Serum GlycA Level Is Elevated in Active Systemic Lupus Erythematosus and Correlates to Disease Activity and Lupus Nephritis Severity

 , and
, and
Abstract
1. Introduction
2. Materials and Methods
2.1. Patient Demographics & Ethics
2.2. Clinical and Conventional Biological Metrics
2.3. GlycA Quantification
2.4. Statistical Analysis
3. Results
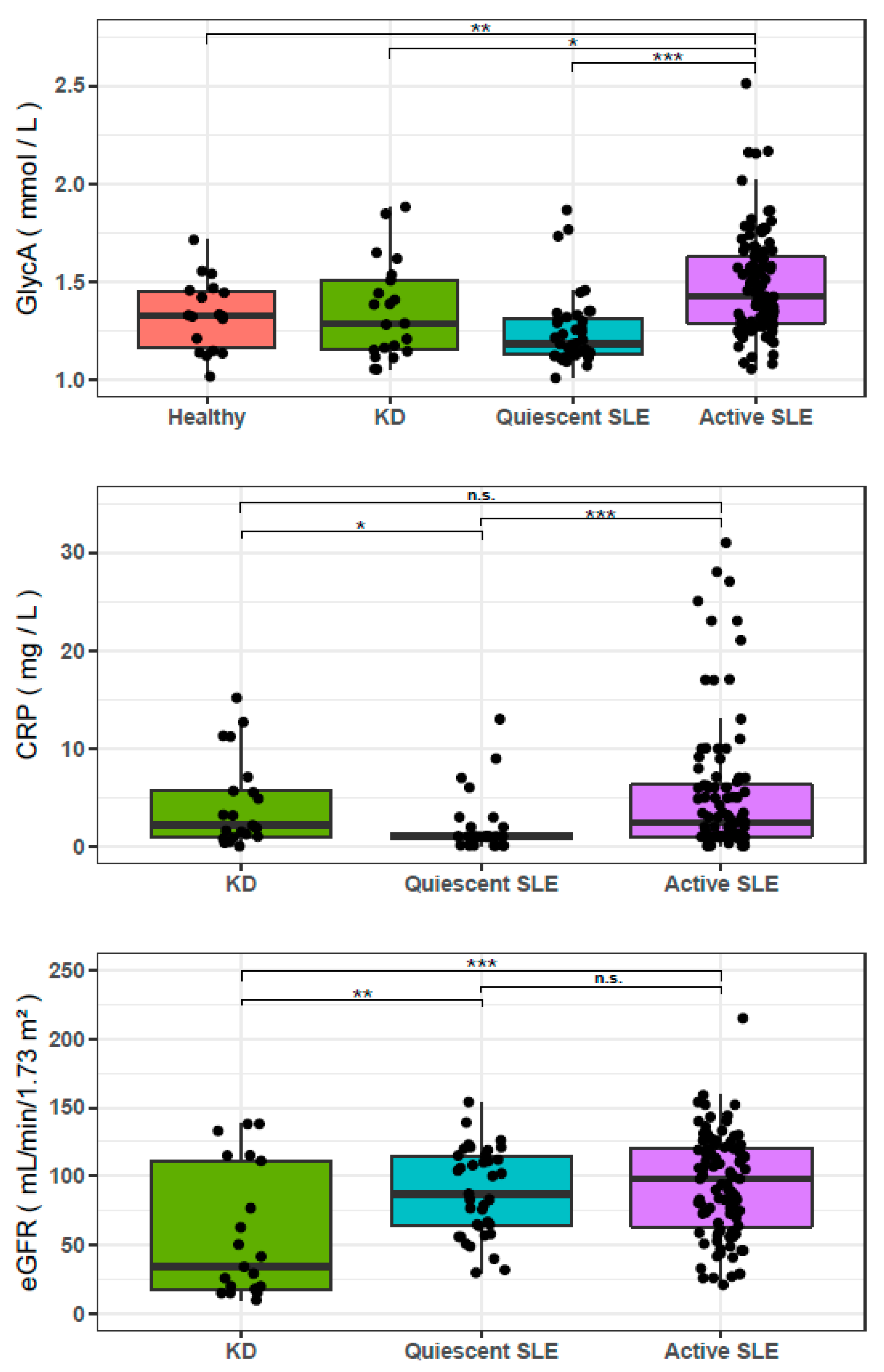
3.1. GlycA is Elevated in Patients with Active SLE
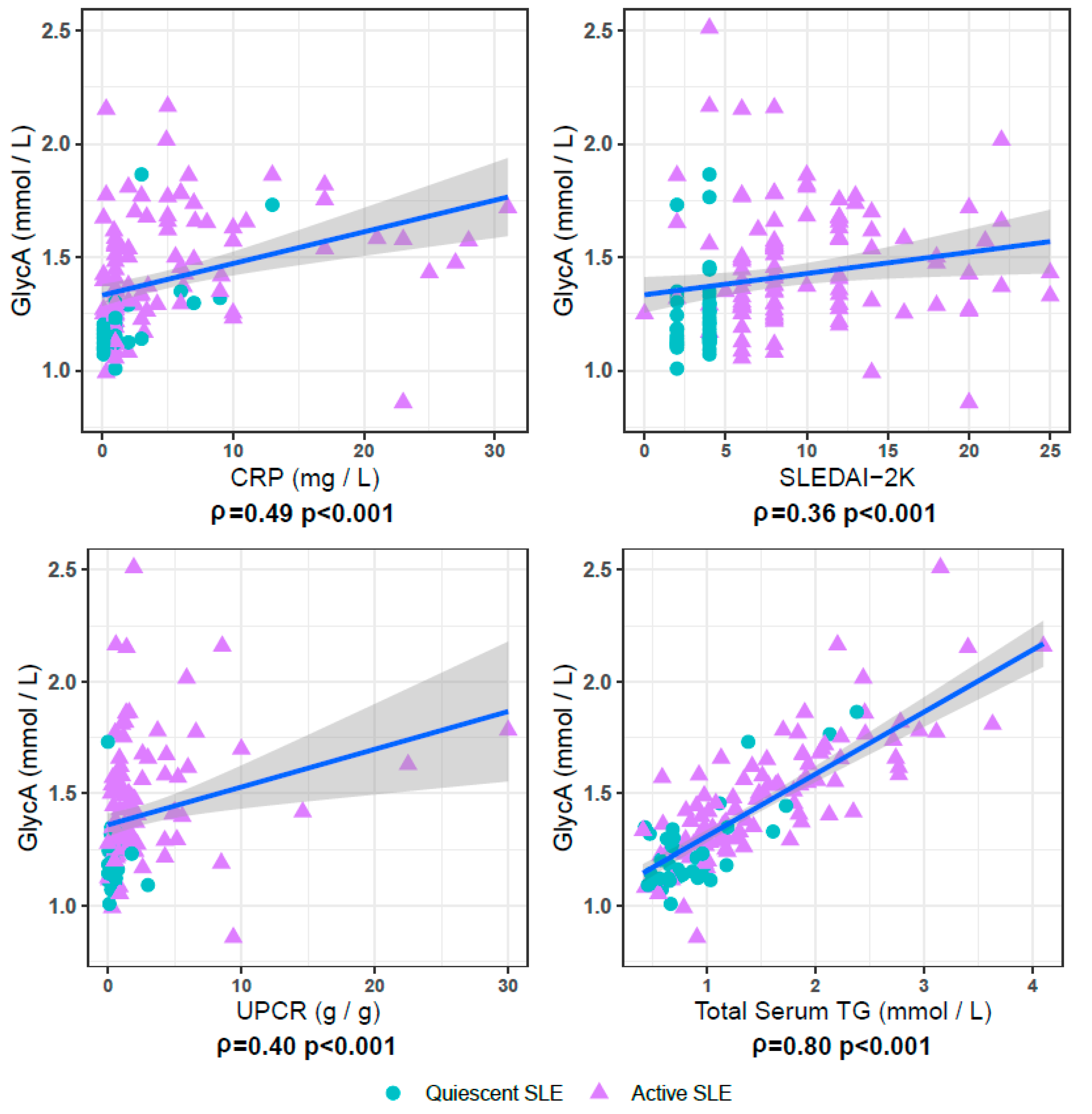
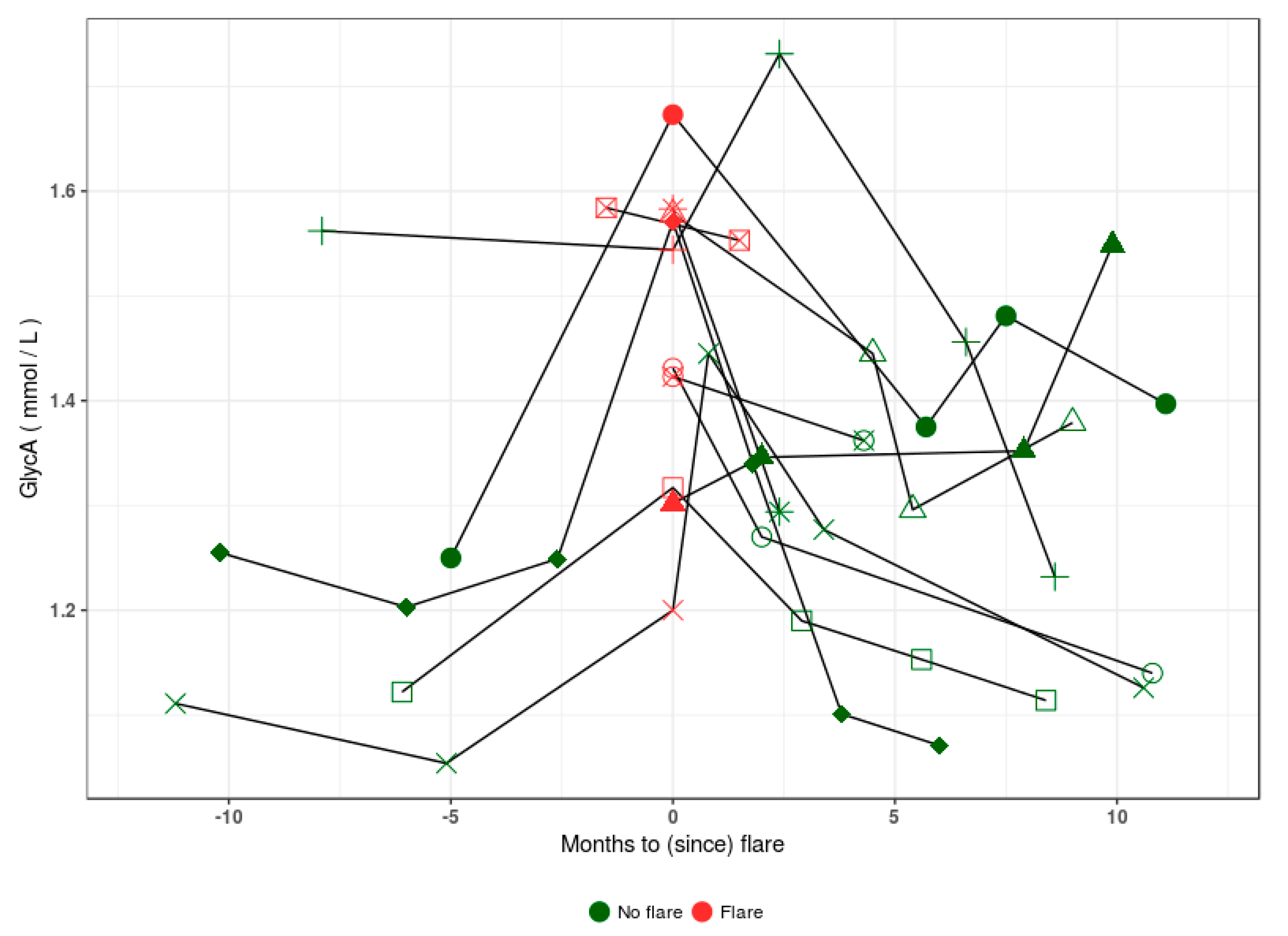
3.2. GlycA Is Associated with Disease Activity in SLE
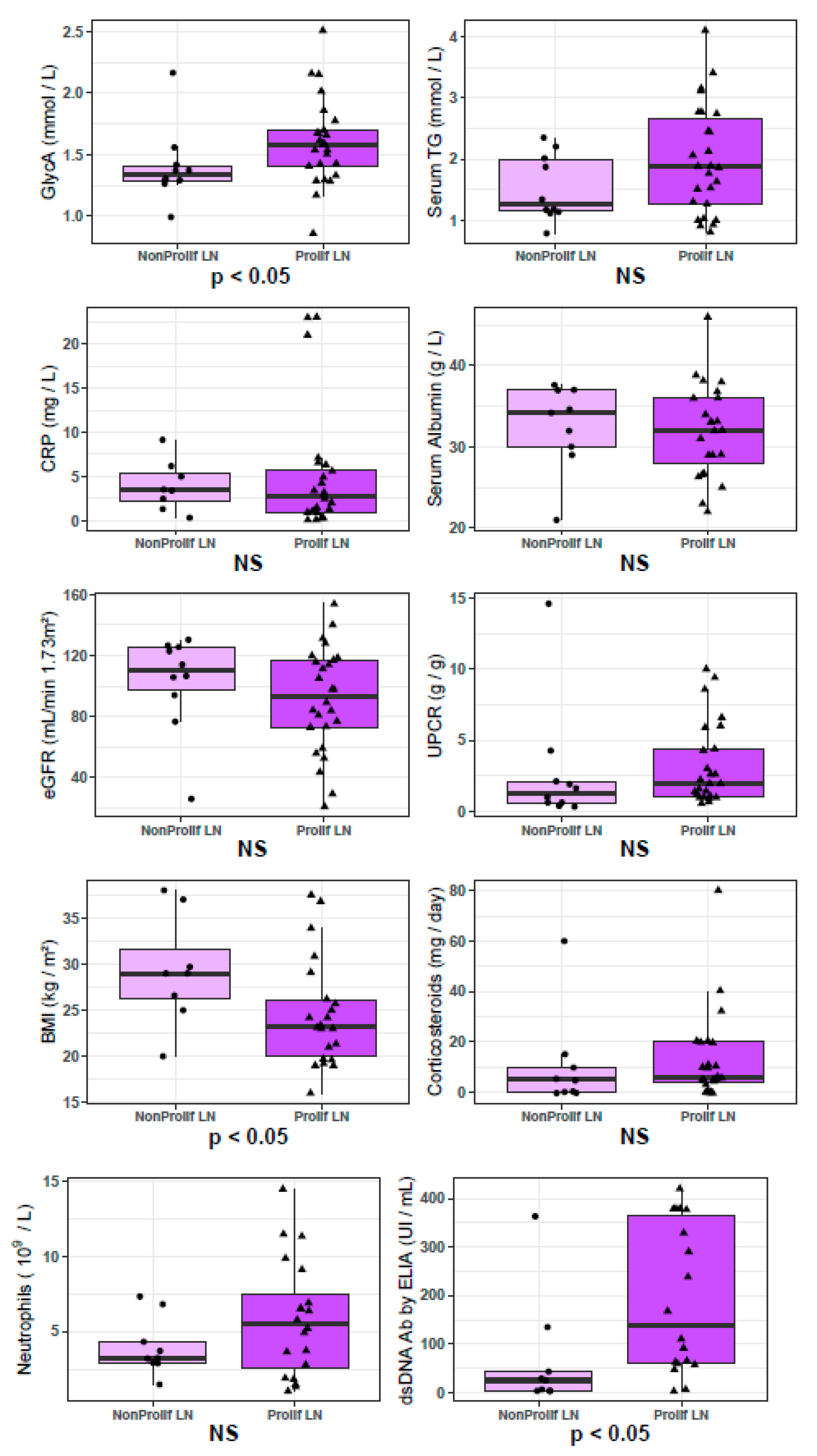
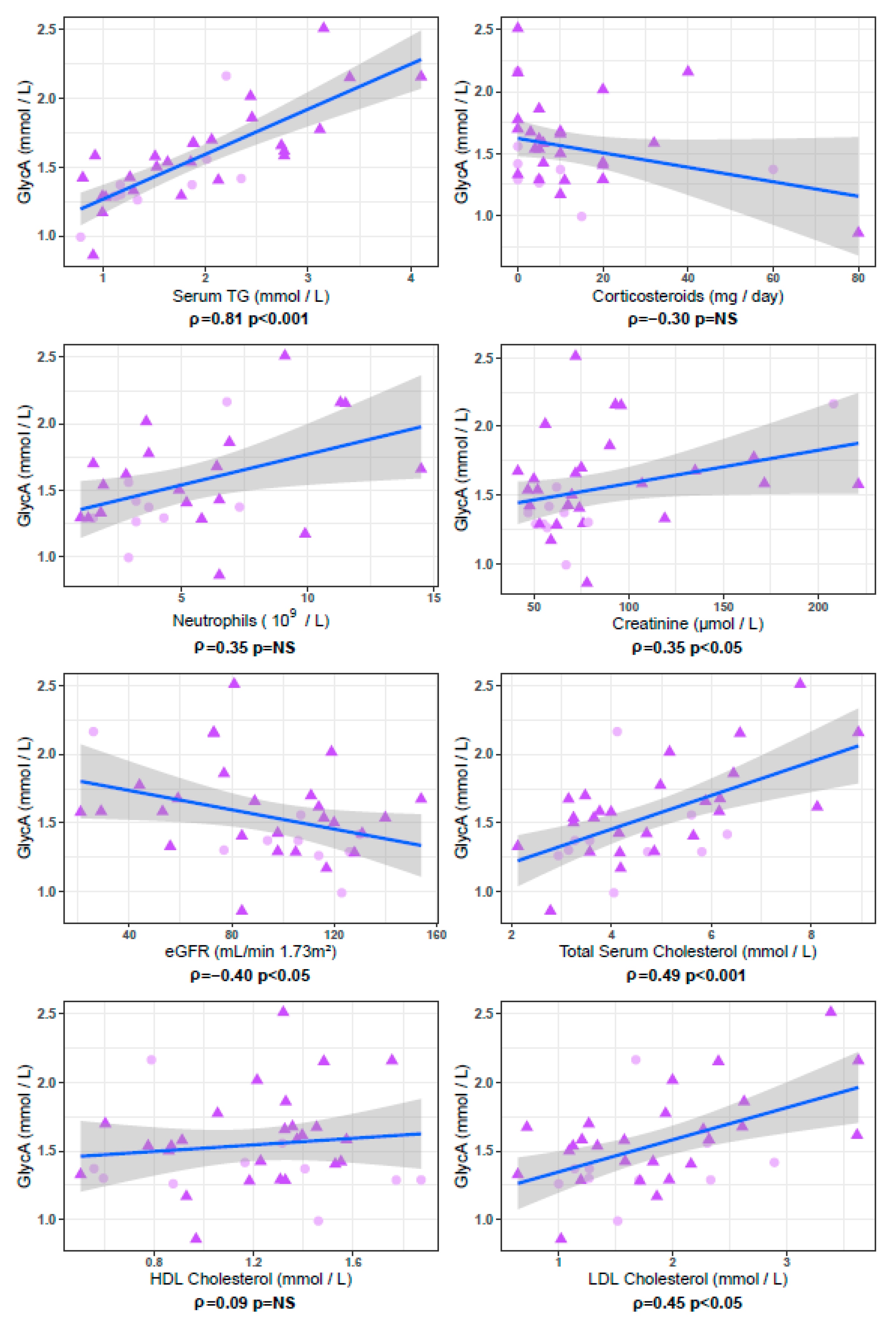
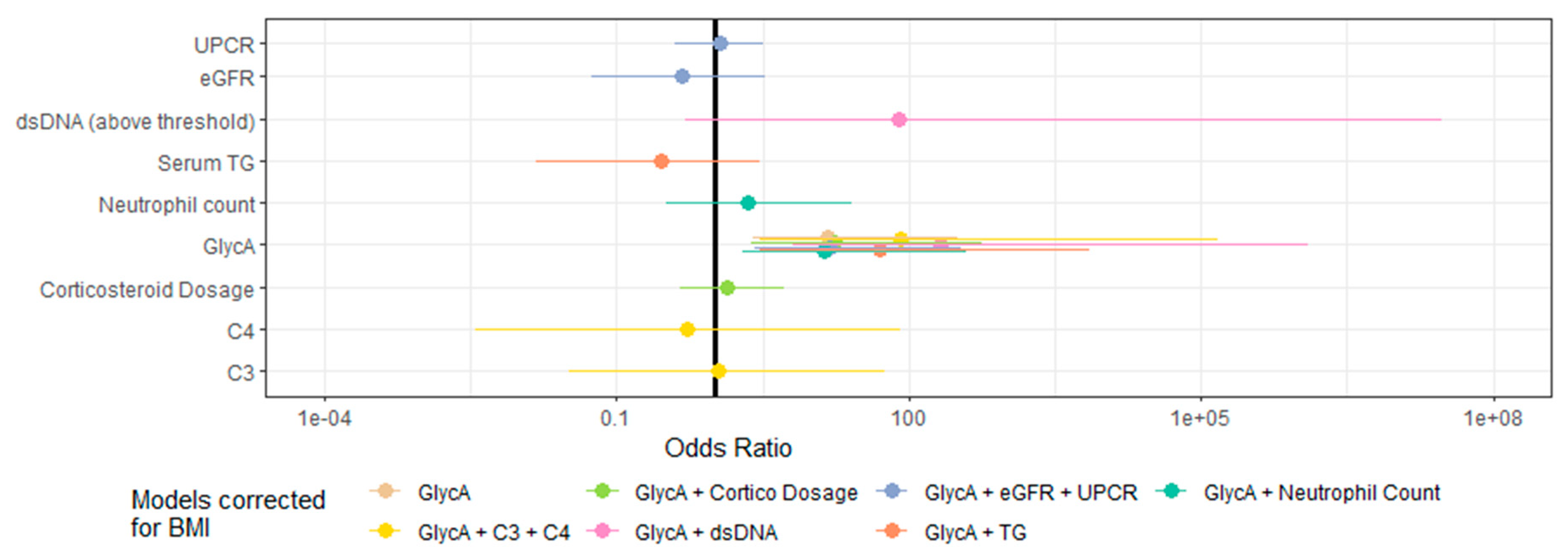
3.3. GlycA Is Associated with the Pathological Severity of LN
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Arriens, C.; Wren, J.D.; Munroe, M.E.; Mohan, C. Systemic lupus erythematosus biomarkers: The challenging quest. Rheumatology 2017, 56, i32–i45. [Google Scholar] [CrossRef]
- Bertsias, G.K.; Tektonidou, M.G.; Amoura, Z.; Aringer, M.; Bajema, I.; Berden, J.H.M.; Boletis, J.; Cervera, R.; Dörner, T.; Doria, A.; et al. Joint European League Against Rheumatism and European Renal Association–European Dialysis and Transplant Association (EULAR/ERA-EDTA) recommendations for the management of adult and paediatric lupus nephritis. Ann. Rheum. Dis. 2012, 71, 1771–1782. [Google Scholar] [CrossRef] [PubMed]
- Hermansen, M.-L.; Lindhardsen, J.; Torp-Pedersen, C.; Faurschou, M.; Jacobsen, S. The risk of cardiovascular morbidity and cardiovascular mortality in systemic lupus erythematosus and lupus nephritis: A Danish nationwide population-based cohort study. Rheumatology 2017, 56, 709–715. [Google Scholar] [CrossRef] [PubMed]
- Thomas, G.; Mancini, J.; Jourde-Chiche, N.; Sarlon, G.; Amoura, Z.; Harle, J.-R.; Jougla, E.; Chiche, L. Mortality associated with systemic lupus erythematosus in France assessed by multiple-cause-of-death analysis. Arthritis Rheumatol. 2014, 66, 2503–2511. [Google Scholar] [CrossRef] [PubMed]
