Self-Rated Health in Migrant and Non-Migrant Women before, during and after Pregnancy: A Population-Based Study of 0.5 Million Pregnancies from the Swedish Pregnancy Register

 , , , , ,
, , , , ,  and
and
Abstract
1. Introduction
2. Methods
2.1. Study Design
2.2. Study Variables
2.3. Statistical Analysis
3. Results
3.1. Descriptive Data
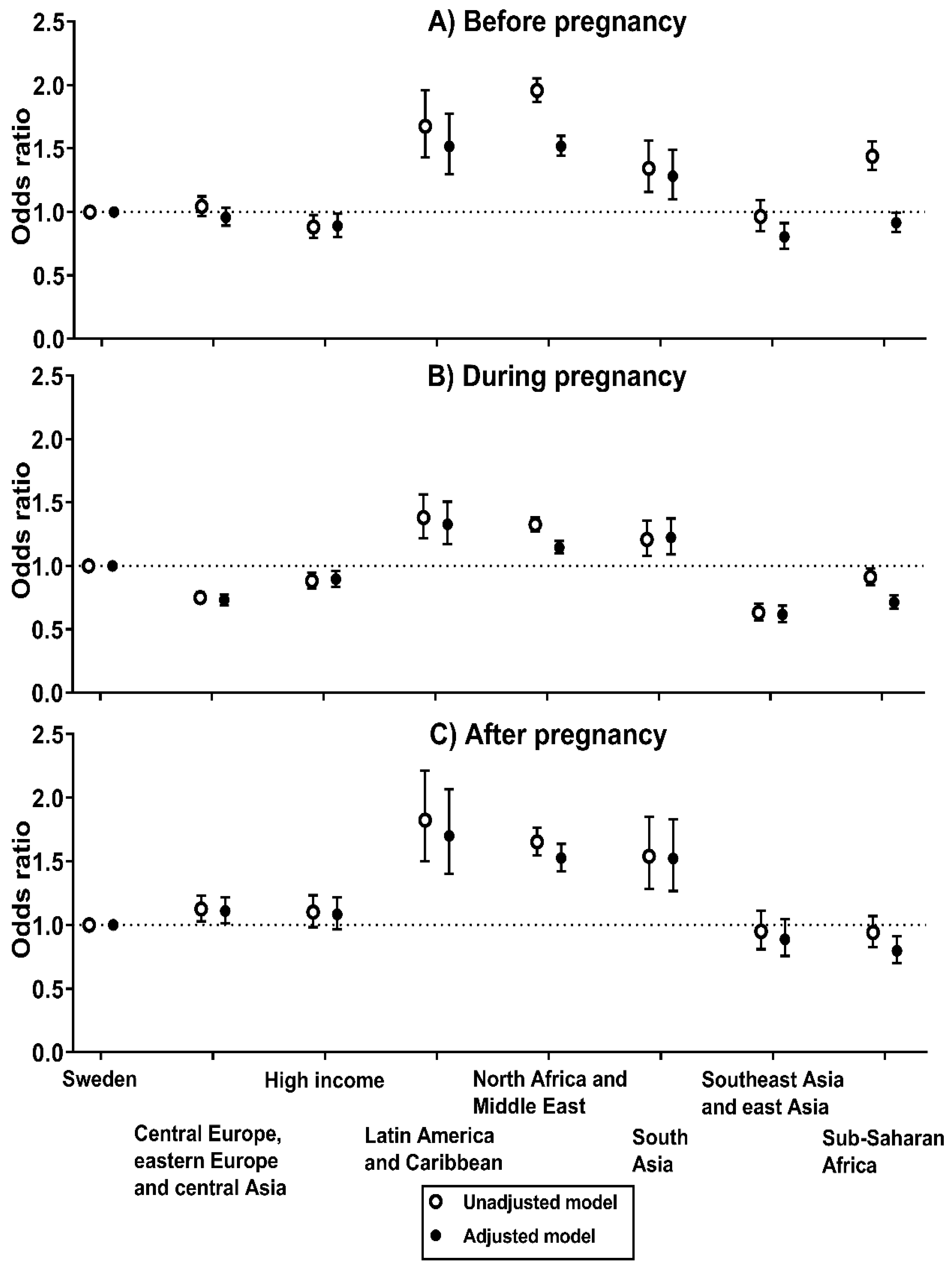
3.2. Odds of Poor Self-Rated Health before Pregnancy
3.3. Odds of Poor Self-Rated Health during Pregnancy
3.4. Odds of Poor Self-Rated Health after Pregnancy
3.5. Sensitivity Analyses
4. Discussion
4.1. Main Findings
4.2. Interpretation
4.3. Strengths and Limitations
4.4. Clinical and Public Health Implications
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- DeSalvo, K.B.; Bloser, N.; Reynolds, K.; He, J.; Muntner, P. Mortality prediction with a single general self-rated health question. A meta-analysis. J. Gen. Intern. Med. 2006, 21, 267–275. [Google Scholar] [CrossRef]
- Ganna, A.; Ingelsson, E. 5 year mortality predictors in 498,103 UK Biobank participants: A prospective population-based study. Lancet 2015, 386, 533–540. [Google Scholar] [CrossRef]
- Mavaddat, N.; Parker, R.A.; Sanderson, S.; Mant, J.; Kinmonth, A.L. Relationship of self-rated health with fatal and non-fatal outcomes in cardiovascular disease: A systematic review and meta-analysis. PLoS ONE 2014, 9, e103509. [Google Scholar] [CrossRef] [PubMed]
- Vie, T.L.; Hufthammer, K.O.; Meland, E.; Breidablik, H.J. Self-rated health (SRH) in young people and causes of death and mortality in young adulthood. A prospective registry-based Norwegian HUNT-study. SSM Popul. Health 2019, 7, 100364. [Google Scholar] [CrossRef] [PubMed]
- Zulkifly, H.H.; Clavarino, A.; Kassab, Y.W.; Dingle, K. The association between perception of health during pregnancy and the risk of cardiovascular disease: A prospective study. SpringerPlus. 2016, 5, 6. [Google Scholar] [CrossRef]
- Ambresin, G.; Chondros, P.; Dowrick, C.; Herrman, H.; Gunn, J.M. Self-rated health and long-term prognosis of depression. Ann. Fam. Med. 2014, 12, 57–65. [Google Scholar] [CrossRef]
- Stepanikova, I.; Kukla, L.; Svancara, J. Predictive value of self-rated health in pregnancy for childbirth complications, adverse birth outcomes, and maternal health. Int. J. Gynaecol. Obstet. 2016, 135, 56–60. [Google Scholar] [CrossRef]
- El-Khoury, F.; Sutter-Dallay, A.L.; Panico, L.; Charles, M.A.; Azria, E.; Van der Waerden, J.; Melchior, M. Women’s mental health in the perinatal period according to migrant status: The French representative ELFE birth cohort. Eur. J. Public Health 2018, 28, 458–463. [Google Scholar] [CrossRef]
- La Parra-Casado, D.; Stornes, P.; Solheim, E.F. Self-rated health and wellbeing among the working-age immigrant population in Western Europe: Findings from the European social survey (2014) special module on the social determinants of health. Eur. J. Public Health 2017, 27, 40–46. [Google Scholar] [CrossRef]
