Effectiveness of Vestibular Training for Balance and Dizziness Rehabilitation in People with Multiple Sclerosis: A Systematic Review and Meta-Analysis

 ,
,  ,
,  , and
, and 
Abstract
1. Introduction
2. Methods
2.1. Data Sources and Search Strategy
2.2. Research Question and Study Selection Criteria
2.3. Data Extraction and Quality Assessment
2.4. Data Analysis
3. Results
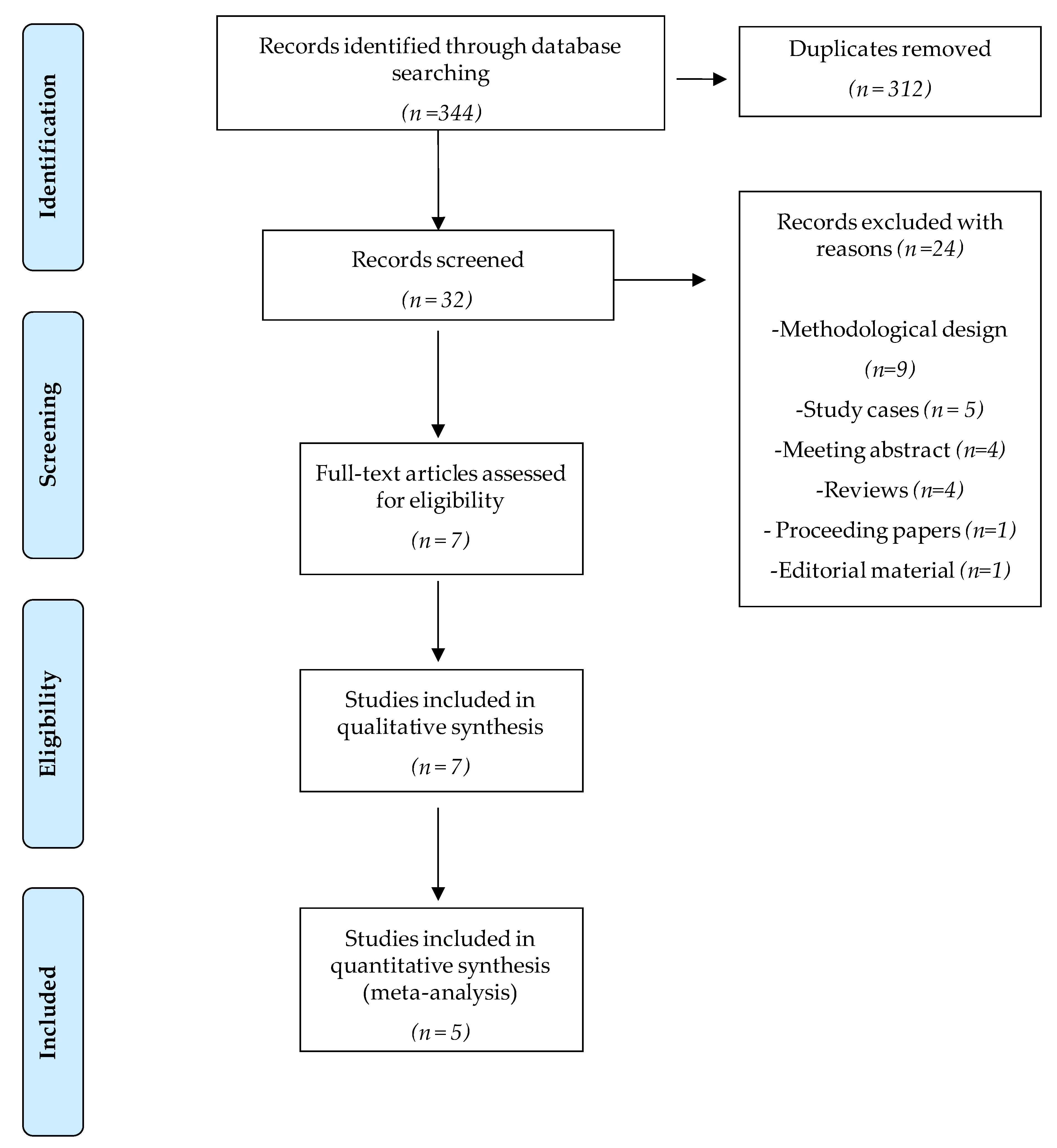
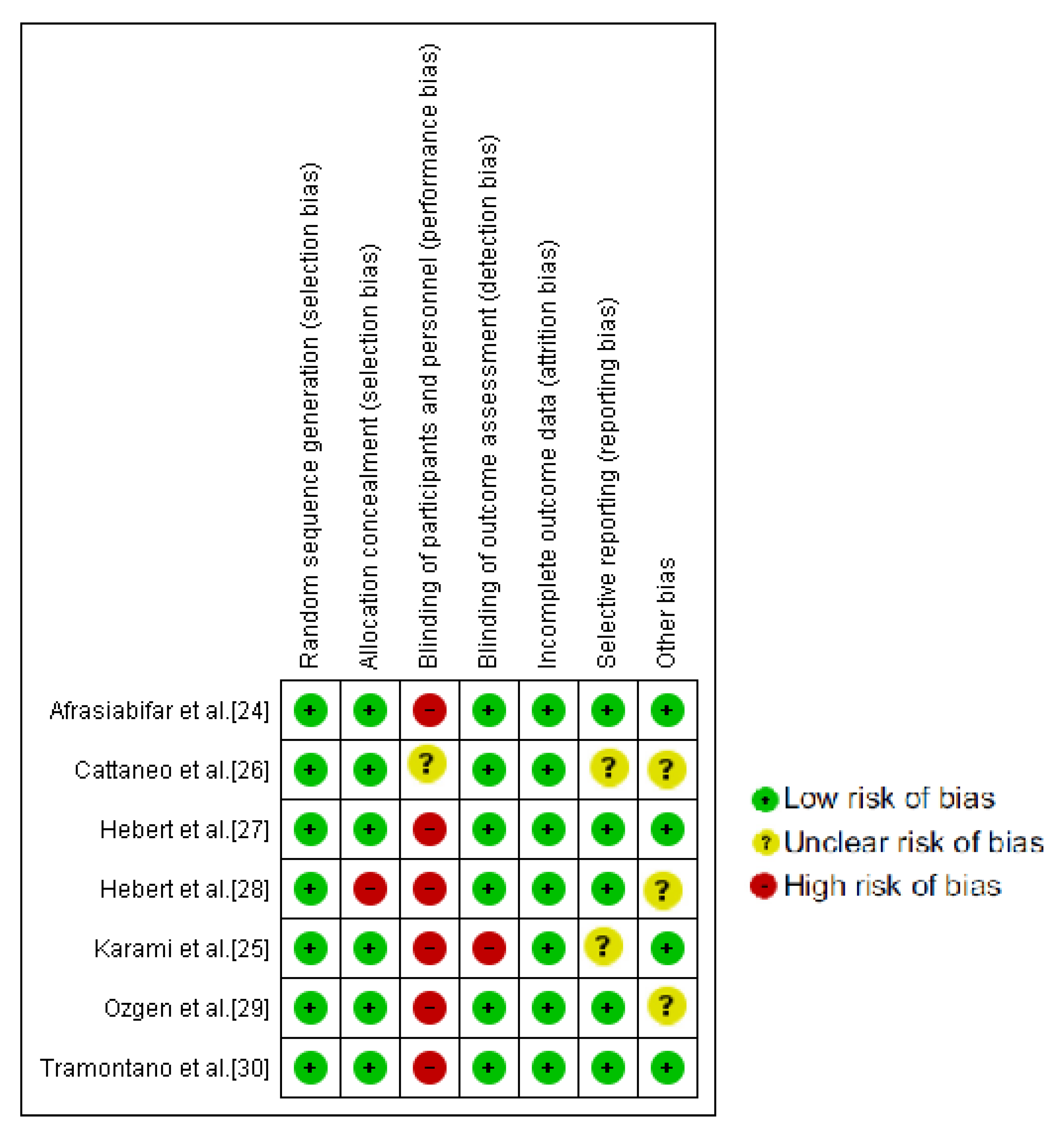
3.1. Study Selection and Methodological Quality Assessment
3.2. Study Design and Population Characteristics
3.3. Results for Primary Outcomes
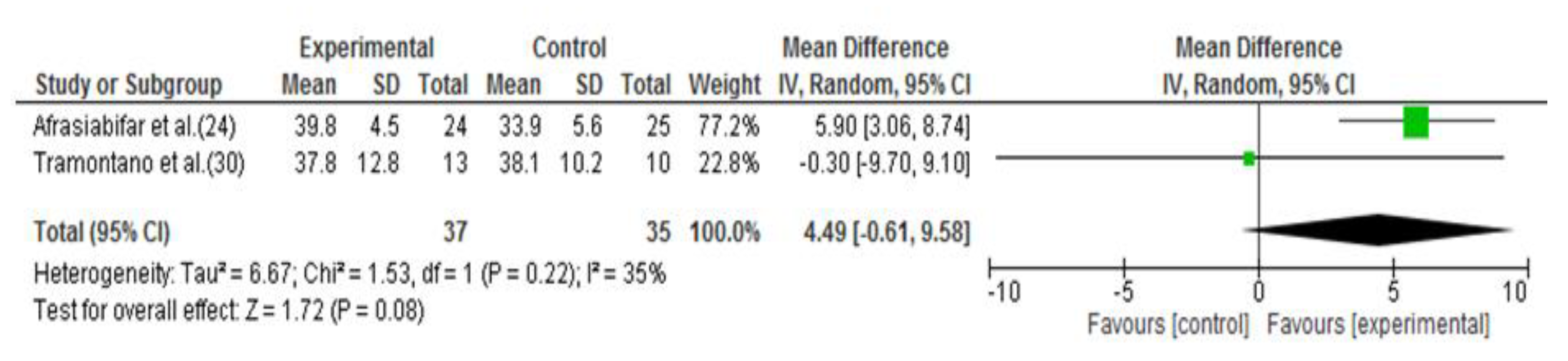
3.3.1. Balance
3.3.2. Dizziness
3.4. Results for Secondary Outcomes
3.4.1. Fatigue
3.4.2. Walking Speed
3.4.3. Depression
4. Discussion
4.1. Study Limitations
4.2. Clinical Implications
Author Contributions
Funding
Conflicts of Interest
Appendix A. Detailed Search Strategy
| Nº term used |
| #1 “Vestibular rehabilitation” #2 “Vestibular training” #3 “Vestibular cues” #4 “Vestibular therapy” #5 “Multiple sclerosis” #6 “Fatigue” #7 “Posture” #8 “Balance” #9 “Postural control” #10 “Imbalance” #11 “Dizziness” #12 “Vertigo” #13 “Walking” #14 “Gait” |
- #1 OR #2 OR #3 OR #4 AND #7 OR #8 OR #9 OR #10 OR #11 OR #12 AND #6 OR #13 OR #14 AND #5 (6 potential articles)
- #1 OR #2 OR #3 OR #4 AND #7 OR #8 OR #9 OR #10 OR #11 OR #12 AND #5 (26 potential articles)
- #1 OR #2 OR #3 OR #4 AND #6 OR #13 OR #14 AND #5 (16 potential articles)
- #1 OR #2 OR #3 OR #4 AND #6 AND #5 (11 potential articles)
- #1 OR #2 OR #3 OR #4 AND #13 OR #14 AND #5 (11 potential articles)
- #1 OR #2 OR #3 OR #4 AND #11 OR #12 AND #5 (17 potential articles)
- #1 OR #2 OR #3 OR #4 AND #5 (28 potential articles)
- #1 OR #2 OR #3 OR #4 AND #7 OR #8 OR #9 OR #10 OR #11 OR #12 AND #6 OR #13 OR #14 AND #5 (10 potential articles)
- #1 OR #2 OR #3 OR #4 AND #7 OR #8 OR #9 OR #10 OR #11 OR #12 AND #5 (19 potential articles)
- #1 OR #2 OR #3 OR #4 AND #6 OR #13 OR #14 AND #5 (10 potential articles)
- #1 OR #2 OR #3 OR #4 AND #6 AND #5 (4 potential articles)
- #1 OR #2 OR #3 OR #4 AND #13 OR #14 AND #5 (9 potential articles)
- #1 OR #2 OR #3 OR #4 AND #11 OR #12 AND #5 (12 potential articles)
- #1 OR #2 OR #3 OR #4 AND #5 (19 potential articles)
- #1 OR #2 OR #3 OR #4 AND #7 OR #8 OR #9 OR #10 OR #11 OR #12 AND #6 OR #13 OR #14 AND #5 (10 potential articles)
- #1 OR #2 OR #3 OR #4 AND #7 OR #8 OR #9 OR #10 OR #11 OR #12 AND #5 (14 potential articles)
- #1 OR #2 OR #3 OR #4 AND #6 OR #13 OR #14 AND #5 (11 potential articles)
- #1 OR #2 OR #3 OR #4 AND #6 AND #5 (8 potential articles)