- Costenbader, K.H.; Desai, A.; Alarcón, G.S.; Hiraki, L.T.; Shaykevich, T.; Brookhart, M.A.; Massarotti, E.; Lu, B.; Solomon, D.H.; Winkelmayer, W.C. Trends in the incidence, demographics, and outcomes of end-stage renal disease due to lupus nephritis in the US from 1995 to 2006. Arthritis Rheum. 2011, 63, 1681–1688. [Google Scholar] [CrossRef] [PubMed]
- Bajema, I.M.; Wilhelmus, S.; Alpers, C.E.; Bruijn, J.A.; Colvin, R.B.; Cook, H.T.; D’Agati, V.D.; Ferrario, F.; Haas, M.; Jennette, J.C.; et al. Revision of the International Society of Nephrology/Renal Pathology Society classification for lupus nephritis: Clarification of definitions, and modified National Institutes of Health activity and chronicity indices. Kidney Int. 2018, 93, 789–796. [Google Scholar] [CrossRef]
- Dörner, T.; Furie, R. Novel paradigms in systemic lupus erythematosus. Lancet 2019, 393, 2344–2358. [Google Scholar] [CrossRef]
- Mohan, C.; Putterman, C. Genetics and pathogenesis of systemic lupus erythematosus and lupus nephritis. Nat. Rev. Nephrol. 2015, 11, 329–341. [Google Scholar] [CrossRef]
- Aringer, M. Inflammatory markers in systemic lupus erythematosus. J. Autoimmun. 2019, 102374, 102374. [Google Scholar] [CrossRef]
- Würtz, P.; Kangas, A.; Soininen, P.; Lawlor, D.; Smith, G.D.; Ala-Korpela, M. Quantitative Serum Nuclear Magnetic Resonance Metabolomics in Large-Scale Epidemiology: A Primer on -Omic Technologies. Am. J. Epidemiol. 2017, 186, 1084–1096. [Google Scholar] [CrossRef]
- Soininen, P.; Kangas, A.; Würtz, P.; Suna, T.; Ala-Korpela, M. Quantitative Serum Nuclear Magnetic Resonance Metabolomics in Cardiovascular Epidemiology and Genetics. Circ. Cardiovasc. Genet. 2015, 8, 192–206. [Google Scholar] [CrossRef] [PubMed]
- Connelly, M.A.; Otvos, J.D.; Shalaurova, I.; Playford, M.; Mehta, N.N. GlycA, a novel biomarker of systemic inflammation and cardiovascular disease risk. J. Transl. Med. 2017, 15, 219. [Google Scholar] [CrossRef] [PubMed]
- Lawler, P.R.; Akinkuolie, A.O.; Chandler, P.D.; Moorthy, M.V.; Vandenburgh, M.J.; Schaumberg, D.A.; Lee, I.M.; Glynn, R.J.; Ridker, P.M.; Buring, J.E.; et al. Circulating N-Linked Glycoprotein Acetyls and Longitudinal Mortality RiskNovelty and Significance. Circ. Res. 2016, 118, 1106–1115. [Google Scholar] [CrossRef] [PubMed]
