High Electrode Impedance Values in Pediatric Cochlear Implant Recipients May Imply Insufficient Auditory and Language Skills Development



Abstract
1. Introduction
2. Material and Methods
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Venail, F.; Mathiolon, C.; Menjot de Champfleur, S.; Piron, J.P.; Sicard, M.; Villemus, F.; Vessigaud, M.A.; Sterkers-Artieres, F.; Mondain, M.; Uziel, A. Effects of electrode array length on frequency-place mismatch and speech perception with cochlear implants. Audiol. Neurootol. 2015, 20, 102–111. [Google Scholar] [CrossRef] [PubMed]
- Zadrozniak, M.; Szymański, M.; Siwiec, H.; Broda, T. Impedance changes in cochlear implant users. Otolaryngol. Pol. 2011, 65, 214–217. [Google Scholar] [PubMed]
- Wu, W.; Jia, H.; Li, Y.; Tang, Z.; Huang, Q.; Yang, J.; Mei, L.; Haung, Z.; Wu, H. Observation on the change of electrode impedance and THR/MCL values in 20 cases with Med-EL Combi 40+ cochlear implant. Lin Chung Er Bi Yan Hou Tou Jing Wai Ke Za Zhi 2013, 27, 1238–1242. [Google Scholar] [PubMed]
- Vargas, J.L.; Sainz, M.; Roldan, C.; Alvarez, I.; de la Torre, A. Analysis of electrical thresholds and maximum comfortable levels in cochlear implant patients. Auris Nasus Larynx 2013, 40, 260–265. [Google Scholar] [CrossRef] [PubMed]
- Sainz, M.; Skarzynski, H.; Allum, J.H.; Helms, J.; Rivas, A.; Martin, J.; Zorowka, P.G.; Phillips, L.; Delauney, J.; Brockmeyer, S.J.; et al. Assessment of auditoryskills in 140 cochlear implantchil-dren using the EARS protocol. ORL J. Otorhinolaryngol. Relat. Spec. 2003, 65, 91–96. [Google Scholar] [CrossRef] [PubMed]
- Xi, X.; Han, D.; Huang, D.; Yang, W.; Hong, M. A longitudinal study of electrode impedance in nucleus 24M cochlear implant users. Lin Chuang Er Bi Yan Hou Ke Za Zhi 2003, 17, 593–595. [Google Scholar] [PubMed]
- Petrov, S.M.; Shchukina, A.A. Monitoring of implant electrode impedance. Vestn. Otorinolaringol. 2011, 2, 30–32. [Google Scholar]
- Henkin, Y.; Kaplan-Neeman, R.; Muchnik, C.; Kronenberg, J.; Hildesheimer, M. Changes over time in electrical stimulation levels and electrode impedance values in children using the Nucleus 24 M cochlear implant. Int. J. Pediatr. Otorhinolaryngol. 2003, 67, 873–880. [Google Scholar] [CrossRef]
- Molisz, A.; Zarowski, A.; Vermeiren, A.; Theunen, T.; De Coninck, L.; Siebert, J.; Offeciers, E.F. Postimplantation changes of electrophysiological parameters in patients with cochlear implants. Audiol. Neurootol. 2015, 20, 222–228. [Google Scholar] [CrossRef] [PubMed]