- #1 OR #2 OR #3 OR #4 AND #13 OR #14 AND #5 (9 potential articles)
- #1 OR #2 OR #3 OR #4 AND #11 OR #12 AND #5 (5 potential articles)
- #1 OR #2 OR #3 OR #4 AND #5 (16 potential articles)
- #1 AND #5 (4 potential articles)
- #1 AND #8 AND #5 (3 potential articles)
- #1 AND #6 AND #5 (2 potential articles)
- #1 AND #11 AND #5 (2 potential articles)
- #1 AND #14 AND #5 (1 potential article)
- #1 AND #5 (2 potential articles)
- #1 AND #8 AND #5 (1 potential article)
- #1 AND #11 AND #5 (2 potential articles)
- #1 AND #14 AND #5 (1 potential article)
- #1 OR #2 OR #3 OR #4 AND #7 OR #8 OR #9 OR #10 OR #11 OR #12 AND #6 OR #13 OR #14 AND #5 (5 potential articles)
- #1 OR #2 OR #3 OR #4 AND #7 OR #8 OR #9 OR #10 OR #11 OR #12 AND #5 (19 potential articles)
- #1 OR #2 OR #3 OR #4 AND #6 OR #13 OR #14 AND #5 (5 potential articles)
- #1 OR #2 OR #3 OR #4 AND #6 AND #5 (5 potential articles)
- #1 OR #2 OR #3 OR #4 AND #13 OR #14 AND #5 (3 potential articles)
- #1 OR #2 OR #3 OR #4 AND #11 OR #12 AND #5 (7 potential articles)
- #1 OR #2 OR #3 OR #4 AND #5 (9 potential articles)
References
- Gossman, W.; Ehsan, M.; Xixis, K. Multiple Sclerosis; StatPearls Publishing: Treasure Island, FL, USA, 2019; pp. 1–10. [Google Scholar]
- Marrie, R.A.; Cutter, G.R.; Tyry, T. Substantial burden of dizziness in multiple sclerosis. Mult. Scler. Relat. Disord. 2013, 2, 21–28. [Google Scholar] [CrossRef] [PubMed]
- Cattaneo, D.; Jonsdottir, J. Sensory impairments in quiet standing in subjects with multiple sclerosis. Mult. Scler. 2009, 15, 59–67. [Google Scholar] [CrossRef] [PubMed]
- Alpini, D.; Berardino, F.D.; Mattei, V.; Caputo, D.; Schalek, P.; Cesarani, A. Characteristics of multiple sclerosis patient stance control disorders, measured by means of posturography and related to brainstem lesions. Audiol. Res. 2012, 2, 43–47. [Google Scholar] [CrossRef][Green Version]
- Doty, R.L.; MacGillivray, M.R.; Talab, H.; Tourbier, I.; Reish, M.; Davis, S.; Cuzzocreo, J.L.; Shepard, N.T.; Pham, D.L. Balance in multiple sclerosis: Relationship to central brain regions. Exp. Brain Res. 2018, 236, 2739–2750. [Google Scholar] [CrossRef]
- Fling, B.W.; Dutta, G.G.; Schlueter, H.; Cameron, M.H.; Horak, F.B. Associations between Proprioceptive Neural Pathway Structural Connectivity and Balance in People with Multiple Sclerosis. Front. Hum. Neurosci. 2014, 8, 814. [Google Scholar] [CrossRef]
- Van Emmerik, R.E.A.; Remelius, J.G.; Johnson, M.B.; Chung, L.H.; Kent-Braun, J.A. Postural control in women with multiple sclerosis: Effects of task, vision and symptomatic fatigue. Gait Posture 2010, 32, 608–614. [Google Scholar] [CrossRef]