- Gruppen, E.G.; Riphagen, I.J.; Connelly, M.A.; Otvos, J.D.; Bakker, S.J.L.; Dullaart, R.P.F. GlycA, a Pro-Inflammatory Glycoprotein Biomarker, and Incident Cardiovascular Disease: Relationship with C-Reactive Protein and Renal Function. PLoS ONE 2015, 10, e0139057. [Google Scholar] [CrossRef]
- Duprez, D.A.; Otvos, J.; Sanchez, O.A.; Mackey, R.H.; Tracy, R.; Jacobs, D.R. Comparison of the Predictive Value of GlycA and Other Biomarkers of Inflammation for Total Death, Incident Cardiovascular Events, Noncardiovascular and Noncancer Inflammatory-Related Events, and Total Cancer Events. Clin. Chem. 2016, 62, 1020–1031. [Google Scholar] [CrossRef]
- Ritchie, S.C.; Würtz, P.; Nath, A.P.; Abraham, G.; Havulinna, A.S.; Fearnley, L.G.; Sarin, A.-P.; Kangas, A.; Soininen, P.; Aalto, K.; et al. The Biomarker GlycA Is Associated with Chronic Inflammation and Predicts Long-Term Risk of Severe Infection. Cell Syst. 2015, 1, 293–301. [Google Scholar] [CrossRef]
- Titan, S.M.; Pecoits-Filho, R.F.; Barreto, S.M.; Lopes, A.A.; Bensenor, I.J.; Lotufo, P.A. GlycA, a marker of protein glycosylation, is related to albuminuria and estimated glomerular filtration rate: The ELSA-Brasil study. BMC Nephrol. 2017, 18, 367. [Google Scholar] [CrossRef]
- Dierckx, T.; Verstockt, B.; Vermeire, S.; Van Weyenbergh, J. GlycA, a nuclear magnetic resonance spectroscopy measure for protein glycosylation, is a viable biomarker for disease activity in IBD. J. Crohns Colitis 2018, 13, 389–394. [Google Scholar] [CrossRef]
- Rother, N.; Pieterse, E.; Lubbers, J.; Hilbrands, L.; Van Der Vlag, J. Acetylated Histones in Apoptotic Microparticles Drive the Formation of Neutrophil Extracellular Traps in Active Lupus Nephritis. Front. Immunol. 2017, 8, 1–12. [Google Scholar] [CrossRef]
- Jourde-Chiche, N.; Whalen, E.; Gondouin, B.; Speake, C.; Gersuk, V.; Dussol, B.; Burtey, S.; Pascual, V.; Chaussabel, D.; Chiche, L. Modular transcriptional repertoire analyses identify a blood neutrophil signature as a candidate biomarker for lupus nephritis. Rheumatology 2016, 56, kew439. [Google Scholar] [CrossRef]
- Petri, M.; Orbai, A.-M.; Alarcón, G.S.; Gordon, C.; Merrill, J.T.; Fortin, P.R.; Bruce, I.N.; Isenberg, D.A.; Wallace, D.J.; Nived, O.; et al. Derivation and validation of the Systemic Lupus International Collaborating Clinics classification criteria for systemic lupus erythematosus. Arthritis Rheum. 2012, 64, 2677–2686. [Google Scholar] [CrossRef] [PubMed]
