Iron Deficiency: Impact on Functional Capacity and Quality of Life in Heart Failure with Preserved Ejection Fraction

 , , , , , and
, , , , , and
Abstract
1. Introduction
2. Methods
2.1. Study Design and Population
2.2. Study Definitions
2.3. Statistical Analysis
3. Results
3.1. Baseline Characteristics
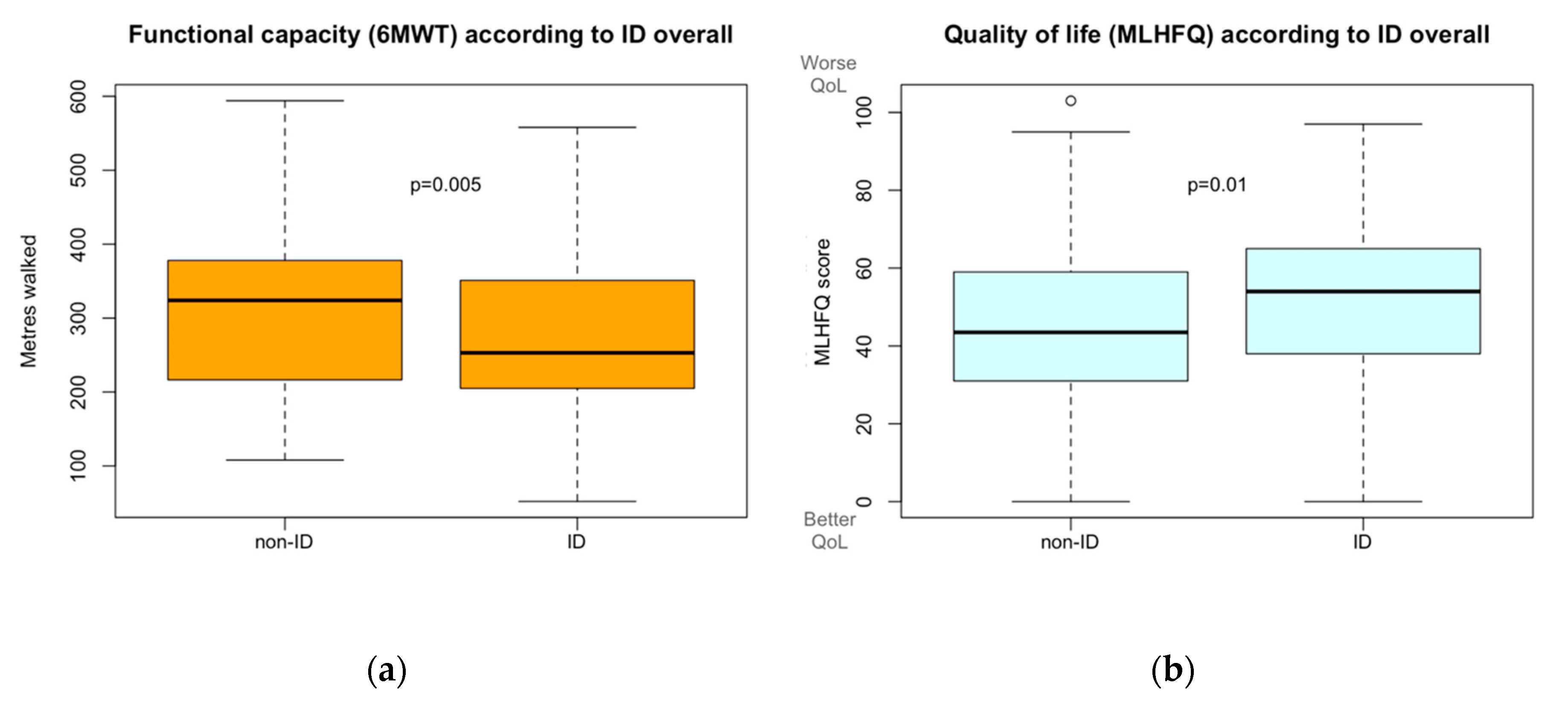
3.2. Functional Capacity and Iron Deficiency
3.3. Quality of Life and Iron Deficiency
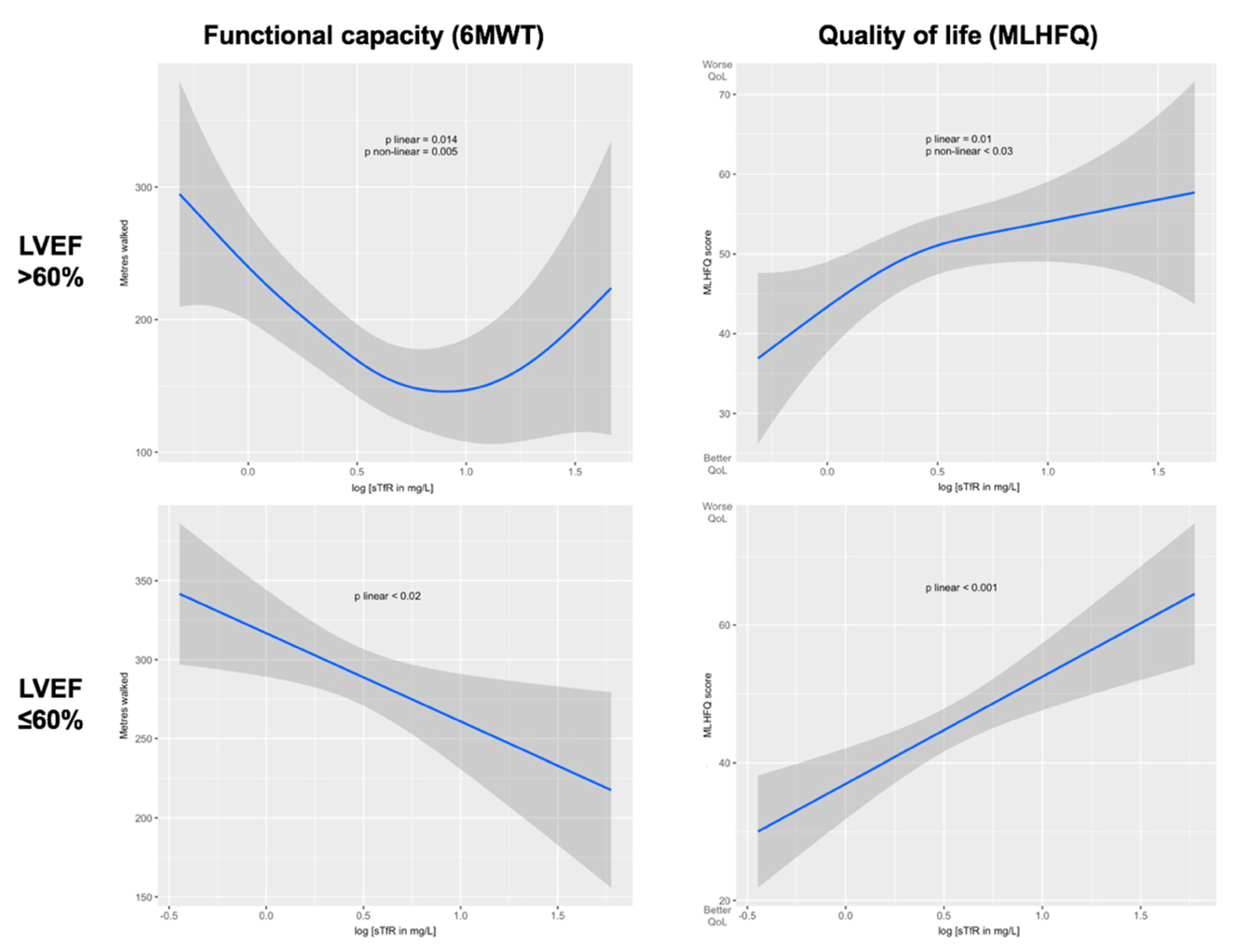
3.4. Linear Regression Predictive Models
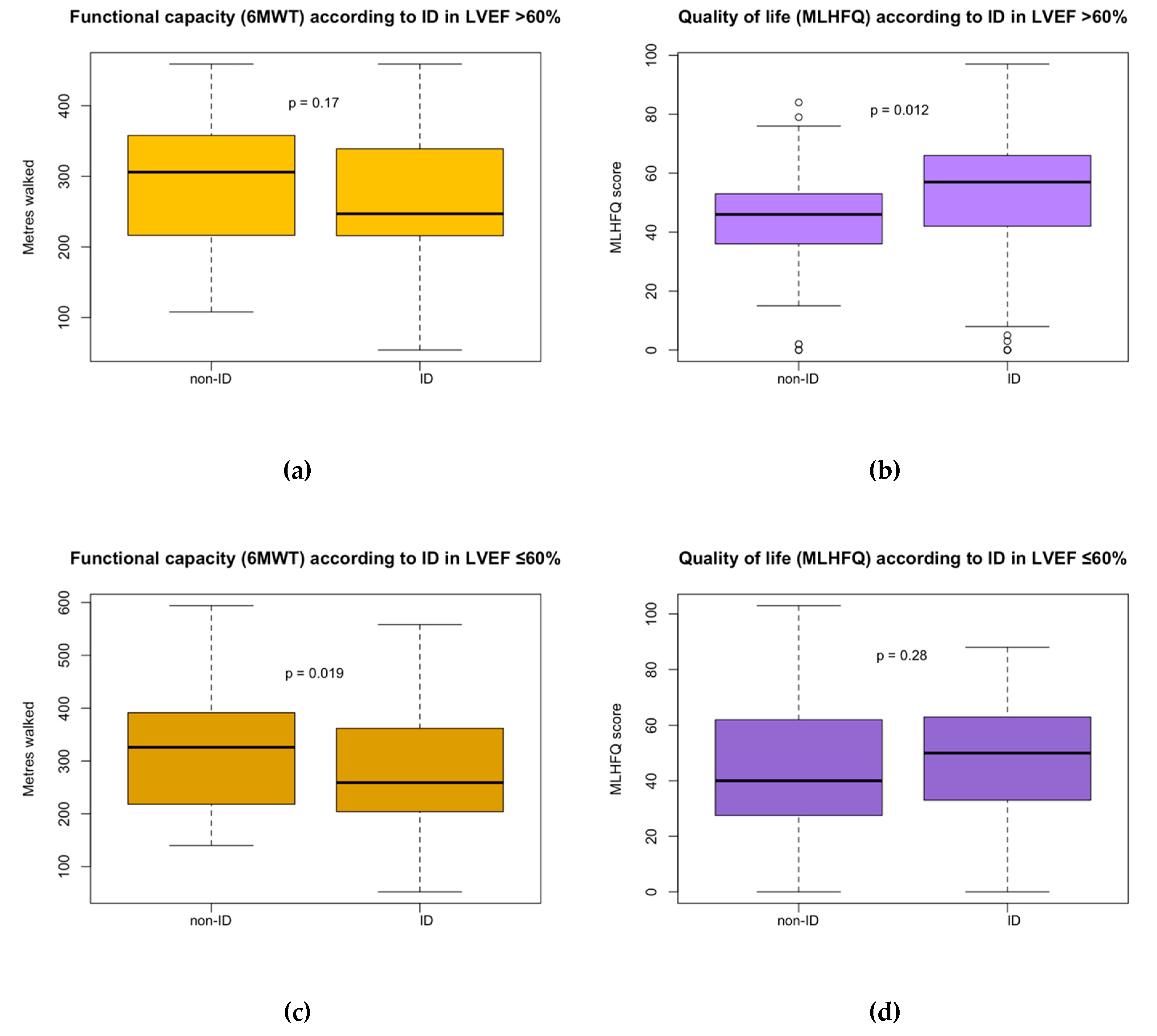
3.5. Differences within HFpEF according to LVEF
4. Discussion
4.1. Functional Capacity Impairment and Quality of Life Worsening by Iron Deficiency
4.2. Iron Deficiency in HFpEF according to LVEF
4.3. Clinical Implications
4.4. Limitations of the Study
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Dunlay, S.M.; Roger, V.L.; Redfield, M.M. Epidemiology of heart failure with preserved ejection fraction. Nat. Rev. Cardiol. 2017, 14, 591–602. [Google Scholar] [CrossRef] [PubMed]
- Farre, N.; Vela, E.; Clèries, M.; Bustins, M.; Cainzos-Achirica, M.; Enjuanes, C.; Moliner, P.; Ruiz, S.; Rotellar, J.M.V.; Comín-Colet, J. Real world heart failure epidemiology and outcome: A population-based analysis of 88,195 patients. PLoS ONE 2017, 12, e0172745. [Google Scholar] [CrossRef] [PubMed]
- Aragam, K.G.; Chaffin, M.D.; Levinson, R.T.; McDermott, G.; Choi, S.-H.; Shoemaker, M.B.; Haas, M.E.; Weng, L.-C.; Lindsay, M.E.; Smith, J.G.; et al. Phenotypic refinement of heart failure in a national biobank facilitates genetic discovery. Circulation 2019, 139, 489–501. [Google Scholar] [CrossRef] [PubMed]
- Shah, S.J.; Kitzman, D.W.; Borlaug, B.A.; Van Heerebeek, L.; Zile, M.R.; Kass, D.A.; Paulus, W.J. Phenotype-specific treatment of heart failure with preserved ejection fraction. Circulation 2016, 134, 73–90. [Google Scholar] [CrossRef] [PubMed]
- McMurray, J.J.; Packer, M.; Desai, A.S.; Gong, J.; Lefkowitz, M.P.; Rizkala, A.R.; Rouleau, J.; Shi, V.C.; Solomon, S.D.; Swedberg, K.; et al. Angiotensin-neprilysin inhibition versus enalapril in heart failure. N. Engl. J. Med. 2014, 371, 993–1004. [Google Scholar] [CrossRef] [PubMed]
