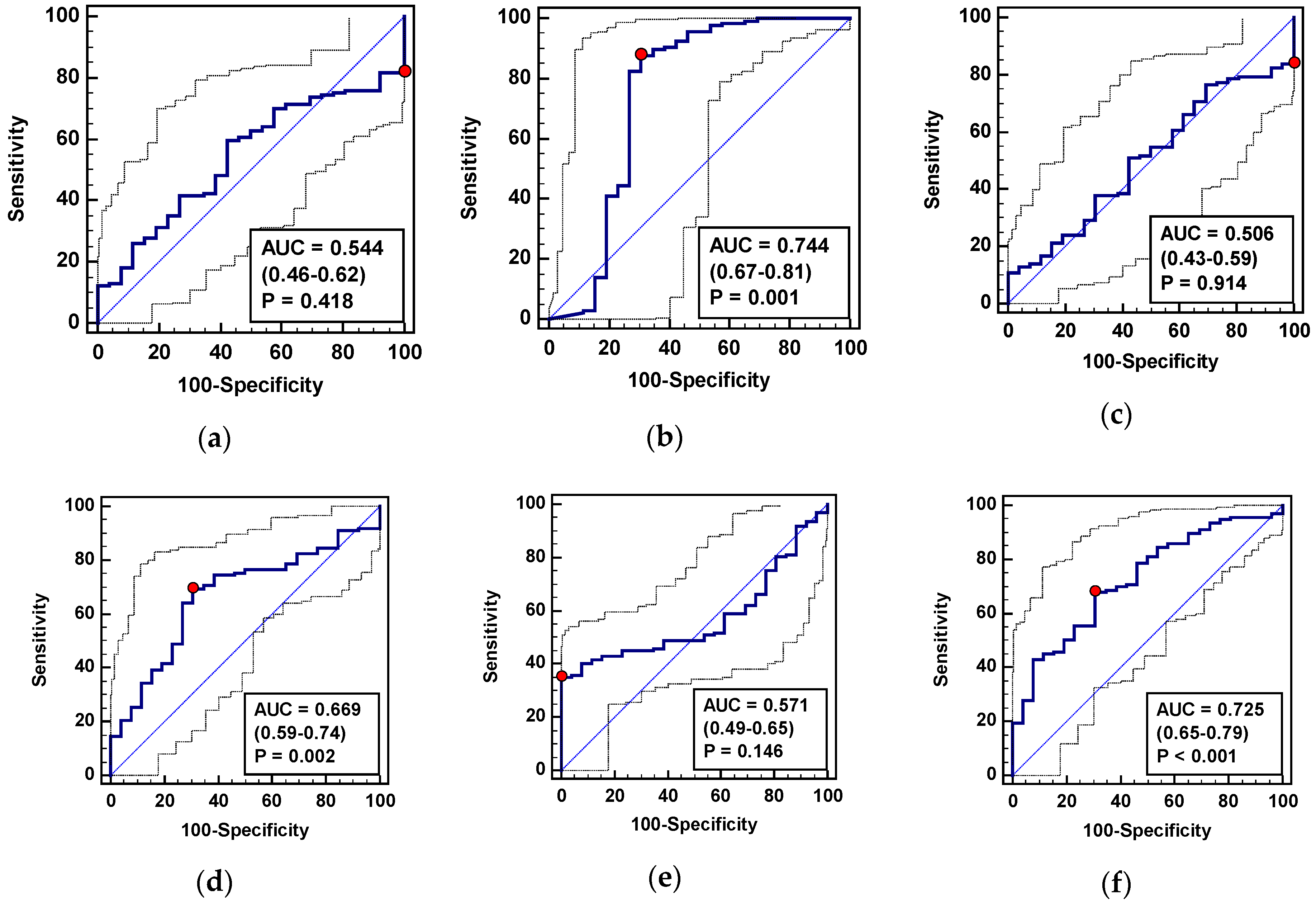
54]. Here, patients with a prolonged gut dysmotility had a higher concentration of SDMA in the early postoperative period. It may be associated with a proinflammatory character of the metabolite as, in addition to being a weak inhibitor of NOS enzymes, SDMA activates NFκB and increases monocyte expression and secretion of IL-6 and TNFα [
55]. Together, a panel consisting of arginine, ADMA, and SDMA displayed a superior performance in predicting persistent postoperative ileus over individual markers, with a satisfactory overall accuracy and specificity.
