Strength of the Association of Elevated Vitamin B12 and Solid Cancers: An Adjusted Case-Control Study

 ,
, 
 , and
, and
Abstract
1. Introduction
2. Materials and Methods
2.1. Ethics and Statement for Study Checklist
2.2. Study Population
2.3. Plasma Vitamin B12 Assay
2.4. Collected Data
2.5. Statistical Methods
2.5.1. Association Between Solid Cancers and High-B12 Group
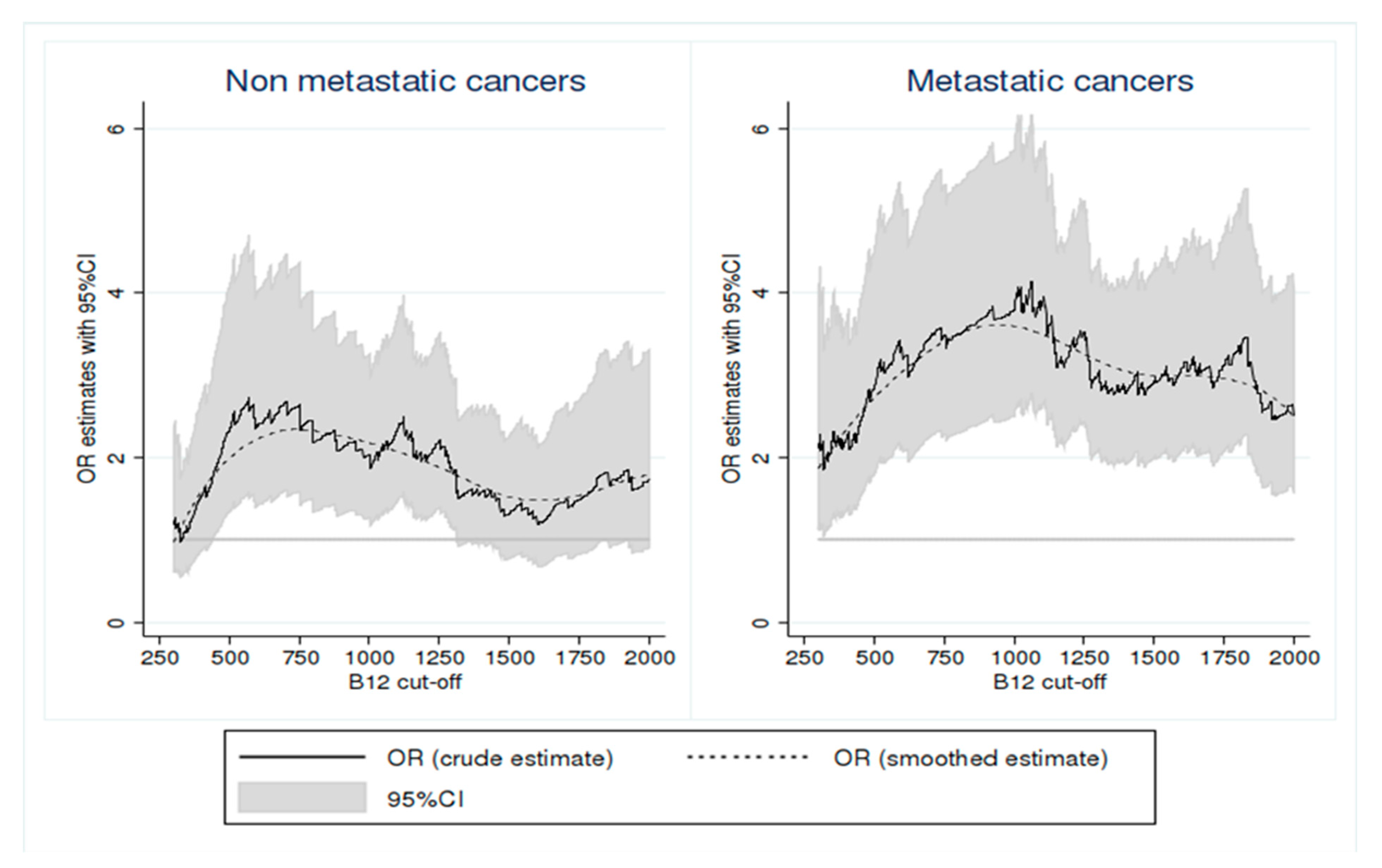
2.5.2. To Determine the Threshold of B12 Level Maximizing the Association Between an Elevated B12 and Solid Cancers According to the Presence or Absence of Metastases
2.5.3. The Association Between Elevated B12 and Solid Cancers by Interval of B12 Level According to the Metastatic Status
2.5.4. The Association Between the High-B12 Group and Solid Cancers According to the Type of Cancer and the Primary Tumor and Metastatic Site
3. Results
3.1. Population Description (Table 1)
3.2. Causes of Elevated B12 in Multivariate Analysis
3.3. Determination of the Best Thresholds of B12 Level to Evaluate the Association with Solid Cancers Based on the Presence or Absence of Metastases
3.4. Strength of the Association Between Solid Cancers and Elevated B12
3.4.1. Based on the Metastatic Status of the Cancer by Plasma B12 Level Intervals (Table 3)
3.4.2. According to the Primary Cancer and Metastatic Site (Table 4)
4. Discussion
5. Conclusions
Author Contributions
Conflicts of Interest
References
- Stabler, S.P. Vitamin B12 Deficiency. N. Engl. J. Med. 2013, 368, 149–160. [Google Scholar] [CrossRef] [PubMed]
- Andres, E.; Serraj, K.; Zhu, J.; Vermorken, A.J.M. The pathophysiology of elevated vitamin B12 in clinical practice. QJM 2013, 106, 505–515. [Google Scholar] [CrossRef] [PubMed]
- Chiche, L.; Jean, R.; Romain, F.; Roux, F.; Thomas, G.; Canavese, S.; Branger, S.; Harlé, J.-R.; Durand, J.-M. Implications cliniques de la découverte d’une hypervitaminémie B12 en médecine interne. Rev. Méd. Int. 2008, 29, 187–194. [Google Scholar] [CrossRef] [PubMed]
- Cappello, S.; Cereda, E.; Rondanelli, M.; Klersy, C.; Cameletti, B.; Albertini, R.; Magno, D.; Caraccia, M.; Turri, A.; Caccialanza, R. Elevated Plasma Vitamin B12 Concentrations Are Independent Predictors of In-Hospital Mortality in Adult Patients at Nutritional Risk. Nutrients 2016, 9, 1. [Google Scholar] [CrossRef]
- Serraj, K.; Mecili, M.; Housni, I.; Andrès, E. Hypervitaminémie B12: Physiopathologie et intérêt en pratique clinique. Presse Médicale 2011, 40, 1120–1127. [Google Scholar] [CrossRef]
- Arendt, J.F.B.; Nexo, E. Cobalamin Related Parameters and Disease Patterns in Patients with Increased Serum Cobalamin Levels. PLoS ONE 2012, 7, e45979. [Google Scholar] [CrossRef]