- Hebert, J.R.; Corboy, J.R. The association between multiple sclerosis-related fatigue and balance as a function of central sensory integration. Gait Posture 2013, 38, 37–42. [Google Scholar] [CrossRef]
- Manjaly, Z.M.; Harrison, N.A.; Critchley, H.D.; Do, C.T.; Stefanics, G.; Wenderoth, N.; Lutterotti, A.; Müller, A.; Stephan, K.E. Pathophysiological and cognitive mechanisms of fatigue in multiple sclerosis. J. Neurol. Neurosurg. Psychiatry 2019, 90, 642–651. [Google Scholar] [CrossRef]
- Kutz, J.W. The dizzy patient. Med. Clin. N. Am. 2010, 94, 989–1002. [Google Scholar] [CrossRef]
- Zeigelboim, B.S.; Arruda, W.O.; Mangabeira-Albernaz, P.L.; Iorio, M.C.; Jurkiewicz, A.L.; Martins-Bassetto, J.; Klagenberg, K.F. Vestibular findings in relapsing, remitting multiple sclerosis: A study of thirty patients. Int. Tinnitus J. 2008, 14, 139–145. [Google Scholar]
- Frohman, E.; Kramer, P.; Dewey, R.; Kramer, L.; Frohman, T. Benign paroxysmal positioning vertigo in multiple sclerosis: Diagnosis, pathophysiology and therapeutic techniques. Mult. Scler. 2003, 9, 250–255. [Google Scholar] [CrossRef] [PubMed]
- Tjernström, F.; Zur, O.; Jahn, K. Current concepts and future approaches to vestibular rehabilitation. J. Neurol. 2016, 263, 65–70. [Google Scholar] [CrossRef] [PubMed]
- Whitney, S.L.; Alghwiri, A.; Alghadir, A. Chapter 13. An overview of vestibular rehabilitation. In Handbook of Clinical Neurology, 1st ed.; Elsevier: Amsterdan, The Netherlands, 2016; Volume 137, pp. 187–205. [Google Scholar]
- Whitney, S.L.; Sparto, P.J. Principles of vestibular physical therapy rehabilitation. NeuroRehabilitation 2011, 29, 157–166. [Google Scholar] [CrossRef] [PubMed]
- Han, B.I.; Song, H.S.; Kim, J.S. Vestibular rehabilitation therapy: Review of indications, mechanisms, and key exercises. J. Clin. Neurol. 2011, 7, 184–196. [Google Scholar] [CrossRef]
- Hain, T.C. Neurophysiology of vestibular rehabilitation. NeuroRehabilitation 2011, 29, 127–141. [Google Scholar] [CrossRef]
- Brown, K.E.; Whitney, S.L.; Marchetti, G.F.; Wrisley, D.M.; Furman, J.M. Physical therapy for central vestibular dysfunction. Arch. Phys. Med. Rehabil. 2006, 87, 76–81. [Google Scholar] [CrossRef]
- National Clinical Guideline Centre. Multiple Sclerosis. Management of Multiple Sclerosis in Primary and Secondary Care; Clin Guidel 186; Springer, Humana Press: London, UK, 2014; Volume 1304. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Preferred reporting itemps for systematic reviews and meta-analyses: The PRISMA Statement. Ann. Intern. Med. 2009, 151, 264–269. [Google Scholar] [CrossRef]