- Steiman, A.J.; Gladman, D.D.; Ibañez, D.; Urowitz, M.B. Prolonged Serologically Active Clinically Quiescent Systemic Lupus Erythematosus: Frequency and Outcome. J. Rheumatol. 2010, 37, 1822–1827. [Google Scholar] [CrossRef] [PubMed]
- Nikpour, M.; Urowitz, M.B.; Ibañez, D.; Gladman, D.D. Frequency and determinants of flare and persistently active disease in systemic lupus erythematosus. Arthritis Rheum. 2009, 61, 1152–1158. [Google Scholar] [CrossRef] [PubMed]
- Levey, A.S.; Coresh, J.; Greene, T.; Stevens, L.A.; Zhang, Y.L.; Hendriksen, S.; Kusek, J.W.; Van Lente, F.; Chronic Kidney Disease Epidemiology Collaboration. Using standardized serum creatinine values in the modification of diet in renal disease study equation for estimating glomerular filtration rate. Ann. Intern. Med. 2006, 145, 247–254. [Google Scholar] [CrossRef]
- Purmalek, M.M.; Carlucci, P.M.; Dey, A.K.; Sampson, M.; Temesgen-Oyelakin, Y.; Sakhardande, S.; Lerman, J.B.; Fike, A.; Davis, M.; Chung, J.H.; et al. Association of lipoprotein subfractions and glycoprotein acetylation with coronary plaque burden in SLE. Lupus Sci. Med. 2019, 6, e000332. [Google Scholar] [CrossRef]
- Svenungsson, E.; Gunnarsson, I.; Fei, G.-Z.; Lundberg, I.E.; Klareskog, L.; Frostegård, J. Elevated triglycerides and low levels of high-density lipoprotein as markers of disease activity in association with up-regulation of the tumor necrosis factor α/tumor necrosis factor receptor system in systemic lupus erythematosus. Arthritis Rheum. 2003, 48, 2533–2540. [Google Scholar] [CrossRef]
- Durcan, L.; Winegar, D.A.; Connelly, M.A.; Otvos, J.D.; Magder, L.S.; Petri, M. Longitudinal Evaluation of Lipoprotein Variables in Systemic Lupus Erythematosus Reveals Adverse Changes with Disease Activity and Prednisone and More Favorable Profiles with Hydroxychloroquine Therapy. J. Rheumatol. 2016, 43, 745–750. [Google Scholar] [CrossRef]
- Szabó, M.Z.; Szodoray, P.; Kiss, E. Dyslipidemia in systemic lupus erythematosus. Immunol. Res. 2017, 65, 543–550. [Google Scholar] [CrossRef]