- Gimsing, P. Cobalamin forms and analogues in plasma and myeloid cells during chronic myelogenous leukaemia related to clinical condition. Br. J. Haematol. 2008, 89, 812–819. [Google Scholar] [CrossRef]
- Gimsing, P. Cobalamin metabolism in chronic myelogenous leukemia. Dan. Med. Bull. 1998, 45, 459–479. [Google Scholar]
- Vlasveld, L.T.; Bos, G.M.J.; Ermens, A.A.M.; Bakker, J.A.; Lindemans, J. Hyperhomocysteinemia and functional cobalamin deficiency due to granulocytosis-induced alterations in the cobalamin-binding protein. Haematologica 2006, 91, 394–396. [Google Scholar] [PubMed]
- Simonsen, K.; Rode, A.; Nicoll, A.; Villadsen, G.; Espelund, U.; Lim, L.; Angus, P.; Arachchi, N.; Vilstrup, H.; Nexo, E.; et al. Vitamin B12 and its binding proteins in hepatocellular carcinoma and chronic liver diseases. Scand. J. Gastroenterol. 2014, 49, 1096–1102. [Google Scholar] [CrossRef]
- Baker, H.; Leevy, C.B.; DeAngelis, B.; Frank, O.; Baker, E.R. Cobalamin (vitamin B12) and holotranscobalamin changes in plasma and liver tissue in alcoholics with liver disease. J. Am. Coll. Nutr. 1998, 17, 235–238. [Google Scholar] [CrossRef] [PubMed]
- Lambert, D.; Benhayoun, S.; Adjalla, C.; Gélot, M.M.; Renkes, P.; Gérard, P.; Felden, F.; Belleville, F.; Gaucher, P.; Guéant, J.L.; et al. Alcoholic Cirrhosis and Cobalamin Metabolism. Digestion 1997, 58, 64–71. [Google Scholar] [CrossRef] [PubMed]
- Hannibal, L.; Siebert, M.; Basgalupp, S.; Vario, F.; Spiekerkoetter, U.; Blom, H.J. Hampered Vitamin B12 Metabolism in Gaucher Disease? J. Inborn Errors Metab. Screen. 2017, 5. [Google Scholar] [CrossRef]
- Arendt, J.F.B.; Pedersen, L.; Nexo, E.; Sørensen, H.T. Elevated Plasma Vitamin B12 Levels as a Marker for Cancer: A Population-Based Cohort Study. JNCI J. Natl. Cancer Inst. 2013, 105, 1799–1805. [Google Scholar] [CrossRef] [PubMed]
- Arendt, J.F.H.; Sørensen, H.T.; Horsfall, L.J.; Petersen, I. Elevated Vitamin B12 Levels and Cancer Risk in UK Primary Care: A THIN Database Cohort Study. Cancer Epidemiol. Biomarkers Prev. 2019, 28, 814–821. [Google Scholar] [CrossRef]
- Jammal, M.; Deneuville, T.; Mario, N.; Tiev, K.; Tolédano, C.; Josselin-Mahr, L.; Pateron, D.; Guidet, B.; Retbi, A.; Taright, N.; et al. Concentration plasmatique élevée de la vitamine B12: Un indicateur des maladies hépatiques ou tumorales. Rev. Médecine Interne 2013, 34, 337–341. [Google Scholar] [CrossRef]
- Collin, S.M. Folate and B12 in prostate cancer. Adv. Clin. Chem. 2013, 60, 1–63. [Google Scholar]
- Matejcic, M.; de Batlle, J.; Ricci, C.; Biessy, C.; Perrier, F.; Huybrechts, I.; Weiderpass, E.; Boutron-Ruault, M.C.; Cadeau, C.; His, M.; et al. Biomarkers of folate and vitamin B12 and breast cancer risk: Report from the EPIC cohort: Biomarkers of folate and vitamin B12 and BC risk. Int. J. Cancer 2017, 140, 1246–1259. [Google Scholar] [CrossRef]