- Dorman, M.F.; Smith, L.M.; Dankowski, K.; McCandless, G.; Parkin, J.L. Long-term measures of electrode impedance and auditory thresholds for the Ineraid cochlear implant. J. Speech. Hear. Res. 1992, 35, 1126–1130. [Google Scholar] [CrossRef] [PubMed]
- Busby, P.A.; Plant, K.L.; Whitford, L.A. Electrode impedance in adults and children using the Nucleus 24 cochlear implant system. Cochlear Implants Int. 2002, 3, 87–103. [Google Scholar] [CrossRef] [PubMed]
- Henkin, Y.; Kaplan-Neeman, R.; Kronenberg, J.; Migirov, L.; Hildesheimer, M.; Muchnik, C. Electrical stimulation levels and electrode impedance values in children using the Med-El Combi 40+ cochlear implant: A one year follow-up. J. Basic Clin. Physiol. Pharmacol. 2005, 16, 127–137. [Google Scholar] [CrossRef] [PubMed]
- Mirsalehi, M.; Rau, T.S.; Harbach, L.; Hügl, S.; Mohebbi, S.; Lenarz, T.; Majdani, O. Insertion forces and intracochlear trauma in temporal bone specimens implanted with a straight atraumatic electrode array. Eur. Arch. Otorhinolaryngol. 2017, 274, 2131–2140. [Google Scholar] [CrossRef] [PubMed]
- Hu, H.C.; Chen, J.K.; Li, L.P.; Chen, W.K.; Huang, M.J.; Yeh, C.H.; Chen, L.C.; Tung, T.H. Evolution of impedance values in two different electrode array designs following activation of cochlear implants 1 day after surgery: A study of 58 patients. Clin. Otolaryngol. 2019, 13327. [Google Scholar] [CrossRef] [PubMed]
- Henkin, Y.; Kaplan-Neeman, R.; Kronenberg, J.; Migirov, L.; Hildesheimer, M.; Muchnik, C. A longitudinal study of electrical stimulation levels and electrode impedance in children using the Clarion cochlear implant. Acta Otolaryngol. 2006, 126, 581–586. [Google Scholar] [CrossRef] [PubMed]
- Andrade, K.C.; Leal Mde, C.; Muniz, L.F.; Menezes Pde, L.; Albuquerque, K.M.; Carnaúba, A.T. The importance of electrically evoked stapedial reflex in cochlear implant. Braz. J. Otorhinolaryngol. 2014, 80, 68–77. [Google Scholar] [PubMed]
- Jia, H.; Venail, F.; Piron, J.P.; Batrel, C.; Pelliccia, P.; Artières, F.; Uziel, A.; Mondain, M. Effect of surgical technique on electrode impedance after cochlear implantation. Ann. Otol. Rhinol. Laryngol. 2011, 120, 529–534. [Google Scholar] [CrossRef] [PubMed]
