Impact of New Chemotherapy Regimens on the Treatment Landscape and Survival of Locally Advanced and Metastatic Pancreatic Cancer Patients

 , ,
, ,
Abstract
:1. Introduction
2. Experimental Section
2.1. Study Design
2.2. Statistics
3. Results
3.1. Patient Characteristics
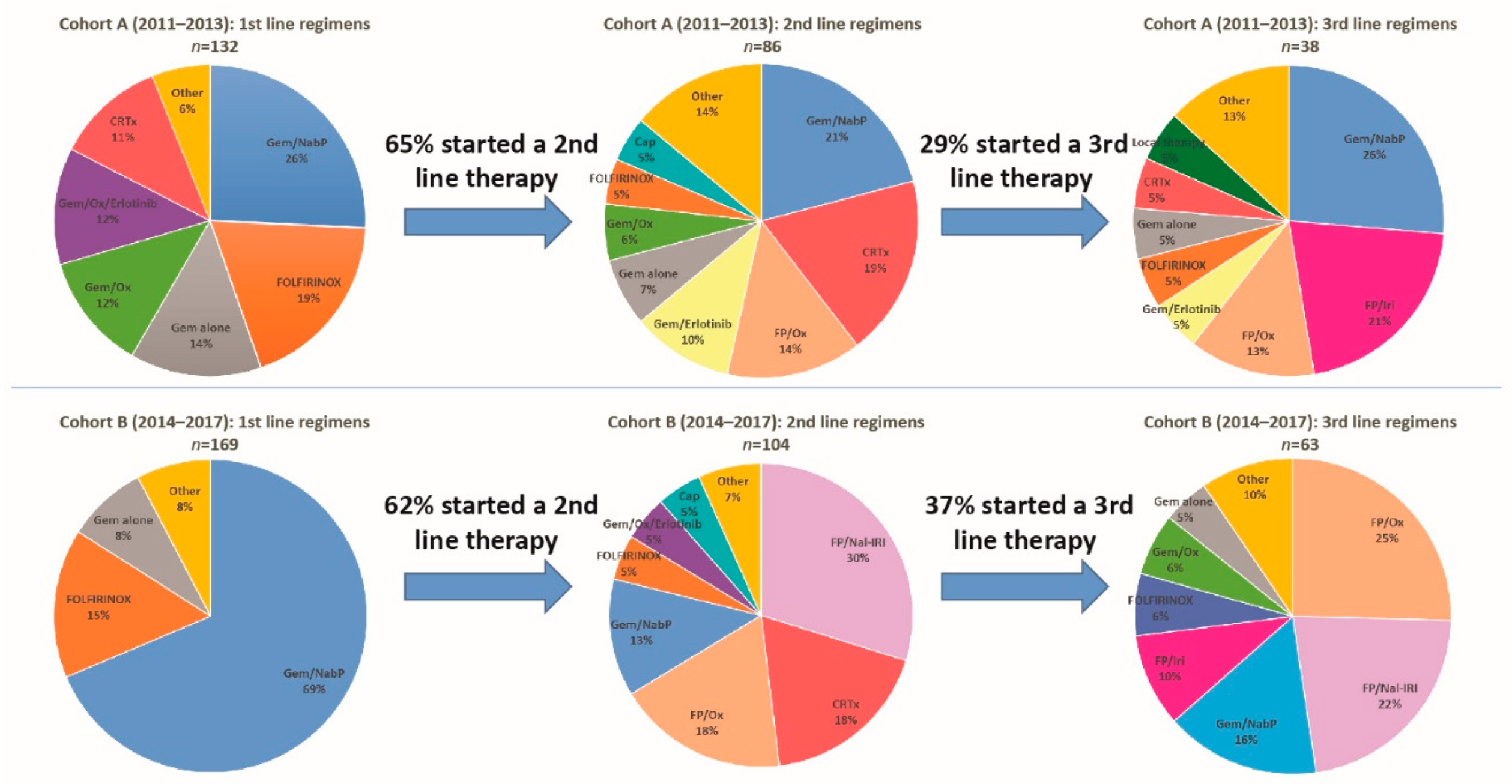
3.2. Treatment Landscape
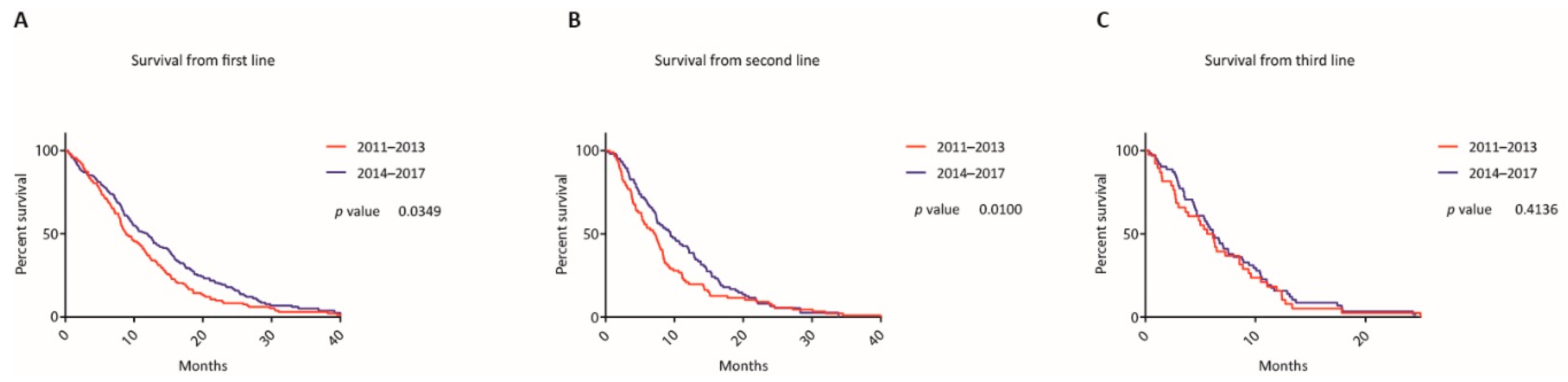
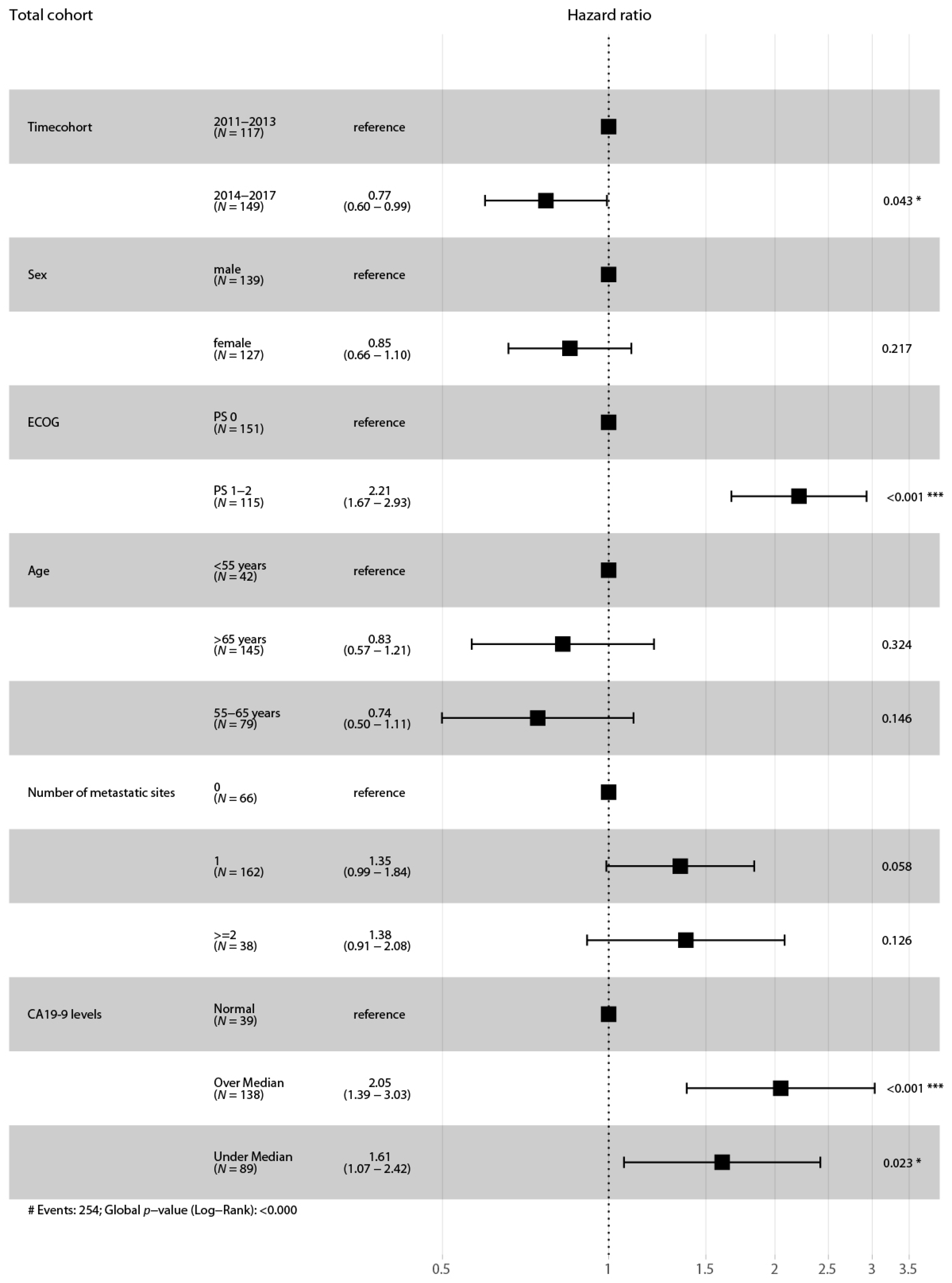
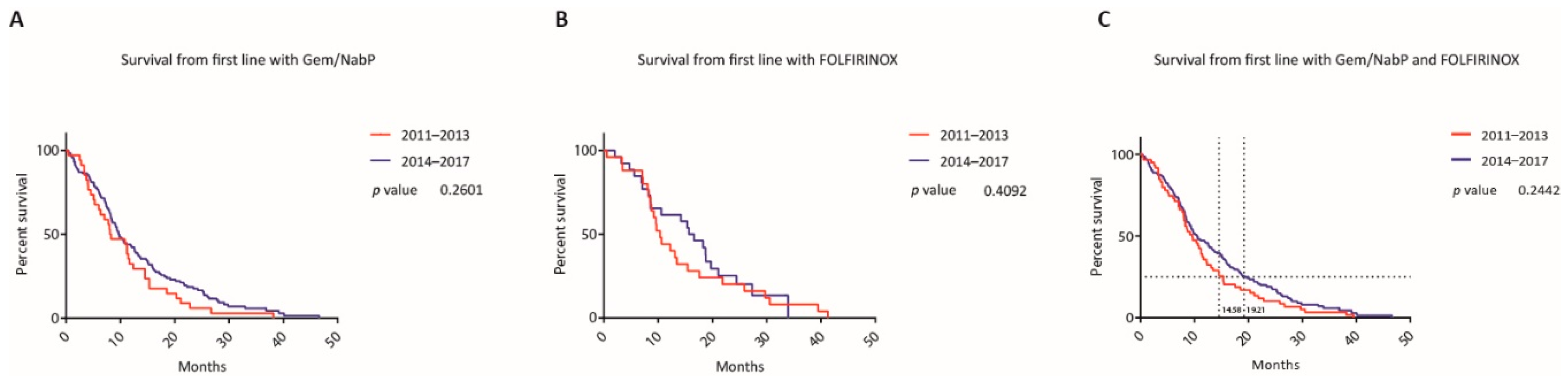
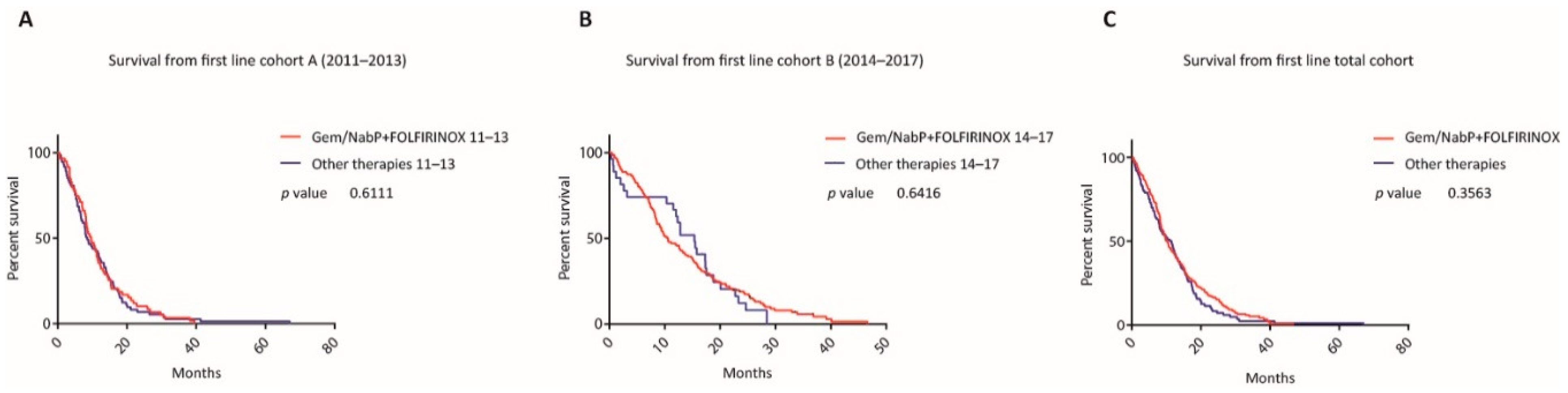
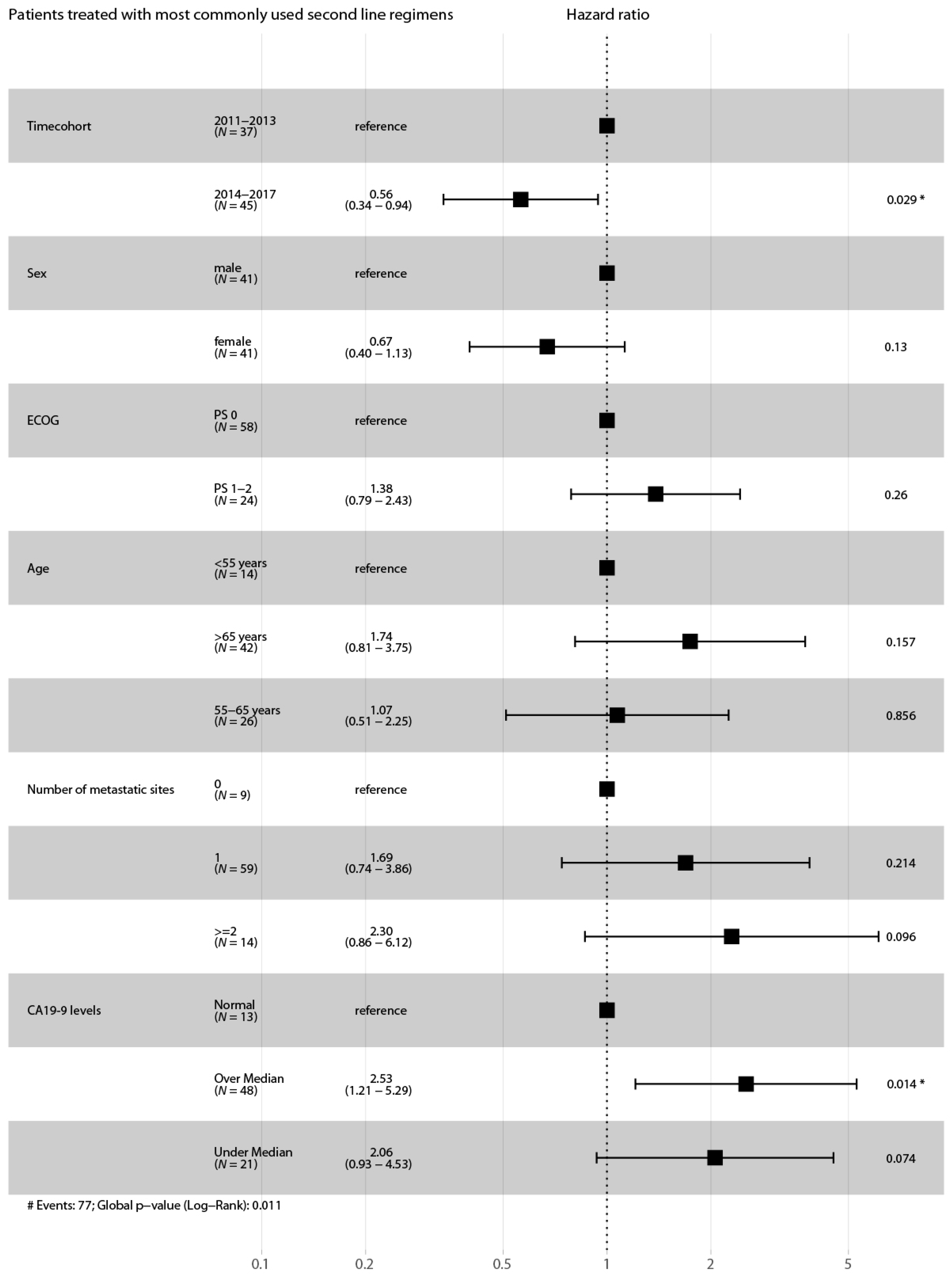
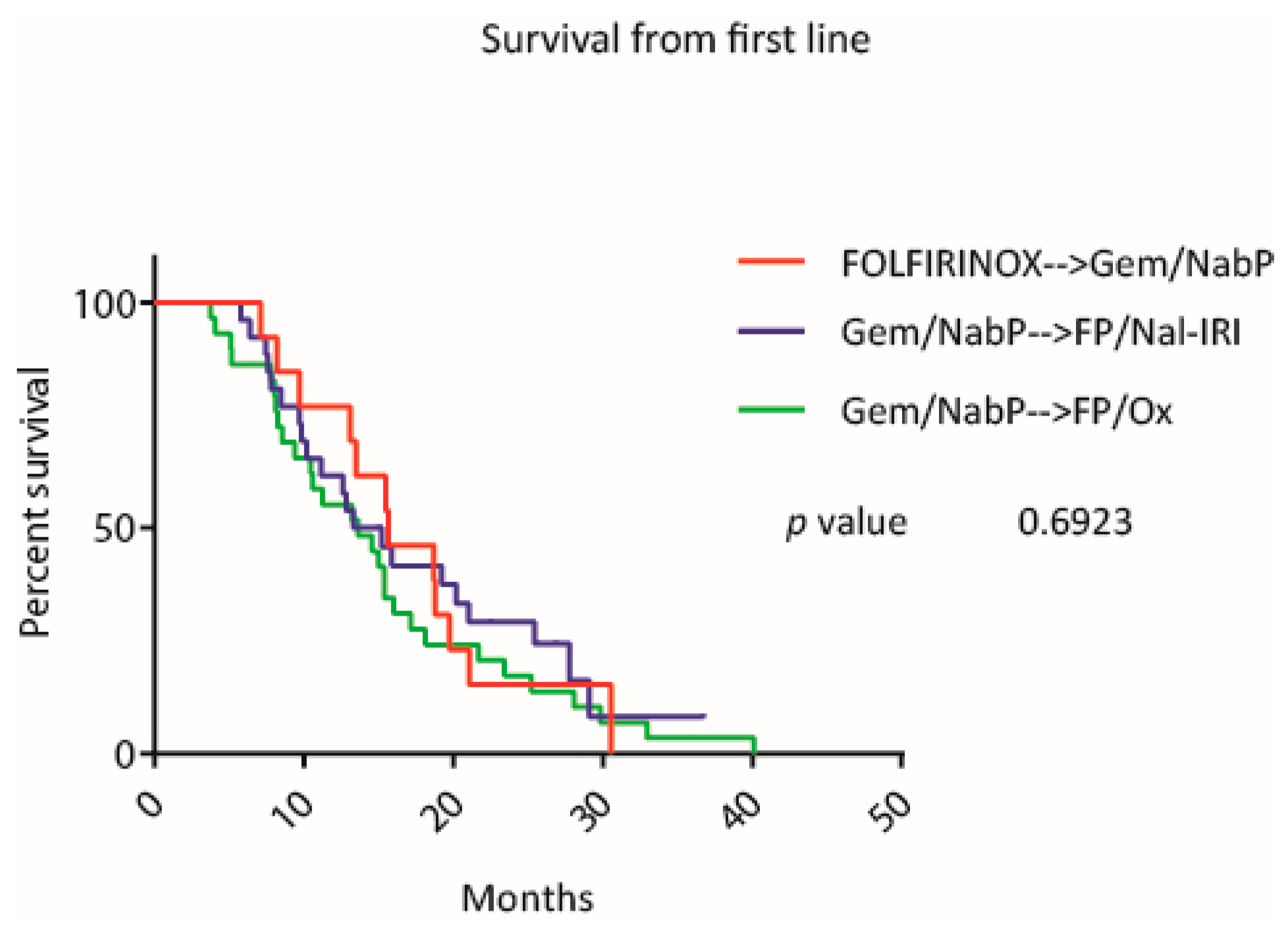
3.3. Clinical Outcome
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Rahib, L.; Smith, B.D.; Aizenberg, R.; Rosenzweig, A.B.; Fleshman, J.M.; Matrisian, L. Projecting cancer incidence and deaths to 2030: The unexpected burden of thyroid, liver, and pancreas cancers in the United States. Cancer Res. 2014, 74, 2913–2921. [Google Scholar] [CrossRef] [Green Version]
- Malvezzi, M.; Bertuccio, P.; Rosso, T.; Rota, M.; Levi, F.; La Vecchia, C.; Negri, E. European cancer mortality predictions for the year 2015: Does lung cancer have the highest death rate in EU women? Ann. Oncol. 2015, 26, 779–786. [Google Scholar] [CrossRef]
- Singhi, A.D.; Koay, E.J.; Chari, S.T.; Maitra, A. Early Detection of Pancreatic Cancer: Opportunities and Challenges. Gastroenterology 2019, 156, 2024–2040. [Google Scholar] [CrossRef] [Green Version]
- Kleeff, J.; Korc, M.; Apte, M.; La Vecchia, C.; Johnson, C.D.; Biankin, A.V.; Neale, R.E.; Tempero, M.; Tuveson, D.A.; Hruban, R.H.; et al. Pancreatic cancer. Nat. Rev. Dis. Primers 2016, 2, 16022. [Google Scholar] [CrossRef]