- Liu, C.; Ahlberg, M.; Hjern, A.; Stephansson, O. Perinatal health of refugee and asylum-seeking women in Sweden 2014-17: A register-based cohort study. Eur. J. Public Health 2019, 29, 1048–1055. [Google Scholar] [CrossRef]
- Nielsen, S.S.; Krasnik, A. Poorer self-perceived health among migrants and ethnic minorities versus the majority population in Europe: A systematic review. Int. J. Public Health 2010, 55, 357–371. [Google Scholar] [CrossRef] [PubMed]
- Abubakar, I.; Aldridge, R.W.; Devakumar, D.; Orcutt, M.; Burns, R.; Barreto, M.L.; Dhavan, P.; Fouad, F.M.; Groce, N.; Guo, Y.; et al. The UCL-Lancet Commission on Migration and Health: The health of a world on the move. Lancet 2018, 392, 2606–2654. [Google Scholar] [CrossRef]
- Rechel, B.; Mladovsky, P.; Ingleby, D.; Mackenbach, J.P.; McKee, M. Migration and health in an increasingly diverse Europe. Lancet 2013, 381, 1235–1245. [Google Scholar] [CrossRef]
- Schytt, E.; Hildingsson, I. Physical and emotional self-rated health among Swedish women and men during pregnancy and the first year of parenthood. Sex. Reprod. Healthc. 2011, 2, 57–64. [Google Scholar] [CrossRef]
- Becker, M.; Weinberger, T.; Chandy, A.; Schmukler, S. Depression during Pregnancy and Postpartum. Curr. Psychiatry Rep. 2016, 18, 32. [Google Scholar] [CrossRef]
- Gon, G.; Leite, A.; Calvert, C.; Woodd, S.; Graham, W.J.; Filippi, V. The frequency of maternal morbidity: A systematic review of systematic reviews. Int. J. Gynaecol. 2018, 141, 20–38. [Google Scholar] [CrossRef]
- Narayan, B.; Nelson-Piercy, C. Medical problems in pregnancy. Clin. Med. 2017, 17, 251. [Google Scholar] [CrossRef]
- Murray, C.J.; Callender, C.S.; Kulikoff, X.R.; Srinivasan, V.; Abate, D.; Abate, K.H.; Abay, S.M.; Abbasi, N.; Abbastabar, H.; Abdela, J.; et al. GBD 2017 Population and Fertility collaborators. Population and fertility by age and sex for 195 countries and territories, 1950–2017: A systematic analysis for the Global Burden of Disease Study 2017. Lancet 2018, 392, 1995–2051. [Google Scholar] [CrossRef]
- Stephansson, O.; Petersson, K.; Bjork, C.; Conner, P.; Wikstrom, A.K. The Swedish Pregnancy Register—For quality of care improvement and research. Acta Obstet. Gynecol. Scand. 2018, 97, 466–476. [Google Scholar] [CrossRef]
- Mohseni, M.; Lindstrom, M. Ethnic differences in anticipated discrimination, generalised trust in other people and self-rated health: A population-based study in Sweden. Ethn. Health 2008, 13, 417–434. [Google Scholar] [CrossRef]
- Bennet, L.; Lindstrom, M. Self-rated health and social capital in Iraqi immigrants to Sweden: The MEDIM population-based study. Scand. J. Public Health 2018, 46, 194–203. [Google Scholar] [CrossRef] [PubMed]