- Polman, C.H.; Reingold, S.C.; Banwell, B.; Clanet, M.; Cohen, J.A.; Filippi, M.; Fujihara, K.; Havrdova, E.; Hutchinson, M.; Kappos, L.; et al. Diagnostic criteria for multiple sclerosis: 2010 Revisions to the McDonald criteria. Ann. Neurol. 2011, 69, 292–302. [Google Scholar] [CrossRef]
- Maher, C.; Sherrington, C.; Hebert, R.; Moseley, A.; Elkins, M. Reliability of the PEDro scale for rating quality of randomized controlled trials. Phys. Ther. 2003, 83, 713–721. [Google Scholar] [CrossRef]
- Higgins, J.P.T.; Sterne, J.A.C.; Savović, J.; Page, M.J.; Hróbjartsson, A.; Boutron, I.; Reeves, B.; Eldridge, S. A revised tool for assessing risk of bias in randomized trials. Cochrane Database Syst. Rev. 2016, 10 (Suppl. 1), 29–31. [Google Scholar]
- Afrasiabifar, A.; Karami, F.; Doulatabad, N.S. Comparing the effect of Cawthorne–Cooksey and Frenkel exercises on balance in patients with multiple sclerosis: A randomized controlled trial. Clin. Rehabil. 2018, 32, 57–65. [Google Scholar] [CrossRef] [PubMed]
- Karami, F.; Afrasiabifar, A.; Doulatabad, N.S. Comparing the Effectiveness of Vestibular Rehabilitation and Frenkel Exercise on Fatigue Reduction in Patients with Multiple Sclerosis: A Randomized Controlled Trial. Iran. Red Crescent Med. J. 2018, 20, e68913. [Google Scholar] [CrossRef]
- Cattaneo, D.; Jonsdottir, J.; Regola, A.; Carabalona, R. Stabilometric assessment of context dependent balance recovery in persons with multiple sclerosis: A randomized controlled study. J. Neuroeng. Rehabil. 2014, 11, 1–7. [Google Scholar] [CrossRef]
- Hebert, J.R.; Corboy, J.R.; Manago, M.M.; Schenkman, M. Effects of Vestibular Rehabilitation on Multiple Sclerosis–Related Fatigue and Upright Postural Control: A Randomized Controlled Trial. Phys. Ther. 2011, 91, 1166–1183. [Google Scholar] [CrossRef] [PubMed]
- Hebert, J.R.; Corboy, J.R.; Vollmer, T.; Forster, J.E.; Schenkman, M. Efficacy of Balance and Eye-Movement Exercises for Persons With Multiple Sclerosis (BEEMS). Neurology 2018, 90, 797–807. [Google Scholar] [CrossRef] [PubMed]
- Ozgen, G.; Karapolat, H.; Akkoc, Y.; Yuceyar, N. Is customized vestibular rehabilitation effective in patients with multiple sclerosis? A randomized controlled trial. Eur. J. Phys. Rehabil. Med. 2016, 52, 466–478. [Google Scholar] [PubMed]
- Tramontano, M.; Martino Cinnera, A.; Manzari, L.; Tozzi, F.F.; Caltagirone, C.; Morone, G.; Pompa, A.; Grasso, M.G. Vestibular rehabilitation has positive effects on balance, fatigue and activities of daily living in highly disabled multiple sclerosis people: A preliminary randomized controlled trial. Restor. Neurol. Neurosci. 2018, 36, 709–718. [Google Scholar] [CrossRef]
