Outcomes of Chronic Phase Chronic Myeloid Leukemia after Treatment with Multiple Tyrosine Kinase Inhibitors

 ,
, 
Abstract
1. Introduction
2. Materials and Methods
Statistical Analysis
3. Results
3.1. Patients’ Characteristics
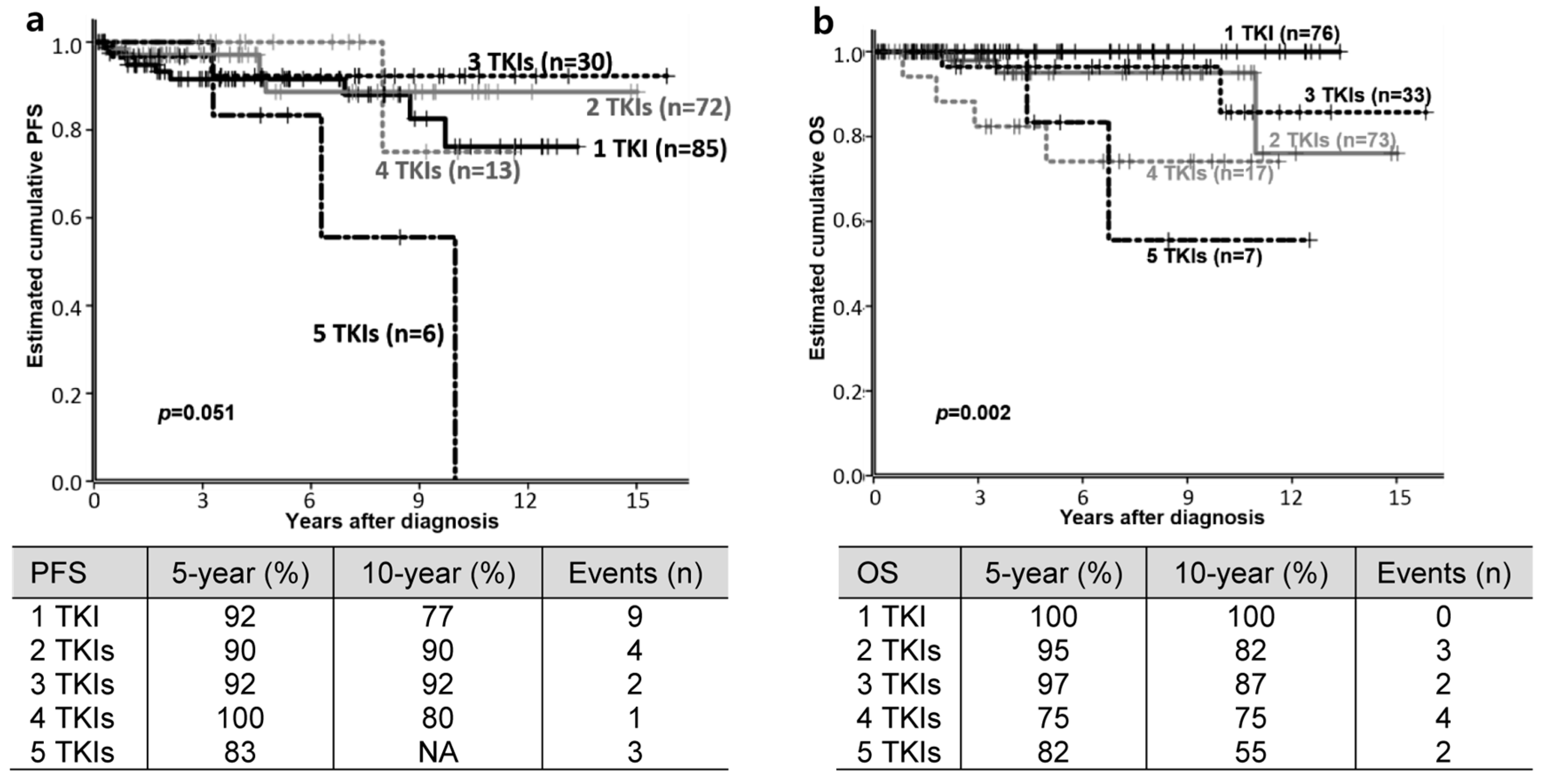
3.2. Clinical Outcomes
3.3. Outcomes According to First-Line TKI: IM vs. NG-TKI
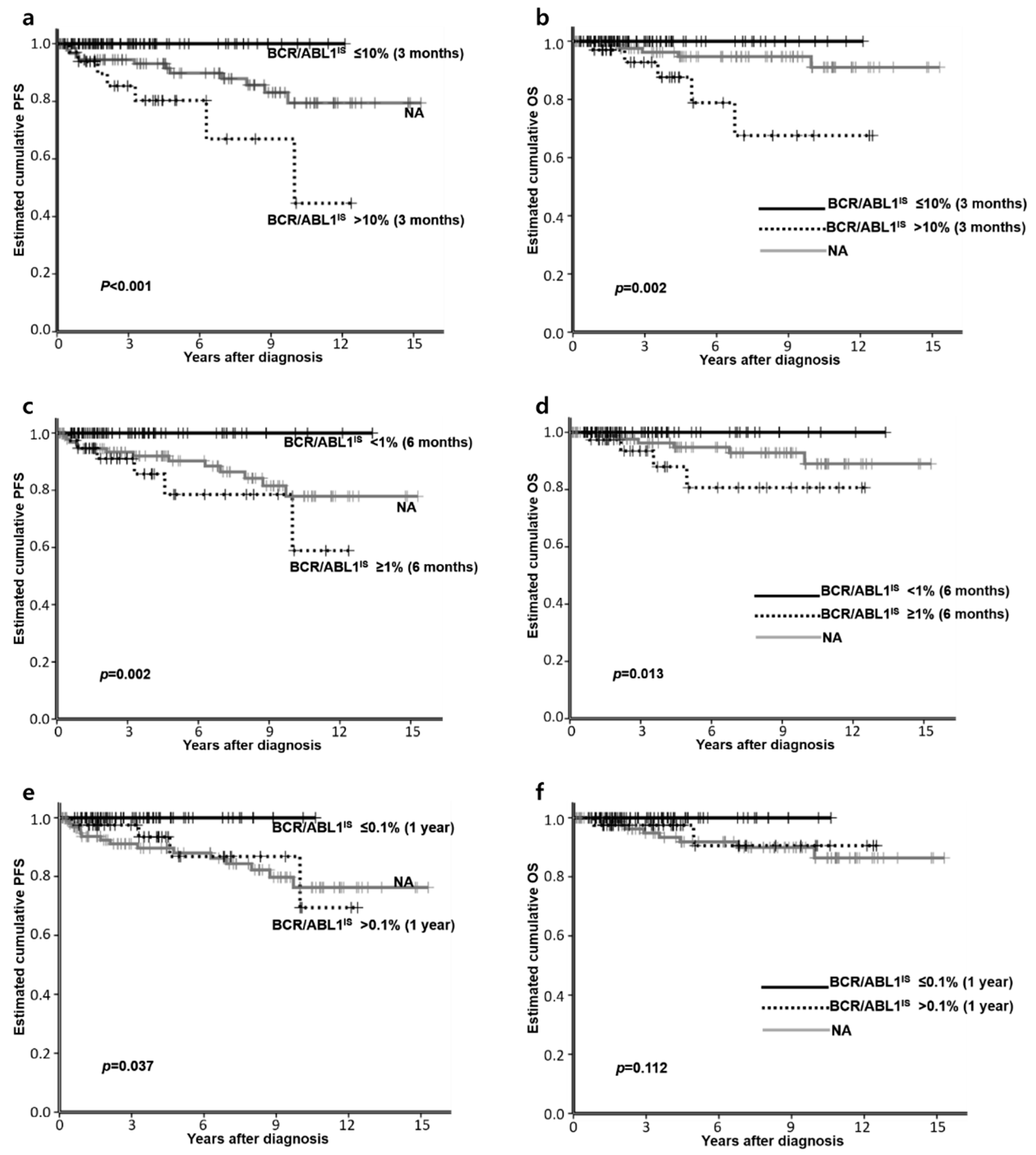
3.4. Factors Affecting PFS or OS
3.5. TKI Discontinuation
4. Discussion
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Faderl, S.; Talpaz, M.; Estrov, Z.; O’Brien, S.; Kurzrock, R.; Kantarjian, H.M. The biology of chronic myeloid leukemia. N. Engl. J. Med. 1999, 341, 164–172. [Google Scholar] [CrossRef]
- Bower, H.; Bjorkholm, M.; Dickman, P.W.; Hoglund, M.; Lambert, P.C.; Andersson, T.M. Life expectancy of patients with chronic myeloid leukemia approaches the life expectancy of the general population. J. Clin. Oncol. 2016, 34, 2851–2857. [Google Scholar] [CrossRef] [PubMed]
- Haznedaroglu, I.C. Current concerns of undertreatment and overtreatment in chronic myeloid leukemia based on european leukemianet 2013 recommendations. Expert Opin. Pharmacother. 2013, 14, 2005–2010. [Google Scholar] [CrossRef][Green Version]
- Cortes, J.E.; Kim, D.W.; Pinilla-Ibarz, J.; le Coutre, P.; Paquette, R.; Chuah, C.; Nicolini, F.E.; Apperley, J.F.; Khoury, H.J.; Talpaz, M.; et al. A phase 2 trial of ponatinib in philadelphia chromosome-positive leukemias. N. Engl. J. Med. 2013, 369, 1783–1796. [Google Scholar] [CrossRef] [PubMed]
- Russo Rossi, A.; Breccia, M.; Abruzzese, E.; Castagnetti, F.; Luciano, L.; Gozzini, A.; Annunziata, M.; Martino, B.; Stagno, F.; Cavazzini, F.; et al. Outcome of 82 chronic myeloid leukemia patients treated with nilotinib or dasatinib after failure of two prior tyrosine kinase inhibitors. Haematologica 2013, 98, 399–403. [Google Scholar] [CrossRef] [PubMed]
- Klamova, H.; Faber, E.; Zackova, D.; Markova, M.; Voglova, J.; Cmunt, E.; Novakova, L.; Machova-Polakova, K.; Moravcova, J.; Dvorakova, D.; et al. Dasatinib in imatinib-resistant or -intolerant cml patients: Data from the clinical practice of 6 hematological centers in the czech republic. Neoplasma 2010, 57, 355–359. [Google Scholar]
