Associations between the Quality of Life and Nasal Polyp Size in Patients Suffering from Chronic Rhinosinusitis without Nasal Polyps, with Nasal Polyps or Aspirin-Exacerbated Respiratory Disease

 , , , ,
, , , , 
Abstract
1. Introduction
2. Experimental Section
2.1. Study Population
2.2. Outcome Measures
2.3. Statistical Analysis
3. Results
3.1. Patient Characteristics
3.2. Highest TPS and SNOT-20 GAV Scores were Observed in Patients suffering from AERD
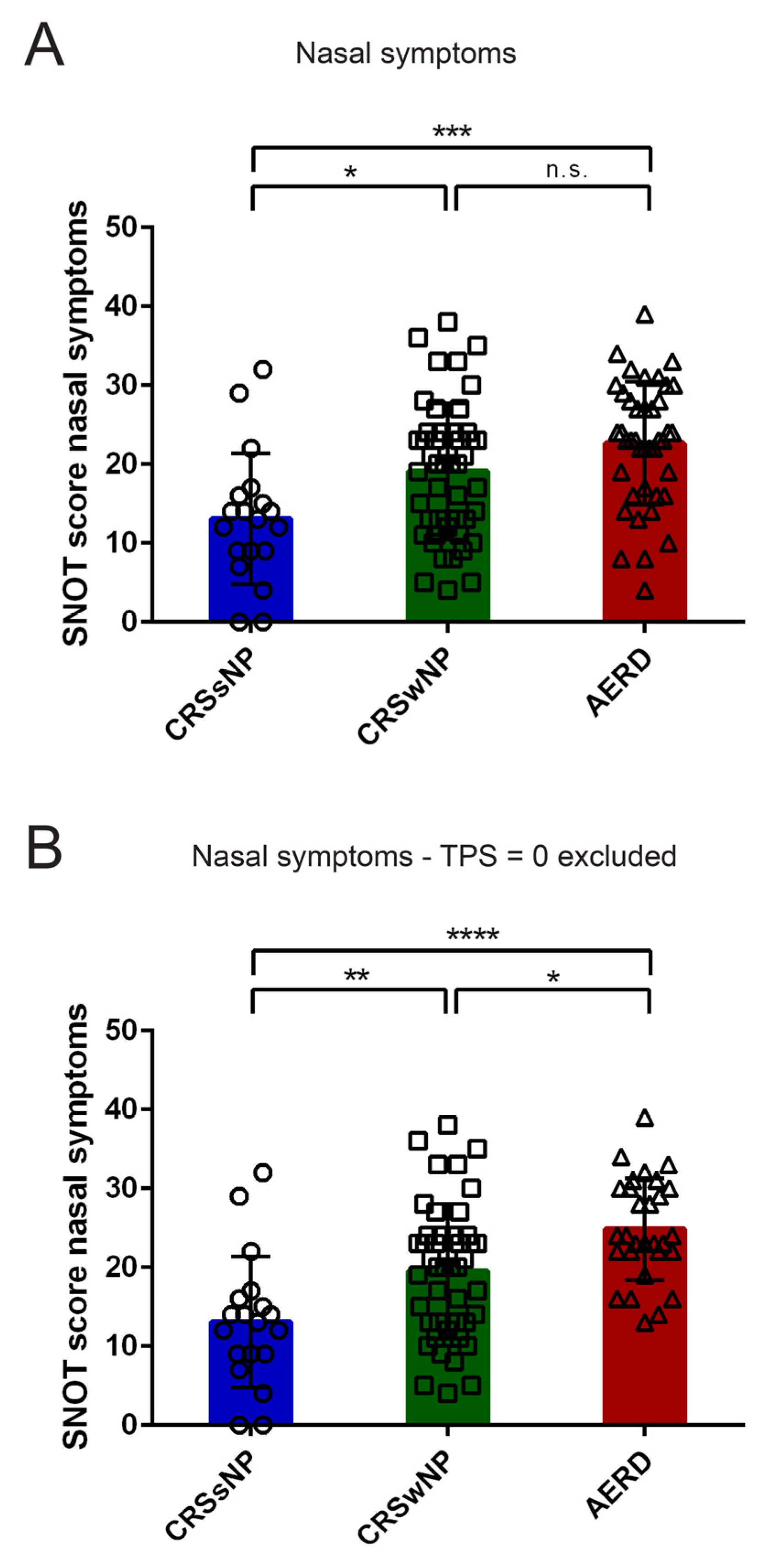
3.3. AERD Patients Suffer More from Nasal Symptoms as Compared to CRSsNP and CRSwNP Patients
3.4. Quality of Life in AERD and CRSwNP Patients after Surgery in a Subset of Patients
3.5. Correlation of TPS with Nasal Symptoms in Patients with AERD but not with CRSwNP
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- DeConde, A.S.; Soler, Z.M. Chronic rhinosinusitis: Epidemiology and burden of disease. Am. J. Rhinol. Allergy 2016, 30, 134–139. [Google Scholar] [CrossRef] [PubMed]
- Hastan, D.; Fokkens, W.J.; Bachert, C.; Newson, R.B.; Bislimovska, J.; Bockelbrink, A.; Bousquet, P.J.; Brozek, G.; Bruno, A.; Dahlen, S.E.; et al. Chronic rhinosinusitis in europe—An underestimated disease. A ga(2)len study. Allergy 2011, 66, 1216–1223. [Google Scholar] [CrossRef]
- Chen, Y.; Dales, R.; Lin, M. The epidemiology of chronic rhinosinusitis in canadians. Laryngoscope 2003, 113, 1199–1205. [Google Scholar] [CrossRef] [PubMed]
- Bachert, C.; Akdis, C.A. Phenotypes and emerging endotypes of chronic rhinosinusitis. J. Allergy Clin. Immunol. Pract. 2016, 4, 621–628. [Google Scholar] [CrossRef] [PubMed]
- Fokkens, W.J.; Lund, V.J.; Hopkins, C.; Hellings, P.W.; Kern, R.; Reltsma, S.; Toppila-Salmi, S.; Bernal-Sprekelsen, M.; Mullol, J.; Alobid, I.; et al. European position paper on rhinosinusitis and nasal polyps 2020. Rhinology 2020, 58 (Suppl. S29), 1–464. [Google Scholar] [CrossRef]
- Rajan, J.P.; Wineinger, N.E.; Stevenson, D.D.; White, A.A. Prevalence of aspirin-exacerbated respiratory disease among asthmatic patients: A meta-analysis of the literature. J. Allergy Clin. Immunol. 2015, 135, 676–681.e671. [Google Scholar] [CrossRef] [PubMed]
- Ting, F.; Hopkins, C. Outcome measures in chronic rhinosinusitis. Curr. Otorhinolaryngol. Rep. 2018, 6, 271–275. [Google Scholar] [CrossRef]
- Psaltis, A.J.; Li, G.; Vaezeafshar, R.; Cho, K.S.; Hwang, P.H. Modification of the lund-kennedy endoscopic scoring system improves its reliability and correlation with patient-reported outcome measures. Laryngoscope 2014, 124, 2216–2223. [Google Scholar] [CrossRef]
- Meltzer, E.O.; Hamilos, D.L.; Hadley, J.A.; Lanza, D.C.; Marple, B.F.; Nicklas, R.A.; Adinoff, A.D.; Bachert, C.; Borish, L.; Chinchilli, V.M.; et al. Rhinosinusitis: Developing guidance for clinical trials. J. Allergy Clin. Immunol. 2006, 118, S17–S61. [Google Scholar] [CrossRef]
