Non-Vitamin K Oral Anticoagulants (NOAC) versus Vitamin K Antagonists (VKA) for Atrial Fibrillation with Elective or Urgent Percutaneous Coronary Intervention: A Meta-Analysis with a Particular Focus on Combination Type

 , , , ,
, , , ,  and
and
Abstract
1. Introduction
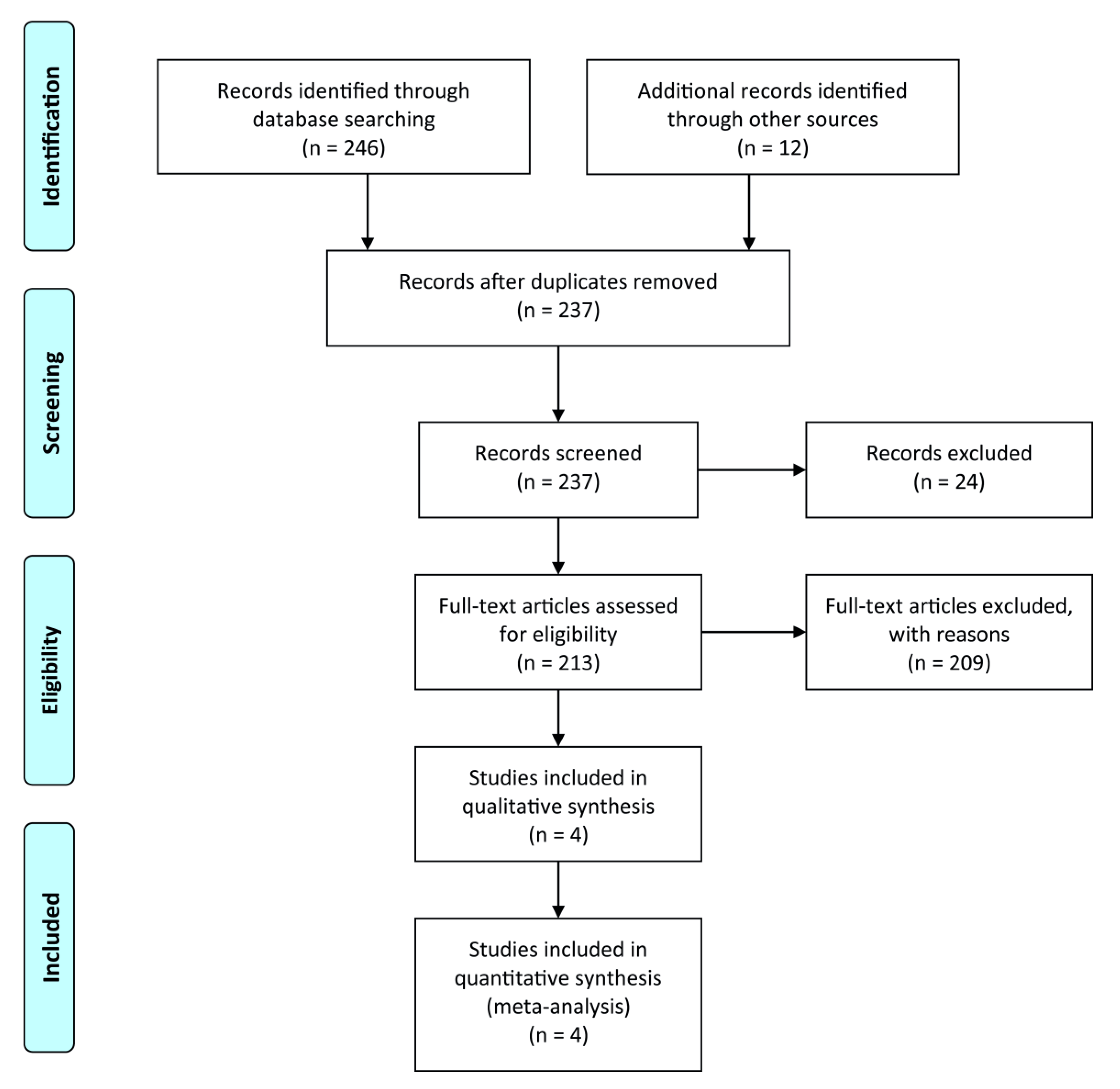
2. Methods
Statistics
3. Results
3.1. Dual Antithrombotic Therapy (DAT) Consisting of a NOAC and a Single Antiplatelet Drug (SAPT: P2Y12 Inhibitor) vs. Triple Antithrombotic Therapy (TAT) Consisting of a VKA and Dual Antiplatelet Therapy (DAPT: P2Y12 Inhibitor and Aspirin)
3.2. NOAC with Any Antiplatelet Combination vs. VKA with Any Antiplatelet Combination
3.3. Subgroup Analyses
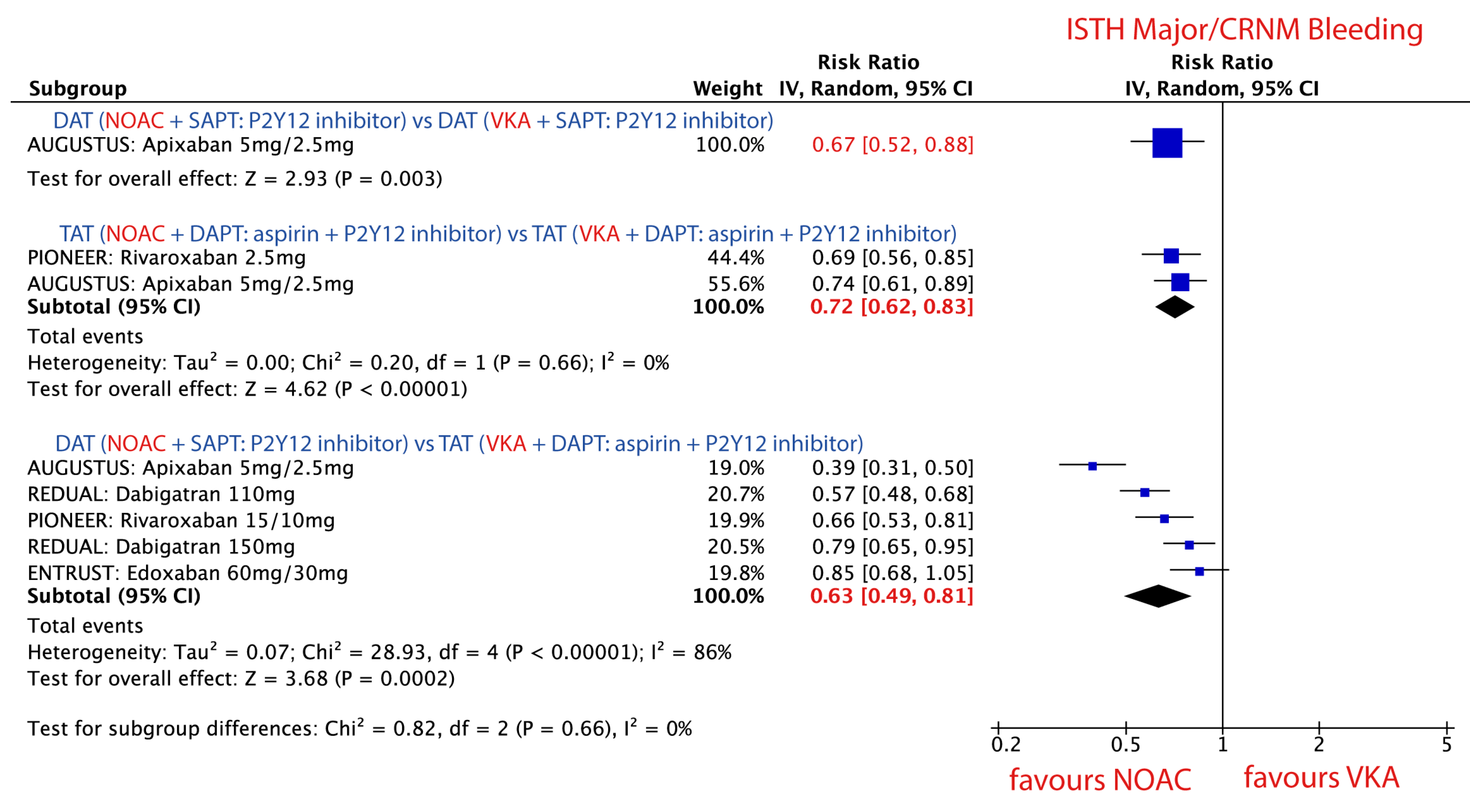
3.3.1. ISTH Major or CRNM Bleeding Events in Patients Treated with Combinations Consisting of a NOAC vs. a VKA
3.3.2. DAT vs. DAT: NOAC + P2Y12 Inhibitor vs. VKA + P2Y12 Inhibitor
3.3.3. TAT vs. TAT: NOAC + P2Y12 Inhibitor + Aspirin vs. VKA + P2Y12 Inhibitor + Aspirin
3.3.4. DAT vs. TAT: NOAC + P2Y12 Inhibitor vs. VKA + P2Y12 Inhibitor + Aspirin
3.3.5. Stent Thrombosis (ST) in Patients Treated with Combinations Consisting of NOAC vs. VKA
3.3.6. Major Adverse Cardiac Events (MACE) in Patients Treated with Combinations Consisting of NOAC vs. VKA
3.3.7. All-Cause Mortality in Patients Treated with Combinations Consisting of NOAC vs. VKA
3.4. Sensitivity Analysis
3.4.1. ISTH Major/CRNM Bleeding
3.4.2. Stent Thrombosis
4. Discussion
5. Conclusions
6. Summary Box
6.1. What Is Already Known on This Topic
6.2. What This Study Adds
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
Ethical Approval
Data Sharing
Abbreviations
| Atrial fibrillation | AF |
| Percutaneous coronary intervention | PCI |
| Coronary artery disease | CAD |
| Vitamin K antagonists | VKAs |
| Non–vitamin K antagonist oral anticoagulants | NOACs |
| Dual antiplatelet therapy | DAPT |
| Acute coronary syndrome | ACS |
| Myocardial infarction | MI |
| Stent thrombosis | ST |
| Triple antithrombotic therapy | TAT |