- Ongoren, S.; Eskazan, A.E.; Suzan, V.; Savci, S.; Erdogan Ozunal, I.; Berk, S.; Yalniz, F.F.; Elverdi, T.; Salihoglu, A.; Erbilgin, Y.; et al. Third-line treatment with second-generation tyrosine kinase inhibitors (dasatinib or nilotinib) in patients with chronic myeloid leukemia after two prior tkis: Real-life data on a single center experience along with the review of the literature. Hematol. Am. Soc. Hematol. Educ. Program 2017, 1–9. [Google Scholar] [CrossRef]
- Shah, N.P.; Rousselot, P.; Schiffer, C.; Rea, D.; Cortes, J.E.; Milone, J.; Mohamed, H.; Healey, D.; Kantarjian, H.; Hochhaus, A.; et al. Dasatinib in imatinib-resistant or -intolerant chronic-phase, chronic myeloid leukemia patients: 7-year follow-up of study ca180-034. Am. J. Hematol. 2016, 91, 869–874. [Google Scholar] [CrossRef]
- Eghtedar, A.; Kantarjian, H.; Jabbour, E.; O’Brien, S.; Burton, E.; Garcia-Manero, G.; Verstovsek, S.; Ravandi, F.; Borthakur, G.; Konopleva, M.; et al. Outcome after failure of second generation tyrosine kinase inhibitors treatment as first-line therapy for patients with chronic myeloid leukemia. Clin. Lymphoma Myeloma Leuk. 2013, 13, 477–484. [Google Scholar] [CrossRef]
- Garg, R.J.; Kantarjian, H.; O’Brien, S.; Quintás-Cardama, A.; Faderl, S.; Estrov, Z.; Cortes, J. The use of nilotinib or dasatinib after failure to 2 prior tyrosine kinase inhibitors: Long-term follow-up. Blood 2009, 114, 4361–4368. [Google Scholar] [CrossRef]
- Giles, F.J.; Abruzzese, E.; Rosti, G.; Kim, D.W.; Bhatia, R.; Bosly, A.; Goldberg, S.; Kam, G.L.; Jagasia, M.; Mendrek, W.; et al. Nilotinib is active in chronic and accelerated phase chronic myeloid leukemia following failure of imatinib and dasatinib therapy. Leukemia 2010, 24, 1299–1301. [Google Scholar] [CrossRef] [PubMed]