- R Core Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2017. [Google Scholar]
- Wickam, H. ggplot2: Elegant Graphics for Data Analysis; Springer: New York, NY, USA, 2009. [Google Scholar]
- Chung, C.P.; Ormseth, M.J.; Connelly, M.A.; Oeser, A.; Solus, J.F.; Otvos, J.D.; Raggi, P.; Stein, C.M. GlycA, a novel marker of inflammation, is elevated in systemic lupus erythematosus. Lupus 2016, 25, 296–300. [Google Scholar] [CrossRef]
- Fizelova, M.; Jauhiainen, R.; Kangas, A.; Soininen, P.; Ala-Korpela, M.; Kuusisto, J.; Laakso, M.; Stančáková, A. Differential Associations of Inflammatory Markers with Insulin Sensitivity and Secretion: The Prospective METSIM Study. J. Clin. Endocrinol. Metab. 2017, 102, 3600–3609. [Google Scholar] [CrossRef]
- Akinkuolie, A.O.; Buring, J.E.; Ridker, P.M.; Mora, S. A Novel Protein Glycan Biomarker and Future Cardiovascular Disease Events. J. Am. Heart Assoc. 2014, 3, e001221. [Google Scholar] [CrossRef] [PubMed]
- Chandler, P.; Akinkuolie, A.O.; Tobias, D.K.; Lawler, P.R.; Li, C.; Moorthy, M.V.; Wang, L.; Duprez, D.A.; Jacobs, D.R.; Glynn, R.J.; et al. Association of N-Linked Glycoprotein Acetyls and Colorectal Cancer Incidence and Mortality. PLoS ONE 2016, 11, e0165615. [Google Scholar] [CrossRef] [PubMed]
- Harpsøe, M.C.; Basit, S.; Andersson, M.; Nielsen, N.M.; Frisch, M.; Wohlfahrt, J.; Nohr, E.A.; Linneberg, A.; Jess, T. Body mass index and risk of autoimmune diseases: A study within the Danish National Birth Cohort. Int. J. Epidemiol. 2014, 43, 843–855. [Google Scholar] [CrossRef] [PubMed]
- Versini, M.; Jeandel, P.-Y.; Rosenthal, E.; Shoenfeld, Y. Obesity in autoimmune diseases: Not a passive bystander. Autoimmun. Rev. 2014, 13, 981–1000. [Google Scholar] [CrossRef] [PubMed]
- Oeser, A.; Chung, C.P.; Asanuma, Y.; Avalos, I.; Stein, C.M. Obesity is an independent contributor to functional capacity and inflammation in systemic lupus erythematosus. Arthritis Rheum. 2005, 52, 3651–3659. [Google Scholar] [CrossRef]
- Rizk, A.; Gheita, T.A.; Nassef, S.; Abdallah, A. The impact of obesity in systemic lupus erythematosus on disease parameters, quality of life, functional capacity and the risk of atherosclerosis. Int. J. Rheum. Dis. 2012, 15, 261–267. [Google Scholar] [CrossRef]