| Oral anticoagulants | OAC |
| Randomized controlled trials | RCTs |
| Single antiplatelet therapy | SAPT |
| International Society on Thrombosis and Hemostasis | ISTH |
| Thrombolysis in Myocardial Infarction | TIMI |
| Major adverse cardiovascular events | MACE |
| Confidence interval | CI |
| Dual antithrombotic therapy | DAT |
| Hazard ratio | HR |
References
- Lip, G.Y.; Fauchier, L.; Freedman, S.B.; Van Gelder, I.; Natale, A.; Gianni, C.; Nattel, S.; Potpara, T.; Rienstra, M.; Tse, H.F.; et al. Atrial fibrillation. Nat. Rev. Dis. Prim. 2016, 2, 16016. [Google Scholar] [CrossRef] [PubMed]
- Kralev, S.; Schneider, K.; Lang, S.; Süselbeck, T.; Borggrefe, M. Incidence and severity of coronary artery disease in patients with atrial fibrillation undergoing first-time coronary angiography. PLoS ONE 2011, 6. [Google Scholar] [CrossRef] [PubMed]
- Capodanno, D.; Lip, G.Y.; Windecker, S.; Huber, K.; Kirchhof, P.; Boriani, G.; Lane, D.; Gilard, M.; Collet, J.P.; Valgimigli, M.; et al. Triple antithrombotic therapy in atrial fibrillation patients with acute coronary syndromes or undergoing percutaneous coronary intervention or transcatheter aortic valve replacement. EuroIntervention 2015, 10, 1015–1021. [Google Scholar] [CrossRef] [PubMed]
- Heidbuchel, H.; Verhamme, P.; Alings, M.; Antz, M.; Diener, H.-C.; Hacke, W.; Oldgren, J.; Sinnaeve, P.; Camm, J.; Kirchhof, P.; et al. Updated European Heart Rhythm Association Practical Guide on the use of non-vitamin K antagonist anticoagulants in patients with non-valvular atrial fibrillation. Ep. Eur. 2015, 17, 1467–1507. [Google Scholar] [CrossRef] [PubMed]
- Golwala, H.B.; Cannon, C.P.; Steg, P.G.; Doros, G.; Qamar, A.; Ellis, G.S.; Oldgren, J.; Berg, M.T.J.; Kimura, T.; Hohnloser, S.H.; et al. Safety and efficacy of dual vs. triple antithrombotic therapy in patients with atrial fibrillation following percutaneous coronary intervention: A systematic review and meta-analysis of randomized clinical trials. Eur. Heart J. 2018, 39, 1726–1735. [Google Scholar] [CrossRef]
