Risk, Diagnostic and Predictor Factors for Classical Hodgkin Lymphoma in HIV-1-Infected Individuals: Role of Plasma Exosome-Derived miR-20a and miR-21

 ,
,  ,
, 
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design and Population
2.2. Laboratory Measurements
2.3. Quantification of Plasma Exosome-Derived miRs
2.4. Soluble Plasma Cytokine Quantification
2.5. Cellular Phenotyping: Antibody Staining, Flow Cytometry Acquisition, and Analysis
2.6. B lymphocyte Phenotyping and Activation
2.7. T Lymphocyte Phenotyping and Activation
2.8. Natural Killer Cell Phenotyping and Activation
3. Statistical Analyses
4. Results
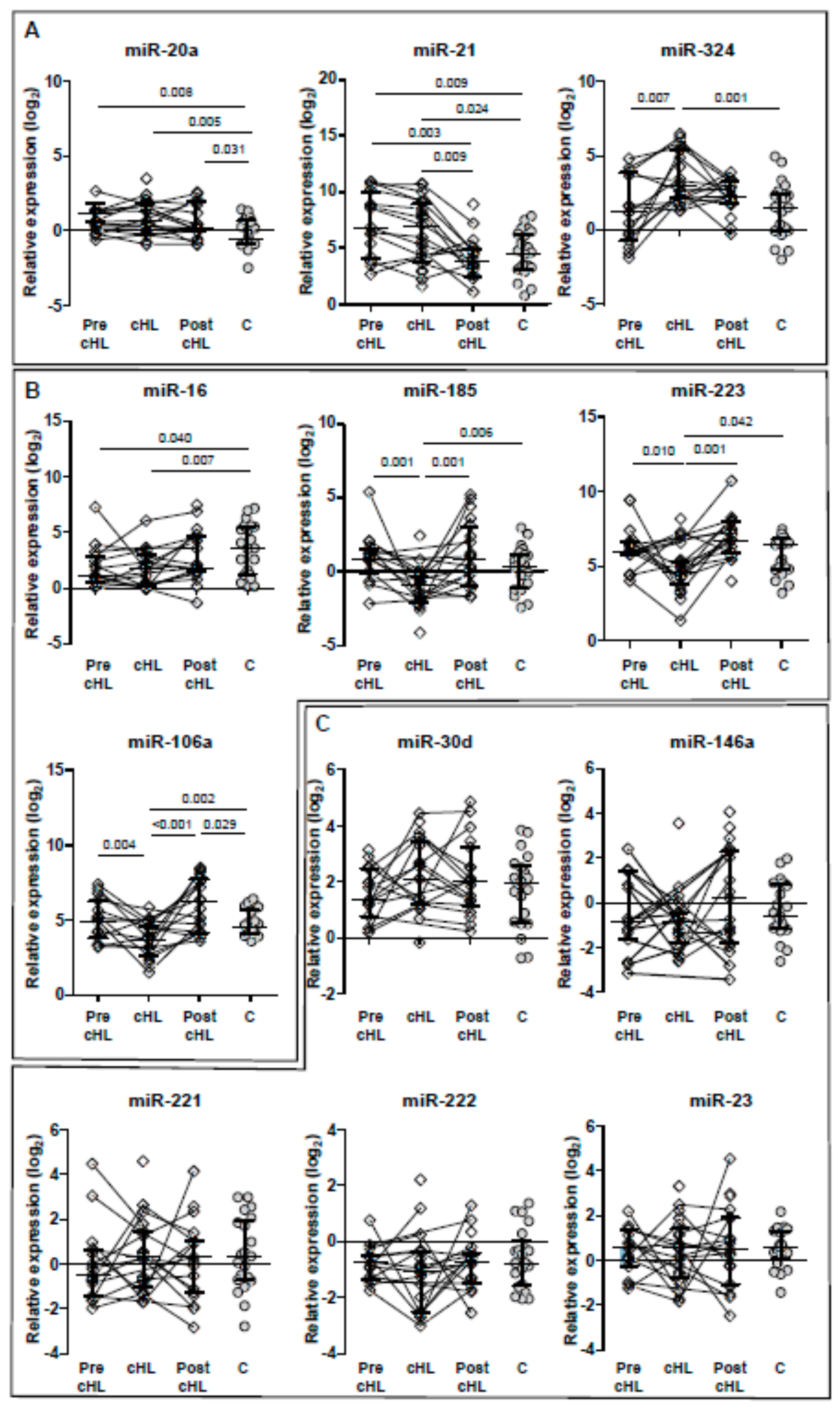
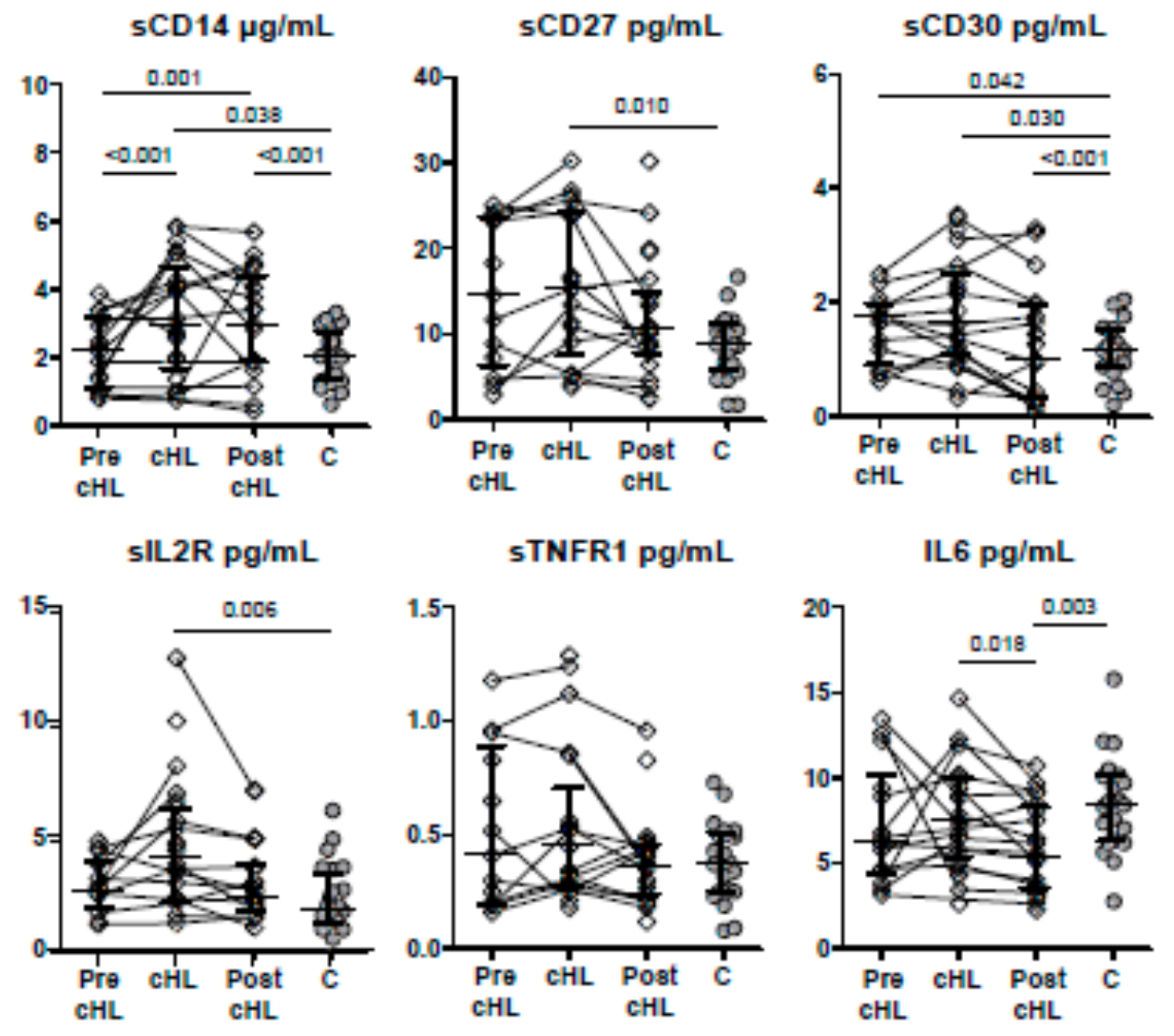
4.1. Biomarkers Profile at Pre-cHL Diagnosis
4.2. Biomarkers Profile at cHL Diagnosis
5. Discussion
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Chiu, C.G.; Smith, D.; Salters, K.A.; Zhang, W.; Kanters, S.; Milan, D.; Montaner, J.S.G.; Coldman, A.; Hogg, R.S.; Wiseman, S.M. Overview of cancer incidence and mortality among people living with HIV/AIDS in British Columbia, Canada: Implications for HAART use and NADM development. BMC Cancer 2017, 17, 270. [Google Scholar] [CrossRef]
- Hentrich, M.; Maretta, L.; Chow, K.U.; Bogner, J.R.; Schürmann, D.; Neuhoff, P.; Jäger, H.; Reichelt, D.; Vogel, M.; Ruhnke, M.; et al. Highly active antiretroviral therapy (HAART) improves survival in HIV-associated Hodgkin’s disease: Results of a multicenter study. Ann. Oncol. 2006, 17, 914–919. [Google Scholar] [CrossRef] [PubMed]
- Uldrick, T.S.; Little, R.F. How I treat classical Hodgkin lymphoma in patients infected with human immunodeficiency virus. Blood 2015, 125, 1226–1235. [Google Scholar] [CrossRef] [PubMed]
- Hleyhel, M.; Hleyhel, M.; Bouvier, A.M.; Belot, A.; Tattevin, P.; Pacanowski, J.; Genet, P.; De Castro, N.; Berger, J.L.; Dupont, C.; et al. Cancer Risk Group of the French Hospital Database on HIV (FHDH-ANRS CO4). Risk of non-AIDS-defining cancers among HIV-1-infected individuals in France between 1997 and 2009: Results from a French cohort. AIDS 2014, 28, 2109–2118. [Google Scholar] [CrossRef] [PubMed]
- Shiels, M.S.; Koritzinsky, E.H.; Clarke, C.A.; Suneja, G.; Morton, L.M.; Engels, E.A. Prevalence of HIV Infection among U.S. Hodgkin lymphoma cases. Cancer Epidemiol. Biomark. 2014, 23, 274–281. [Google Scholar] [CrossRef] [PubMed]
- Franzetti, M.; Ricci, E.; Bonfanti, P. The pattern of non-AIDS-defining cancers in the HIV population: Epidemiology, risk factors and prognosis. A review. Curr. HIV Res. 2019, 17, 1–12. [Google Scholar] [CrossRef]
- Shiels, M.S.; Pfeiffer, R.M.; Gail, M.H.; Hall, H.I.; Li, J.; Chaturvedi, A.K.; Bhatia, K.; Uldrick, T.S.; Yarchoan, R.; Goedert, J.J.; et al. Cancer burden in the HIV-infected population in the United States. J. Natl. Cancer Inst. 2011, 103, 753–762. [Google Scholar] [CrossRef]
- Bedimo, R.J.; McGinnis, K.A.; Dunlap, M.; Rodriguez-Barradas, M.C.; Justice, A.C. Incidence of non-AIDS-defining malignancies in HIV-infected versus non-infected patients in the HAART Era: Impact of immunosuppression. J. Acquir. Immune Defic. Syndr. 2009, 52, 203–208. [Google Scholar] [CrossRef]
- Franceschi, S.; Lise, M.; Clifford, G.M.; Rickenbach, M.; Levi, F.; Maspoli, M.; Bouchardy, C.; Dehler, S.; Jundt, G.; Ess, S.; et al. Changing patterns of cancer incidence in the early-and late-HAART periods: The Swiss HIV Cohort Study. Br. J. Cancer 2010, 103, 416–422. [Google Scholar] [CrossRef]