Independently from its role as a NO precursor, arginine is crucial for optimal functioning of the immune system. It stimulates T and NK cell proliferation, differentiation, and cytotoxicity. Accelerated arginine uptake by tumor cells yields T and NK cells deficient in arginine and abolishes their functioning. Moreover, the cancer-related increase in arginase-1 activity in macrophages further supports cancer growth by inducing immunosuppression [
36]. Dysfunctional immune systems might render cancer patients more susceptible to infections. Correspondingly, our patients who developed surgical site infections were those who had earlier and more markedly decreased arginine. Additionally, NO participates in creating an immunosuppressive environment by stimulating cyclooxygenase-2 and the synthesis of proinflammatory mediators [
36]. Accordingly, the NOS inhibitor, ADMA, was more pronouncedly decreased and proinflammatory SDMA was steadily increasing in patients who subsequently developed surgical site infections. A panel including all three metabolites had a very good overall accuracy and an excellent sensitivity owing to arginine and ADMA, and improved specificity as compared to individual metabolites owing to SDMA.
Anastomotic leakage is the most dreaded complication following colorectal surgery and its early indicators are sought after. Of the available biochemical markers, inflammatory indices C-reactive protein (CRP) and procalcitonin are used in the clinical practice and CRP is considered an extremely accurate biomarker of AL and thus a gold standard [
56]. From among the metabolites investigated here, an index based on ADMA dynamics displayed fair accuracy and good sensitivity and specificity as an AL marker, however, it was inferior to the literature-reported performance of CRP [
56,
57].
As operative morbidity is dependent, among others, on the patient’s age, sex, weight, and health status [
58,
59,
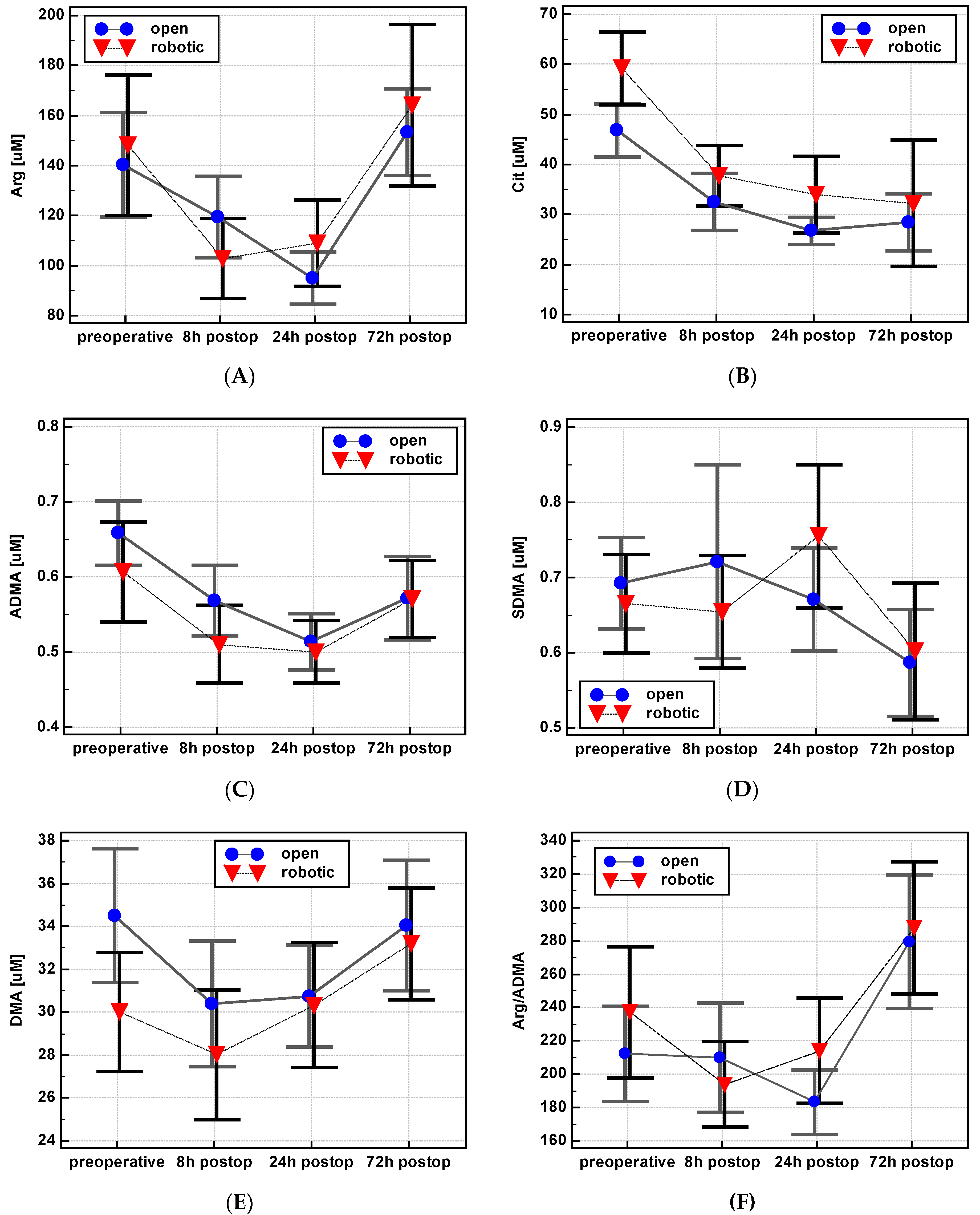
60], the potential effects of age, sex, BMI, and ASA and CCI grade on metabolite dynamics in the postoperative period were examined. None were found except for arginine and the arginine-to-ADMA ratio, which decreased directly following surgery exclusively in female patients. In addition, the type of surgery affected arginine, ADMA, and SDMA. After an initial drop, their concentration increased more markedly following minimally-invasive robot-assisted surgery. Surgical resection is the mainstay of treatment for CRC and open surgery has been the gold standard of CRC resections over the past century. However, the shift to a minimally invasive surgery in this field began in the 1990s and laparoscopy has become the surgical approach of choice for most colorectal resections. It has been shown to improve short-term outcomes, without negatively affecting oncological outcomes [
61]. Robotic surgery is believed to be the next step in this evolution. Robotic systems overcome certain limitations of laparoscopy and offer hand wristed instruments, three active working arms and a superb view of the operative field. All these factors make surgical robots the perfect tool for complex abdominal procedures [
