Helmet CPAP to Treat Acute Hypoxemic Respiratory Failure in Patients with COVID-19: A Management Strategy Proposal

 ,
, 
{kind=link}
Abstract
1. Effects of the Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2) Pandemic in Italy
2. Pathology and Pathophysiology of COVID-19 Pulmonary Damage
3. Rationale for Helmet Continuous Positive Airway Pressure (CPAP) in Severe COVID-19 Pneumonia
4. CPAP Side Effects and Helmet Pitfalls
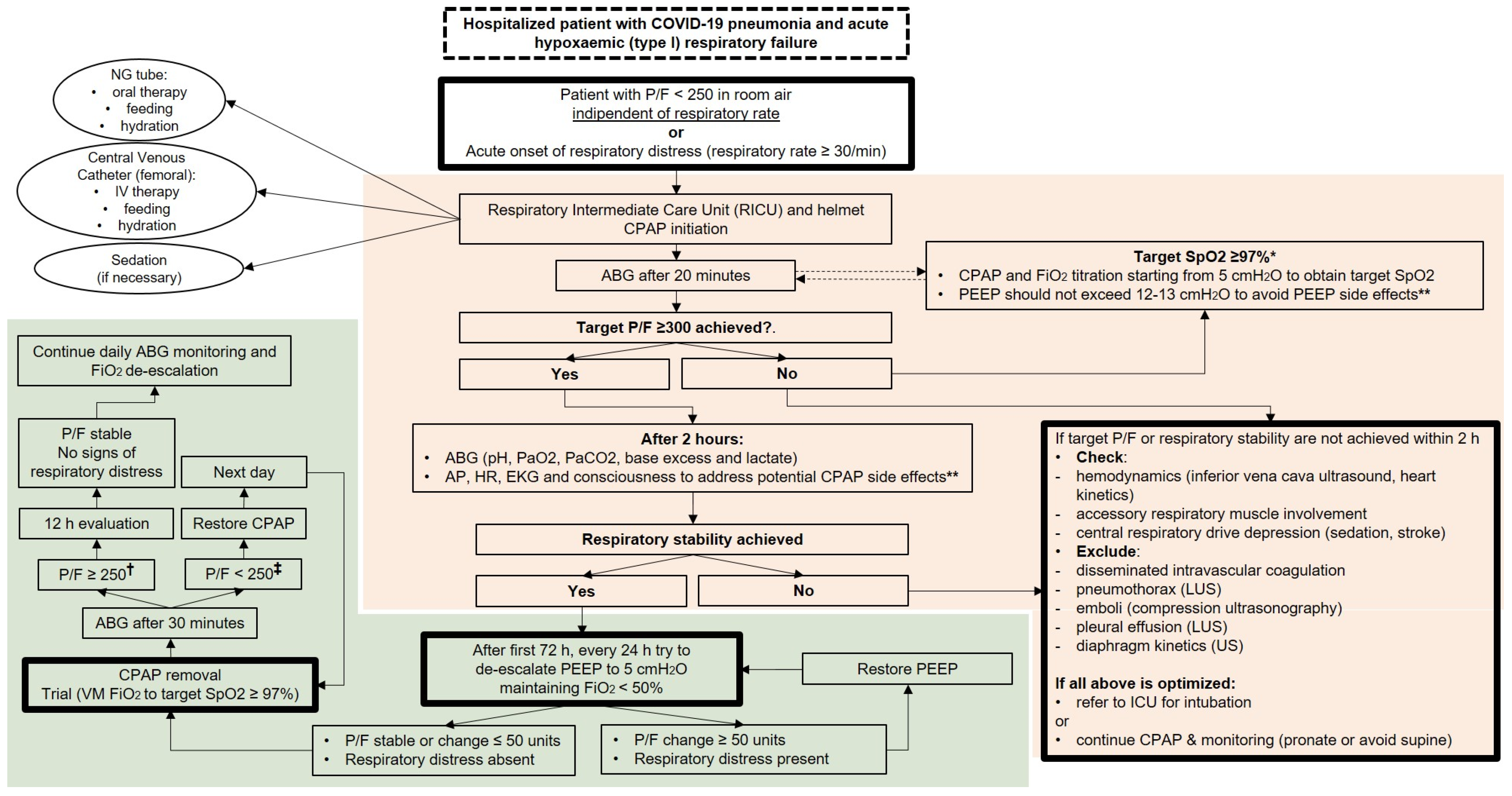
5. A Management Algorithm for COVID-19 Patients with De Novo Respiratory Failure
6. Conclusions
Supplementary Materials
Author Contributions
Conflicts of Interest
References
- World Health Organization. COVID-19 Situation in the WHO European Region. Available online: https://who.maps.arcgis.com/apps/opsdashboard/index.html#/ead3c6475654481ca51c248d52ab9c61 (accessed on 27 March 2020).