- Balachandran, V.P.; Beatty, G.L.; Dougan, S.K. Broadening the Impact of Immunotherapy to Pancreatic Cancer: Challenges and Opportunities. Gastroenterology 2019, 156, 2056–2072. [Google Scholar] [CrossRef]
- Neesse, A.; Bauer, C.A.; Öhlund, D.; Lauth, M.; Buchholz, M.; Michl, P.; Tuveson, D.A.; Gress, T. Stromal biology and therapy in pancreatic cancer: Ready for clinical translation? Gut 2019, 68, 159–171. [Google Scholar] [CrossRef]
- Burris, A.H.; Moore, M.J.; Andersen, J.; Green, M.R.; Rothenberg, M.L.; Modiano, M.R.; Cripps, M.C.; Portenoy, R.K.; Storniolo, A.M.; Tarassoff, P.; et al. Improvements in survival and clinical benefit with gemcitabine as first-line therapy for patients with advanced pancreas cancer: A randomized trial. J. Clin. Oncol. 1997, 15, 2403–2413. [Google Scholar] [CrossRef] [Green Version]
- Heinemann, V.; Böck, S.; Hinke, A.; Labianca, R.; Louvet, C. Meta-analysis of randomized trials: Evaluation of benefit from gemcitabine-based combination chemotherapy applied in advanced pancreatic cancer. BMC Cancer 2008, 8, 82. [Google Scholar] [CrossRef] [Green Version]
- Sultana, A.; Smith, C.T.; Cunningham, D.; Starling, N.; Neoptolemos, J.P.; Ghaneh, P. Meta-analyses of chemotherapy for locally advanced and metastatic pancreatic cancer. J. Clin. Oncol. 2007, 25, 2607–2615. [Google Scholar] [CrossRef]
- Moore, M.J.; Goldstein, D.; Hamm, J.; Figer, A.; Hecht, J.R.; Gallinger, S.; Au, H.J.; Murawa, P.; Walde, D.; Wolff, R.A.; et al. Erlotinib Plus Gemcitabine Compared With Gemcitabine Alone in Patients With Advanced Pancreatic Cancer: A Phase III Trial of the National Cancer Institute of Canada Clinical Trials Group. J. Clin. Oncol. 2007, 25, 1960–1966. [Google Scholar] [CrossRef]