- D’Agati, V.D.; Chagnac, A.; De Vries, A.; Levi, M.; Porrini, E.; Herman-Edelstein, M.; Praga, M. Obesity-related glomerulopathy: Clinical and pathologic characteristics and pathogenesis. Nat. Rev. Nephrol. 2016, 12, 453–471. [Google Scholar] [CrossRef]
- Li-Gao, R.; Hughes, D.; Le Cessie, S.; De Mutsert, R.; Heijer, M.D.; Rosendaal, F.R.; Van Dijk, K.W.; Timpson, N.J.; Mook-Kanamori, D.O. Assessment of reproducibility and biological variability of fasting and postprandial plasma metabolite concentrations using 1H-NMR spectroscopy. PLoS ONE 2019, 14, e0218549. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| NMR Measurement | Healthy Controls (n = 20) | Non-Lupus Kidney Disease (n =21) | Quiescent SLE (n = 39) | Active SLE (n = 105) | All SLE (n = 144) | All SLE vs. HC | Quiescent SLE vs. HC | Active SLE vs. HC | Active SLE vs. Quiescent SLE | Active SLE vs. Non-Lupus KD |
|---|---|---|---|---|---|---|---|---|---|---|
| Serum albumin (NMR signal area) | 0.089, 0.085–0.092 | 0.079, 0.074–0.082 | 0.086, 0.083–0.088 | 0.078, 0.070–0.081 | 0.079, 0.074–0.085 | *** | NS | *** | *** | NS |
| Serum creatinin (µmol/L) | 51, 38–63 | 126, 74–218 | 57, 48–68 | 57, 47–74 | 57, 47–71 | NS | NS | NS | NS | *** |
| Total cholesterol (mmol/L) | 2.48, 2.21–2.89 | 3.65, 3.03–5.06 | 4.04, 2.91–4.49 | 4.12, 3.53–4.92 | 4.08, 3.34–4.77 | *** | *** | *** | * | NS |
| HDL cholesterol (mmol/L) | 0.76, 0.64–0.92 | 1.14, 0.99–1.26 | 1.55, 1.31–1.86 | 1.39, 1.05–1.70 | 1.43, 1.16–1.76 | *** | *** | *** | * | * |
| LDL cholesterol (mmol/L) | 0.81, 0.68–1.11 | 1.41, 1.04–2.01 | 1.18, 0.82–1.47 | 1.50, 1.18–1.85 | 1.43, 1.11–1.71 | *** | * | *** | *** | NS |
| Total triglycerides (mmol/L) | 0.89, 0.72–0.97 | 1.11, 0.87–1.91 | 0.75, 0.65–0.97 | 1.28, 0.95–1.91 | 1.10, 0.79–1.81 | ** | NS | *** | *** | NS |
| GlycA (mmol/L) | 1.32, 1.14–1.45 | 1.29, 1.15–1.51 | 1.18, 1.13–1.31 | 1.42, 1.29–1.62 | 1.349, 1.232–1.564 | NS | NS | ** | *** | * |
| Characteristics | Quiescent SLE n = 39 | Active SLE n = 105 | All SLE n = 144 |
|---|---|---|---|
| Age | −0.06 | −0.17 | −0.2 |
| Gender female (%) | NS | NS | NS |
| Ethnicity caucasian (%) | NS | NS | NS |