62,
63]. Shibata et al. [
64] and our group [
54,
65,
66] have shown that robot-assisted colorectal surgery is also beneficial in terms of the inflammatory and immune response, in addition to the improvement of clinical outcomes [
67]. Still, the biochemical background of the body’s favorable response to robot-assisted surgery is poorly understood. To determine this advantage, we have compared changes in L-arginine/NO pathway metabolites following robot-assisted and classic open colorectal surgery. A slightly but significantly higher ADMA and SDMA concentration observed following the robot-assisted surgery in our study might contribute to reduced arginine availability for inducible NOS, and thus alleviate NO-associated inflammation and oxidative stress. Both dimethylarginines inhibit arginine uptake by the cationic amino acid transporter (CAT)-1 in addition to ADMA being a strong and SDMA a weak NOS inhibitor [
11]. The more prompt restoration of arginine concentration following robotic surgery observed in this study seems to be beneficial, also in light of its role as a pharmaco-nutrient. Surgery-induced deficiency in arginine contributes to the disadvantageous immune shift towards Th2 response and postoperative immunosuppression [
68]. These findings add to the existing literature, fostering a better understanding of the immune and inflammatory response that follows minimally invasive surgery.
In addition to the type of surgery, early postoperative dynamics of arginine and ADMA concentration were affected by the degree of blood loss. In particular, a metabolite drop at 24 h as compared to 8 h was more pronounced (thus yielding smaller Δ
24/8 values) in patients with an estimated blood loss (EBL). This finding is consistent with the known causative effect of adverse circulatory conditions, including hemorrhage, on the dysfunction of endothelial cells [
69]. Dysfunctional endothelium is characterized by a reduced NO synthesis by endothelial isoforms of NOS and a low-grade inflammation, conditions aggravated by decreased arginine availability. Accordingly, a restorative effect on endothelium has been attributed to L-arginine supplementation [
69]. In turn, the lower the initial drop was in arginine, the higher the EBL. While counterintuitive, it may be the effect of interference by confounding factors at play during surgery. As an example, some of our patients were introduced to perioperative warming, a procedure reportedly associated with reduced intraoperative blood loss, since amino acids have been shown to induce a thermogenic response and counteract surgery-associated hypothermia [
70]. Accordingly, a drop in arginine after 8 and 24 h post incision was lower, and the Arg/ADMA ratio even increased at 24 h in patients subjected to perioperative warming.

 ,
, 


















{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}