- Patti, G.; Pecen, L.; Lucerna, M.; Huber, K.; Rohla, M.; Renda, G.; Siller-Matula, J.; Ricci, F.; Kirchhof, P.; De Caterina, R. Net clinical benefit of non-vitamin K antagonist vs. vitamin K antagonist anticoagulants in elderly patients with atrial fibrillation. Am. J. Med. 2019, 132, 749–757. [Google Scholar] [CrossRef]
- Patti, G.; Pecen, L.; Lucerna, M.; Huber, K.; Rohla, M.; Renda, G.; Siller-Matula, J.; Schnabel, R.B.; Cemin, R.; Kirchhof, P.; et al. Outcomes of anticoagulated patients with atrial fibrillation treated with or without antiplatelet therapy-A pooled analysis from the PREFER in AF and PREFER in AF PROLONGATON registries. Int. J. Cardiol. 2018, 270, 160–166. [Google Scholar] [CrossRef]
- Guedeney, P.; Vogel, B.; Mehran, R. Non-vitamin K Antagonist Oral Anticoagulant After Acute Coronary Syndrome: Is There a Role? Interv. Cardiol. Rev. 2018, 13, 93. [Google Scholar] [CrossRef]
- Lopes, R.D.; Vora, A.N.; Liaw, D.; Granger, C.B.; Darius, H.; Goodman, S.G.; Mehran, R.; Windecker, S.; Alexander, J.H. An open-Label, 2 × 2 factorial, randomized controlled trial to evaluate the safety of apixaban vs. vitamin K antagonist and aspirin vs. placebo in patients with atrial fibrillation and acute coronary syndrome and/or percutaneous coronary intervention: Rationale and design of the AUGUSTUS trial. Am. Heart J. 2018, 200, 17–23. [Google Scholar] [CrossRef]
- Lopes, R.D.; Heizer, G.; Aronson, R.; Vora, A.N.; Massaro, T.; Mehran, R.; Goodman, S.G.; Windecker, S.; Darius, H.; Li, J.; et al. Antithrombotic therapy after acute coronary syndrome or PCI in atrial fibrillation. N. Engl. J. Med. 2019, 380, 1509–1524. [Google Scholar] [CrossRef]
- Gibson, C.M.; Mehran, R.; Bode, C.; Halperin, J.; Verheugt, F.W.; Wildgoose, P.; Birmingham, M.; Janus, J.; Burton, P.; Eickels, M.V.; et al. Prevention of bleeding in patients with atrial fibrillation undergoing PCI. N. Engl. J. Med. 2016, 375, 2423–2434. [Google Scholar] [CrossRef] [PubMed]