- Hui, D.S.; Chow, B.K.; Lo, T.; Tsang, O.T.Y.; Ko, F.W.; Ng, S.S.; Gin, T.; Chan, M.T.V. Exhaled air dispersion during high-flow nasal cannula therapy versus CPAP via different masks. Eur. Respir. J. 2019, 4, 1802339. [Google Scholar] [CrossRef] [PubMed]
- Ñamendys-Silva, S.A. Respiratory support for patients with COVID-19 infection. Lancet Respir. Med. 2020. [Google Scholar] [CrossRef]
- Gattinoni, L.; Coppola, S.; Cressoni, M.; Busana, M.; Rossi, S.; Chiumello, D. Covid-19 Does Not Lead to a “Typical” Acute Respiratory Distress Syndrome. Am. J. Respir. Crit. Care Med. 2020. [Google Scholar] [CrossRef] [PubMed]
- Tan, C.W.; Low, J.G.H.; Wong, W.H.; Chua, Y.Y.; Goh, S.L.; Ng, H.J. Critically Ill COVID-19 Infected Patients Exhibit Increased Clot Waveform Analysis Parameters Consistent with Hypercoagulability. Am. J. Hematol. 2020. [Google Scholar] [CrossRef]
- Xu, Z.; Shi, L.; Wang, Y.; Zhang, J.; Huang, L.; Zhang, C.; Liu, S.; Zhao, P.; Liu, H.; Zhu, L.; et al. Pathological findings of COVID-19 associated with acute respiratory distress syndrome. Lancet Respir. Med. 2020. [Google Scholar] [CrossRef]
- Navalesi, P.; Maggiore, S.M. Positive end-expiratory pressure. In Principles and Practice of Mechanical Ventilation, 3rd ed.; Tobin, M.J., Ed.; McGraw Hill Medical: New York, NY, USA, 2013; pp. 253–302. [Google Scholar]
- Chiumello, D.; Esquinas, A.M.; Moerer, O.; Terzi, N. A systematic technical review of the systems for the continuous positive airway pressure. Minerva Anestesiol. 2012, 78, 1385–1393. [Google Scholar]
- Chiumello, D.; Brochard, L.; Marini, J.J.; Slutsky, A.S.; Mancebo, J.; Ranieri, V.M.; Thompson, B.T.; Papazian, L.; Schultz, M.J.; Amato, M.; et al. Respiratory support in patients with acute respiratory distress syndrome: An expert opinion. Crit. Care 2017, 12, 240. [Google Scholar] [CrossRef]
- Chiumello, D.; Pelosi, P.; Carlesso, E.; Severgnini, P.; Aspesi, M.; Gamberoni, C.; Antonelli, M.; Conti, G.; Chiaranda, M.; Gattinoni, L. Noninvasive positive pressure ventilation delivered by helmet vs. standard face mask. Intensive Care Med. 2003, 29, 1671–1679. [Google Scholar] [CrossRef]
- Cosentini, R.; Brambilla, A.M.; Aliberti, S.; Bignamini, A.; Nava, S.; Maffei, A.; Martinotti, R.; Tarsia, P.; Monzani, V.; Pelosi, P. Helmet continuous positive airway pressure vs oxygen therapy to improve oxygenation in community-acquired pneumonia: A randomized, controlled trial. Chest 2010, 138, 114–120. [Google Scholar] [CrossRef]
- Brambilla, A.M.; Aliberti, S.; Prina, E.; Nicoli, F.; Del Forno, M.; Nava, S.; Ferrari, G.; Corradi, F.; Pelosi, P.; Bignamini, A.; et al. Helmet CPAP vs. oxygen therapy in severe hypoxemic respiratory failure due to pneumonia. Intensive Care Med. 2014, 40, 942–949. [Google Scholar] [CrossRef]
- Squadrone, V.; Coha, M.; Cerutti, E.; Schellino, M.M.; Biolino, P.; Occella, P.; Belloni, G.; Vilianis, G.; Fiore, G.; Cavallo, F.; et al. Piedmont Intensive Care Units Network (PICUN). Continuous positive airway pressure for treatment of postoperative hypoxemia: A randomized controlled trial. JAMA 2005, 293, 589–595. [Google Scholar] [CrossRef] [PubMed]
- Squadrone, V.; Massaia, M.; Bruno, B.; Marmont, F.; Falda, M.; Bagna, C.; Bertone, S.; Filippini, C.; Slutsky, A.S.; Vitolo, U.; et al. Early CPAP prevents evolution of acute lung injury in patients with hematologic malignancy. Intensive Care Med. 2010, 36, 1666–1674. [Google Scholar] [CrossRef] [PubMed]
- Ferioli, M.; Cisternino, C.; Leo, V.; Pisani, L.; Palange, P.; Nava, S. Protecting healthcare workers from SARS-CoV-2 infection: Practical indications. Eur. Respir. Rev. 2020, 29. [Google Scholar] [CrossRef] [PubMed]