- Conroy, T.; Desseigne, F.; Ychou, M.; Bouche, O.; Guimbaud, R.; Bécouarn, Y.; Adenis, A.; Raoul, J.-L.; Gourgou-Bourgade, S.; De La Fouchardiere, C.; et al. FOLFIRINOX versus gemcitabine for metastatic pancreatic cancer. N. Engl. J. Med. 2011, 364, 1817–1825. [Google Scholar] [CrossRef] [Green Version]
- Von Hoff, D.D.; Ervin, T.; Arena, F.P.; Chiorean, E.G.; Infante, J.; Moore, M.; Seay, T.; Tjulandin, S.A.; Ma, W.W.; Saleh, M.N.; et al. Increased survival in pancreatic cancer with nab-paclitaxel plus gemcitabine. N. Engl. J. Med. 2013, 369, 1691–1703. [Google Scholar] [CrossRef] [Green Version]
- Wang-Gillam, A.; Li, C.-P.; Bodoky, G.; Dean, A.; Shan, Y.-S.; Jameson, G.; Macarulla, T.; Lee, K.-H.; Cunningham, D.; Blanc, J.F.; et al. Nanoliposomal irinotecan with fluorouracil and folinic acid in metastatic pancreatic cancer after previous gemcitabine-based therapy (NAPOLI-1): A global, randomised, open-label, phase 3 trial. Lancet 2016, 387, 545–557. [Google Scholar] [CrossRef]
- Oettle, H.; Riess, H.; Stieler, J.M.; Heil, G.; Schwaner, I.; Seraphin, J.; Görner, M.; Mölle, M.; Greten, T.F.; Lakner, V.; et al. Second-line oxaliplatin, folinic acid, and fluorouracil versus folinic acid and fluorouracil alone for gemcitabine-refractory pancreatic cancer: Outcomes from the CONKO-003 trial. J. Clin. Oncol. 2014, 32, 2423–2429. [Google Scholar] [CrossRef]
- Gill, S.; Ko, Y.-J.; Cripps, C.; Beaudoin, A.; Dhesy-Thind, S.; Zulfiqar, M.; Zalewski, P.; Do, T.; Cano, P.; Lam, W.Y.H.; et al. PANCREOX: A Randomized Phase III Study of Fluorouracil/Leucovorin With or Without Oxaliplatin for Second-Line Advanced Pancreatic Cancer in Patients Who Have Received Gemcitabine-Based Chemotherapy. J. Clin. Oncol. 2016, 34, 3914–3920. [Google Scholar] [CrossRef]
