Prognosis-Predicting Model Based on [18F]fluorodeoxyglucose PET Metabolic Parameters in Locally Advanced Cervical Cancer Patients Treated with Concurrent Chemoradiotherapy: Multi-Center Retrospective Study

 , , , , ,
, , , , ,
Abstract
1. Introduction
2. Materials and Methods
2.1. Patients
2.2. Treatment
2.3. Pre-Treatment Assessment
2.4. Image Analysis
2.5. Clinical Follow-up
2.6. Statistical Analysis
2.7. Validation of the Nomogram
3. Results
3.1. Independent Prognostic Factors for the Risk Model
3.2. Nomogram and Computation of Risk Scores for Predicting Tumor Recurrence
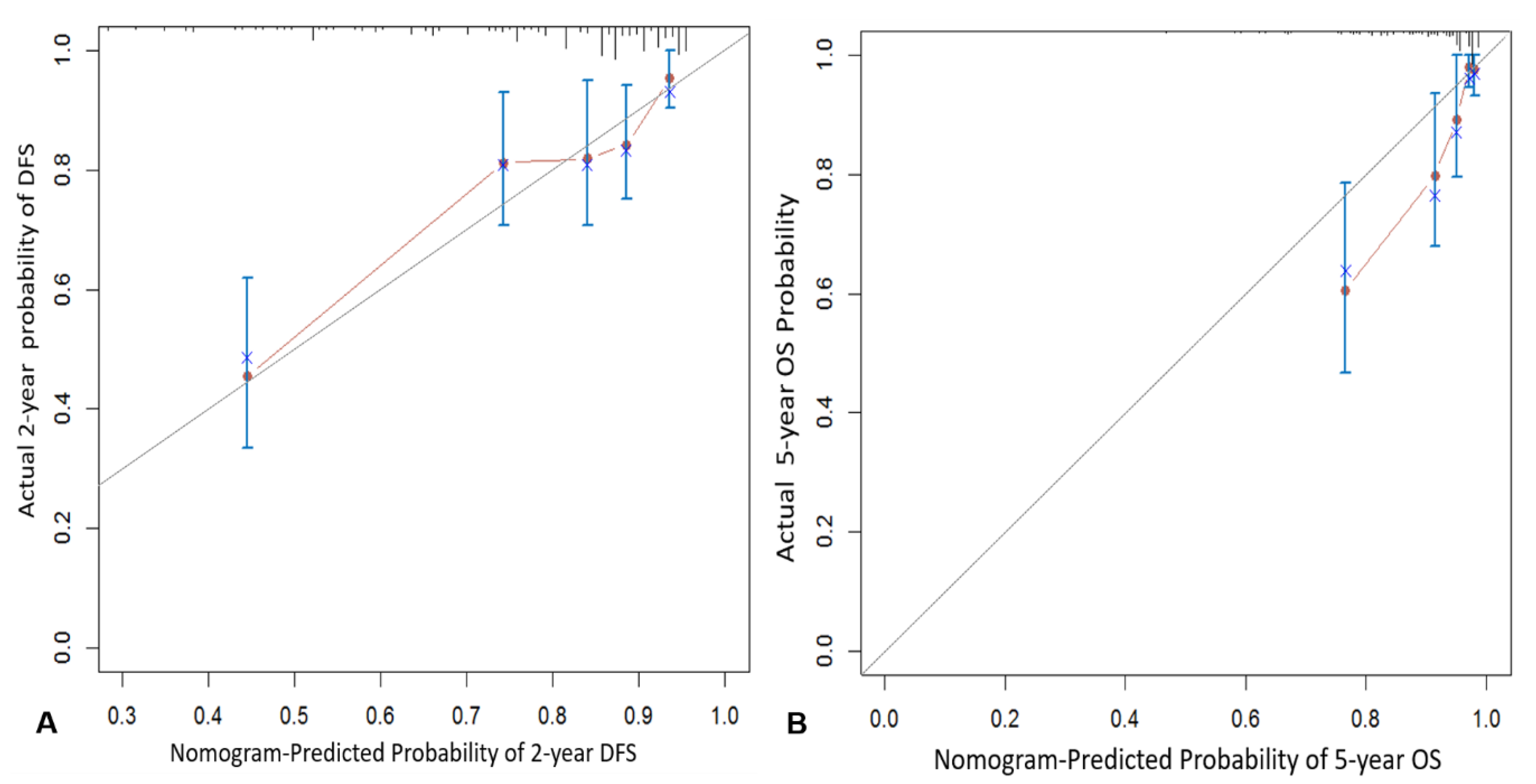
3.3. Internal Validation
3.4. Discrimination Ability of Nomogram for Prognosis
4. Discussion
5. Conclusion
Author Contributions
Funding
Conflicts of Interest
Ethical Approval
Informed Consent
References
- Green, J.A.; Kirwan, J.M.; Tierney, J.F.; Symonds, P.; Fresco, L.; Collingwood, M.; Williams, C.J. Survival and recurrence after concomitant chemotherapy and radiotherapy for cancer of the uterine cervix: A systematic review and meta-analysis. Lancet 2001, 358, 781–786. [Google Scholar] [CrossRef]
- Whitney, C.W.; Sause, W.; Bundy, B.N.; Malfetano, J.H.; Hannigan, E.V.; Fowler, W.C., Jr.; Clarke-Pearson, D.L.; Liao, S.Y. Randomized comparison of fluorouracil plus cisplatin versus hydroxyurea as an adjunct to radiation therapy in stage IIB-IVA carcinoma of the cervix with negative para-aortic lymph nodes: A Gynecologic Oncology Group and Southwest Oncology Group study. J. Clin. Oncol. 1991, 17, 1339–1348. [Google Scholar] [CrossRef] [PubMed]
- Collaboration Chemoradiotherapy for Cervical Cancer Meta-Analysis Collaboration. Reducing uncertainties about the effects of chemoradiotherapy for cervical cancer: A systematic review and metaanalysis of individual patient data from 18 randomized trials. J. Clin. Oncol. 2008, 26, 5802–5812. [Google Scholar] [CrossRef] [PubMed]
- Lee, D.W.; Kim, Y.T.; Kim, J.H.; Kim, S.; Kim, S.W.; Nam, E.J.; Kim, J.W. Clinical significance of tumor volume and lymph node involvement assessed by MRI in stage IIB cervical cancer patients treated with concurrent chemoradiation therapy. J. Gynecol. Oncol. 2010, 21, 18–23. [Google Scholar] [CrossRef]