- Dinesen, C.; Nielsen, S.S.; Mortensen, L.H.; Krasnik, A. Inequality in self-rated health among immigrants, their descendants and ethnic Danes: Examining the role of socioeconomic position. Int. J. Public Health 2011, 56, 503–514. [Google Scholar] [CrossRef] [PubMed]
- Wiking, E.; Johansson, S.E.; Sundquist, J. Ethnicity, acculturation, and self reported health. A population based study among immigrants from Poland, Turkey, and Iran in Sweden. J. Epidemiol. Community Health 2004, 58, 574–582. [Google Scholar] [CrossRef] [PubMed]
- Rowland, G. Does the Provision of a Native Language Maternity Information DVD for Non-English-Speaking Somali Women Improve their Knowledge of Maternity Care in a Manner That They Find Acceptable and Useful? Ph.D. Thesis, University of Southampton, Faculty of Health Sciences, Southampton, UK, January 2016. [Google Scholar]
- Herrel, N.; Olevitch, L.; DuBois, D.K.; Terry, P.; Thorp, D.; Kind, E.; Said, A. Somali refugee women speak out about their needs for care during pregnancy and delivery. J. Midwifery Women Health 2004, 49, 345–349. [Google Scholar] [CrossRef]
- Wiklund, H.; Aden, A.S.; Hogberg, U.; Wikman, M.; Dahlgren, L. Somalis giving birth in Sweden: A challenge to culture and gender specific values and behaviours. Midwifery 2000, 16, 105–115. [Google Scholar] [CrossRef]
- Allen, C.D.; McNeely, C.A.; Orme, J.G. Self-Rated Health Across Race, Ethnicity, and Immigration Status for US Adolescents and Young Adults. J. Adolesc. Health 2016, 58, 47–56. [Google Scholar] [CrossRef]
- Chandola, T.; Jenkinson, C. Validating self-rated health in different ethnic groups. Ethn. Health 2000, 5, 151–159. [Google Scholar] [CrossRef]
- Erdem, O.; Riva, E.; Prins, R.G.; Burdorf, A.; van der Doef, M. Health-related behaviours mediate the relation between ethnicity and (mental) health in the Netherlands. Ethn. Health 2019, 24, 287–300. [Google Scholar] [CrossRef]
- Rodriguez-Alvarez, E.; Gonzalez-Rabago, Y.; Borrell, L.N.; Lanborena, N. Perceived discrimination and self-rated health in the immigrant population of the Basque Country, Spain. Gac. Sanit. 2017, 31, 390–395. [Google Scholar] [CrossRef]
- Salinero-Fort, M.Á.; del Otero-Sanz, L.; Martín-Madrazo, C.; de Burgos-Lunar, C.; Chico-Moraleja, R.M.; Rodés-Soldevila, B.; Jiménez-García, R.; Gómez-Campelo, P. The relationship between social support and self-reported health status in immigrants: An adjusted analysis in the Madrid Cross Sectional Study. BMC Fam. Pract. 2011, 12, 46. [Google Scholar] [CrossRef]
- Malmusi, D. Immigrants’ health and health inequality by type of integration policies in European countries. Eur. J. Public Health 2015, 25, 293–299. [Google Scholar] [CrossRef] [PubMed]