- Giles, F.J.; le Coutre, P.D.; Pinilla-Ibarz, J.; Larson, R.A.; Gattermann, N.; Ottmann, O.G.; Hochhaus, A.; Radich, J.P.; Saglio, G.; Hughes, T.P.; et al. Nilotinib in imatinib-resistant or imatinib-intolerant patients with chronic myeloid leukemia in chronic phase: 48-month follow-up results of a phase ii study. Leukemia 2013, 27, 107–112. [Google Scholar] [CrossRef] [PubMed]
- Brummendorf, T.H.; Cortes, J.E.; Khoury, H.J.; Kantarjian, H.M.; Kim, D.W.; Schafhausen, P.; Conlan, M.G.; Shapiro, M.; Turnbull, K.; Leip, E.; et al. Factors influencing long-term efficacy and tolerability of bosutinib in chronic phase chronic myeloid leukaemia resistant or intolerant to imatinib. Br. J. Haematol. 2016, 172, 97–110. [Google Scholar] [CrossRef] [PubMed]
- Cortes, J.E.; Khoury, H.J.; Kantarjian, H.M.; Lipton, J.H.; Kim, D.W.; Schafhausen, P.; Matczak, E.; Leip, E.; Noonan, K.; Brummendorf, T.H.; et al. Long-term bosutinib for chronic phase chronic myeloid leukemia after failure of imatinib plus dasatinib and/or nilotinib. Am. J. Hematol. 2016, 91, 1206–1214. [Google Scholar] [CrossRef]
- Hochhaus, A.; Baccarani, M.; Silver, R.T.; Schiffer, C.; Apperley, J.F.; Cervantes, F.; Clark, R.E.; Cortes, J.E.; Deininger, M.W.; Guilhot, F.; et al. European leukemianet 2020 recommendations for treating chronic myeloid leukemia. Leukemia 2020, 34, 966–984. [Google Scholar] [CrossRef]
- Swerdlow, S.H.; Campo, E.; Harris, N.L.; Jaffe, E.S.; Pileri, S.A.; Stein, H.; Thiele, J.; Vardiman, J.W. The World Health Organization (Who) Classification of Tumors of the Hematopoietic and Lymphoid Tissues, 4th ed.; IARC Press: Lyon, France, 2008. [Google Scholar]
- Baccarani, M.; Saglio, G.; Goldman, J.; Hochhaus, A.; Simonsson, B.; Appelbaum, F.; Apperley, J.; Cervantes, F.; Cortes, J.; Deininger, M.; et al. Evolving concepts in the management of chronic myeloid leukemia: Recommendations from an expert panel on behalf of the european leukemianet. Blood 2006, 108, 1809–1820. [Google Scholar] [CrossRef]
- Baccarani, M.; Deininger, M.W.; Rosti, G.; Hochhaus, A.; Soverini, S.; Apperley, J.F.; Cervantes, F.; Clark, R.E.; Cortes, J.E.; Guilhot, F.; et al. European leukemianet recommendations for the management of chronic myeloid leukemia: 2013. Blood 2013, 122, 872–884. [Google Scholar] [CrossRef]