- Cannon, C.P.; Bhatt, D.L.; Oldgren, J.; Lip, G.Y.H.; Ellis, S.G.; Kimura, T.; Maeng, M.; Merkely, B.; Zeymer, U.; Gropper, S.; et al. Dual antithrombotic therapy with dabigatran after PCI in atrial fibrillation. N. Engl. J. Med. 2019, 377, 1513–1524. [Google Scholar] [CrossRef] [PubMed]
- Gibson, C.M.; Mehran, R.; Bode, C.; Halperin, J.; Verheugt, F.; Wildgoose, P.; Eickels, M.V.; Lip, G.Y.H.; Cohen, M.; Husted, S.; et al. An open-label, randomized, controlled, multicenter study exploring two treatment strategies of rivaroxaban and a dose-adjusted oral vitamin K antagonist treatment strategy in subjects with atrial fibrillation who undergo percutaneous coronary intervention (PIONEER AF-PCI). Am. Heart J. 2015, 169, 472–478. [Google Scholar] [CrossRef] [PubMed]
- Vranckx, P.; Valgimigli, M.; Eckardt, L.; Tijssen, J.; Lewalter, T.; Gargiulo, G.; Batuchkin, V.; Campo, G.; Lysak, Z.; Vakaliuk, I.; et al. Edoxaban-based versus vitamin K antagonist-based antithrombotic regimen after successful coronary stenting in patients with atrial fibrillation (ENTRUST-AF PCI): A randomised, open-label, phase 3b trial. Lancet 2019, 10206, 1335–1343. [Google Scholar] [CrossRef]
- Lopes, R.D.; Leonardi, S.; Wojdyla, D.M.; Vora, A.N.; Thomas, L.; Storey, R.F.; Vinereanu, D.; Granger, C.B.; Goodman, S.G.; Aronson, R.; et al. Stent Thrombosis in Patients with Atrial Fibrillation Undergoing Coronary Stenting in the AUGUSTUS Trial. Circulation 2019, 141, 781–783. [Google Scholar] [CrossRef]
- Biondi-Zoccai, G.G.; Lotrionte, M.; Abbate, A.; Testa, L.; Remigi, E.; Burzotta, F.; Valgimili, M.; Romagnoli, E.; Crea, F.; Agostoni, P. Compliance with QUOROM and quality of reporting of overlapping meta-analyses on the role of acetylcysteine in the prevention of contrast associated nephropathy: Case study. BMJ Open 2006, 332, 202–209. [Google Scholar] [CrossRef]
- Manager, R. (RevMan). Version 5.3. Copenhagen, Denmark: Nordic Cochrane Center, Cochrane Collaboration. 2012. Available online: https://community.cochrane.org/help/tools-and-software/revman-5 (accessed on 14 April 2020).