- Powles, T.; Robinson, D.; Stebbing, J.; Shamash, J.; Nelson, M.; Gazzard, B.; Mandelia, S.; Møller, H.; Bower, M. Highly active antiretroviral therapy and the incidence of non-AIDS-defining cancers in people with HIV infection. J. Clin. Oncol 2009, 27, 884–890. [Google Scholar] [CrossRef]
- Han, X.; Jemal, A.; Hulland, E.; Simard, E.P.; Nastoupil, L.; Ward, E.; Flowers, C.R. HIV infection and survival of lymphoma patients in the era of highly active antiretroviral therapy. Cancer Epidemiol. Prev. Biomark. 2017, 26, 303–311. [Google Scholar] [CrossRef] [PubMed]
- Bohlius, J.; Schmidlin, K.; Boué, F.; Fätkenheuer, G.; May, M.; Caro-Murillo, A.M.; Mocroft, A.; Bonnet, F.; Clifford, G.; Paparizos, V.; et al. Collaboration of Observational HIV Epidemiological Research Europe. HIV-1-related Hodgkin lymphoma in the era of combination antiretroviral therapy: Incidence and evolution of CD4+ T-cell lymphocytes. Blood 2011, 117, 6100–6108. [Google Scholar] [CrossRef]
- Hoffmann, C.; Hentrich, M.; Gillor, D.; Behrens, G.; Jensen, B.; Stoehr, A.; Esser, S.; van Lunzen, J.; Krznaric, I.; Müller, M.; et al. Hodgkin lymphoma is as common as non-Hodgkin lymphoma in HIV-positive patients with sustained viral suppression and limited immune deficiency: A prospective cohort study. HIV Med. 2015, 16, 261–264. [Google Scholar] [CrossRef] [PubMed]
- Simard, E.P.; Pfeiffer, R.M.; Engels, E.A. Spectrum of cancer risk late after AIDS onset in the United States. Arch. Intern. Med. 2010, 170, 1337–1345. [Google Scholar] [CrossRef] [PubMed]
- Martis, N.; Mounier, N. Hodgkin lymphoma in patients with HIV infection: A review. Curr. Hematol. Malig. Rep. 2012, 7, 228–234. [Google Scholar] [CrossRef]
- Pantanowitz, L.; Carbone, A.; Dolcetti, R. Microenvironment and HIV-related lymphomagenesis. Semin. Cancer Biol. 2015, 34, 52–57. [Google Scholar] [CrossRef]
- De Paoli, P.; Carbone, A. Microenvironmental abnormalities induced by viral cooperation: Impact on lymphomagenesis. Semin. Cancer Biol. 2015, 34, 70–80. [Google Scholar] [CrossRef]
- Tanaka, L.F.; Latorre, R.D.; Gutierrez, E.B.; Heumann, C.; Herbinger, K.H.; Froeschl, G. Trends in the incidence of AIDS-defining and non-AIDS-defining cancers in people living with AIDS: A population-based study from São Paulo, Brazil. Int. J. STD AIDS 2017, 28, 1190–1198. [Google Scholar] [CrossRef]
- Kowalkowski, M.A.; Mims, M.A.; Day, R.S.; Du, X.L.; Chan, W.; Chiao, E.Y. Longer duration of combination antiretroviral therapy reduces the risk of Hodgkin lymphoma: A cohort study of HIV-infected male veterans. Cancer Epidemiol. 2014, 38, 386–392. [Google Scholar] [CrossRef]
- Tanday, S. HBV and HCV co-infection increases cancer risk in HIV patients. Lancet Oncol. 2016, 17, e484. [Google Scholar] [CrossRef]
- Carbone, A.; Gloghini, A.; Caruso, A.; De Paoli, P.; Dolcetti, R. The impact of EBV and HIV infection on the microenvironmental niche underlying Hodgkin lymphoma pathogenesis. Int. J. Cancer 2017, 140, 1233–1245. [Google Scholar] [CrossRef] [PubMed]
- Thompson, L.D.; Fisher, S.I.; Chu, W.S.; Nelson, A.; Abbondanzo, S.L. HIV-associated Hodgkin lymphoma: Clinicopathologic and immunophenotypic study of 45 cases. Am. J. Clin. Pathol. 2004, 121, 727–738. [Google Scholar] [CrossRef] [PubMed]