- Abrams, T.A.; Meyer, G.; Meyerhardt, J.A.; Wolpin, B.M.; Schrag, D.; Fuchs, C.S. Patterns of Chemotherapy Use in a U.S.-Based Cohort of Patients With Metastatic Pancreatic Cancer. Oncologist 2017, 22, 925–933. [Google Scholar] [CrossRef] [Green Version]
- Nagai, K.; Terashima, T.; Yamashita, T.; Kido, H.; Hayashi, K.; Sunagozaka, H.; Nakai, R.; Mizuno, H.; Hayakawa, H.; Nomura, Y.; et al. Dynamical Changes of Treatment Patterns and Outcomes of Unresectable Pancreatic Cancer Patients in Real-Life Practice. J. Clin. Oncol. 2019, 37, 407. [Google Scholar] [CrossRef]
- Cheung, W.Y.; Zhang, H.; Tang, P.A.; Spratlin, J.; Lee-Ying, R.M.; Goodwin, R.A.; Meyers, B.M.; Armstrong, D.; Ramjeesingh, R.; Vickers, M.M.; et al. A real world multicenter study of first (1L) and second (2L) line treatment patterns and outcomes in advanced pancreatic cancer (APC). J. Clin. Oncol. 2018, 36, 476. [Google Scholar] [CrossRef]
- Terashima, T.; Yamashita, T.; Sakai, A.; Ohta, H.; Hinoue, Y.; Toya, D.; Kawai, H.; Yonejima, M.; Urabe, T.; Noda, Y.; et al. Treatment Patterns and Outcomes of Unresectable Pancreatic Cancer Patients in Real-Life Practice: A Region-Wide Analysis. Jpn. J. Clin. Oncol. 2018, 48, 966–973. [Google Scholar] [CrossRef]
- Chou, W.-C.; Chen, Y.-Y.; Hung, C.-Y.; Chen, J.-S.; Lu, C.-H.; Chang, P.-H. Evolution of the Chemotherapeutic Landscape and Survival Outcome in Patients With Metastatic Pancreatic Cancer: A Four-Institute Cohort Study in Taiwan, 2010-2016. Cancer Manag. Res. 2019, 11, 2119–2127. [Google Scholar] [CrossRef] [Green Version]
- Kordes, M.; Yu, J.; Malgerud, O.; Liljefors, M.G.; Löhr, J.M. Survival Benefits of Chemotherapy for Patients With Advanced Pancreatic Cancer in A Clinical Real-World Cohort. Cancers 2019, 11, 1326. [Google Scholar] [CrossRef] [Green Version]