- Higgins, J.P.; Thompson, S.G. Quantifying heterogeneity in a meta-analysis. Stat. Med. 2002, 21, 1539–1558. [Google Scholar] [CrossRef]
- Leon, M.B.; Baim, D.S.; Popma, J.J.; Gordon, P.C.; Cutlip, D.E.; Ho, K.K.L.; Gimbartolomei, A.; Diver, D.J.; Lasords, D.M.; Williams, D.O.; et al. A clinical trial comparing three antithrombotic-drug regimens after coronary-artery stenting. N. Engl. J. Med. 1998, 339, 1665–1671. [Google Scholar] [CrossRef]
- Schömig, A.; Neumann, F.J.; Kastrati, A.; Schühlen, H.; Blasini, R.; Hadamitzky, M.; Walter, H.; Zitzmann-Roth, E.M.; Richardt, G.; Alt, E.; et al. A randomized comparison of antiplatelet and anticoagulant therapy after the placement of coronary-artery stents. N. Engl. J. Med. 1996, 334, 1084–1089. [Google Scholar] [CrossRef]
- Site, H.G. Clopidogrel plus aspirin versus oral anticoagulation for atrial fibrillation in the Atrial fibrillation Clopidogrel Trial with Irbesartan for prevention of Vascular Events (ACTIVE W): A randomised controlled trial. Lancet 2006, 367, 1903–1912. [Google Scholar] [CrossRef]
- Lip, G.Y.H.; Collet, J.P.; Haude, M.; Byrne, M.; Chung, E.H.; Fauchier, L.; Halvorsen, S.; Lau, D.; Lopez-Cabanillas, N.; Lettino, M.; et al. Joint European consensus document on the management of antithrombotic therapy in atrial fibrillation patients presenting with acute coronary syndrome and/or undergoing percutaneous cardiovascular interventions: A joint consensus document of the European Heart Rhythm Association (EHRA), European Society of Cardiology Working Group on Thrombosis, European Association of Percutaneous Cardiovascular Interventions (EAPCI), and European Association of Acute Cardiac Care (ACCA) endorsed by the Heart Rhythm Society (HRS), Asia-Pacific Heart Rhythm Society (APHRS), Latin America Heart Rhythm Society (LAHRS), and Cardiac Arrhythmia Society of Southern Africa (CASSA). Europace. 2019, 21, 192–193. [Google Scholar] [CrossRef]
- Gargiulo, G.; Goette, A.; Tijssen, J.; Eckardt, L.; Lewalter, T.; Vranckx, P.; Valgimigli, M. Safety and efficacy outcomes of double vs. triple antithrombotic therapy in patients with atrial fibrillation following percutaneous coronary intervention: A systematic review and meta-analysis of non-vitamin K antagonist oral anticoagulant-based randomized clinical trials. Eur. Heart J. 2019, 40, 3757–3767. [Google Scholar] [CrossRef] [PubMed]
- Winter, M.P.; Grove, E.L.; De Caterina, R.; Gorog, D.A.; Ahrens, I.; Geisler, T.; Gurbel, P.A.; Tantry, U.; Navarese, E.P.; Siller-Matula, J.M. Advocating cardiovascular precision medicine with P2Y12 receptor inhibitors. Eur. Heart J. 2017, 3, 221–234. [Google Scholar] [CrossRef] [PubMed]
- Komosa, A.; Siller-Matula, J.M.; Lesiak, M.; Michalak, M.; Kowal, J.; Maczynski, M.; Siniawski, A.; Mularek-Kubzdela, T.; Wisniewski, S.; Grajek, S. Association between high on-treatment platelet reactivity and occurrence of cerebral ischemic events in patients undergoing percutaneous coronary intervention. Thromb. Res. 2016, 138, 49–54. [Google Scholar] [CrossRef] [PubMed]