- Palmataa, J.; Sjörgren, T.; Peurala, S.; Heinonen, A. Effects of physiotherapy interventions on balance in multiple sclerosis: A systematic review and meta-analysis of randomized controlled trials. J. Rehabil. Med. 2012, 44, 811–823. [Google Scholar]
- Campbell, E.; Coulter, E.H.; Mattison, P.G.; Miller, L.; McFadyen, A.; Paul, L. Physiotherapy rehabilitation for people with progressive multiple sclerosis: A systematic review. Arch. Phys. Med. Rehabil. 2016, 97, 141–151. [Google Scholar] [CrossRef]
- Charron, S.; McKay, K.A.; Tremlett, H. Physical activity and disability outcomes in multiple sclerosis: A systematic review (2011–2016). Mult. Scler. Relat. Disord. 2018, 20, 169–177. [Google Scholar] [CrossRef]
- e Silva, D.C.M.; Bastos, V.H.; de Oliveira Sanchez, M.; Nunes, M.K.G.; Orsini, M.; Ribeiro, P.; Velasques, B.; Teixeira, S.S. Effects of vestibular rehabilitation in the elderly: A systematic review. Aging Clin. Exp. Res. 2016, 28, 599–606. [Google Scholar] [CrossRef] [PubMed]
- Murray, D.A.; Meldrum, D.; Lennon, O. Can vestibular rehabilitation exercises help patients with concussion? A systematic review of efficacy, prescription and progression patterns. Br. J. Sports Med. 2017, 51, 442–451. [Google Scholar] [CrossRef] [PubMed]
- Hebert, J.R.; Foster, J.E.; Sterans-Yoder, K.A.; Penzenik, M.E.; Brenner, L.A. Persistent Symptoms and Objectively Measured Balance Performance Among OEF/OIF Veterans with Remote Mild Traumatic Brain Injury. J. Head Trauma Rehabil. 2018, 33, 403–411. [Google Scholar] [CrossRef] [PubMed]
- Gurley, J.M.; Hujsak, B.D.; Kelly, J.L. Vestibular rehabilitation following mild traumatic brain injury. NeuroRehabilitation 2013, 32, 519–528. [Google Scholar] [CrossRef] [PubMed]
- Amatya, B.; Young, J.; Khan, F. Non-pharmacological interventions for chronic pain in multiple sclerosis. Cochrane Database Syst. Rev. 2018, 12, CD012622. [Google Scholar] [CrossRef]
- Rietberg, M.; Veerbeek, J.; Gosselink, R.; Kwakkel, G.; Van Wegen, E. Respiratory muscle training for multiple sclerosis. Cochrane Database Syst. Rev. 2017, 12, CD009424. [Google Scholar] [CrossRef]
- Dunlap, P.M.; Holmberg, J.M.; Whitney, S.L. Vestibular rehabilitation: Advances in peripheral and central vestibular disorders. Curr. Opin. Neurol. 2019, 32, 137–144. [Google Scholar] [CrossRef]
- Zambare, P.D.; Soni, N.; Sharma, P. Effect of Cawthorne and Cooksey Exercise Program on Balance and Likelihood of Fall in Older Women. Indian J. Physiother. Occup. Ther. An. Int. J. 2015, 9, 55. [Google Scholar] [CrossRef]