- Ponikowski, P.; Voors, A.A.; Anker, S.D.; Bueno, H.; Cleland, J.G.; Coats, A.J.; Falk, V.; González-Juanatey, J.R.; Harjola, V.-P.; Jankowska, E.A.; et al. 2016 ESC guidelines for the diagnosis and treatment of acute and chronic heart failure. Eur. Heart J. 2016, 37, 2129–2200. [Google Scholar] [CrossRef]
- Silverman, D.N.; Shah, S.J. Treatment of heart failure with preserved ejection fraction (HFpEF): The phenotype-guided approach. Curr. Treat. Options Cardiovasc. Med. 2019, 21, 20. [Google Scholar] [CrossRef]
- Shah, S.J.; Borlaug, B.A.; Kitzman, D.W.; McCulloch, A.D.; Blaxall, B.C.; Agarwal, R.; Chirinos, J.A.; Collins, S.; Deo, R.C.; Gladwin, M.T.; et al. Research priorities for heart failure with preserved ejection fraction. Circulation 2020, 141, 1001–1026. [Google Scholar] [CrossRef]
- Solomon, S.D.; McMurray, J.J.; Anand, I.S.; Ge, J.; Lam, C.S.; Maggioni, A.P.; Martinez, F.; Packer, M.; Pfeffer, M.A.; Pieske, B.; et al. Angiotensin-neprilysin inhibition in heart failure with preserved ejection fraction. N. Engl. J. Med. 2019, 381, 1609–1620. [Google Scholar] [CrossRef]
- Martens, P.; Nijst, P.; Verbrugge, F.H.; Smeets, K.; Dupont, M.; Mullens, W. Impact of iron deficiency on exercise capacity and outcome in heart failure with reduced, mid-range and preserved ejection fraction. Acta Cardiol. 2017, 73, 115–123. [Google Scholar] [CrossRef]
- Lewis, G.D.; Malhotra, R.; Hernandez, A.F.; McNulty, S.E.; Smith, A.; Felker, G.M.; Tang, W.H.W.; LaRue, S.J.; Redfield, M.M.; Semigran, M.J.; et al. Effect of oral iron repletion on exercise capacity in patients with heart failure with reduced ejection fraction and iron deficiency: The IRONOUT HF randomized clinical trial. JAMA 2017, 317, 1958–1966. [Google Scholar] [CrossRef] [PubMed]
- Beale, A.; Carballo, D.; Stirnemann, J.; Garin, N.; Agoritsas, T.; Serratrice, J.; Kaye, D.M.; Meyer, P.; Carballo, S.; Carballo, D. Iron deficiency in acute decompensated heart failure. J. Clin. Med. 2019, 8, 1569. [Google Scholar] [CrossRef] [PubMed]