- Besson, C.; Lancar, R.; Prevot, S.; Brice, P.; Meyohas, M.C.; Marchou, B.; Gabarre, J.; Bonnet, F.; Goujard, C.; Lambotte, O.; et al. High risk features contrast with favorable outcomes in HIV-associated Hodgkin lymphoma in the modern cART era, ANRS CO16 LYMPHOVIR Cohort. Clin. Infect. Dis. 2015, 61, 1469–1475. [Google Scholar] [CrossRef] [PubMed]
- Sorigué, M.; García, O.; Tapia, G.; Baptista, M.J.; Moreno, M.; Mate, J.L.; Sancho, J.M.; Feliu, E.; Ribera, J.M.; Navarro, J.T. HIV-infection has no prognostic impact on advanced-stage Hodgkin lymphoma. AIDS 2017, 31, 1445–1449. [Google Scholar] [CrossRef] [PubMed]
- Ul-Haq, I.; Dalla Pria, A.; Suardi, E.; Pinato, D.J.; Froeling, F.; Forni, J.; Randell, P.; Bower, M. Blood Epstein-Barr virus DNA does not predict outcome in advanced HIV-associated Hodgkin lymphoma. Med. Oncol. 2018, 35, 53. [Google Scholar] [CrossRef]
- Jacobson, C.A.; Abramson, J.S. HIV-associated Hodgkin’s lymphoma: Prognosis and therapy in the era of cART. Adv. Hematol. 2012, 2012, 507257. [Google Scholar] [CrossRef] [PubMed]
- Guo, H.; Ingolia, N.T.; Weissman, J.S.; Bartel, D.P. Mammalian microRNAs predominantly act to decrease target mRNA levels. Nature 2010, 466, 835–840. [Google Scholar] [CrossRef]
- Bartel, D.P. MicroRNAs: Genomics, biogenesis, mechanism, and function. Cell 2004, 116, 281–297. [Google Scholar] [CrossRef]
- Lodish, H.F.; Zhou, B.; Liu, G.; Chen, C.Z. Micromanagement of the immune system by microRNAs. Nat. Rev. Immunol. 2008, 8, 120–130. [Google Scholar] [CrossRef]
- Swaminathan, G.; Navas-Martín, S.; Martín-García, J. MicroRNAs and HIV-1 infection: Antiviral activities and beyond. J. Mol. Biol. 2014, 426, 1178–1197. [Google Scholar] [CrossRef]
- Narla, V.; Bhakta, N.; Freedman, J.E.; Tanriverdi, K.; Maka, K.; Deeks, S.G.; Ganz, P.; Hsue, P. Unique circulating microRNA profiles in HIV infection. J. Acquir. Immune Defic. Syndr. 2018, 79, 644–650. [Google Scholar] [CrossRef] [PubMed]
- Duskova, K.; Nagilla, P.; Le, H.-S.; Iyer, P.; Thalamuthu, A.; Martinson, J.; Bar-Joseph, Z.; Buchanan, W.; Rinaldo, C.; Ayyavoo, V. MicroRNA regulation and its effect on cellular transcriptome in human immunodeficiency virus 1 (HIV-1) infected individuals with distinct viral load and CD4 cell counts. BMC Infect. Dis. 2013, 13, 250. [Google Scholar] [CrossRef] [PubMed]
- Su, B.; Fu, Y.; Liu, Y.; Wu, H.; Ma, P.; Zeng, W.; Zhang, T.; Lian, S.; Wu, H. Potential application of microRNA profiling to the diagnosis and prognosis of HIV-1 infection. Front. Microbiol. 2018, 9, 3185. [Google Scholar] [CrossRef] [PubMed]
- Squillace, N.; Bresciani, E.; Torsello, A.; Bandera, A.; Sabbatini, F.; Giovannetti, C.; Giunta, G.; Rovati, L.; Del Bene, M.; Locatelli, V.; et al. Changes in subcutaneous adipose tissue microRNA expression in HIV-infected individuals. J. Antimicrob. Chemother. 2014, 69, 3067–3075. [Google Scholar] [CrossRef]
- Caro-Murillo, A.M.; Castilla, J.; Pérez-Hoyos, S.; Miro, J.M.; Podzamczer, D.; Rubio, R.; Riera, M.; Viciana, P.; Lopez, J.A.; Iribarren, J.A.; et al. Spanish cohort of naïve HIV-infected individuals (CoRIS): Rationale, organization and initial results. Enferm. Infecc. Microbiol. Clin. 2007, 25, 23–31. [Google Scholar] [CrossRef]
- Garcia-Merino, I.; de las Cuevas, N.; Jimenez, J.L.; Gallego, J.; Gomez, C.; Prieto, C.; Serramia, M.J.; Lorente, R.; Munoz-Fernandez, M.; BioBank. The Spanish HIV BioBank: A model of cooperative HIV research. Retrovirology 2009, 6, 27. [Google Scholar] [CrossRef] [PubMed]