- Hasford, J.; Baccarani, M.; Hoffmann, V.; Guilhot, J.; Saussele, S.; Rosti, G.; Guilhot, F.; Porkka, K.; Ossenkoppele, G.; Lindoerfer, D.; et al. Predicting complete cytogenetic response and subsequent progression-free survival in 2060 patients with cml on imatinib treatment: The eutos score. Blood 2011, 118, 686–692. [Google Scholar] [CrossRef]
- Mitelman, F. The cytogenetic scenario of chronic myeloid leukemia. Leuk. Lymphoma 1993, 11 (Suppl. 1), 11–15. [Google Scholar] [CrossRef]
- Cortes, J.E.; Saglio, G.; Kantarjian, H.M.; Baccarani, M.; Mayer, J.; Boque, C.; Shah, N.P.; Chuah, C.; Casanova, L.; Bradley-Garelik, B.; et al. Final 5-year study results of dasision: The dasatinib versus imatinib study in treatment-naïve chronic myeloid leukemia patients trial. J. Clin. Oncol. 2016, 34, 2333–2340. [Google Scholar] [CrossRef]
- Hochhaus, A.; Saglio, G.; Hughes, T.P.; Larson, R.A.; Kim, D.W.; Issaragrisil, S.; le Coutre, P.D.; Etienne, G.; Dorlhiac-Llacer, P.E.; Clark, R.E.; et al. Long-term benefits and risks of frontline nilotinib vs imatinib for chronic myeloid leukemia in chronic phase: 5-year update of the randomized enestnd trial. Leukemia 2016, 30, 1044–1054. [Google Scholar] [CrossRef] [PubMed]
- Hochhaus, A.; Larson, R.A.; Guilhot, F.; Radich, J.P.; Branford, S.; Hughes, T.P.; Baccarani, M.; Deininger, M.W.; Cervantes, F.; Fujihara, S.; et al. Long-term outcomes of imatinib treatment for chronic myeloid leukemia. N. Engl. J. Med. 2017, 376, 917–927. [Google Scholar] [CrossRef] [PubMed]
- Akosile, M.; Pierce, S.; Brandt, M.; Verstovsek, S.; Borthakur, G.; Kantarjian, H.; Ravandi, F.; Wierda, W.; Garcia-Manero, G.; Daver, N.; et al. Survival impact of patients (pts) with chronic myeloid leukemia (cml) due to failure from the use of one or more tyrosine kinase inhibitors (tki). Blood 2015, 126, 1587. [Google Scholar] [CrossRef]
- Kong, J.H.; Winton, E.F.; Heffner, L.T.; Chen, Z.; Langston, A.A.; Hill, B.; Arellano, M.; El-Rassi, F.; Kim, A.; Jillella, A.; et al. Does the frequency of molecular monitoring after tyrosine kinase inhibitor discontinuation affect outcomes of patients with chronic myeloid leukemia? Cancer 2017, 123, 2482–2488. [Google Scholar] [CrossRef] [PubMed]