- Beattie, J.M.; Khatib, R.; Phillips, C.J.; Williams, S.G. Iron deficiency in 78,805 people admitted with heart failure across England: A retrospective cohort study. Open Heart 2020, 7, e001153. [Google Scholar] [CrossRef] [PubMed]
- Núñez, J.; Monmeneu, J.V.; Mollar, A.; Núñez, E.; Bodí, V.; Miñana, G.; García-Blas, S.; Santas, E.; Aguero, J.; Chorro, F.J.; et al. Left ventricular ejection fraction recovery in patients with heart failure treated with intravenous iron: A pilot study. ESC Heart Fail. 2016, 3, 293–298. [Google Scholar] [CrossRef]
- Moliner, P.; A Jankowska, E.; Van Veldhuisen, D.J.; Farre, N.; Rozentryt, P.; Enjuanes, C.; Polonski, L.; Meroño, O.; Voors, A.A.; Ponikowski, P.; et al. Clinical correlates and prognostic impact of impaired iron storage versus impaired iron transport in an international cohort of 1821 patients with chronic heart failure. Int. J. Cardiol. 2017, 243, 360–366. [Google Scholar] [CrossRef]
- McDonagh, T.; MacDougall, I.C. Iron therapy for the treatment of iron deficiency in chronic heart failure: Intravenous or oral? Eur. J. Heart Fail. 2015, 17, 248–262. [Google Scholar] [CrossRef]
- McDonagh, T.; Damy, T.; Doehner, W.; Lam, C.S.; Sindone, A.; Van Der Meer, P.; Cohen-Solal, A.; Kindermann, I.; Manito, N.; Pfister, O.; et al. Screening, diagnosis and treatment of iron deficiency in chronic heart failure: Putting the 2016 European society of cardiology heart failure guidelines into clinical practice. Eur. J. Heart Fail. 2018, 20, 1664–1672. [Google Scholar] [CrossRef]
- Enjuanes, C.; Bruguera, J.; Grau, M.; Cladellas, M.; Gonzalez, G.; Meroño, O.; Moliner-Borja, P.; Verdú, J.M.; Farre, N.; Lupón, J. Iron status in chronic heart failure: Impact on symptoms, functional class and submaximal exercise capacity. Rev. Esp. Cardiol. 2016, 69, 247–255. [Google Scholar] [CrossRef]
- Comin-Colet, J.; Enjuanes, C.; Gonzalez, G.; Torrens, A.; Cladellas, M.; Meroño, O.; Ribas, N.; Ruiz, S.; Gomez, M.; Verdú, J.M.; et al. Iron deficiency is a key determinant of health-related quality of life in patients with chronic heart failure regardless of anaemia status. Eur. J. Heart Fail. 2013, 15, 1164–1172. [Google Scholar] [CrossRef]