- Scandroglio, M.; Piccolo, U.; Mazzone, E.; Agrati, P.; Aspesi, M.; Gamberoni, C.; Severgnini, P.; Di Stella, R.; Chiumello, D.; Minoja, G.; et al. Use and nursing of the helmet in delivering non invasive ventilation. Minerva Anestesiol. 2002, 68, 475–480. [Google Scholar]
- Crimi, C.; Noto, A.; Princi, P.; Esquinas, A.; Nava, S. A European survey of noninvasive ventilation practices. Eur. Respir. J. 2010, 36, 362–369. [Google Scholar] [CrossRef]
- Patroniti, N.; Foti, G.; Manfio, A.; Coppo, A.; Bellani, G.; Pesenti, A. Head helmet versus face mask for non-invasive continuous positive airway pressure: A physiological study. Int. Care Med. 2003, 29, 1680–1687. [Google Scholar] [CrossRef]
- Radovanovic, D.; Schnell, T.; McLachlan, A.; Shaikh, H.; Jubran, A.; Tobin, M.J.; Laghi, F. Can external positive end expiratory pressure worsen the neuromechanical coupling of the diaphragm in patients with COPD? Am. J. Respir. Crit. Care Med. 2016, 193, A5234. [Google Scholar]
- Liu, W.; Tao, Z.W.; Lei, W.; Ming-Li, Y.; Kui, L.; Ling, Z.; Shuang, W.; Yan, D.; Jing, L.; Liu, H.G.; et al. Analysis of factors associated with disease outcomes in hospitalized patients with 2019 novel coronavirus disease. Chin. Med. J. 2020. [Google Scholar] [CrossRef]
- Guan, W.J.; Ni, Z.Y.; Hu, Y.; Liang, W.H.; Ou, C.Q.; He, J.X.; Liu, L.; Shan, H.; Lei, C.L.; Hui, D.S.C.; et al. China Medical Treatment Expert Group for Covid-19. Clinical characteristics of coronavirus disease 2019 in China. N. Engl. J. Med. 2020. [Google Scholar] [CrossRef]
- Esquinas Rodriguez, A.M.; Papadakos, P.J.; Carron, M.; Cosentini, R.; Chiumello, D. Clinical review: Helmet and non-invasive mechanical ventilation in critically ill patients. Crit. Care 2013, 17, 223. [Google Scholar] [CrossRef]
- Racca, F.; Appendini, L.; Gregoretti, C.; Stra, E.; Patessio, A.; Donner, C.F.; Ranieri, V.M. Effectiveness of mask and helmet interfaces to deliver noninvasive ventilation in a human model of resistive breathing. J. Appl. Physiol. 2005, 99, 1262–1271. [Google Scholar] [CrossRef] [PubMed]
- Taccone, P.; Hess, D.; Caironi, P.; Bigatello, L.M. Continuous positive airway pressure delivered with a “helmet”: Effects on carbon dioxide rebreathing. Crit. Care Med. 2004, 32, 2090–2096. [Google Scholar] [CrossRef] [PubMed]
- Milan, M.; Zanella, A.; Isgrò, S.; Deab, S.A.; Magni, F.; Pesenti, A.; Patroniti, N. Performance of different continuous positive airway pressure helmets equipped with safety valves during failure of fresh gas supply. Intensive Care Med. 2011, 37, 1031–1035. [Google Scholar] [CrossRef]
- Cunningham, D.J.C.; Robbins, P.A.; Wolff, C.B. Integration of Respiratory Responses to Changes in Alveolar Partial Pressures of CO2 and O2 and in Arterial pH. Compr. Physiol. 2011, (Suppl. 11), 475–528. [Google Scholar] [CrossRef]
- Easton, P.A.; Slykerman, L.J.; Anthonisen, N.R. Ventilatory response to sustained hypoxia in normal adults. J. Appl. Physiol. 1986, 61, 906–911. [Google Scholar] [CrossRef] [PubMed]
- Coppola, S.; Caccioppola, A.; Froio, S.; Ferrari, E.; Gotti, M.; Formenti, P.; Chiumello, D. Dynamic hyperinflation and intrinsic positive end-expiratory pressure in ARDS patients. Crit. Care 2019, 23, 375. [Google Scholar] [CrossRef]
- Richardson, A.; Killen, A. How long do patients spend weaning from CPAP in critical care? Intensive Crit. Care Nurs. 2006, 22, 206–213. [Google Scholar] [CrossRef]