- Fanidi, A.; Carreras-Torres, R.; Larose, T.L.; Yuan, J.-M.; Stevens, V.L.; Weinstein, S.J.; Albanes, D.; Prentice, R.; Pettinger, M.; Cai, Q.; et al. Is high vitamin B12 status a cause of lung cancer? Is high vitamin B12 status a cause of lung cancer? Int. J. Cancer 2019, 145, 1499–1503. [Google Scholar] [CrossRef]
- Tastekin, D.; Erturk, K.; Bozbey, H.U.; Olmuscelik, O.; Kiziltan, H.; Tuna, S.; Tas, F. Plasma homocysteine, folate and vitamin B12 levels in patients with lung cancer. Exp. Oncol. 2015, 37, 218–222. [Google Scholar] [CrossRef]
- Arshad, M.; Rezvandoost, N.; Pazouki, A.; Riazi, S.; Aghababa Rangraz, M.; Mokhber, S. Assessment of the Serum Levels of Hemoglobin, Ferritin, and Vitamin B12 in a Sample of Iranian Population With Morbid Obesity. J. Minim. Invasive Surg. Sci. 2016, 5. [Google Scholar] [CrossRef]
- Frenkel, E.P.; White, J.D.; Reisch, J.S.; Sheehan, R.G. Comparison of two methods for radioassay of vitamin B12 in serum. Clin. Chem. 1973, 19, 1357–1360. [Google Scholar] [CrossRef] [PubMed]
- Berg, R.L.; Shaw, G.R. Laboratory Evaluation for Vitamin B12 Deficiency: The Case for Cascade Testing. Clin. Med. Res. 2013, 11, 7–15. [Google Scholar] [CrossRef] [PubMed]
- McMahon, G.M.; Hwang, S.-J.; Tanner, R.M.; Jacques, P.F.; Selhub, J.; Muntner, P.; Fox, C.S. The association between vitamin B12, albuminuria and reduced kidney function: An observational cohort study. BMC Nephrol. 2015, 16, 7. [Google Scholar] [CrossRef]
- Andrès, E.; Kurtz, J.-E.; Perrin, A.-E.; Maloisel, F.; Demangeat, C.; Goichot, B.; Schlienger, J.-L. Oral cobalamin therapy for the treatment of patients with food-cobalamin malabsorption. Am. J. Med. 2001, 111, 126–129. [Google Scholar] [CrossRef]
- Rochat, M.C.; Vollenweider, P.; Waeber, G. Therapeutic and clinical implications of elevated levels of vitamin B12. Rev. Med. Suisse 2012, 8, 2072–2074. [Google Scholar]
- Rain, J.D. Intérêt en hématologie du dosage des cobalamines et des folates. Immuno-Anal. Biol. Spéc. 1992, 7, 17–24. [Google Scholar] [CrossRef]
- Cowppli-Bony, A.; Colonna, M.; Ligier, K.; Jooste, V.; Defossez, G.; Monnereau, A.; Amadeo, B.; Arveux, P.; Baldi, I.; Bara, S.; et al. Épidémiologie descriptive des cancers en France métropolitaine: Incidence, survie et prévalence. Bull. Cancer (Paris) 2019, 106, 617–634. [Google Scholar] [CrossRef]
- Arendt, J.F.H.; Farkas, D.K.; Pedersen, L.; Nexo, E.; Sørensen, H.T. Elevated plasma vitamin B12 levels and cancer prognosis: A population-based cohort study. Cancer Epidemiol. 2016, 40, 158–165. [Google Scholar] [CrossRef]