- Schoergenhofer, C.; Hobl, E.L.; Schellongowski, P.; Heinz, G.; Speidl, W.S.; Siller-Matula, J.M.; Schmid, M.; Sunder-Plaßmann, R.; Stimpfl, T.; Hackl, M.; et al. Clopidogrel in critically ill patients. Clin. Pharmacol. Ther. 2018, 103, 217–223. [Google Scholar] [CrossRef]
- Oldgren, J.; Steg, P.G.; Hohnloser, S.H.; Lip, G.Y.H.; Kimura, T.; Nordaby, M.; Brueckmann, M.; Kleine, E.; Berg, J.M.T.; Bhatt, D.L.; et al. Dabigatran dual therapy with ticagrelor or clopidogrel after percutaneous coronary intervention in atrial fibrillation patients with or without acute coronary syndrome: A subgroup analysis from the RE-DUAL PCI trial. Eur. Heart J. 2019, 40, 1553–1562. [Google Scholar] [CrossRef]
- Christ, G.; Siller-Matula, J.M.; Francesconi, M.; Dechant, C.; Grohs, K.; Podczeck-Schweighofer, A. Individualising dual antiplatelet therapy after percutaneous coronary intervention: The IDEAL-PCI registry. BMJ Open 2014, 4, e005781. [Google Scholar] [CrossRef] [PubMed]
- Lopes, R.D.; Hong, H.; Harskamp, R.E.; Bhatt, D.L.; Mehran, R.; Cannon, C.P.; Granger, C.B.; Verheugt, F.W.; Li, J.; Jurriën, M.; et al. Safety and Efficacy of Antithrombotic Strategies in Patients With Atrial Fibrillation Undergoing Percutaneous Coronary Intervention: A Network Meta-analysis of Randomized Controlled Trials. JAMA Cardiol. 2019. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| PIONEER AF-PCI | RE-DUAL PCI | ENTRUST AF PCI | AUGUSTUS | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Rivaroxaban 15 mg QD + P2Y12 Inhibitor (N = 709) | Rivaroxaban 2.5 mg + DAPT (N = 709) | VKA + DAPT (N = 706) | Dabigatran 110 mg + P2Y12 Inhibitor (N = 981) | Dabigatran 150 mg + P2Y12 Inhibitor (N = 763) | VKA + DAPT (N = 981) | Edoxaban + P2Y12 Inhibitor (N = 751) | VKA + DAPT (N = 755) | Apixaban + P2Y12 Inhibitor (N = 2306) | VKA + P2Y12 Inhibitor (N = 2308) | Aspirin (N = 2307) | Aspirin-Matched Placebo (N = 2307) | |
| Age (year) | 70.4 ± 9.1 | 70.0 ± 9.1 | 69.9 ± 8.7 | 71.5 ± 8.9 | 68.6 ± 7.7 | 71.7 ± 8.9 | 69 (63–77) | 70 (64–77) | 70.4 (64.1–77.2) | 70.9 (64.3–77.2) | 70.8 (64.4–77.3) | 70.6 (63.8–77.2) |
| Female (%) | 25.5 | 24.5 | 26.6 | 25.8 | 22.4 | 23.5 | 26 | 25 | 29.1 | 28.9 | 30.2 | 27.8 |
| BMI, median (IQR) | 28.6 (25.7–32.4) | 28.4 (25.6–32.1) | 29.0 (25.8–32.8) | NR | NR | NR | NR | NR | NR | NR | NR | NR |
| Diabetes mellitus (%) | 28.8 | 28.1 | 31.3 | 36.9 | 34.1 | 37.9 | 34 | 34 | 36.5 | 36.2 | 36.5 | 36.2 |
| Hypertension (%) | 73.3 | 73.2 | 75.4 | NR | NR | NR | 90 | 91 | 88.6 | 88.0 | 88.0 | 88.5 |
| Dyslipidemia (%) | 42.6 | 41.6 | 44.8 | NR | NR | NR | 66 | 64 | NR | NR | NR | NR |
| Current smoker (%) | 5.2 | 7.9 | 6.8 | NR | NR | NR | NR | NR | NR | NR | NR | NR |
| History OF MI (%) | 19.8 | 25.4 | 25.4 | 24.2 | 25.4 | 27.3 | 25 | 23 | NR | NR | NR | NR |