- Caparello, C.; Vivaldi, C.; Fornaro, L.; Musettini, G.; Pasquini, G.; Catanese, S.; Masi, G.; Lencioni, M.; Falcone, A.; Vasile, E. Second-Line Therapy for Advanced Pancreatic Cancer: Evaluation of Prognostic Factors and Review of Current Literature. Futur. Oncol. 2016, 12, 901–908. [Google Scholar] [CrossRef]
- Zhang, H.; Kellett, C.; Lambert, P.; Kim, C.A. Efficacy and Tolerability of Second-Line Nab-Paclitaxel and Gemcitabine After Failure of First-Line FOLFIRINOX for Advanced Pancreas Cancer: A Single-Institution Experience. Clin. Color. Cancer 2018, 17, e451–e456. [Google Scholar] [CrossRef]
- Zhang, Y.; Hochster, H.S.; Stein, S.; Lacy, J. Gemcitabine Plus Nab-Paclitaxel for Advanced Pancreatic Cancer After First-Line FOLFIRINOX: Single Institution Retrospective Review of Efficacy and Toxicity. Exp. Hematol. Oncol. 2015, 4, 29. [Google Scholar] [CrossRef] [Green Version]
- Shin, S.; Park, C.M.; Kwon, H.; Lee, K.-H. Erlotinib Plus Gemcitabine Versus Gemcitabine for Pancreatic Cancer: Real-World Analysis of Korean National Database. BMC Cancer 2016, 16, 443. [Google Scholar] [CrossRef] [Green Version]
- Smyth, E.N.; Bapat, B.; Ball, D.E.; André, T.; Kaye, J.A. Metastatic Pancreatic Adenocarcinoma Treatment Patterns, Health Care Resource Use, and Outcomes in France and the United Kingdom Between 2009 and 2012: A Retrospective Study. Clin. Ther. 2015, 37, 1301–1316. [Google Scholar] [CrossRef] [Green Version]
- Seal, B.; Xia, F.; Rietschel, P.; Germino, R.; Asche, C.; D’Souza, A.; Morland, K.; Eaddy, M. Treatment Patterns And Cost Of Care For Patients With Pancreatic Cancer. Value Heal. 2014, 17, A132. [Google Scholar] [CrossRef] [Green Version]