- Amatya, S.; Macomber, M.; Bhutada, A.; Rastogi, D.; Rastogi, S. Sudden versus gradual pressure wean from Nasal CPAP in preterm infants: A randomized controlled trial. J. Perinatol. 2017, 37, 662–667. [Google Scholar] [CrossRef]
- Jason, T.P.; Bhakti, K.P.; Andrew, M.D. Management of Critically Ill Adults with COVID-19. JAMA 2020. [Google Scholar] [CrossRef]
- Vitacca, M.; Nava, S.; Santus, P.; Harari, S. Early consensus management for non-ICU ARF SARS-CoV-2 emergency in Italy: From ward to trenches. Eur. Respir. J. 2020. [Google Scholar] [CrossRef]
- Zhou, F.; Yu, T.; Du, R.; Fan, G.; Liu, Y.; Liu, Z.; Xiang, J.; Wang, Y.; Song, B.; Gu, X.; et al. Clinical course and risk factors for mortality of adult inpatients with COVID-19 in Wuhan, China: A retrospective cohort study. Lancet 2020, 395, 1054–1062. [Google Scholar] [CrossRef]
- Shi, S.; Qin, M.; Shen, B.; Cai, Y.; Liu, T.; Yang, F.; Gong, W.; Liu, X.; Liang, J.; Zhao, Q.; et al. Association of Cardiac Injury with Mortality in Hospitalized Patients With COVID-19 in Wuhan, China. JAMA Cardiol. 2020. [Google Scholar] [CrossRef]
- Tang, X.; Du, R.; Wang, R.; Cao, T.; Guan, L.; Yang, C.; Zhu, Q.; Hu, M.; Li, X.; Li, Y.; et al. Comparison of Hospitalized Patients with Acute Respiratory Distress Syndrome Caused by COVID-19 and H1N1. Chest 2020. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Lu, X.; Chen, H.; Chen, T.; Su, N.; Huang, F.; Zhou, J.; Zhang, B.; Li, Y.; Yan, F.; et al. Clinical Course and Outcomes of 344 Intensive Care Patients with COVID-19. Am. J. Respir. Crit. Care Med. 2020. [Google Scholar] [CrossRef] [PubMed]
- Grasselli, G.; Zangrillo, A.; Zanella, A.; Antonelli, M.; Cabrini, L.; Castelli, A.; Cereda, D.; Coluccello, A.; Foti, G.; Fumagalli, R.; et al. COVID-19 Lombardy ICU Network. Baseline Characteristics and Outcomes of 1591 Patients Infected With SARS-CoV-2 Admitted to ICUs of the Lombardy Region, Italy. JAMA 2020. [Google Scholar] [CrossRef] [PubMed]
- Bhatraju, P.K.; Ghassemieh, B.J.; Nichols, M.; Kim, R.; Jerome, K.R.; Nalla, A.K.; Greninger, A.L.; Pipavath, S.; Wurfel, M.M.; Evans, L.; et al. Covid-19 in Critically Ill Patients in the Seattle Region—Case Series. N. Engl. J. Med. 2020. [Google Scholar] [CrossRef]
- Cao, J.; Tu, W.J.; Cheng, W.; Yu, L.; Liu, Y.K.; Hu, X.; Liu, Q. Clinical Features and Short-term Outcomes of 102 Patients with Corona Virus Disease 2019 in Wuhan, China. Clin. Infect. Dis. 2020. [Google Scholar] [CrossRef]

© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Radovanovic, D.; Rizzi, M.; Pini, S.; Saad, M.; Chiumello, D.A.; Santus, P. Helmet CPAP to Treat Acute Hypoxemic Respiratory Failure in Patients with COVID-19: A Management Strategy Proposal. J. Clin. Med. 2020, 9, 1191. https://doi.org/10.3390/jcm9041191
Radovanovic D, Rizzi M, Pini S, Saad M, Chiumello DA, Santus P. Helmet CPAP to Treat Acute Hypoxemic Respiratory Failure in Patients with COVID-19: A Management Strategy Proposal. Journal of Clinical Medicine. 2020; 9(4):1191. https://doi.org/10.3390/jcm9041191
Chicago/Turabian StyleRadovanovic, Dejan, Maurizio Rizzi, Stefano Pini, Marina Saad, Davide Alberto Chiumello, and Pierachille Santus. 2020. "Helmet CPAP to Treat Acute Hypoxemic Respiratory Failure in Patients with COVID-19: A Management Strategy Proposal" Journal of Clinical Medicine 9, no. 4: 1191. https://doi.org/10.3390/jcm9041191
APA StyleRadovanovic, D., Rizzi, M., Pini, S., Saad, M., Chiumello, D. A., & Santus, P. (2020). Helmet CPAP to Treat Acute Hypoxemic Respiratory Failure in Patients with COVID-19: A Management Strategy Proposal. Journal of Clinical Medicine, 9(4), 1191. https://doi.org/10.3390/jcm9041191