- Endo, D.; Todo, Y.; Okamoto, K.; Ninobe, S.; Kato, H.; Nishiyama, N. Prognostic factors for patients with cervical cancer treated with concurrent chemoradiotherapy: A retrospective analysis in a Japanese cohort. J. Gynecol. Oncol. 2015, 26, 12–18. [Google Scholar] [CrossRef]
- Wong, T.Z.; Jones, E.L.; Coleman, R.E. Positron emission tomography with 2-deoxy-2-[(18)F]fluoro-D-glucose for evaluating local and distant disease in patients with cervical cancer. Mol. Imaging Biol. 2004, 6, 55–62. [Google Scholar] [CrossRef]
- Kidd, E.A.; Siegel, B.A.; Dehdashti, F.; Grigsby, P.W. Pelvic lymph node F-18 fluorodeoxyglucose uptake as a prognostic biomarker in newly diagnosed patients with locally advanced cervical cancer. Cancer 2010, 116, 1469–1475. [Google Scholar] [CrossRef]
- Onal, C.; Reyhan, M.; Parlak, C.; Guler, O.C.; Oymak, E. Prognostic value of pretreatment 18F-fluorodeoxyglucose uptake in patients with cervical cancer treated with definitive chemoradiotherapy. Int. J. Gynecol. Cancer 2013, 23, 1104–1110. [Google Scholar] [CrossRef]
- Onal, C.; Guler, O.C.; Reyhan, M.; Yapar, A.F. Prognostic value of 18F-fluorodeoxyglucose uptake in pelvic lymph nodes in patients with cervical cancer treated with definitive chemoradiotherapy. Gynecol. Oncol. 2015, 137, 40–46. [Google Scholar] [CrossRef]
- Bollineni, V.R.; Ytre-Hauge, S.; Gulati, A.; Halle, M.K.; Woie, K.; Salvensen, Ø.; Trovik, J.; Krakstad, C.; Haldorsen, I.S. The prognostic value of preoperative FDG-PET/CT metabolic parameters in cervical cancer patients. Eur. J. Hybrid. Imaging 2018, 24, 1–14. [Google Scholar] [CrossRef]
- Lucia, F.; Visvikis, D.; Desseroit, M.C.; Miranda, O.; Malhaire, J.P.; Robin, P.; Pradier, O.; Hatt, M.; Schick, U. Prediction of outcome using pretreatment 18F-FDG PET/CT and MRI radiomics in locally advanced cervical cancer treated with chemoradiotherapy. Eur. J. Nucl. Med. Mol. Imaging 2018, 45, 768–786. [Google Scholar] [CrossRef] [PubMed]
- Chong, G.O.; Jeong, S.Y.; Park, S.H.; Lee, Y.H.; Lee, S.W.; Hong, D.G.; Kim, J.C.; Lee, Y.S.; Cho, Y.L. Comparison of the Prognostic Value of F-18 Pet Metabolic Parameters of Primary Tumors and Regional Lymph Nodes in Patients with Locally Advanced Cervical Cancer Who Are Treated with Concurrent Chemoradiotherapy. PLoS ONE 2015, 10, e0137743. [Google Scholar] [CrossRef] [PubMed]