- Arendt, J.F.B.; Nexo, E. Unexpected high plasma cobalamin/Proposal for a diagnostic strategy. Clin. Chem. Lab. Med. 2013, 51, 489–496. [Google Scholar] [CrossRef]
- Ermens, A.a.M.; Vlasveld, L.T.; Lindemans, J. Significance of elevated cobalamin (vitamin B12) levels in blood. Clin. Biochem. 2003, 36, 585–590. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Normal-B12 * (n = 785) | High-B12 † (n = 785) | p-value | |
|---|---|---|---|
| General characteristics | |||
| Age (years) | 82.0 (73.0–89.0) | 82.0 (73.0–89.0) | - |
| Sex (women) | 472 (60.1%) | 472 (60.1%) | - |
| Vitamin B12 (ng/L) | 388 (277–534) | 1408 (1147–1868) | <0.001 |
| Elevated B12-related causes | |||
| Chronic liver diseases | 25 (3.2%) | 54 (6.9%) | 0.001 |
| Acute liver diseases | 20 (2.5%) | 64 (8.2%) | <0.001 |
| Severe chronic kidney failure | 74 (9.4%) | 128 (16.3%) | <0.001 |
| Autoimmune/inflammatory diseases | 68 (8.7%) | 49 (6.2%) | 0.09 |
| Excessive vitamin B12 supplementation | 3 (0.4%) | 16 (2.0%) | 0.004 |
| Myeloid blood malignancies | 8 (1.0%) | 34 (4.3%) | <0.001 |
| Lymphoid blood malignancies | 25 (3.2%) | 24 (3.1%) | >0.99 |
| Solid cancers | |||
| Without metastases | 64 (8.2%) | 152 (19.4%) | <0.001 |
| With metastases | 33 (4.2%) | 100 (12.7%) | <0.001 |
| Site of primary cancer | |||
| Colon/rectum | 10 (1.3%) | 25 (3.2%) | 0.02 |
| Liver | 3 (0.4%) | 7 (0.9%) | 0.34 |
| Pancreas | 3 (0.4%) | 11 (1.4%) | 0.06 |
| Skin | 2 (0.3%) | 6 (0.8%) | 0.29 |
| Lungs | 9 (1.1%) | 16 (2.0%) | 0.23 |
| Prostate | 13 (1.7%) | 28 (3.6%) | 0.03 |
| Kidneys | 5 (0.6%) | 3 (0.4%) | 0.73 |
| Breast | 11 (1.4%) | 22 (2.8%) | 0.06 |
| Urothelium | 4 (0.5%) | 15 (1.9%) | 0.01 |
| Uterus (body/neck) and ovaries | 4 (0.5%) | 8 (1.0%) | 0.38 |
| Esophagus and stomach | 2 (0.3%) | 8 (1.0%) | 0.11 |
| Others | 3 (0.4%) | 22 (2.8%) | <0.001 |
| Location of metastases | |||
| Brain | 7 (0.9%) | 9 (1.1%) | 0.79 |
| Liver | 10 (1.3%) | 56 (7.1%) | <0.001 |
| Bones | 9 (1.1%) | 44 (5.6%) | <0.001 |
| Lungs | 9 (1.1%) | 28 (3.6%) | 0.002 |
| Lymph nodes | 7 (0.9%) | 30 (3.8%) | <0.001 |
| Others | 12 (1.5%) | 25 (3.2%) | 0.03 |
| Adjusted OR * [95% CI] | p-value | |
|---|---|---|
| Sex (Males) | 0.87 [0.70–1.08] | 0.21 |
| Age † | 0.93 [0.75–1.17] | 0.55 |
| Chronic liver diseases | 2.80 [1.65–4.76] | <10−4 |
| Acute liver diseases | 2.43 [1.40–4.21] | 0.002 |
| Severe chronic kidney failure | 2.03 [1.43–2.88] | <10−4 |
| Autoimmune or inflammatory diseases | 0.83 [0.56–1.23] | 0.35 |
| Excessive vitamin B12 supplementation | 6.87 [1.98–23.86] | 0.002 |
| Myeloid malignancies | 5.46 [2.44–12.25] | <10−4 |
| Lymphoid malignancies | 1.22 [0.65–2.30] | 0.53 |
| Cancer | ||
| No cancer | 1.0 (reference) ‡ | - |