- Gaikwad, S.B.; Mukherjee, T.; Shah, P.V.; Ambode, O.I.; Johnson, E.G.; Daher, N.S. Home exercise program adherence strategies in vestibular rehabilitation: A systematic review. Phys. Ther. Rehabil. Sci. 2016, 5, 53–62. [Google Scholar] [CrossRef]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Section/Theme | Afrasiabifar et al. [24] | Karami et al. [25] | Cattaneo et al. [26] | Hebert et al. [27] | Hebert et al. [28] | Ozgen et al. [29] | Tramontano et al. [30] |
|---|---|---|---|---|---|---|---|
| Eligibility criteria | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
| Random allocation | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
| Concealled allocation | Yes | Yes | Yes | Yes | No | Yes | Yes |
| Baseline comparability | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
| Blind subjects | No | No | Yes | No | No | No | No |
| Blind therapists | No | No | No | No | No | No | No |
| Blind assessors | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
| Adequate follow-up | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
| Intention to treat analysis | Yes | Yes | No | Yes | No | No | Yes |
| Between-group comparisons | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
| Point estimates and variability | Yes | Yes | No | Yes | Yes | Yes | Yes |
| Total score | 8/10 | 8/10 | 7/10 | 8/10 | 6/10 | 7/10 | 8/10 |
| Study | Design, PEDro Score | Participants, Characteristics and Sample Size | Intervention (VR Group) | Control Group | Outcome Measures | Main Results |
|---|---|---|---|---|---|---|
| Afrasiabifar et al. [24] | RCT, 8/10 | EG mean age(SD): 32.4 (8.1) G2 mean age SD): 32 (6.7) CG mean age (SD): 33.6 (7.3) N = 72 (EG: 24, G2: 23, CG: 25), 3 drop out 64 MSRR 4 MSPP/SP Location of intervention: clinic | EG: Cawthorne–Cooksey vestibular rehabilitation exercise protocol 3 session week, 60 min 12 weeks intervention | G2: Frenkel exercises, 3 session per week, 60 min CG: no intervention | Berg Balance Scale (BBS) | EG-CG/G2: Significant differences in favour of the experimental group for BBS in comparison with CG (p = 0.001) and G2 (p = 0.001) G2-CG: Significant differences in favour of G2 for BBS (p = 0.01) |
| Karami et al. [25] | RCT, 8/10 | Fatigue: FIS | EG-CG/G2: Significant differences in favour of the experimental group in comparison with the CG (p = 0.001) and G2 (p= 0.007) G2-CG: Significant differences in favour ofthe G2 (p = 0.001) | |||