- Ruiz-de-León, M.J.; Jiménez-Sousa, M.A.; Moreno, S.; Garcia, M.; Gutierrez-Rivas, M.; Leon, A.; Montero-Alonso, M.; Gonzalez-Garcia, J.; Resino, S.; Rallon, N.; et al. Lower expression of plasma-derived exosome miR-21 levels in HIV-1 elite controllers with decreasing CD4 T cell count. J. Microbiol. Immunol. Infect. 2019, 52, 667–671. [Google Scholar] [CrossRef]
- Livak, K.J.; Schmittgen, T.D. Analysis of relative gene expression data using real-time quantitative PCR and the 2 (-Delta Delta C(T)) Method. Methods 2001, 25, 402–408. [Google Scholar] [CrossRef]
- Mestdagh, P.; Van Vlierberghe, P.; De Weer, A.; Muth, D.; Westermann, F.; Speleman, F.; Vandesompele, J. A novel and universal method for microRNA RT-qPCR data normalization. Genome Biol. 2009, 10, R64. [Google Scholar] [CrossRef]
- Farina, N.H.; Wood, M.E.; Perrapato, S.D.; Francklyn, C.S.; Stein, G.S.; Stein, J.L.; Lian, J.B. Standardizing analysis of circulating microRNA: Clinical and biological relevance. J. Cell. Biochem. 2014, 115, 805–811. [Google Scholar] [CrossRef]
- Allegra, A.; Alonci, A.; Campo, S.; Penna, G.; Petrungaro, A.; Gerace, D.; Musolino, C. Circulating microRNAs: New biomarkers in diagnosis, prognosis and treatment of cancer. Int. J. Oncol. 2012, 41, 1897–1912. [Google Scholar] [CrossRef] [PubMed]
- Cordeiro, A.; Monzó, M.; Navarro, A. Non-Coding RNAs in Hodgkin Lymphoma. Int. J. Mol. Sci. 2017, 18, 1154. [Google Scholar] [CrossRef] [PubMed]
- Gibcus, J.H.; Tan, L.P.; Harms, G.; Schakel, R.N.; de Jong, D.; Blokzijl, T.; Möller, P.; Poppema, S.; Kroesen, B.J.; van den Berg, A. Hodgkin lymphoma cell lines are characterized by a specific miRNA expression profile. Neoplasia 2009, 11, 166–176. [Google Scholar] [CrossRef] [PubMed]
- Navarro, A.; Gaya, A.; Martinez, A.; Urbano-Ispizua, A.; Pons, A.; Balagué, O.; Gel, B.; Abrisqueta, P.; Lopez-Guillermo, A.; Artells, R. MicroRNA expression profiling in classic Hodgkin lymphoma. Blood 2008, 111, 2825–2832. [Google Scholar] [CrossRef] [PubMed]
- Paydas, S.; Acikalin, A.; Ergin, M.; Celik, H.; Yavuz, B.; Tanriverdi, K. Micro-RNA (miRNA) profile in Hodgkin lymphoma: Association between clinical and pathological variables. Med. Oncol. 2016, 33, 34. [Google Scholar] [CrossRef]
- Van Vlierberghe, P.; de Weer, A.; Mestdagh, P.; Feys, T.; de Preter, K.; de Paepe, P.; Lambein, K.; Vandesompele, J.; van Roy, N.; Verhasselt, B. Comparison of miRNA profiles of microdissected Hodgkin/Reed-Sternberg cells and Hodgkin cell lines versus cd77+B-cells reveals a distinct subset of differentially expressed miRNAs. Br. J. Haematol. 2009, 147, 686–690. [Google Scholar] [CrossRef]
- Wang, J.; Yin, K.; Lv, X.; Yang, Q.; Shao, M.; Liu, X.; Sun, H. MicroRNA-24-3p regulates Hodgkin’s lymphoma cell proliferation, migration and invasion by targeting DEDD. Oncol. Lett. 2019, 17, 365–371. [Google Scholar] [CrossRef]
- Zhu, M.; Xu, Z.; Wang, K.; Wang, N.; Zhu, M.; Wang, S. MicroRNA and gene networks in human Hodgkin’s lymphoma. Mol. Med. Rep. 2013, 8, 1747–1754. [Google Scholar] [CrossRef]
- Sekar, D.; Hairul Islam, V.I.; Thirugnanasambantham, K.; Saravanan, S. Relevance of miR-21 in HIV and non-HIV-related lymphomas. Tumour. Biol. 2014, 35, 8387–8393. [Google Scholar] [CrossRef]