- Wu, E.Q.; Guerin, A.; Yu, A.P.; Bollu, V.K.; Guo, A.; Griffin, J.D. Retrospective real-world comparison of medical visits, costs, and adherence between nilotinib and dasatinib in chronic myeloid leukemia. Curr. Med. Res. Opin. 2010, 26, 2861–2869. [Google Scholar] [CrossRef]
- Jabbour, E.; Cortes, J.; Nazha, A.; O’Brien, S.; Quintas-Cardama, A.; Pierce, S.; Garcia-Manero, G.; Kantarjian, H. Eutos score is not predictive for survival and outcome in patients with early chronic phase chronic myeloid leukemia treated with tyrosine kinase inhibitors: A single institution experience. Blood 2012, 119, 4524–4526. [Google Scholar] [CrossRef]
- Sato, E.; Iriyama, N.; Tokuhira, M.; Takaku, T.; Ishikawa, M.; Nakazato, T.; Sugimoto, K.J.; Fujita, H.; Fujioka, I.; Asou, N.; et al. Introduction of second-generation tyrosine kinase inhibitors may reduce the prognostic impact of high-risk patients, according to the european treatment and outcome study (eutos) score. Leuk. Lymphoma 2017, 1–8. [Google Scholar] [CrossRef]
- Hoffmann, V.S.; Baccarani, M.; Hasford, J.; Castagnetti, F.; Di Raimondo, F.; Casado, L.F.; Turkina, A.; Zackova, D.; Ossenkoppele, G.; Zaritskey, A.; et al. Treatment and outcome of 2904 cml patients from the eutos population-based registry. Leukemia 2017, 31, 593–601. [Google Scholar] [CrossRef]
- Branford, S.; Yeung, D.T.; Ross, D.M.; Prime, J.A.; Field, C.R.; Altamura, H.K.; Yeoman, A.L.; Georgievski, J.; Jamison, B.A.; Phillis, S.; et al. Early molecular response and female sex strongly predict stable undetectable bcr-abl1, the criteria for imatinib discontinuation in patients with cml. Blood 2013, 121, 3818–3824. [Google Scholar] [CrossRef]
- Hehlmann, R.; Lauseker, M.; Saussele, S.; Pfirrmann, M.; Krause, S.; Kolb, H.J.; Neubauer, A.; Hossfeld, D.K.; Nerl, C.; Gratwohl, A.; et al. Assessment of imatinib as first-line treatment of chronic myeloid leukemia: 10-year survival results of the randomized cml study iv and impact of non-cml determinants. Leukemia 2017, 31, 2398–2406. [Google Scholar] [CrossRef]