| Cattaneo et al. [26] | RCT 7/10 | EG mean age(SD): 48.5 (11.01) CG mean age (SD): 48.2 (12.05) N = 53 (EG: 25, CG: 28) 24 MSRR 3 MSPP 26 MSSP EDSS: 1–6.5 Location: clinic hospital. | EG: Balance exercises with open/closed eyes on different surfaces plus head–eyes movements (vestibular cues) 15 sessions of 45 min, 3 weeks intervention | CG: usualrehabilitation based on range motion, muscle force, postural changes and gait on firm surface 15 sessions of 45 min, 3 weeks intervention | Balance: COP disturbances in six different conditions (eyes open/closed and sway referenced on firm and foam surfaces) | EG-CG: Significant differences in favour of the experimental group for eyes closed firm surface (p = 0.033, eyes opencompliant surface (p = 0.01), eyes closed compliant surface (p = 0.039) and sway referenced compliant surface (p = 0.017) |
| Hebert et al. [27] | RCT, 8/10 | EG mean age(SD): 46.8 (10.5) G2 mean age(SD): 42.6 (10.4) CG mean age (SD): 50.2 (9.2) N = 38 (EG: 12, G2: 13, CG: 13) 34 MSRR 4MSSP Location: human performance laboratory and home exercises | EG: upright postural control and eye movement exercises, Perform of 1–2 min each item 2 session/week, 60 min + a daily independent home exercise program 6 weeks of intervention | G2: endurance of static bicycling and stretching exercise of lower limb muscles; stretches were held for 30 s Samefrequency and duration CG: no intervention | Balance: posturography (SOT) Fatigue: MFIS Dizziness: DHI Exercise capacity: 6MWT Depression: BDI-II | EG-CG/G2: Significant differences in favour of the experimental group in comparison with control group for balance (p=0.003), fatigue (p=0.005) and dizziness (p=0.009) and G2 for balance(p< 0.001) G2-CG: No statistical differences between groups for any of the variables |
| Hebert et al. [28] | RCT, 6/10 | EG Mean age(SD): 46.5 (8.8) CG Mean age(SD): 43 (10.8) N = 88 (EG: 44, CG: 44), 12 drop out EDSS: 3.34–3.5 Location: human performance laboratoryand home exercises | EG: BEEMS protocol, 2 s/w + daily home exercise (phase 1). Phase 2: 1 s/w + daily home exercises 14 weeks intervention | CG: no intervention | Balance: CDP-SOT Fatigue: MFIS Dizziness: DHI, DVAT, GST Gait: T25FW Quality of life: PDQ, SF-36 Mental and Physical component | EG-CG: Significant differences in favour of the experimental group for balance, fatigue and dizziness/DHI (p< 0.0001); quality of life/PDQ (p=0.0008), SF-36 MC (p = 0.02) and SF-36 PC (p = 0.01) A greater improvement was observedin participants with brainstem/cerebellar lesion compared with those without in CDP-SOT composite (p = 0.04) and MFIS total (p = 0.02) |