- Durisin, M.; Krause, C.; Arnoldner, C.; Kontorinis, G.; Buechner, A.; Lenarz, T.; Lesinki-Schiedat, A.; Profant, O.; Neuburger, J. Electron microscopy changes of cochlear implant electrodes with permanently high impedances. Cochlear Implants Int. 2011, 12, 228–233. [Google Scholar] [CrossRef] [PubMed]
- Neuburger, J.; Lenarz, T.; Lesinski-Schiedat, A.; Büchner, A. Spontaneous increases in imp edance following cochlear implantation: Suspected causes and management. Int. J. Audiol. 2009, 48, 233–239. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.; Sun, J.; Sun, J.; Chen, J. Variations in electrode impedance during and after cochlear implantation: Round window versus extended round window insertions. Int. J. Pediatr. Otorhinolaryngol. 2017, 102, 44–48. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
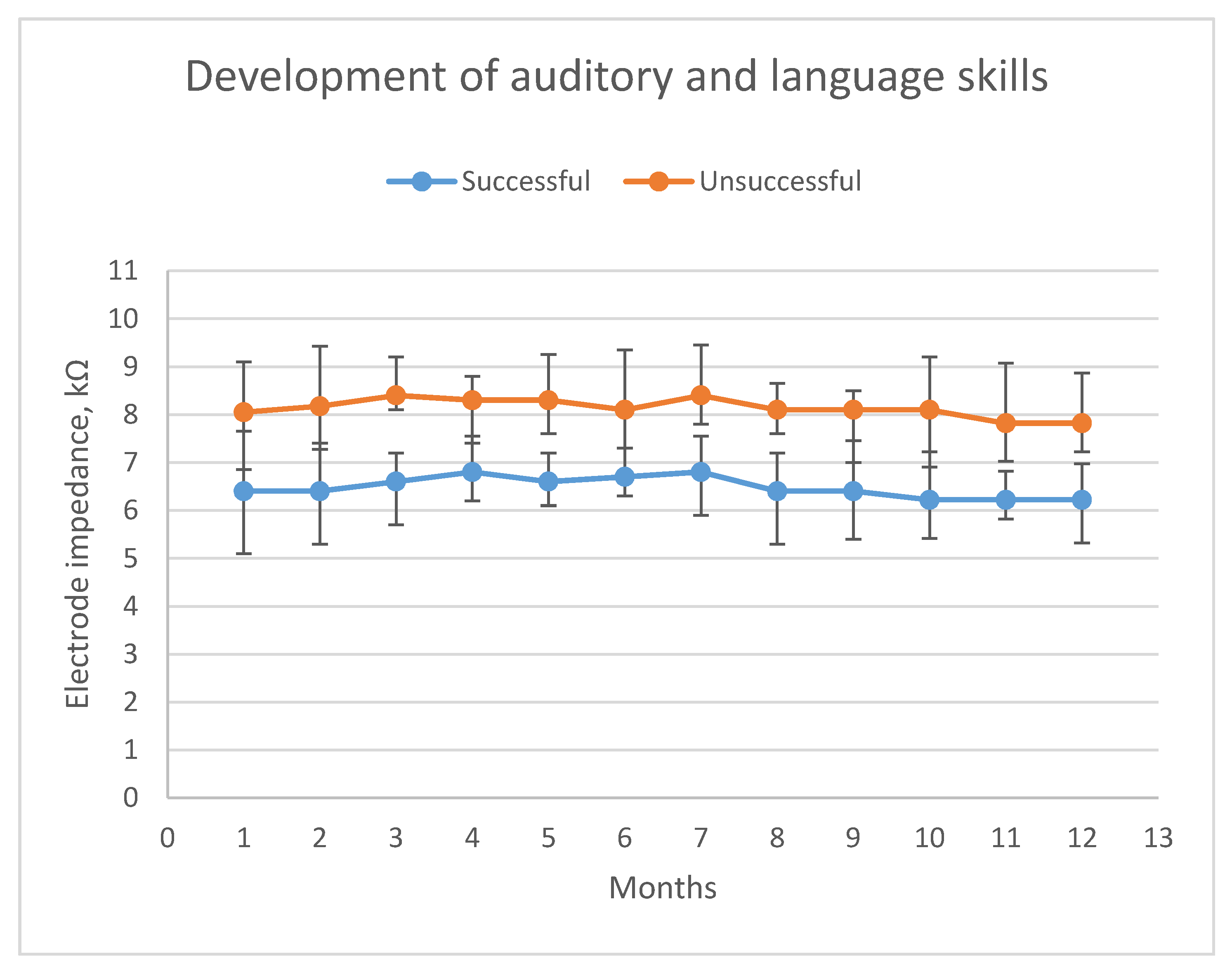
| Auditory and Language Development | Mean Age, Years | Male/Female, n | Male/Female, % | EI Values after 12 Months, kΩ | n, % |
|---|---|---|---|---|---|
| Successful | 4.1 | 15/10 | 60.0/40.0 | 6.22 ± 0.75 | 25/59.5 |
| Unsuccessful | 4.3 | 11/6 | 64.7/35.3 | 7.82 ± 1.05 | 17/40.5 |
| Total | 4.2 | 26/16 | 61.3/38.1 | 6.68 ± 0.87 | 42/100 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Brkic, F.F.; Umihanic, S.; Harcinovic, A.; Piric, L.; Brkic, F. High Electrode Impedance Values in Pediatric Cochlear Implant Recipients May Imply Insufficient Auditory and Language Skills Development. J. Clin. Med. 2020, 9, 506. https://doi.org/10.3390/jcm9020506
Brkic FF, Umihanic S, Harcinovic A, Piric L, Brkic F. High Electrode Impedance Values in Pediatric Cochlear Implant Recipients May Imply Insufficient Auditory and Language Skills Development. Journal of Clinical Medicine. 2020; 9(2):506. https://doi.org/10.3390/jcm9020506
Chicago/Turabian StyleBrkic, Faris F., Sekib Umihanic, Alen Harcinovic, Lejla Piric, and Fuad Brkic. 2020. "High Electrode Impedance Values in Pediatric Cochlear Implant Recipients May Imply Insufficient Auditory and Language Skills Development" Journal of Clinical Medicine 9, no. 2: 506. https://doi.org/10.3390/jcm9020506
APA StyleBrkic, F. F., Umihanic, S., Harcinovic, A., Piric, L., & Brkic, F. (2020). High Electrode Impedance Values in Pediatric Cochlear Implant Recipients May Imply Insufficient Auditory and Language Skills Development. Journal of Clinical Medicine, 9(2), 506. https://doi.org/10.3390/jcm9020506