- Levin, L.I.; Breen, E.C.; Birmann, B.M.; Batista, J.L.; Magpantay, L.I.; Li, Y.; Ambinder, R.F.; Mueller, N.E.; Martínez-Maza, O. Elevated serum levels of sCD30 and IL6 and detectable IL10 precede classical Hodgkin lymphoma diagnosis. Cancer Epidemiol. Biomark. Prev. 2017, 26, 1114–1123. [Google Scholar] [CrossRef]
- Purdue, M.P.; Lan, Q.; Hoffman-Bolton, J.; Hildesheim, A.; Callahan, C.L.; Strickland, P.; Visvanathan, K.; Rothman, N. Circulating sCD27 and sCD30 in pre-diagnostic samples collected fifteen years apart and future non-Hodgkin lymphoma risk. Int. J. Cancer 2019, 144, 1780–1785. [Google Scholar] [CrossRef] [PubMed]
- Gottesman, S. CD30: Receptor, marker, target. Path Lab. Med. Int. 2016, 8, 27–36. [Google Scholar] [CrossRef]
- Michel, T.; Poli, A.; Cuapio, A.; Briquemont, B.; Iserentant, G.; Ollert, M.; Zimmer, J. Human CD56bright NK Cells: An Update. J. Immunol. 2016, 196, 2923–2931. [Google Scholar] [CrossRef] [PubMed]
- Cooper, M.A.; Fehniger, T.A.; Turner, S.C.; Chen, K.S.; Ghaheri, B.A.; Ghayur, T.; Carson, W.E.; Caligiuri, M.A. Human natural killer cells: A unique innate immunoregulatory role for the CD56 (bright) subset. Blood 2001, 97, 3146–3151. [Google Scholar] [CrossRef] [PubMed]
- Chiu, J.; Ernst, D.M.; Keating, A. Acquired natural killer cell dysfunction in the tumor microenvironment of classic Hodgkin lymphoma. Front. Immunol. 2018, 9, 267. [Google Scholar] [CrossRef] [PubMed]
- Serrano-Villar, S.; Pérez-Elías, M.J.; Dronda, F.; Casado, J.L.; Moreno, A.; Royuela, A.; Pérez-Molina, J.A.; Sainz, T.; Navas, E.; Hermida, J.M.; et al. Increased risk of serious non-AIDS-related events in HIV-infected subjects on antiretroviral therapy associated with a low CD4/CD8 ratio. PLoS ONE 2014, 9, e85798. [Google Scholar] [CrossRef]
- Hoffmann, C.; Schommers, P.; Wolf, E.; Müller, M.; Schultze, A.; Krznaric, I.; Stoehr, A.; Wolf, T.; Fäktenheuer, G.; Stier, B.; et al. CD4+ and CD8+ T-cell kinetics in aviremic HIV-infected patients developing Hodgkin or non-Hodgkin lymphoma. AIDS 2016, 30, 753–760. [Google Scholar] [CrossRef]
- Gupta, R.K.; Marks, M.; Edwards, S.G.; Smith, K.; Fletcher, K.; Lee, S.M.; Ramsay, A.; Copas, A.J.; Miller, R.F. A declining CD4 count and diagnosis of HIV-associated Hodgkin lymphoma: Do prior clinical symptoms and laboratory abnormalities aid diagnosis? PLoS ONE 2014, 9, e87442. [Google Scholar] [CrossRef]
- Sánchez-Espiridión, B.; Martín-Moreno, A.M.; Montalbán, C.; Figueroa, V.; Vega, F.; Younes, A.; Medeiros, L.J.; Alvés, F.J.; Canales, M.; Estévez, M. MicroRNA signatures and treatment response in patients with advanced classical Hodgkin lymphoma. Br. J. Haematol. 2013, 162, 336–347. [Google Scholar] [CrossRef]
- Jones, K.; Nourse, J.P.; Keane, C.; Bhatnagar, A.; Gandhi, M.K. Plasma microRNA are disease response biomarkers in classical Hodgkin lymphoma. Clin. Cancer Res. 2014, 20, 253–264. [Google Scholar] [CrossRef]
- Biswas, S.; Haleyurgirisetty, M.; Lee, S.; Hewlett, I.; Devadas, K. Development and validation of plasma miRNA biomarker signature panel for the detection of early HIV-1 infection. EBioMedicine 2019, 43, 307–316. [Google Scholar] [CrossRef] [PubMed]
- Marri, P.R.; Hodge, L.S.; Maurer, M.J.; Ziesmer, S.C.; Slager, S.L.; Habermann, T.M.; Link, B.K.; Cerhan, J.R.; Novak, A.J.; Ansell, S.M. Prognostic significance of pretreatment serum cytokines in classical Hodgkin lymphoma. Clin. Cancer Res. 2013, 19, 6812–6819. [Google Scholar] [CrossRef] [PubMed]