- Chong, G.O.; Lee, W.K.; Jeong, S.Y.; Park, S.H.; Lee, Y.H.; Lee, S.W.; Hong, D.G.; Kim, J.C.; Lee, Y.S. Prognostic value of intratumoral metabolic heterogeneity on F-18 fluorodeoxyglucose positron emission tomography/computed tomography in locally advanced cervical cancer patients treated with concurrent chemoradiotherapy. Oncotarget 2017, 8, 90402–90412. [Google Scholar] [CrossRef] [PubMed]
- Seo, Y.S.; Yoo, S.Y.; Kim, M.S.; Yang, K.M.; Yoo, H.J.; Kim, J.H.; Shin, Y.J.; Kang, J.K.; Lee, K.H.; Lee, E.D.; et al. Nomogram prediction of overall survival after curative irradiation for uterine cervical cancer. Nomogram prediction of overall survival after curative irradiation for uterine cervical cancer. Int. J. Radiat. Oncol. Biol. Phys. 2011, 79, 782–787. [Google Scholar] [CrossRef] [PubMed]
- Tseng, J.Y.; Yen, M.S.; Twu, N.F.; Lai, C.R.; Horng, H.C.; Tseng, C.C.; Chao, K.C.; Juang, C.M. Prognostic nomogram for overall survival in stage IIB-IVA cervical cancer patients treated with concurrent chemoradiotherapy. Am. J. Obstet. Gynecol. 2010, 202, e1–e7. [Google Scholar] [CrossRef] [PubMed]
- Shim, S.H.; Lee, S.W.; Park, J.Y.; Kim, Y.S.; Kim, D.Y.; Kim, J.H.; Kim, Y.M.; Kim, Y.T.; Nam, J.H. Risk assessment model for overall survival in patients with locally advanced cervical cancer treated with definitive concurrent chemoradiotherapy. Gynecol. Oncol. 2013, 128, 54–59. [Google Scholar] [CrossRef]
- Rose, P.G.; Java, J.; Whitney, C.W.; Stehman, F.B.; Lanciano, R.; Thomas, G.M.; DiSilvestro, P.A. Nomograms Predicting Progression-Free Survival, Overall Survival, and Pelvic Recurrence in Locally Advanced Cervical Cancer Developed From an Analysis of Identifiable Prognostic Factors in Patients From NRG Oncology/Gynecologic Oncology Group Randomized Trials of Chemoradiotherapy. J. Clin. Oncol. 2015, 33, 2136–2142. [Google Scholar]
- Wang, W.; Liu, X.; Meng, Q.; Zhang, F.; Hu, K. Nomograms predicting survival and patterns of failure in patients with cervical cancer treated with concurrent chemoradiotherapy: A special focus on lymph nodes metastases. PLoS ONE 2019, 14, e0214498. [Google Scholar] [CrossRef]