- Bachert, C.; Mannent, L.; Naclerio, R.M.; Mullol, J.; Ferguson, B.J.; Gevaert, P.; Hellings, P.; Jiao, L.; Wang, L.; Evans, R.R.; et al. Effect of subcutaneous dupilumab on nasal polyp burden in patients with chronic sinusitis and nasal polyposis: A randomized clinical trial. JAMA 2016, 315, 469–479. [Google Scholar] [CrossRef]
- Gevaert, P.; Calus, L.; Van Zele, T.; Blomme, K.; De Ruyck, N.; Bauters, W.; Hellings, P.; Brusselle, G.; De Bacquer, D.; van Cauwenberge, P.; et al. Omalizumab is effective in allergic and nonallergic patients with nasal polyps and asthma. J. Allergy Clin. Immunol. 2013, 131, 110–116.e111. [Google Scholar] [CrossRef] [PubMed]
- Piccirillo, J.F.; Merritt, M.G., Jr.; Richards, M.L. Psychometric and clinimetric validity of the 20-item sino-nasal outcome test (snot-20). Otolaryngol. Head Neck Surg. 2002, 126, 41–47. [Google Scholar] [CrossRef] [PubMed]
- Gray, S.T.; Phillips, K.M.; Hoehle, L.P.; Caradonna, D.S.; Sedaghat, A.R. The 22-item sino-nasal outcome test accurately reflects patient-reported control of chronic rhinosinusitis symptomatology. Int. Forum Allergy Rhinol. 2017, 7, 945–951. [Google Scholar] [CrossRef] [PubMed]
- Morley, A.D.; Sharp, H.R. A review of sinonasal outcome scoring systems—Which is best? Clin. Otolaryngol. 2006, 31, 103–109. [Google Scholar] [CrossRef] [PubMed]
- Baumann, I.; Plinkert, P.K.; De Maddalena, H. Development of a grading scale for the sino-nasal outcome test-20 german adapted version (snot-20 gav). HNO 2008, 56, 784–788. [Google Scholar] [CrossRef]
- Hopkins, C.; Browne, J.P.; Slack, R.; Lund, V.; Brown, P. The lund-mackay staging system for chronic rhinosinusitis: How is it used and what does it predict? Otolaryngol. Head Neck Surg. 2007, 137, 555–561. [Google Scholar] [CrossRef]
- Dejaco, D.; Riedl, D.; Huber, A.; Moschen, R.; Giotakis, A.I.; Bektic-Tadic, L.; Steinbichler, T.; Kahler, P.; Riechelmann, H. The snot-22 factorial structure in european patients with chronic rhinosinusitis: New clinical insights. Eur. Arch. Otorhinolaryngol. 2019, 276, 1355–1365. [Google Scholar] [CrossRef]
- Ryan, W.R.; Ramachandra, T.; Hwang, P.H. Correlations between symptoms, nasal endoscopy, and in-office computed tomography in post-surgical chronic rhinosinusitis patients. Laryngoscope 2011, 121, 674–678. [Google Scholar] [CrossRef]
- Sedaghat, A.R.; Gray, S.T.; Caradonna, S.D.; Caradonna, D.S. Clustering of chronic rhinosinusitis symptomatology reveals novel associations with objective clinical and demographic characteristics. Am. J. Rhinol. Allergy 2015, 29, 100–105. [Google Scholar] [CrossRef]