- Umino, K.; Fujiwara, S.I.; Ikeda, T.; Kawaguchi, S.I.; Toda, Y.; Ito, S.; Ochi, S.I.; Nagayama, T.; Mashima, K.; Minakata, D.; et al. Predictive value of soluble interlukin-2 receptor level at diagnosis on the outcome for patients with classical Hodgkin lymphoma treated with ABVD with or without radiotherapy. Ann. Hematol. 2019, 98, 2121–2129. [Google Scholar] [CrossRef] [PubMed]
- Plattel, W.J.; Alsada, Z.N.; van Imhoff, G.W.; Diepstra, A.; van den Berg, A.; Visser, L. Biomarkers for evaluation of treatment response in classical Hodgkin lymphoma: Comparison of sGalectin-1, sCD163 and sCD30 with TARC. Br. J. Haematol. 2016, 175, 868–875. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| HIV-1-Infected Individuals with Classical Hodgkin Lymphoma N = 37 | HIV-1-Infected Individuals (Controls) N = 74 | p | |
|---|---|---|---|
| Adjusted factors | |||
| Age at HIV-1 diagnosis (years) | 34 [29–43] | 31 [26–38] | ns |
| Age at cHL or sample (years) | 45 [38–46] | 44 [39–47] | ns |
| Gender (female) | 6 (16.2%) | 12 (16.2%) | ns |
| HIV-1 transmission risk | |||
| MSM | 18 (48.6%) | 36 (48.6%) | ns |
| Heterosexual | 10 (27.0%) | 20 (27.0%) | ns |
| Former injecting drug users | 6 (16.2%) | 12 (16.2%) | ns |
| Other | 3 (8.1%) | 6 (8.1%) | ns |
| Anti-HCV antibodies | |||
| Positive | 12 (32.4%) | 24 (32.4%) | ns |
| Negative | 24 (64.8%) | 50 (67.6%) | |
| Unknown | 1 (2.7%) | 0 | |
| HIV-1 treatment | |||
| cART | 28 (75.6%) | 58 (76.3%) | ns |
| None | 9 (24.3%) | 18 (23.7%) | ns |
| HIV-1 load (RNA copies/mL) * | 4.8 [3.5–5.4] | 4.5 [4.2–5.1] | ns |
| Not adjusted factors | |||
| Time from HIV-1 diagnosis to cHL or sample (months) | 63 [16–103] | 129 [52–187] | 0.031 |
| Time from HIV-1 diagnosis to ART initiation (months) | 15 [1–54] | 17 [3–62] | 0.816 |
| ART exposure (months)** | 47 [15–126] | 96 [42–158] | 0.074 |
| Pre-ART HIV-1 load (RNA copies/mL) | 5.1 [4.4–5.5] | 5.0 [4.5–5.5] | 0.677 |
| CD4 nadir (cells/mm3) | 120 [70–241] | 196 [83–292] | 0.119 |
| CD4 count (cells/mm3) | 259 [115–385] | 511 [285–695] | <0.001 |
| CD4 T cell percentage | 20 [13.7–30] | 24.4 [17.5–30.6] | 0.516 |
| CD8 count (cells/mm3) | 554 [370–892] | 872 [650–1072] | 0.018 |
| CD8 T cell percentage | 53.7 [32.7–60.2] | 42.9 [36.8–53.5] | 0.174 |
| CD4/CD8 ratio | 0.48 [0.32–0.81] | 0.66 [0.47–0.87] | 0.046 |
| Pre-cHL CD4 count (cells/mm3) | 378 [202–545] | 515 [285–695] | 0.142 |
| Post cHL CD4 count (cells/mm3) | 338 [261–410] | 515 [285–695] | 0.006 |
| N = 37 | |
|---|---|
| Pathologic Stage | |
| I | 4 (10.8%) |
| II | 3 (8.1%) |
| III | 4 (10.8%) |
| IV | 15 (40.5%) |
| Unknown | 11 (29.7%) |
| Classification (cHL) | |
| Nodular sclerosis | 8 (21.6%) |
| Mixed cellularity | 19 (51.3%) |
| Lymphocyte depleted | 1 (2.7%) |
| Lymphocyte-rich | 2 (5.4%) |
| Unknown | 7 (18.9%) |
| Pre cHL | cHL | Post cHL | Control Group | p | |||
|---|---|---|---|---|---|---|---|
| N = 6 | N = 9 | N = 9 | N = 9 | Pre cHL vs. Control | cHL vs. Control | Post cHL vs. Control | |
| Natural killer cell subsets | |||||||
| CD56dimCD16- | 9.17 [8.43–11.45] | 8.99 [7.94–12.29] | 6.75 [6.08–9.44] | 9.75 [8.18–10.22] | 0.413 | 0.789 | 0.169 |
| CD56brCD16- | 8.53 [6.51–9.08] | 5.64 [3.42–7.41] | 10.21 [8.06–12.34] | 12.24 [8.83–13.76] | 0.050 | 0.003 | 0.290 |