- Eskazan, A.E.; Sadri, S.; Keskin, D.; Ayer, M.; Kantarcioglu, B.; Demirel, N.; Aydin, D.; Aydinli, F.; Yokus, O.; Ozunal, I.E.; et al. Outcomes of chronic myeloid leukemia patients with early molecular response at 3 and 6 months: A comparative analysis of generic imatinib and glivec. Clin. Lymphoma Myeloma Leuk. 2017, 17, 804–811. [Google Scholar] [CrossRef] [PubMed]
- Marin, D.; Ibrahim, A.R.; Lucas, C.; Gerrard, G.; Wang, L.; Szydlo, R.M.; Clark, R.E.; Apperley, J.F.; Milojkovic, D.; Bua, M.; et al. Assessment of bcr-abl1 transcript levels at 3 months is the only requirement for predicting outcome for patients with chronic myeloid leukemia treated with tyrosine kinase inhibitors. J. Clin. Oncol. 2012, 30, 232–238. [Google Scholar] [CrossRef] [PubMed]
- Jain, P.; Kantarjian, H.; Nazha, A.; O’Brien, S.; Jabbour, E.; Romo, C.G.; Pierce, S.; Cardenas-Turanzas, M.; Verstovsek, S.; Borthakur, G.; et al. Early responses predict better outcomes in patients with newly diagnosed chronic myeloid leukemia: Results with four tyrosine kinase inhibitor modalities. Blood 2013, 121, 4867–4874. [Google Scholar] [CrossRef]
- Jabbour, E.; Kantarjian, H.M.; Saglio, G.; Steegmann, J.L.; Shah, N.P.; Boque, C.; Chuah, C.; Pavlovsky, C.; Mayer, J.; Cortes, J.; et al. Early response with dasatinib or imatinib in chronic myeloid leukemia: 3-year follow-up from a randomized phase 3 trial (dasision). Blood 2014, 123, 494–500. [Google Scholar] [CrossRef] [PubMed]
- Perry, A.M.; Brunner, A.M.; Zou, T.; McGregor, K.L.; Amrein, P.C.; Hobbs, G.S.; Ballen, K.K.; Neuberg, D.S.; Fathi, A.T. Association between insurance status at diagnosis and overall survival in chronic myeloid leukemia: A population-based study. Cancer 2017, 123, 2561–2569. [Google Scholar] [CrossRef]
- Noens, L.; van Lierde, M.A.; De Bock, R.; Verhoef, G.; Zachee, P.; Berneman, Z.; Martiat, P.; Mineur, P.; Van Eygen, K.; MacDonald, K.; et al. Prevalence, determinants, and outcomes of nonadherence to imatinib therapy in patients with chronic myeloid leukemia: The adagio study. Blood 2009, 113, 5401–5411. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| n | % | ||