- DeConde, A.S.; Bodner, T.E.; Mace, J.C.; Alt, J.A.; Rudmik, L.; Smith, T.L. Development of a clinically relevant endoscopic grading system for chronic rhinosinusitis using canonical correlation analysis. Int. Forum Allergy Rhinol. 2016, 6, 478–485. [Google Scholar] [CrossRef]
- Jang, D.W.; Comer, B.T.; Lachanas, V.A.; Kountakis, S.E. Aspirin sensitivity does not compromise quality-of-life outcomes in patients with samter’s triad. Laryngoscope 2014, 124, 34–37. [Google Scholar] [CrossRef] [PubMed]
- Gudziol, V.; Michel, M.; Sonnefeld, C.; Koschel, D.; Hummel, T. Olfaction and sinonasal symptoms in patients with CRSwNP and AERD and without AERD: A cross-sectional and longitudinal study. Eur. Arch. Otorhinolaryngol. 2017, 274, 1487–1493. [Google Scholar] [CrossRef] [PubMed]
- Katotomichelakis, M.; Riga, M.; Davris, S.; Tripsianis, G.; Simopoulou, M.; Nikolettos, N.; Simopoulos, K.; Danielides, V. Allergic rhinitis and aspirin-exacerbated respiratory disease as predictors of the olfactory outcome after endoscopic sinus surgery. Am. J. Rhinol. Allergy 2009, 23, 348–353. [Google Scholar] [CrossRef] [PubMed]
- DeConde, A.S.; Mace, J.C.; Levy, J.M.; Rudmik, L.; Alt, J.A.; Smith, T.L. Prevalence of polyp recurrence after endoscopic sinus surgery for chronic rhinosinusitis with nasal polyposis. Laryngoscope 2017, 127, 550–555. [Google Scholar] [CrossRef]
- Morrissey, D.K.; Bassiouni, A.; Psaltis, A.J.; Naidoo, Y.; Wormald, P.J. Outcomes of modified endoscopic Lothrop in aspirin-exacerbated respiratory disease with nasal polyposis. Int. Forum Allergy Rhinol. 2016, 6, 820–825. [Google Scholar] [CrossRef]
- Kowalski, M.L.; Agache, I.; Bavbek, S.; Bakirtas, A.; Blanca, M.; Bochenek, G.; Bonini, M.; Heffler, E.; Klimek, L.; Laidlaw, T.M.; et al. Diagnosis and management of nsaid-exacerbated respiratory disease (n-erd)-a eaaci position paper. Allergy 2019, 74, 28–39. [Google Scholar] [CrossRef]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences; Academic Press: New York, NY, USA, 2012; pp. 1–579. [Google Scholar]
- Greguric, T.; Trkulja, V.; Baudoin, T.; Grgic, M.; Smigovec, I.; Kalogjera, L. Differences in the sino-nasal outcome test 22 and visual analog scale symptom scores in chronic rhinosinusitis with and without nasal polyps. Am. J. Rhinol. Allergy 2016, 30, 107–112. [Google Scholar] [CrossRef]
- Dietz de Loos, D.A.; Hopkins, C.; Fokkens, W.J. Symptoms in chronic rhinosinusitis with and without nasal polyps. Laryngoscope 2013, 123, 57–63. [Google Scholar] [CrossRef]
- Sweet, J.M.; Stevenson, D.D.; Simon, R.A.; Mathison, D.A. Long-term effects of aspirin desensitization--treatment for aspirin-sensitive rhinosinusitis-asthma. J. Allergy Clin. Immunol. 1990, 85, 59–65. [Google Scholar] [CrossRef]
- Berges-Gimeno, M.P.; Simon, R.A.; Stevenson, D.D. Long-term treatment with aspirin desensitization in asthmatic patients with aspirin-exacerbated respiratory disease. J. Allergy Clin. Immunol. 2003, 111, 180–186. [Google Scholar] [CrossRef]