- Beale, A.; Warren, J.L.; Roberts, N.; Meyer, P.; Townsend, N.; Kaye, D. Iron deficiency in heart failure with preserved ejection fraction: A systematic review and meta-analysis. Open Heart 2019, 6, e001012. [Google Scholar] [CrossRef]
- Núñez, J.; Dominguez, E.; Ramón, J.M.; Núñez, E.; Sanchis, J.; Santas, E.; Heredia, R.; González, J.; Minana, G.; López, L.; et al. Iron deficiency and functional capacity in patients with advanced heart failure with preserved ejection fraction. Int. J. Cardiol. 2016, 207, 365–367. [Google Scholar] [CrossRef]
- Bekfani, T.; Pellicori, P.; Morris, D.; Ebner, N.; Valentova, M.; Sandek, A.; Doehner, W.; Cleland, J.G.; Lainscak, M.; Schulze, P.C.; et al. Iron deficiency in patients with heart failure with preserved ejection fraction and its association with reduced exercise capacity, muscle strength and quality of life. Clin. Res. Cardiol. 2018, 108, 203–211. [Google Scholar] [CrossRef] [PubMed]
- KDOQI; National Kidney Foundation. KDOQI clinical practice guidelines and clinical practice recommendations for Anemia in chronic kidney disease. Am. J. Kidney Dis. 2006, 47. [Google Scholar] [CrossRef]
- Anker, S.D.; Lupón, J.; Filippatos, G.; Willenheimer, R.; Dickstein, K.; Drexler, H.; Lüscher, T.F.; Bart, B.; Banasiak, W.; Niegowska, J.; et al. Ferric carboxymaltose in patients with heart failure and iron deficiency. N. Engl. J. Med. 2009, 361, 2436–2448. [Google Scholar] [CrossRef] [PubMed]
- Naito, Y.; Tsujino, T.; Matsumoto, M.; Sakoda, T.; Ohyanagi, M.; Masuyama, T. Adaptive response of the heart to long-term anemia induced by iron deficiency. Am. J. Physiol. Circ. Physiol. 2009, 296, H585–H593. [Google Scholar] [CrossRef]
- Houstis, N.E.; Eisman, A.S.; Pappagianopoulos, P.P.; Wooster, L.; Bailey, C.S.; Wagner, P.D.; Lewis, G.D. Exercise intolerance in heart failure with preserved ejection fraction: Diagnosing and ranking its causes using personalized O2 pathway analysis. Circulation 2017, 137, 148–161. [Google Scholar] [CrossRef]