| Cancer without metastases | 1.96 [1.18–3.25] | 0.003 |
| Cancer with metastases | 4.21 [2.67–6.64] | <10−4 |
| Vitamin B12 (ng/L) | 0–749 | 750–999 | 1000–1249 | 1250–1749 | ≥1750 |
|---|---|---|---|---|---|
| No cancer (n, %) | 665/719 (92.5%) | 56/66 (84.8%) | 246/285 (86.3%) | 211/268 (78.7%) | 176/232 (75.9%) |
| Cancer without metastases (n, %) | 23/719 (3.2%) | 8/66 (12.1%) | 14/285(4.9%) | 23/268 (8.6%) | 15/232 (6.5%) |
| Cancer with metastases(n, %) | 31/719 (4.3%) | 2/66 (3.0%) | 25/285(8.8%) | 34/268 (12.7%) | 41/232 (17.7%) |
| Adjusted OR * [95%CI] | p-value | |
|---|---|---|
| A—Sites of solid cancers † | ||
| Colon and rectum | 3.02 [1.35–6.75] | 0.007 |
| Liver | 1.46 [0.30–7.15] | 0.64 |
| Pancreas | 4.00 [1.02–15.65] | 0.04 |
| Skin | 2.62 [0.49–13.92] | 0.26 |
| Lungs | 2.89 [1.14–7.35] | 0.03 |
| Prostate | 2.17 [1.02–4.63] | 0.04 |
| Kidneys | 0.31 [0.06–1.66] | 0.17 |
| Breasts | 1.86 [0.77–4.47] | 0.17 |
| Urothelium | 7.40 [1.77–30.87] | 0.006 |
| Uterus (body/neck) and ovaries | 1.07 [0.30–3.82] | 0.91 |
| Esophagus and stomach | 3.47 [0.69–17.49] | 0.13 |
| Others | 14.94 [3.89–57.3] | <10−4 |
| B—Sites of metastases † | ||
| Brain | 0.57 [0.14–2.30] | 0.43 |
| Liver | 4.88 [2.16–11.00] | <10−4 |
| Bones | 3.11 [1.33–7.27] | 0.009 |
| Lungs | 2.10 [0.76–5.82] | 0.15 |
| Lymph nodes | 2.58 [0.94–7.07] | 0.07 |
| Others | 0.59 [0.22–1.58] | 0.29 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Urbanski, G.; Hamel, J.-F.; Prouveur, B.; Annweiler, C.; Ghali, A.; Cassereau, J.; Lozac’h, P.; Lavigne, C.; Lacombe, V. Strength of the Association of Elevated Vitamin B12 and Solid Cancers: An Adjusted Case-Control Study. J. Clin. Med. 2020, 9, 474. https://doi.org/10.3390/jcm9020474
Urbanski G, Hamel J-F, Prouveur B, Annweiler C, Ghali A, Cassereau J, Lozac’h P, Lavigne C, Lacombe V. Strength of the Association of Elevated Vitamin B12 and Solid Cancers: An Adjusted Case-Control Study. Journal of Clinical Medicine. 2020; 9(2):474. https://doi.org/10.3390/jcm9020474
Chicago/Turabian StyleUrbanski, Geoffrey, Jean-François Hamel, Benoît Prouveur, Cédric Annweiler, Alaa Ghali, Julien Cassereau, Pierre Lozac’h, Christian Lavigne, and Valentin Lacombe. 2020. "Strength of the Association of Elevated Vitamin B12 and Solid Cancers: An Adjusted Case-Control Study" Journal of Clinical Medicine 9, no. 2: 474. https://doi.org/10.3390/jcm9020474
APA StyleUrbanski, G., Hamel, J.-F., Prouveur, B., Annweiler, C., Ghali, A., Cassereau, J., Lozac’h, P., Lavigne, C., & Lacombe, V. (2020). Strength of the Association of Elevated Vitamin B12 and Solid Cancers: An Adjusted Case-Control Study. Journal of Clinical Medicine, 9(2), 474. https://doi.org/10.3390/jcm9020474