- Moullan, Y.; Jusot, F. Why is the ‘healthy immigrant effect’ different between European countries? Eur. J. Public Health 2014, 24, 80–86. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Characteristics | Sweden | Central Europe, Eastern Europe and Central Asia 1 | High Income Countries 2 | Latin America and the Caribbean 3 | North Africa and the Middle East 4 | South Asia 5 | Southeast Asia and East Asia 6 | Sub-Saharan Africa 7 |
|---|---|---|---|---|---|---|---|---|
| n (%) | 456,045 | 28,180 | 16,308 | 3732 | 40,172 | 4948 | 9877 | 18,503 |
| (78.9%) | (4.9%) | (2.8%) | (0.6%) | (7.0%) | (0.9%) | (1.7%) | (3.2%) | |
| Age (years) | 30.7 ± 5.0 | 30.6 ± 5.2 | 32.7 ± 5.0 | 32.2 ± 5.3 | 30.1 ± 4.5 | 30.5 ± 4.5 | 32.1 ± 5.1 | 30.3 ± 5.7 |
| Primiparous | 45.1% | 43.3% | 44.6% | 43.6% | 35.1% | 47.5% | 44.8% | 29.5% |
| Educational attainment | ||||||||
| No or elementary school | 4.4% | 13.3% | 4.6% | 9.4% | 29.1% | 12.4% | 24.4% | 50.9% |
| High school | 41.1% | 41.5% | 25.5% | 41.7% | 37.9% | 28.9% | 36.2% | 35.2% |
| University | 54.5% | 45.2% | 69.9% | 48.8% | 33.0% | 58.7% | 39.4% | 13.8% |
| BMI (kg/m2) | 24.8 ± 4.7 | 24.2 ± 4.4 | 24.5 ± 4.7 | 25.2 ± 4.4 | 25.7 ± 4.6 | 24.8 ± 4.4 | 22.8 ± 3.8 | 26.1 ± 5.3 |
| Poor self-reported health | ||||||||
| Before pregnancy | 2.7% | 2.8% | 2.4% | 4.4% | 5.1% | 3.6% | 2.6% | 3.8% |
| During pregnancy 8 | 8.6% | 6.6% | 7.7% | 11.5% | 11.1% | 10.2% | 5.6% | 7.9% |
| After pregnancy 9 | 2.5% | 2.8% | 2.7% | 4.4% | 4.0% | 3.8% | 2.3% | 2.3% |
- Data is presented as the mean ± standard deviation or as %. BMI, body mass index.
- 1 Included regions/countries were: Central Asia (Armenia, Azerbaijan, Georgia, Kazakhstan, Kyrgyzstan, Mongolia, Tajikistan, Turkmenistan and Uzbekistan); Central Europe (Albania, Bosnia and Herzegovina, Bulgaria, Croatia, Czech Republic, Hungary, Macedonia, Montenegro, Poland, Romania, Serbia, Slovakia and Slovenia); Eastern Europe (Belarus, Estonia, Latvia, Lithuania, Moldova, Russia and Ukraine).
- 2 Included countries were: Australasia (Australia and New Zealand); high-income Asia Pacific (Brunei, Japan, Singapore and South Korea); high-income North America (Canada, Greenland and USA); Southern Latin America (Argentina, Chile and Uruguay); Western Europe (Andorra, Austria, Belgium, Cyprus, Denmark, Finland, France, Germany, Greece, Iceland, Ireland, Israel, Italy, Luxembourg, Malta, Netherlands, Norway, Portugal, Spain, Switzerland and UK).
- 3 Included regions/countries were: Andean Latin America (Bolivia, Ecuador, Peru); the Caribbean (Antigua and Barbuda, The Bahamas, Barbados, Belize, Bermuda, Cuba, Dominica, Dominican Republic, Grenada, Guyana, Haiti, Jamaica, Puerto Rico, Saint Lucia, Saint Vincent and the Grenadines, Suriname, Trinidad and Tobago and Virgin Islands); Central Latin America (Colombia, Costa Rica, El Salvador, Guatemala, Honduras, Mexico, Nicaragua, Panama and Venezuela); Tropical Latin America (Brazil and Paraguay).