- Wijk, S.S.-V.; Van Empel, V.; Davarzani, N.; Maeder, M.T.; Handschin, R.; Pfisterer, M.E.; Rocca, H.P.B.-L.; TIME-CHF Investigators. Circulating biomarkers of distinct pathophysiological pathways in heart failure with preserved vs. reduced left ventricular ejection fraction. Eur. J. Heart Fail. 2015, 17, 1006–1014. [Google Scholar] [CrossRef]
- Paulus, W.J.; Tschöpe, C. A novel paradigm for heart failure with preserved ejection fraction. J. Am. Coll. Cardiol. 2013, 62, 263–271. [Google Scholar] [CrossRef]
- Weiss, G.; Goodnough, L.T. Anemia of chronic disease. N. Engl. J. Med. 2005, 352, 1011–1023. [Google Scholar] [CrossRef]
- Weber, C.S.; Da Silva, L.B.; Goldraich, L.A.; Biolo, A.; Clausell, N. Anemia in heart failure: Association of hepcidin levels to iron deficiency in stable outpatients. Acta Haematol. 2013, 129, 55–61. [Google Scholar] [CrossRef]
- Von Haehling, S.; Ebner, N.; Evertz, R.; Ponikowski, P.; Anker, S.D. Iron deficiency in heart failure. JACC Heart Fail. 2019, 7, 36–46. [Google Scholar] [CrossRef] [PubMed]
- Perticone, M.; Zito, R.; Miceli, S.; Pinto, A.; Suraci, E.; Greco, M.; Gigliotti, S.; Hribal, M.L.; Corrao, S.; Sesti, G.; et al. Immunity, inflammation and heart failure: Their role on cardiac function and iron status. Front. Immunol. 2019, 10, 2315. [Google Scholar] [CrossRef] [PubMed]
- Ferguson, B.J.; Skikne, B.S.; Simpson, K.M.; Baynes, R.D.; Cook, J.D. Serum transferrin receptor distinguishes the anemia of chronic disease from iron deficiency anemia. J. Lab. Clin. Med. 1992, 119, 385–390. [Google Scholar] [PubMed]
- Skikne, B.S. Serum transferrin receptor. Am. J. Hematol. 2008, 83, 872–875. [Google Scholar] [CrossRef]
- Burton, J.K.; Yates, L.C.; Whyte, L.; Fitzsimons, E.; Stott, D.J. New horizons in iron deficiency anaemia in older adults. Age Ageing 2020. [Google Scholar] [CrossRef]
- Effect of IV Iron in Patients with Heart Failure with Preserved Ejection Fraction (FAIR-HFpEF). Available online: https://clinicaltrials.gov/ct2/show/NCT03074591 (accessed on 25 February 2020).