- Cho, K.S.; Soudry, E.; Psaltis, A.J.; Nadeau, K.C.; McGhee, S.A.; Nayak, J.V.; Hwang, P.H. Long-term sinonasal outcomes of aspirin desensitization in aspirin exacerbated respiratory disease. Otolaryngol. Head Neck Surg. 2014, 151, 575–581. [Google Scholar] [CrossRef] [PubMed]
- Cooper, T.; Greig, S.R.; Zhang, H.; Seemann, R.; Wright, E.D.; Vliagoftis, H.; Cote, D.W.J. Objective and subjective sinonasal and pulmonary outcomes in aspirin desensitization therapy: A prospective cohort study. Auris Nasus Larynx 2019, 46, 526–532. [Google Scholar] [CrossRef] [PubMed]
- Ren, L.; Zhang, N.; Zhang, L.; Bachert, C. Biologics for the treatment of chronic rhinosinusitis with nasal polyps-state of the art. World Allergy Organ. J. 2019, 12, 100050. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| CRSsNP (n = 19) | CRSwNP (n = 47) | AERD (n = 41) | ||
|---|---|---|---|---|
| Gender (m/f) | 15/4 | 31/16 | 18/23 | |
| Age | ||||
| mean | 44.11 | 47.62 | 45.41 | |
| range | 21–69 | 21–79 | 18–70 | |
| Total polyp score | ||||
| mean | 0.00 | 3.40 | 4.02 | |
| range | 0 | 0–8 | 0–8 | |
| Total SNOT score | ||||
| mean | 30.89 | 36.31 | 43.41 | |
| range | 4–73 | 11–76 | 6–95 | |
| History of prior surgery (y/n) | 5/14 | 23/24 | 38/3 | |
| Average Value ± Standard Deviation | p-Value of Pairwise Comparison | |||||
|---|---|---|---|---|---|---|
| CRSsNP | CRSwNP | AERD | CRSsNP-CRSwNP | CRSsNP-AERD | CRSwNP-AERD | |
| Total polyp score | 0 ± 0 | 3.40 ± 2.01 | 4.02 ± 2.89 | <0.0001 | <0.0001 | 0.3985 |
| Total SNOT-20 GAV score | 30.89 ± 19.92 | 36.32 ± 18.17 | 43.41 ± 19.23 | 0.5434 | 0.0488 | 0.1891 |
| Total SNOT-20 GAV score if patients with TPS = 0 excluded | N/A | 37.24 ± 18.01 | 49.14 ± 17.03 | 0.0028 | 0.0192 | |
| All Patients | CRSwNP | AERD | |||||
|---|---|---|---|---|---|---|---|
| r | p-value | r | p-value | r | p-value | ||
| Total SNOT score | 0.29 | 0.0056 | 0.34 | 0.0195 | 0.23 | 0.1407 | |
| Nasal symptoms | 0.32 | 0.0024 | 0.24 | 0.1063 | 0.37 | 0.0160 | |
| Need to clear throat/dry throat | 0.06 | 0.6112 | 0.22 | 0.1431 | −0.10 | 0.5424 | |
| Sneezing | 0.27 | 0.0108 | 0.16 | 0.2905 | 0.31 | 0.0462 | |
| Runny nose | 0.22 | 0.0423 | 0.06 | 0.6753 | 0.35 | 0.0279 | |
| Cough | 0.06 | 0.5892 | 0.09 | 0.5571 | −0.01 | 0.9689 | |
| Post-nasal discharge | 0.10 | 0.3560 | 0.02 | 0.9063 | 0.14 | 0.3793 | |
| Thick nasal discharge | 0.20 | 0.0627 | 0.20 | 0.1916 | 0.18 | 0.2631 | |
| Sense of smell | 0.33 | 0.0017 | 0.25 | 0.0974 | 0.42 | 0.0066 | |
| Blockage/Congestion of nose | 0.53 | <0.0001 | 0.40 | 0.0051 | 0.65 | <0.0001 | |
| Otological symptoms | 0.11 | 0.3038 | 0.21 | 0.1551 | 0.01 | 0.9412 | |
| Ear congestion | 0.10 | 0.3405 | 0.04 | 0.7751 | 0.11 | 0.4821 | |