| CD56brCD16+ | 3.00 [2.14–4.30] | 5.24 [3.61–7.15] | 4.04 [3.52–4.72] | 2.31 [1.24–3.59] | 0.224 | 0.010 | 0.019 |
| CD56dimCD16+ | 56.28 [54.58–60.99] | 52.94 [47.37–57.05] | 52.24 [45.17–61.00] | 56.77 [48.15–61.65] | 0.866 | 0.258 | 0.495 |
| CD56-CD16+ | 21.55 [16.24–27.56] | 25.98 [23.85–27.66] | 26.41 [17.53–31.57] | 21.46 [17.69–26.52] | 0.968 | 0.161 | 0.278 |
| Inhibitory CD94+ | 22.03 [18.11–27.72] | 20.36 [17.96–24.46] | 20.43 [16.19–22.75] | 17.89 [14.05–19.06] | 0.088 | 0.040 | 0.077 |
| Activating NKp46+ | 7.87 [6.51–10.63] | 8.37 [5.87–9.96] | 6.74 [5.98–9.19] | 11.24 [9.04–12.16] | 0.076 | 0.031 | 0.012 |
| Activating NKp30+ | 1.06 [0.86–1.25] | 0.98 [0.78–1.28] | 1.14 [0.81–1.42] | 1.36 [0.97–1.57] | 0.087 | 0.052 | 0.234 |
| Activating NKG2D+ | 1.82 [1.48–2.04] | 1.85 [1.47–2.22] | 1.74 [1.46–2.14] | 2.23 [1.89–2.54] | 0.055 | 0.083 | 0.077 |
| Lymphocyte B cell subsets | |||||||
| Resting memory | 25.83 [13.92–32.90] | 32.56 [24.37–39.91] | 32.42 [24.16–35.01] | 22.88 [17.07–28.25] | 0.689 | 0.048 | 0.139 |
| Activated memory | 27.58 [18.33–32.22] | 16.95 [11.14–22.73] | 22.57 [20.20–27.31] | 26.15 [19.10–32.11] | 0.823 | 0.018 | 0.518 |
| Naive | 29.34 [20.56–38.41] | 40.50 [28.62–46.21] | 31.58 [24.65–34.01] | 31.02 [28.97–40.52] | 0.571 | 0.347 | 0.135 |
| Tissue-like memory | 14.79 [9.25–23.87] | 9.90 [4.47–15.11] | 12.24 [10.26–20.16] | 10.36 [6.35–18.98] | 0.324 | 0.477 | 0.702 |
| Immature/Transitional | 2.27 [1.41–3.41] | 1.17 [0.75–3.14] | 1.98 [1.55–3.19] | 1.68 [1.22–2.60] | 0.456 | 0.993 | 0.318 |
| Plasmablast | 0.74 [0.53–1.15] | 0.11 [0.07–0.80] | 0.67 [0.14–0.77] | 0.14 [0.09–0.79] | 0.224 | 0.745 | 0.304 |
| Lymphocyte CD4 T cell subsets | |||||||
| Naive | 18.60 [10.94–21.02] | 22.82 [16.59–27.61] | 18.57 [10.33–19.85] | 17.55 [11.62–23.68] | 0.880 | 0.155 | 0.496 |
| Central memory | 30.20 [26.84–38.63] | 43.48 [38.52–46.08] | 38.36 [30.99–40.81] | 35.98 [24.26–45.45] | 0.558 | 0.072 | 0.593 |
| Effector memory | 47.90 [40.16–51.80] | 33.48 [24.14–39.56] | 40.84 [39.26–53.19] | 41.51 [30.42–63.57] | 0.827 | 0.050 | 0.945 |
| TemRA+ | 3.40 [1.91–5.87] | 1.36 [0.25–2.80] | 1.80 [0.34–2.32] | 1.24 [0.80–3.17] | 0.067 | 0.582 | 0.526 |
| CD4 T cell activation | 4.66 [3.57–5.63] | 4.86 [3.37–5.31] | 4.21 [3.85–5.69] | 3.45 [2.67–6.34] | 0.661 | 0.897 | 0.684 |
| CD4 T cell exhaustion | 47.79 [43.14–49.37] | 47.98 [42.66–52.52] | 51.32 [47.98–58.63] | 53.82 [37.06–56.86] | 0.636 | 0.958 | 0.369 |
| Lymphocyte CD8 T cell subsets | |||||||
| Naive | 21.09 [16.79–24.65] | 17.73 [14.73–19.86] | 21.33 [13.89–27.38] | 18.84 [13.12–24.70] | 0.762 | 0.952 | 0.612 |
| Central memory | 12.88 [10.01–18.53] | 24.70 [20.29–35.24] | 17.41 [13.45–21.08] | 11.23 [5.46–13.23] | 0.353 | 0.006 | 0.019 |
| Effector memory | 55.40 [47.09–61.27] | 41.33 [36.80–52.43] | 55.32 [49.14–58.14] | 58.94 [53.39–65.41] | 0.481 | 0.011 | 0.225 |
| TemRA+ | 9.49 [6.45–12.65] | 9.31 [6.24–13.91] | 8.31 [7.19–11.58] | 10.29 [6.59–17.60] | 0.838 | 0.958 | 0.311 |
| CD8 T cell activation | 17.35 [13.11–18.77] | 15.54 [14.90–17.89] | 13.76 [13.07–18.03] | 12.24 [9.48–15.86] | 0.050 | 0.031 | 0.115 |
| CD8 T cell exhaustion | 64.40 [61.96–73.23] | 65.23 [60.17–68.62] | 68.21 [58.43–72.53] | 62.99 [55.31–67.54] | 0.406 | 0.532 | 0.386 |
| Unadjusted | Adjusted | |||
|---|---|---|---|---|