- Effects of Iron Therapy in Heart Failure with Preserved Ejection Fraction and Iron Deficiency (PREFER-HF). Available online: https://clinicaltrials.gov/ct2/show/NCT03833336 (accessed on 25 February 2020).




{kind=link}
{kind=link}
{kind=link}
| Overall N = 447 | Iron Deficiency N = 325 (73%) | No iron Deficiency N = 122 (27%) | p Value | |
|---|---|---|---|---|
| Age (years) | 75.7 ± 9.2 | 75.7 ± 8.7 | 75.9 ± 10.3 | 0.84 |
| Female sex | 264 (59.1) | 202 (62.2) | 62 (50.8) | 0.039 |
| BMI (kg/m2) | 29.1 ± 6.2 | 29.4 ± 6.3 | 28.5 ± 6.0 | 0.19 |
| Systolic BP (mmHg) | 128.4 ± 21.8 | 127.9 ± 20.6 | 131.6 ± 24.4 | 0.10 |
| Heart rate (bpm) | 73.7 ± 14.4 | 74.0 ± 14.6 | 73.4 ± 14.1 | 0.71 |
| LVEF (%) | 62.1 ± 7.8 | 62.8 ± 7.9 | 60.7 ± 7.3 | 0.011 |
| Ischemic etiology of CHF | 100 (22.4) | 77 (23.7) | 23 (18.9) | 0.33 |
| NYHA functional class | ||||
| I | 47 (10.5) | 31 (9.5) | 16 (13.1) | 0.36 |
| II | 193 (43.2) | 143 (44.0) | 50 (40.9) | 0.64 |
| III | 166 (37.1) | 122 (37.5) | 44 (36.1) | 0.86 |
| IV | 38 (8.5) | 27 (8.3) | 11 (9.0) | 0.96 |
| Comorbidities | ||||
| Hypertension | 391 (87.5) | 290 (89.2) | 101 (82.8) | 0.09 |
| COPD | 93 (20.8) | 67 (20.6) | 26 (21.3) | 0.98 |
| Diabetes mellitus | 221 (49.4) | 175 (53.8) | 46 (37.7) | 0.003 |
| Chronic kidney disease | 282 (63.1) | 208 (64.0) | 74 (60.7) | 0.59 |
| Anemia | 249 (55.7) | 195 (60.0) | 54 (44.3) | 0.004 |
| Dependency | 142 (31.8) | 112 (34.6) | 30 (24.6) | 0.16 |
| Medications | ||||
| ACEIs or ARBs | 300 (67.1) | 212 (65.2) | 88 (72.1) | 0.20 |
| Beta-blockers | 352 (78.7) | 261 (80.3) | 91 (74.6) | 0.24 |
| MRAs | 50 (11.2) | 34 (10.5) | 16 (13.1) | 0.61 |
| Digoxin | 71 (15.9) | 46 (14.2) | 25 (20.5) | 0.14 |
| Loop diuretics | 411 (91.9) | 293 (90.2) | 118 (96.7) | 0.038 |
| Statins | 249 (55.7) | 187 (57.5) | 62 (50.8) | 0.24 |
| Antiplatelets | 155 (34.7) | 115 (35.4) | 40 (32.8) | 0.69 |
| Anticoagulants | 260 (58.2) | 186 (57.2) | 74 (60.7) | 0.58 |
| Laboratory parameters | ||||
| Hemoglobin (g/dL) | 12.26 ± 1.89 | 11.91 ± 1.76 | 12.86 ± 2.03 | <0.001 |
| eGFR (mL/min/1.73 m2) | 55.29 ± 23.78 | 54.08 ± 23.76 | 58.06 ± 23.33 | 0.11 |
| Ferritin (ng/mL) | 141 (70.5–285.0) | 99 (55.0–219.0) | 274.5 (178.75–423) | <0.001 |
| Transferrin (mg/dL) | 248.02 ± 51.58 | 256.10 ± 53.31 | 226.57 ± 39.49 | <0.001 |
| Serum iron (pg/dL) | 61.80 ± 32.90 | 50.83 ± 24.81 | 91.02 ± 34.01 | <0.001 |
| TSAT (%) | 18.61 ± 11.17 | 14.42 ± 6.18 | 29.74 ± 13.60 | <0.001 |
| Ferritin index | 0.95 ± 0.71 | 1.06 ± 0.78 | 0.62 ± 0.27 | <0.001 |
| sTfR (mg/L) | 1.92 ± 1.58 | 2.07 ± 1.79 | 1.51 ± 0.66 | <0.001 |
| NT-proBNP (pg/mL) | 1284 (678–2876) | 1304 (685.5–2827.5) | 1108.5 (642–3303.5) | 0.50 |