- 4 Included regions/countries were: Afghanistan, Algeria, Bahrain, Egypt, Iran, Iraq, Jordan, Kuwait, Lebanon, Libya, Morocco, Oman, Palestine, Qatar, Saudi Arabia, Sudan, Syria, Tunisia, Turkey, United Arab Emirates and Yemen.
- 5 Included regions/countries were: Bangladesh, Bhutan, India, Nepal and Pakistan.
- 6 Included regions/countries were: East Asia (China, North Korea and Taiwan (province of China)); Southeast Asia (Cambodia, Indonesia, Laos, Malaysia, Maldives, Mauritius, Myanmar, Philippines, Sri Lanka, Seychelles, Thailand, Timor-Leste and Vietnam). Oceania was not included due too few observations.
- 7 Included regions/countries were: Central Sub-Saharan Africa (Angola, Central African Republic, Democratic Republic of the Congo, Equatorial Guinea and Gabon); Eastern Sub-Saharan Africa (Burundi, Comoros, Djibouti, Eritrea, Ethiopia, Kenya, Madagascar, Malawi, Mozambique, Rwanda, Somalia, South Sudan, Tanzania, Uganda and Zambia); Southern Sub-Saharan Africa (Botswana, Lesotho, Namibia, South Africa, Swaziland (eSwatini) and Zimbabwe); Western Sub-Saharan Africa (Benin, Burkina Faso, Cameroon, Cape Verde, Chad, Côte d’Ivoire, The Gambia, Ghana, Guinea, Guinea-Bissau, Liberia, Mali, Mauritania, Niger, Nigeria, São Tomé and Príncipe, Senegal, Sierra Leone and Togo).
- 8 Number of pregnancies with data on self-reported health during pregnancy were; Sweden (n = 354,242); Central Europe, Eastern Europe and Central Asia (n = 18,859); high income countries (n = 11,652), Latin America and the Caribbean (n = 2456), North Africa and the Middle East (n = 25,257), South Asia (n = 3206), Southeast Asia and East Asia (n = 6830), Sub-Saharan Africa (n = 10,746).
- 9 Number of pregnancies with data self-reported health after pregnancy were; Sweden (n = 347,562), Central Europe, Eastern Europe and Central Asia (n = 18,783), high income countries (n = 11,587), Latin America and the Caribbean (n = 2448), North Africa and the Middle East (n = 25,253), South Asia (n = 3200), Southeast Asia and East Asia (n = 6812), Sub-Saharan Africa (n = 10,779).
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Henriksson, P.; Söderström, E.; Blomberg, M.; Nowicka, P.; Petersson, K.; Thomas, K.; Bendtsen, M.; Estévez-López, F.; Löf, M. Self-Rated Health in Migrant and Non-Migrant Women before, during and after Pregnancy: A Population-Based Study of 0.5 Million Pregnancies from the Swedish Pregnancy Register. J. Clin. Med. 2020, 9, 1764. https://doi.org/10.3390/jcm9061764
Henriksson P, Söderström E, Blomberg M, Nowicka P, Petersson K, Thomas K, Bendtsen M, Estévez-López F, Löf M. Self-Rated Health in Migrant and Non-Migrant Women before, during and after Pregnancy: A Population-Based Study of 0.5 Million Pregnancies from the Swedish Pregnancy Register. Journal of Clinical Medicine. 2020; 9(6):1764. https://doi.org/10.3390/jcm9061764
Chicago/Turabian StyleHenriksson, Pontus, Emmie Söderström, Marie Blomberg, Paulina Nowicka, Kerstin Petersson, Kristin Thomas, Marcus Bendtsen, Fernando Estévez-López, and Marie Löf. 2020. "Self-Rated Health in Migrant and Non-Migrant Women before, during and after Pregnancy: A Population-Based Study of 0.5 Million Pregnancies from the Swedish Pregnancy Register" Journal of Clinical Medicine 9, no. 6: 1764. https://doi.org/10.3390/jcm9061764
APA StyleHenriksson, P., Söderström, E., Blomberg, M., Nowicka, P., Petersson, K., Thomas, K., Bendtsen, M., Estévez-López, F., & Löf, M. (2020). Self-Rated Health in Migrant and Non-Migrant Women before, during and after Pregnancy: A Population-Based Study of 0.5 Million Pregnancies from the Swedish Pregnancy Register. Journal of Clinical Medicine, 9(6), 1764. https://doi.org/10.3390/jcm9061764