|---|---|---|---|
| Median Age at Diagnosis, Years (Range) | a 50 (11–88) | ||
| Sex | M/F | 105/101 | 51/49 |
| Race | African American | 56 | 27.2 |
| Asian | 5 | 2.4 | |
| Hispanic | 6 | 2.9 | |
| White | 106 | 51.5 | |
| Others | 3 | 1.5 | |
| Unknown or declined | 30 | 14.6 | |
| Risk (available, n = 110) | Sokal Low/Intermediate/High | 64/27/19 | 58.2/24.5/17.3 |
| Hasford Low/Intermediate/High | 66/38/6 | 60.0/34.5/5.5 | |
| EUTOS Low/High | 95/15 | 86.4/13.6 | |
| b Additional chromosomal abnormality (available, n = 173) | 12 | 6.9 | |
| Number of used TKI | 1 | 76 | 36.9 |
| 2 | 73 | 35.4 | |
| 3 | 33 | 16.0 | |
| 4 | 17 | 8.3 | |
| 5 | 7 | 3.4 | |
| 1st-line TKI (n = 206) | IM/DAS/NIL/BOS/PON | 145/43/13/4/1 | 70.4/20.9/6.3/1.9/0.5 |
| 2nd-line TKI (n = 130) | IM/DAS/NIL/BOS/PON/REB | 28/68/23/9/1/1 | 21.5/52.3/17.7/6.9/0.8/0.8 |
| 3rd-line TKI (n = 65) | IM/DAS/NIL/BOS/PON | 8/19/21/11/6 | 12.3/29.2/32.3/16.9/9.2 |
| 4th-line TKI (n = 30) | IM/DAS/NIL/BOS/PON/REB | 4/4/1/9/11/1 | 13.3/13.3/3.3/30.0/36.7/3.3 |
| 5th-line TKI (n = 10) | DAS/BOS/PON | 3/3/4 | 30.0/30.0/40.0 |
| Reason for TKI switch or discontinuation (239 events) | R | c 119 | 49.8 |
| I | c 104 | 43.5 | |
| O | c 16 | 6.7 | |
| Nivolumab | 3 | 1.5 | |
| Blinatumomab | 1 | 0.5 | |
| Chemotherapy | 12 | 5.8 | |
| HSCT | Allogeneic/Autologous | 8/1 | 3.9/0.5 |
| dABL domain mutation (n = 72) | Positive | 25 | 34.7 |
| n (%) | IM (n = 145) | NG-TKI (n = 61) | p | |
|---|---|---|---|---|
| Switching TKIs | 93 (64.1) | 37 (60.7) | 0.639 | |
| Median follow up, months (range) | 80.9 (1.4–190.1) | 23.6 (1.7–64.6) | 0.000 | |
| BCR/ABL1IS at 3 months (n = 111) | ≤10% | 39 (59.1) | 39 (86.7) | 0.003 |
| >10% | 27 (40.9) | 6 (13.3) | ||
| BCR/ABL1IS at 6 months (n = 106) | <1% | 36 (54.5) | 32 (80.0) | 0.012 |
| ≥1% | 30 (45.5) | 8 (20.0) | ||
| BCR/ABL1 at 1 year (n = 103) | ≤0.1% | 33 (51.6) | 30 (76.9) | 0.013 |
| >0.1% | 31 (48.4) | 9 (23.1) | ||