| Ozgen et al. [29] | RCT, 7/10 | EG mean age: 42.5 CG mean age: 39.5 N = 40 (EG: 20, CG: 20) 17MSRR 7MSPP 16MSSP Location: human performance laboratory | EG: vestibular rehabilitation program (balance and ambulation exercises) 15–20 min, twice a day 8 weeks of intervention | CG: no intervention | Balance: static posturography, BBS, Romberg tests + foam, FTSTS, TUG, ABC Dizziness: DHI Gait: 6WT, DGI, FGA, Depression: BDI Qualitylife: MSQoL-54 | EG-CG: Significant differences between groups for Tandem Romberg (eyes closed) and foam standing (eyes open) (p<0.05) |
| Tramontano et al. [30] | RCT, 8/10 | EG mean age (SD): 50.64 (11.73) CG Mean age: 45.77 (10.91) N = 30 (EG: 15, CG: 15) 7 dropout EDSS: 6–7 Location: clinic | EG: conventional neurorehabilitation therapy for MS + 10 min exercise for gaze stability + 10 exercise for postural stability Two daily 40 min + 20 min VR, 5days/week 4 weeks intervention | CG: two daily 40-min 5 days/w for 4 weeks of conventional neurorehabilitation therapy for MS. Muscle stretching, postural alignment, active-assisted mobilisations and neuromuscular facilitations, balance training: progressive restrictions of support base, unstable surfaces. | Balance: TBG, BBS Fatigue: FSS Gait: 2MWT, T25FW Disability: EDSS, BI | EG-CG: Significant differences in favour of the experimental group were observed except for 2MWT |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
García-Muñoz, C.; Cortés-Vega, M.-D.; Heredia-Rizo, A.M.; Martín-Valero, R.; García-Bernal, M.-I.; Casuso-Holgado, M.J. Effectiveness of Vestibular Training for Balance and Dizziness Rehabilitation in People with Multiple Sclerosis: A Systematic Review and Meta-Analysis. J. Clin. Med. 2020, 9, 590. https://doi.org/10.3390/jcm9020590
García-Muñoz C, Cortés-Vega M-D, Heredia-Rizo AM, Martín-Valero R, García-Bernal M-I, Casuso-Holgado MJ. Effectiveness of Vestibular Training for Balance and Dizziness Rehabilitation in People with Multiple Sclerosis: A Systematic Review and Meta-Analysis. Journal of Clinical Medicine. 2020; 9(2):590. https://doi.org/10.3390/jcm9020590
Chicago/Turabian StyleGarcía-Muñoz, Cristina, María-Dolores Cortés-Vega, Alberto Marcos Heredia-Rizo, Rocío Martín-Valero, María-Isabel García-Bernal, and María Jesús Casuso-Holgado. 2020. "Effectiveness of Vestibular Training for Balance and Dizziness Rehabilitation in People with Multiple Sclerosis: A Systematic Review and Meta-Analysis" Journal of Clinical Medicine 9, no. 2: 590. https://doi.org/10.3390/jcm9020590
APA StyleGarcía-Muñoz, C., Cortés-Vega, M.-D., Heredia-Rizo, A. M., Martín-Valero, R., García-Bernal, M.-I., & Casuso-Holgado, M. J. (2020). Effectiveness of Vestibular Training for Balance and Dizziness Rehabilitation in People with Multiple Sclerosis: A Systematic Review and Meta-Analysis. Journal of Clinical Medicine, 9(2), 590. https://doi.org/10.3390/jcm9020590