| BMI (kg/m2) | 0.07 | −0.12 | 0.07 |
| Current smoking (%) | NS | NS | NS |
| SLEDAI-2K | 0.15 | 0.01 | 0.36 *** |
| Corticosteroid daily dose (mg) | 0.12 | 0.02 | 0.07 |
| Hydroxychloroquine (%) | NS | NS | NS |
| CRP (mg/L) | 0.57 *** | 0.36 *** | 0.49 *** |
| Serum albumin (g/L) | −0.22 | −0.26 * | −0.41 *** |
| Serum creatinin (µmol/L) | 0.41 * | 0.25 | 0.16 |
| eGFR (mL/min 1.73m2) | −0.37 * | −0.14 | −0.13 |
| C3 (g/L) | −0.06 | −0.13 | −0.18 * |
| C4 (g/L) | −0.08 | 0.04 | −0.1 |
| dsDNA antibody presence (%) | NS | NS | NS |
| UPCR (g/g) | −0.12 | 0.23 * | 0.4 |
| Serum albumin (NMR signal area) | 0.06 | −0.09 | −0.27 ** |
| Serum creatinin (mmol/L) | 0.45 ** | 0.25 * | 0.26 ** |
| Total cholesterol (mmol/L) | 0.3 | 0.32 *** | 0.36 *** |
| HDL cholesterol (mmol/L) | 0.05 | −0.28 ** | −0.25 ** |
| LDL cholesterol (mmol/L) | 0.24 | 0.39 *** | 0.41 *** |
| Total serum triglycerides (mmol/L) | 0.43 ** | 0.81 *** | 0.80 *** |
| Characteristics | Biopsy Proven Flaring Non-Proliferative LN (n = 10) | Biopsy Proven Flaring Proliferative LN (n = 26) | Available Observations | Proliferative Status Wilcoxon/Chi2 p-Value | GlycA Association |
|---|---|---|---|---|---|
| Age | 35.5, 28–38.5 | 32, 25–39 | 36 | 0.46 | −0.10 |
| Gender Female (%) | 90 | 88 | 36 | 1.00 | NS |
| Ethnicity caucasian (%) | 80 | 85 | 36 | 1.00 | NS |
| BMI (kg/m2) | 29, 26.2–31.5 | 23.24, 20.03–26.10 | 30 | 0.04 | −0.002 |
| Currently smoking (%) | 40 | 28 | 35 | 0.77 | NS |
| SLEDAI-2K | 8, 4.5–13.5 | 12, 8–18 | 35 | 0.29 | −0.21 |
| Corticosteroid daily dose (mg) | 5, 0–10 | 6, 4–20 | 34 | 0.28 | −0.30 |
| Receiving Hydroxychloroquine (%) | 60 | 77 | 36 | 0.55 | NS |
| CRP (mg/L) | 3.5, 2.2–5.3 | 2.7, 0.98–5.78 | 32 | 0.60 | 0.01 |
| Serum albumin (g/L) | 34.2, 30–37 | 32, 27.9–36 | 32 | 0.60 | 0.07 |
| Serum creatinin (µmol/L) | 60, 55.5–66.75 | 73, 56.75–95.25 | 36 | 0.22 | 0.35 * |
| eGFR (mL/min/1.73m2) | 110.5, 97–125.25 | 93.5, 73–117 | 36 | 0.28 | −0.40 * |
| Neutrophil count (109/L) | 3.2, 2.9–4.3 | 5.5, 2.58–7.45 | 29 | 0.38 | 0.35 |
| C3 (g/L) | 1.04, 0.54–1.26 | 0.63, 0.45–0.88 | 29 | 0.19 | –0.10 |
| C4 (g/L) | 0.22, 0.08–0.25 | 0.10, 0.04–0.20 | 29 | 0.57 | 0.13 |