- Vogl, U.; Andalibi, H.; Klaus, A.; Vormittag, L.; Schima, W.; Heinrich, B.; Kafka, A.; Winkler, T.; Öhler, L. Nab-Paclitaxel and Gemcitabine or FOLFIRINOX As First-Line Treatment in Patients With Unresectable Adenocarcinoma of the Pancreas: Does Sequence Matter? BMC Cancer 2019, 19, 28. [Google Scholar] [CrossRef] [Green Version]
- Glassman, D.C.; Palmaira, R.L.; Covington, C.M.; Desai, A.M.; Ku, G.Y.; Li, J.; Harding, J.J.; Varghese, A.M.; O’Reilly, E.; Yu, K.H. Nanoliposomal Irinotecan With Fluorouracil for the Treatment of Advanced Pancreatic Cancer, a Single Institution Experience. BMC Cancer 2018, 18, 693. [Google Scholar] [CrossRef] [Green Version]
- Hu, Z.I.; Shia, J.; Stadler, Z.K.; Varghese, A.M.; Capanu, M.; Salo-Mullen, E.; Lowery, M.A.; Diaz, L.A.; Mandelker, D.; Yu, K.H.; et al. Evaluating Mismatch Repair Deficiency in Pancreatic Adenocarcinoma: Challenges and Recommendations. Clin. Cancer Res. 2018, 24, 1326–1336. [Google Scholar] [CrossRef] [Green Version]
- Golan, T.; Hammel, P.; Reni, M.; Van Cutsem, E.; Macarulla, T.; Hall, M.J.; Park, J.-O.; Hochhauser, D.; Arnold, D.; Oh, D.Y.; et al. Maintenance Olaparib for Germline BRCA-Mutated Metastatic Pancreatic Cancer. N. Engl. J. Med. 2019, 381, 317–327. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Cohort A 2011–2013 (n = 132) | Cohort B 2014–2017 (n = 169) | p-Value | |
|---|---|---|---|
| Median age at diagnosis of advanced disease (median, range) | 66.3 (57.3–72.2) | 66.0 (58.3–73.3) | ns |
| Gender (%) | |||
| Female | 53 (41) | 90 (53) | * |
| Male | 79 (59) | 79 (47) | |
| Disease stage (%) | |||
| Locally advanced (unresectable) | 34 (26) | 43 (25) | ns |
| Metastatic | 98 (74) | 126 (75) | |
| Prior surgical resection (%) | 23 (17) | 32 (19) | ns |