| Heart Failure (%) | 25.4 | 26.4 | 24.8 | NR | NR | NR | 56 | 54 | 42.4 | 43.2 | 42.6 | 43.0 |
| History of CABG (%) | NR | NR | NR | 9.9 | 10.4 | 11.3 | 6 | 6 | NR | NR | NR | NR |
| History of PCI (%) | NR | NR | NR | 33.2 | 31.3 | 35.4 | 26 | 26 | NR | NR | NR | NR |
| Type of index event (%) | ||||||||||||
| ACS | 51.5 | 53.2 | 52.2 | 51.9 | 51.2 | 48.4 | 52 | 52 | 61.8 | 60.5 | 60.7 | 61.7 |
| NON-ACS | 48.5 | 46.8 | 47.8 | 48.1 | 48.8 | 51.6 | 48 | 48 | 38.2 | 39.5 | 39.3 | 38.3 |
| Type of stent (%) | ||||||||||||
| Drug-eluting | 65.4 | 66.8 | 66.5 | 82.1 | 81.5 | 84.6 | NR | NR | NR | NR | NR | NR |
| Bare-metal stent | 32.6 | 31.2 | 31.8 | 15.1 | 16.1 | 13.6 | NR | NR | NR | NR | NR | NR |
| Drug-eluting and bare-metal stent | 2.0 | 2.0 | 1.7 | 1.9 | 1.3 | 1.2 | NR | NR | NR | NR | NR | NR |
| Type of P2Y12i (%) | ||||||||||||
| Clopidogrel | 93.1 | 93.7 | 96.3 | 86.4 | 86.9 | 90.3 | 93 | 92 | 93.4 | 91.8 | 92.1 | 93.2 |
| Ticagrelor | 5.2 | 4.8 | 3.0 | 12.6 | 12.1 | 7.8 | 7 | 8 | 5.4 | 7.1 | 6.5 | 5.9 |
| Prasugrel | 1.7 | 1.6 | 0.7 | 0 | 0 | 0 | <1 | <1 | 1.2 | 1.1 | 1.4 | 0.9 |
| Type of P2Y12i CLP/TIG/PRS | 94%/4%/1% | 88%/12%/0% | 92,5%/7,5%/<1% | 92.6%/6.2%/1.1% | ||||||||
| CHA2DS2-VASc score ‡ | 3.7 ± 1.7 | 3.8 ± 1.6 | 3.8 ± 1.6 | 3.7 ± 1.6 | 3.3 ± 1.5 | 3.8 ± 1.5 | 4.0 (3.0-5.0) | 4.0 (3.0-5.0) | 3.9 ± 1.6 | 4.0 ± 1.6 | 3.9 ± 1.6 | 3.9 ± 1.6 |
| HAS-BLED score † | 3.0 ± 0.91 | 2.92 ± 0.96 | 2.98 ± 0.92 | 2.7 ± 0.7 | 2.8 ± 0.8 | 2.6 ± 0.7 | 3.0 (2.0–3.0) | 3.0 (2.0–3.0) | 2.9 ± 1.0 | 2.9 ± 0.9 | 2.8 ± 0.9 | 2.9 ± 1.0 |
| Trial Name | Subgroup | Anticoagulant | Duration (Months) | Patients n/N (%) |
|---|---|---|---|---|
| PIONEER AF-PCI | DAT | Rivaroxaban 15 mg | 12 | 709/709 (100%) |
| Clopidogrel 75 mg | 12 | |||
| TAT | Rivaroxaban 2.5 mg or 15 mg | 1 | 109/709 (15.4%) | |
| 6 | 248/709 (35%) | |||
| 12 | 352/709 (49.6%) | |||
| ASA 75–100 mg | 12 | 709/709 (100%) | ||
| Clopidogrel 75 mg | 1 | 109/709 (15.4%) | ||
| 6 | 248/709 (35%) | |||
| 12 | 352/709 (49.6%) | |||
| TAT | VKA (INR 2.0–3.0) | 12 | 706/706 (100%) | |
| ASA 75–100 mg | 12 | |||
| Clopidogrel 75 mg | 1 | 113/697 (16.2%) | ||
| 6 | 243/697 (34.9%) | |||
| 12 | 341/697 (48.9%) | |||
| RE-DUAL PCI | DAT Dabigatran 110 mg | Dabigatran 110 mg | 14 | 981/981 (100%) |
| Clopidogrel 75 mg | 14 | |||
| DAT Dabigatran 150 mg | Dabigatran 150 mg | 14 | 763/763 (100%) | |
| Clopidogrel 75 mg | 14 | |||
| TAT | VKA (INR 2.0–3.0) | 14 | 981/981 (100%) | |
| ASA 75–100 mg | 1 | 171/981 (17%) | ||
| 3 | 810/981 (83%) | |||
| Clopidogrel 75 mg | 14 | 981/981 (100%) | ||
| ENTRUST AF PCI | DAT | Edoxaban 60 mg | 12 | 751/751 (100%) |
| Clopidogrel 75 mg | 12 | |||
| TAT | VKA (INR 2.0–3.0) | 12 | 755/755 (100%) | |
| ASA 100 mg | 1 to 12 | |||
| Clopidogrel 75 mg | 12 | |||
| AUGUSTUS | DAT | Apixaban 5 mg | 6 | 1153/1153 (100%) |
| Clopidogrel 75 mg | 6 | |||