| dsDNA antibody presence (yes/no) | 60 | 91 | 33 | 0.10 | NS |
| dsDNA antibody ELIA (UI/mL) | 25, 3–43 | 139, 60–365 | 27 | 0.01 | −0.01 |
| UPCR (g/g) | 1.29, 0.60–2.05 | 1.94, 1.05–4.39 | 35 | 0.15 | 0.23 |
| Hematuria (%) | 67 | 70 | 29 | 1.00 | NS |
| Leukocyturia (%) | 56 | 60 | 29 | 1.00 | NS |
| NMR serum albumin (NMR signal area) | 0.070, 0.061–0.077 | 0.070, 0.066–0.079 | 36 | 0.52 | 0.40 * |
| NMR serum creatinin (µmol/L) | 52, 44–55 | 62, 52–79 | 36 | 0.08 | 0.51 ** |
| Total cholesterol (mmol/L) | 4.08, 3.35–5.38 | 4.44, 3.59–6.09 | 36 | 0.39 | 0.49 ** |
| HDL cholesterol (mmol/L) | 1.24, 0.81–1.45 | 1.31, 0.94–1.39 | 36 | 0.88 | 0.09 |
| LDL cholesterol (mmol/L) | 1.598, 1.268–2.154 | 1.845, 1.221–2.306 | 36 | 0.64 | 0.45 ** |
| Serum triglycerides (mmol/L) | 1.258, 1.144–1.977 | 1.869, 1.273–2.669 | 36 | 0.21 | 0.81 *** |
| GlycA (mmol/L) | 1.336, 1.289–1.406 | 1.580, 1.410–1.694 | 36 | 0.04 | 1 *** |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dierckx, T.; Chiche, L.; Daniel, L.; Lauwerys, B.; Van Weyenbergh, J.; Jourde-Chiche, N. Serum GlycA Level Is Elevated in Active Systemic Lupus Erythematosus and Correlates to Disease Activity and Lupus Nephritis Severity. J. Clin. Med. 2020, 9, 970. https://doi.org/10.3390/jcm9040970
Dierckx T, Chiche L, Daniel L, Lauwerys B, Van Weyenbergh J, Jourde-Chiche N. Serum GlycA Level Is Elevated in Active Systemic Lupus Erythematosus and Correlates to Disease Activity and Lupus Nephritis Severity. Journal of Clinical Medicine. 2020; 9(4):970. https://doi.org/10.3390/jcm9040970
Chicago/Turabian StyleDierckx, Tim, Laurent Chiche, Laurent Daniel, Bernard Lauwerys, Johan Van Weyenbergh, and Noémie Jourde-Chiche. 2020. "Serum GlycA Level Is Elevated in Active Systemic Lupus Erythematosus and Correlates to Disease Activity and Lupus Nephritis Severity" Journal of Clinical Medicine 9, no. 4: 970. https://doi.org/10.3390/jcm9040970
APA StyleDierckx, T., Chiche, L., Daniel, L., Lauwerys, B., Van Weyenbergh, J., & Jourde-Chiche, N. (2020). Serum GlycA Level Is Elevated in Active Systemic Lupus Erythematosus and Correlates to Disease Activity and Lupus Nephritis Severity. Journal of Clinical Medicine, 9(4), 970. https://doi.org/10.3390/jcm9040970