| Median CA 19-9 levels in kU/l (range) | 505.35 (68.05–2261.25) | 686.40 (88.25–3771.00) | ns |
| CA 19-9 levels (%) | |||
| Within normal range | 20 (15) | 19 (11) | ns |
| Above normal range | 101 (77) | 132 (78) | |
| n/a | 11 (8) | 18 (11) | ns |
| Site of metastatic disease (%) | |||
| Liver | 73 (55) | 84 (50) | ns |
| Lung | 15 (11) | 21 (12) | ns |
| Peritoneum | 10 (8) | 30 (18) | * |
| Other | 11 (8) | 7 (4) | ns |
| Number of metastatic sites (%) | |||
| 0 | 34 (26) | 43 (25) | ns |
| 1 | 80 (60) | 102 (60) | ns |
| 2 | 14 (11) | 18 (11) | ns |
| ≥3 | 4 (3) | 6 (4) | ns |
| ECOG Performance Status (%) | |||
| 0 | 67 (51) | 100 (59) | ns |
| 1 | 52 (39) | 61 (36) | ns |
| 2 | 8 (6) | 5 (3) | ns |
| n/a | 5 (4) | 3 (2) | ns |
| First Line | p | Second Line | p | Third Line | p | ||||
|---|---|---|---|---|---|---|---|---|---|
| Chemotherapy | 2011–2013 | 2014–2017 | 2011–2013 | 2014–2017 | 2011–2013 | 2014–2017 | |||
| Gem/NabP | 34 (26%) | 116 (69%) | **** | 18 (21%) | 13 (13%) | ns | 10 (26%) | 10 (17%) | ns |
| mFOLFIRINOX | 25 (19%) | 26 (15%) | ns | 4 (5%) | 5 (5%) | ns | 2 (5%) | 4 (7%) | ns |
| Gem/Ox | 16 (12%) | 5 (3%) | ** | 5 (6%) | 2 (2%) | ns | 0 (0%) | 4 (7%) | ns |
| Gem/Ox/Erlotinib | 16 (12%) | 0 (0%) | **** | 3 (3%) | 5 (5%) | ns | 1 (3%) | 0 (0%) | ns |
| Gem alone | 18 (14%) | 14 (8%) | ns | 6 (7%) | 2 (2%) | ns | 2 (5%) | 3 (5%) | ns |
| Gem/Erlotinib | 4 (3%) | 0 (0%) | * | 9 (10%) | 1 (1%) | ** | 2 (5%) | 2 (3%) | ns |
| FP/Ox | 1 (1%) | 2 (1%) | ns | 12 (14%) | 19 (18%) | ns | 5 (13%) | 16 (28%) | ns |
| FP/Iri | 1 (1%) | 0 (0%) | ns | 1 (1%) | 2 (2%) | ns | 8 (21%) | 6 (10%) | ns |
| FP/Nal-IRI | 0 (0%) | 1 (1%) | ns | 0 (0%) | 31 (30%) | **** | 0 (0%) | 14 (24%) | **** |