| TAT | VKA (INR 2.0–3.0) | 6 | 1154/1154 (100%) | |
| ASA 81 mg | 6 | |||
| Clopidogrel 75 mg | 6 |
| ISTH Major/CRNM Bleeding | ||
|---|---|---|
| Study | RR (95% CI) for Each Study | RR (95% CI) for the Total Effect After Exclusion of Each Single Study |
| AUGUSTUS: Apixaban 5mg/2.5mg | 0.39 [0.31, 0.50] | 0.71 [0.59, 0.84] |
| REDUAL: Dabigatran 110mg | 0.57 [0.48, 0.68] | 0.65 [0.47, 0.89] |
| PIONEER: Rivaroxaban 15/10mg | 0.66 [0.53, 0.81] | 0.62 [0.46, 0.85] |
| REDUAL: Dabigatran 150mg | 0.79 [0.65, 0.95] | 0.60 [0.45, 0.80] |
| ENTRUST: Edoxaban 60mg/30mg | 0.85 [0.68, 1.05] | 0.59 [0.45, 0.77] |
| total | 0.63 [0.49, 0.78] | |
| Stent Thrombosis (Definite or Probable) | ||
| Study | RR (95% CI) | RR (95% CI) for the Total Effect After Exclusion of Each Single Study |
| AUGUSTUS: Apixaban 5mg/2.5mg | 1.33 [0.46, 3.81] | 1.40 [0.83, 2.34] |
| ENTRUST: Edoxaban 60mg/30mg | 1.34 [0.47, 3.84] | 1.39 [0.83, 2.33] |
| PIONEER: Rivaroxaban 15/10mg | 1.25 [0.34, 4.64] | 1.40 [0.86, 2.30] |
| REDUAL: Dabigatran 110mg | 1.88 [0.80, 4.40] | 1.22 [0.70, 2.11] |
| REDUAL: Dabigatran 150mg | 1.00 [0.35, 2.84] | 1.50 [0.89, 2.51] |
| total | 1.38 [0.87, 2.20] |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Eyileten, C.; Postula, M.; Jakubik, D.; Toma, A.; Mirowska-Guzel, D.; Patti, G.; Renda, G.; Siller-Matula, J.M. Non-Vitamin K Oral Anticoagulants (NOAC) versus Vitamin K Antagonists (VKA) for Atrial Fibrillation with Elective or Urgent Percutaneous Coronary Intervention: A Meta-Analysis with a Particular Focus on Combination Type. J. Clin. Med. 2020, 9, 1120. https://doi.org/10.3390/jcm9041120
Eyileten C, Postula M, Jakubik D, Toma A, Mirowska-Guzel D, Patti G, Renda G, Siller-Matula JM. Non-Vitamin K Oral Anticoagulants (NOAC) versus Vitamin K Antagonists (VKA) for Atrial Fibrillation with Elective or Urgent Percutaneous Coronary Intervention: A Meta-Analysis with a Particular Focus on Combination Type. Journal of Clinical Medicine. 2020; 9(4):1120. https://doi.org/10.3390/jcm9041120
Chicago/Turabian StyleEyileten, Ceren, Marek Postula, Daniel Jakubik, Aurel Toma, Dagmara Mirowska-Guzel, Giuseppe Patti, Giulia Renda, and Jolanta M. Siller-Matula. 2020. "Non-Vitamin K Oral Anticoagulants (NOAC) versus Vitamin K Antagonists (VKA) for Atrial Fibrillation with Elective or Urgent Percutaneous Coronary Intervention: A Meta-Analysis with a Particular Focus on Combination Type" Journal of Clinical Medicine 9, no. 4: 1120. https://doi.org/10.3390/jcm9041120
APA StyleEyileten, C., Postula, M., Jakubik, D., Toma, A., Mirowska-Guzel, D., Patti, G., Renda, G., & Siller-Matula, J. M. (2020). Non-Vitamin K Oral Anticoagulants (NOAC) versus Vitamin K Antagonists (VKA) for Atrial Fibrillation with Elective or Urgent Percutaneous Coronary Intervention: A Meta-Analysis with a Particular Focus on Combination Type. Journal of Clinical Medicine, 9(4), 1120. https://doi.org/10.3390/jcm9041120