| Dizziness | 0.09 | 0.3917 | 0.31 | 0.0361 | −0.08 | 0.6082 | |
| Ear pain | 0.07 | 0.5225 | 0.12 | 0.4170 | 0.03 | 0.8549 | |
| Facial pain/pressure | 0.06 | 0.5882 | 0.17 | 0.2444 | −0.05 | 0.7478 | |
| Sleep symptoms | 0.22 | 0.0374 | 0.32 | 0.0289 | 0.13 | 0.4143 | |
| Difficulty falling asleep | 0.20 | 0.0548 | 0.32 | 0.0280 | 0.14 | 0.3932 | |
| Waking up at night | 0.14 | 0.1814 | 0.23 | 0.1234 | 0.10 | 0.5436 | |
| Fatigued or tired during the day | 0.21 | 0.0465 | 0.28 | 0.0600 | 0.12 | 0.4448 | |
| Reduced productivity | 0.22 | 0.0360 | 0.30 | 0.0392 | 0.14 | 0.3974 | |
| Reduced concentration | 0.20 | 0.0694 | 0.25 | 0.0958 | 0.15 | 0.3474 | |
| Frustration, restlessness, irritability | 0.08 | 0.4867 | 0.15 | 0.3283 | 0.04 | 0.8043 | |
| Emotional symptoms | 0.27 | 0.0106 | 0.33 | 0.0246 | 0.21 | 0.1835 | |
| Sad | 0.23 | 0.0299 | 0.29 | 0.0470 | 0.16 | 0.3105 | |
| Embarrassed | 0.21 | 0.0516 | 0.25 | 0.0938 | 0.18 | 0.2679 | |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Schneider, S.; Campion, N.J.; Villazala-Merino, S.; Liu, D.T.; Bartosik, T.; Landegger, L.D.; Ahmadi, N.; Mueller, C.A.; Vyskocil, E.; Stanek, V.; et al. Associations between the Quality of Life and Nasal Polyp Size in Patients Suffering from Chronic Rhinosinusitis without Nasal Polyps, with Nasal Polyps or Aspirin-Exacerbated Respiratory Disease. J. Clin. Med. 2020, 9, 925. https://doi.org/10.3390/jcm9040925
Schneider S, Campion NJ, Villazala-Merino S, Liu DT, Bartosik T, Landegger LD, Ahmadi N, Mueller CA, Vyskocil E, Stanek V, et al. Associations between the Quality of Life and Nasal Polyp Size in Patients Suffering from Chronic Rhinosinusitis without Nasal Polyps, with Nasal Polyps or Aspirin-Exacerbated Respiratory Disease. Journal of Clinical Medicine. 2020; 9(4):925. https://doi.org/10.3390/jcm9040925
Chicago/Turabian StyleSchneider, Sven, Nicholas J. Campion, Sergio Villazala-Merino, David Tianxiang Liu, Tina Bartosik, Lukas D. Landegger, Navid Ahmadi, Christian A. Mueller, Erich Vyskocil, Victoria Stanek, and et al. 2020. "Associations between the Quality of Life and Nasal Polyp Size in Patients Suffering from Chronic Rhinosinusitis without Nasal Polyps, with Nasal Polyps or Aspirin-Exacerbated Respiratory Disease" Journal of Clinical Medicine 9, no. 4: 925. https://doi.org/10.3390/jcm9040925
APA StyleSchneider, S., Campion, N. J., Villazala-Merino, S., Liu, D. T., Bartosik, T., Landegger, L. D., Ahmadi, N., Mueller, C. A., Vyskocil, E., Stanek, V., Quint, T., Bangert, C., & Eckl-Dorna, J. (2020). Associations between the Quality of Life and Nasal Polyp Size in Patients Suffering from Chronic Rhinosinusitis without Nasal Polyps, with Nasal Polyps or Aspirin-Exacerbated Respiratory Disease. Journal of Clinical Medicine, 9(4), 925. https://doi.org/10.3390/jcm9040925