| Cap | 0 (0%) | 1 (1%) | ns | 4 (5%) | 5 (5%) | ns | 1 (3%) | 2 (3%) | ns |
| Gem/Cap | 0 (0%) | 1 (1%) | ns | 2 (2%) | 0 (0%) | ns | 0 (0%) | 2 (3%) | ns |
| Ox | 1 (1%) | 0 (0%) | ns | 0 (0%) | 0 (0%) | ns | 1 (3%) | 0 (0%) | ns |
| CRTx | 15 (11%) | 3 (2%) | *** | 16 (19%) | 19 (19%) | ns | 2 (5%) | 0 (0%) | ns |
| MMC | 0 (0%) | 0 (0%) | ns | 1 (1%) | 0 (0%) | ns | 1 (3%) | 0 (0%) | ns |
| Local therapy | 1 (1%) | 0 (0%) | ns | 2 (2%) | 0 (0%) | ns | 2 (5%) | 0 (0%) | ns |
| Gem/Cap/Erlotinib | 0 (0%) | 0 (0%) | ns | 3 (3%) | 0 (0%) | ns | 1 (3%) | 0 (0%) | ns |
| No therapy | 0 (0%) | 0 (0%) | ns | 46 (35%) | 65 (38%) | ns | 94 (71%) | 106 (63%) | ns |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kieler, M.; Unseld, M.; Bianconi, D.; Schindl, M.; Kornek, G.V.; Scheithauer, W.; Prager, G.W. Impact of New Chemotherapy Regimens on the Treatment Landscape and Survival of Locally Advanced and Metastatic Pancreatic Cancer Patients. J. Clin. Med. 2020, 9, 648. https://doi.org/10.3390/jcm9030648
Kieler M, Unseld M, Bianconi D, Schindl M, Kornek GV, Scheithauer W, Prager GW. Impact of New Chemotherapy Regimens on the Treatment Landscape and Survival of Locally Advanced and Metastatic Pancreatic Cancer Patients. Journal of Clinical Medicine. 2020; 9(3):648. https://doi.org/10.3390/jcm9030648
Chicago/Turabian StyleKieler, Markus, Matthias Unseld, Daniela Bianconi, Martin Schindl, Gabriela V. Kornek, Werner Scheithauer, and Gerald W. Prager. 2020. "Impact of New Chemotherapy Regimens on the Treatment Landscape and Survival of Locally Advanced and Metastatic Pancreatic Cancer Patients" Journal of Clinical Medicine 9, no. 3: 648. https://doi.org/10.3390/jcm9030648