| p | B (CI 95%) | p | B (CI 95%) | |
| Pre-cHL | ||||
| miR-16 | 0.044 | 0.693 (0.485–0.991) | ||
| miR-20a | 0.011 | 3.272 (1.307–8.192) | 0.049 | 2.784 (1.007–7.700) |
| miR-21 | 0.009 | 1.564 (1.117–2.189) | 0.035 | 1.478 (1.028–2.124) |
| sCD27 | 0.033 | 1.142 (1.011–1.291) | ||
| sCD30 | 0.042 | 4.190 (1.053–16.665) | ||
| cHL diagnosis | ||||
| Nadir CD4 count | 0.080 | 0.997 (0.994–1.000) | ||
| 11CD4/CD8 ratio | 0.059 | 0.167 (0.026–1.074) | ||
| miR-20a | 0.007 | 2.539 (1.290–4.999) | 0.011 | 4.956 (1.443–17.017) |
| miR-16 | 0.011 | 0.636 (0.450–0.900) | ||
| miR-106a | 0.005 | 0.295 (0.126–0.690) | ||
| miR-21 | 0.020 | 1.386 (1.053–1.824) | ||
| miR-324 | 0.003 | 2.014 (1.260–3.218) | ||
| miR-185 | 0.034 | 0.524 (0.288–0.951) | ||
| miR-223 | 0.039 | 0.611 (0.383–0.975) | ||
| sCD14 | 0.017 | 1.971 (1.130–3.437) | ||
| sCD27 | 0.007 | 1.188 (1.047–1.347) | ||
| sCD30 | 0.017 | 3.406 (1.242–9.338) | ||
| sIL2R | 0.009 | 1.762 (1.153–2.694) | ||
| ROC Curve | Likelihood Ratio (LR) | ||||||||
|---|---|---|---|---|---|---|---|---|---|
| AUC | p | Error | Range | Cut Off | Sensitivity | Specificity | LR+ | LR− | |
| Pre-cHL | |||||||||
| miR-20a | 0.762 | 0.008 | 0.079 | 0.607–0.917 | −0.375 | 93.8 | 57.1 | 2.19 | 0.11 |
| miR-21 | 0.756 | 0.010 | 0.085 | 0.589–0.922 | 6.171 | 66.7 | 71.4 | 2.33 | 0.47 |
| Combined | |||||||||
| miR-20a+miR-21a | 0.832 | 0.001 | 0.070 | 0.694–0.970 | 0.462 | 80.0 | 85.7 | 5.6 | 0.23 |
| cHL diagnosis | |||||||||
| miR-20a | 0.754 | 0.005 | 0.074 | 0.608–0.900 | −0.375 | 85.7% | 57.1% | 2 | 0.25 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hernández-Walias, F.J.; Vázquez, E.; Pacheco, Y.; Rodríguez-Fernández, J.M.; Pérez-Elías, M.J.; Dronda, F.; Casado, J.L.; Moreno, A.; Hermida, J.M.; Quereda, C.; et al. Risk, Diagnostic and Predictor Factors for Classical Hodgkin Lymphoma in HIV-1-Infected Individuals: Role of Plasma Exosome-Derived miR-20a and miR-21. J. Clin. Med. 2020, 9, 760. https://doi.org/10.3390/jcm9030760
Hernández-Walias FJ, Vázquez E, Pacheco Y, Rodríguez-Fernández JM, Pérez-Elías MJ, Dronda F, Casado JL, Moreno A, Hermida JM, Quereda C, et al. Risk, Diagnostic and Predictor Factors for Classical Hodgkin Lymphoma in HIV-1-Infected Individuals: Role of Plasma Exosome-Derived miR-20a and miR-21. Journal of Clinical Medicine. 2020; 9(3):760. https://doi.org/10.3390/jcm9030760
Chicago/Turabian StyleHernández-Walias, Francisco J., Esther Vázquez, Yolanda Pacheco, José M. Rodríguez-Fernández, María J. Pérez-Elías, Fernando Dronda, José L. Casado, Ana Moreno, José M. Hermida, Carmen Quereda, and et al. 2020. "Risk, Diagnostic and Predictor Factors for Classical Hodgkin Lymphoma in HIV-1-Infected Individuals: Role of Plasma Exosome-Derived miR-20a and miR-21" Journal of Clinical Medicine 9, no. 3: 760. https://doi.org/10.3390/jcm9030760
APA StyleHernández-Walias, F. J., Vázquez, E., Pacheco, Y., Rodríguez-Fernández, J. M., Pérez-Elías, M. J., Dronda, F., Casado, J. L., Moreno, A., Hermida, J. M., Quereda, C., Hernando, A., Tejerina-Picado, F., Asensi, V., Galindo, M. J., Leal, M., Moreno, S., & Vallejo, A. (2020). Risk, Diagnostic and Predictor Factors for Classical Hodgkin Lymphoma in HIV-1-Infected Individuals: Role of Plasma Exosome-Derived miR-20a and miR-21. Journal of Clinical Medicine, 9(3), 760. https://doi.org/10.3390/jcm9030760