| The last BCR/ABL1IS <0.1 | 83 (57.2) | 43 (70.5) | 0.086 | |
| Disease progression | 17 (11.7) | 2 (3.3) | 0.066 | |
| Death | 9 (6.2) | 2 (3.3) | 0.513 | |
| TKI | 1 CMR, n (%) | 2 Additional CMR, n (%) | 3 Attempts of TKI Discontinuation, n (%) | 4 TKI Discontinuation, n (%) |
|---|---|---|---|---|
| 1st-line TKI (n = 206) | 69 (33.5) | - | 14 (6.8) | 7 (3.4) |
| 2nd-line TKI (n = 130) | 52 (40.0) | 41 (31.5) | 7 (5.4) | 5 (3.8) |
| 3rd-line TKI (n = 65) | 18 (27.7) | 8 (12.3) | 1 (1.5) | 1 (1.5) |
| 4th-line TKI (n = 30) | 8 (26.7) | 5 (16.7) | 3 (10.0) | 1 (3.3) |
| 5th-line TKI (n = 10) | 1 (10.0) | 1 | 0 | 0 (0) |
| Total (n = 206) | 124(60.2) | - | 25(12.1) | 14 (6.8) |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kong, J.H.; Winton, E.F.; Heffner, L.T.; Gaddh, M.; Hill, B.; Neely, J.; Hatcher, A.; Joseph, M.; Arellano, M.; El-Rassi, F.; et al. Outcomes of Chronic Phase Chronic Myeloid Leukemia after Treatment with Multiple Tyrosine Kinase Inhibitors. J. Clin. Med. 2020, 9, 1542. https://doi.org/10.3390/jcm9051542
Kong JH, Winton EF, Heffner LT, Gaddh M, Hill B, Neely J, Hatcher A, Joseph M, Arellano M, El-Rassi F, et al. Outcomes of Chronic Phase Chronic Myeloid Leukemia after Treatment with Multiple Tyrosine Kinase Inhibitors. Journal of Clinical Medicine. 2020; 9(5):1542. https://doi.org/10.3390/jcm9051542
Chicago/Turabian StyleKong, Jee Hyun, Elliott F. Winton, Leonard T. Heffner, Manila Gaddh, Brittany Hill, Jessica Neely, Angela Hatcher, Meena Joseph, Martha Arellano, Fuad El-Rassi, and et al. 2020. "Outcomes of Chronic Phase Chronic Myeloid Leukemia after Treatment with Multiple Tyrosine Kinase Inhibitors" Journal of Clinical Medicine 9, no. 5: 1542. https://doi.org/10.3390/jcm9051542
APA StyleKong, J. H., Winton, E. F., Heffner, L. T., Gaddh, M., Hill, B., Neely, J., Hatcher, A., Joseph, M., Arellano, M., El-Rassi, F., Kim, A., Khoury, J. H., & Kota, V. K. (2020). Outcomes of Chronic Phase Chronic Myeloid Leukemia after Treatment with Multiple Tyrosine Kinase Inhibitors. Journal of Clinical Medicine, 9(5), 1542. https://doi.org/10.3390/jcm9051542