| C-reactive protein (mg/dL) | 1.66 ± 2.35 | 1.82 ± 2.57 | 1.23 ± 1.58 | 0.004 |
| Iron Deficiency | No Iron Deficiency | p Value | |
|---|---|---|---|
| 6-min walking test (6MWT) | N = 309 | N = 116 | |
| Meters walked | |||
| Overall, N = 202 and N = 80 | 270.7 ± 94.0 | 310.0 ± 108.9 | 0.005 |
| Non-anemics, N = 94 and N = 50 | 286.8 ± 90.2 | 327.9 ± 112.1 | 0.028 |
| N of subjects that walked >300 m | 72 (35.6) | 47 (58.8) | <0.001 |
| N of subjects unable to complete the test | 59 (29.2) | 13 (16.3) | 0.041 |
| N of subjects that developed symptoms | 77 (38.1) | 22 (27.5) | 0.12 |
| N of subjects unable to undergo the test | 107 (34.6) | 36 (31.0) | 0.56 |
| Minnesota living with HF questionnaire (MLHFQ) | N = 325 | N = 122 | |
| Overall summary score (min: 0, max: 105) | |||
| Overall, N = 325 and N = 122 | 49.4 ± 22.44 | 43.1 ± 23.2 | 0.01 |
| Non-anemics, N = 130 & N = 68 | 46.4 ± 26.4 | 43.8 ± 24.0 | 0.46 |
| Composite scores | |||
| Physical dimension (min: 0, max: 40) (sum of items: 2, 3, 4, 5, 6, 7, 12, 13) | 28.4 ± 12.1 | 25.4 ± 12.7 | 0.025 |
| Emotional dimension (min: 0, max: 25) (sum of items: 17, 18, 19, 20, 21) | 8.2 ± 6.0 | 6.9 ± 6.4 | 0.06 |
| Socioeconomic dimension (min: 0, max: 10) (sum of items: 14, 15) | 4.0 ± 2.7 | 3.5 ± 2.7 | 0.09 |
| Social and personal dimension (min: 0, max: 25) (sum of items: 7, 8, 9, 10, 11) | 8.5 ± 6.7 | 6.9 ± 6.3 | 0.018 |
| Univariate Models | Multivariate Models | |||||
|---|---|---|---|---|---|---|
| β Coef. | p Value | Adj. R2 | β Coef. | p Value | Adj. R2 | |
| 6-Min Walking Test (6MWT) | ||||||
| vs. iron deficiency (KDOQI) | −39.77 | 0.003 | 0.03 | −29.66 | 0.007 | 0.35 |
| vs. iron deficiency (FAIR-HF) | −37.23 | 0.002 | 0.03 | −23.35 | 0.021 | 0.35 |
| vs. anemia (WHO) | −40.90 | <0.001 | 0.04 | −21.10 | 0.035 | 0.34 |
| vs. TSAT < 20% | −36.07 | 0.004 | 0.03 | −28.42 | 0.006 | 0.35 |
| vs. sTfR (log) | −29.51 | 0.056 | 0.01 | −27.09 | 0.035 | 0.36 |
| vs. ferritin (log) | 3.71 | 0.55 | <0.01 | −4.99 | 0.34 | 0.34 |
| vs. serum iron (log) | 29.06 | 0.012 | 0.05 | 9.77 | 0.32 | 0.34 |
| Minnesota Living with Heart Failure Questionnaire (MLHFQ) | ||||||
| vs. iron deficiency (KDOQI) | 6.31 | 0.009 | 0.01 | 4.80 | 0.039 | 0.11 |
| vs. iron deficiency (FAIR−HF) | 4.76 | 0.032 | <0.01 | 2.69 | 0.21 | 0.10 |
| vs. anemia (WHO) | 3.78 | 0.08 | <0.01 | 1.42 | 0.50 | 0.10 |
| vs. TSAT < 20% | 4.99 | 0.029 | <0.01 | 3.32 | 0.13 | 0.10 |
| vs. sTfR (log) | 12.96 | <0.001 | 0.05 | 7.95 | <0.001 | 0.15 |
| vs. ferritin (log) | −0.58 | 0.61 | <0.01 | 0.64 | 0.56 | 0.10 |
| vs. serum iron (log) | −3.76 | 0.08 | <0.01 | −1.50 | 0.47 | 0.10 |
| LVEF > 60% Multivariate Models | LVEF ≤ 60% Multivariate Models | |||||
|---|---|---|---|---|---|---|
| β Coef. | p Value | Adj. R2 | β Coef. | p Value | Adj. R2 | |
| 6 Min Walking Test (6MWT) | ||||||
| vs. iron deficiency (KDOQI) | −18.15 | 0.20 | 0.40 | −37.31 | 0.023 | 0.33 |
| vs. iron deficiency (FAIR−HF) | −14.54 | 0.24 | 0.40 | −31.84 | 0.041 | 0.32 |
| vs. anemia (WHO) | −7.48 | 0.56 | 0.40 | −33.00 | 0.031 | 0.32 |
| vs. TSAT < 20% | −16.53 | 0.23 | 0.40 | −35.19 | 0.023 | 0.33 |
| vs. sTfR (log) | 10.13 | 0.54 | 0.39 | −56.04 | 0.004 | 0.36 |
| vs. ferritin (log) | −3.41 | 0.60 | 0.40 | −5.86 | 0.47 | 0.31 |
| vs. serum iron (log) | 5.51 | 0.66 | 0.40 | 15.77 | 0.29 | 0.31 |
| Minnesota Living with Heart Failure Questionnaire (MLHFQ) | ||||||
| vs. iron deficiency (KDOQI) | 6.80 | 0.037 | 0.15 | 2.77 | 0.41 | 0.05 |
| vs. iron deficiency (FAIR−HF) | 4.72 | 0.11 | 0.14 | 0.80 | 0.80 | 0.05 |
| vs. anemia (WHO) | −0.38 | 0.89 | 0.13 | 2.99 | 0.33 | 0.05 |
| vs. TSAT < 20% | 5.30 | 0.09 | 0.14 | 1.07 | 0.74 | 0.05 |
| vs. sTfR (log) | 5.77 | 0.12 | 0.15 | 14.09 | <0.001 | 0.13 |
| vs. ferritin (log) | −0.79 | 0.60 | 0.13 | 2.16 | 0.18 | 0.05 |
| vs. serum iron (log) | −1.76 | 0.55 | 0.13 | −1.44 | 0.63 | 0.05 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Alcaide-Aldeano, A.; Garay, A.; Alcoberro, L.; Jiménez-Marrero, S.; Yun, S.; Tajes, M.; García-Romero, E.; Díez-López, C.; González-Costello, J.; Mateus-Porta, G.; et al. Iron Deficiency: Impact on Functional Capacity and Quality of Life in Heart Failure with Preserved Ejection Fraction. J. Clin. Med. 2020, 9, 1199. https://doi.org/10.3390/jcm9041199
Alcaide-Aldeano A, Garay A, Alcoberro L, Jiménez-Marrero S, Yun S, Tajes M, García-Romero E, Díez-López C, González-Costello J, Mateus-Porta G, et al. Iron Deficiency: Impact on Functional Capacity and Quality of Life in Heart Failure with Preserved Ejection Fraction. Journal of Clinical Medicine. 2020; 9(4):1199. https://doi.org/10.3390/jcm9041199
Chicago/Turabian StyleAlcaide-Aldeano, Alex, Alberto Garay, Lídia Alcoberro, Santiago Jiménez-Marrero, Sergi Yun, Marta Tajes, Elena García-Romero, Carles Díez-López, José González-Costello, Gemma Mateus-Porta, and et al. 2020. "Iron Deficiency: Impact on Functional Capacity and Quality of Life in Heart Failure with Preserved Ejection Fraction" Journal of Clinical Medicine 9, no. 4: 1199. https://doi.org/10.3390/jcm9041199
APA StyleAlcaide-Aldeano, A., Garay, A., Alcoberro, L., Jiménez-Marrero, S., Yun, S., Tajes, M., García-Romero, E., Díez-López, C., González-Costello, J., Mateus-Porta, G., Cainzos-Achirica, M., Enjuanes, C., Comín-Colet, J., & Moliner, P. (2020). Iron Deficiency: Impact on Functional Capacity and Quality of Life in Heart Failure with Preserved Ejection Fraction. Journal of Clinical Medicine, 9(4), 1199. https://doi.org/10.3390/jcm9041199