- Kidd, E.A.; El Naqa, I.; Siegel, B.A.; Dehdashti, F.; Grigsby, P.W. FDG-PET-based prognostic nomograms for locally advanced cervical cancer. Gynecol. Oncol. 2012, 127, 136–140. [Google Scholar] [CrossRef]
- Pecorelli, S. Revised FIGO staging for carcinoma of the vulva, cervix, and endometrium. Int. J. Gynaecol. Obstet. 2009, 105, 103–104. [Google Scholar] [CrossRef]
- Tod, M.; Meredith, W. Treatment of cancer of the cervix uteri—A revised “Manchester method”. Br. J. Radiol. 1953, 26, 252–257. [Google Scholar] [CrossRef] [PubMed]
- Iasonos, A.; Schrag, D.; Raj, G.V.; Panageas, K.S. How to build and interpret a nomogram for cancer prognosis. J. Clin. Oncol. 2008, 26, 1364–1370. [Google Scholar] [CrossRef] [PubMed]
- Kang, S.; Nam, B.H.; Park, J.Y.; Seo, S.S.; Ryu, S.Y.; Kim, J.W.; Kim, S.C.; Park, S.Y.; Nam, J.H. Risk assessment tool for distant recurrence after platinum-based concurrent chemoradiation in patients with locally advanced cervical cancer: A Korean gynecologic oncology group study. J. Clin. Oncol. 2012, 30, 2369–2374. [Google Scholar] [CrossRef] [PubMed]
- Lora, D.; Gómez de la Cámara, A.; Fernández, S.P.; Enríquez de Salamanca, R.; Fermín Pérez Regadera Gómez, J. Prognostic models for locally advanced cervical cancer: External validation of the published models. J. Gynecol. Oncol. 2017, 28, e58. [Google Scholar] [CrossRef]
- Yang, Y.C.; Shen, J.; Tate, J.E.; Wang, K.G.; Su, T.H.; Wang, K.L.; Jeng, C.L.; Chen, H.S.; Chiang, S.; Crum, C. Cervical cancer in young womenin Taiwan: Prognosis is independent of papillomavirus or tumor cell type. Gynecol. Oncol. 1997, 64, 59–63. [Google Scholar] [CrossRef]
- Cao, L.; Li, X.; Zhang, Y.; Li, X.; Wang, Q. Clinical features and prognosis of cervical cancer in young women. J. Central. South Univ. (Med. Sci.) 2010, 35, 875–878. [Google Scholar]
- Wang, J.; Wang, T.; Yang, Y.Y.; Chai, Y.L.; Shi, F.; Liu, Z. Patient age, tumor appearance and tumor size are risk factors for early recurrence of cervical cancer. Mol. Clin. Oncol. 2015, 3, 363–366. [Google Scholar] [CrossRef]
- Pencina, M.J.; D’Agostino, R.B. OverallCas a measure of discrimination in survival analysis: Model specific population value and confidence interval estimation. Stat. Med. 2004, 23, 2109–2123. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Variables | Sample Size (n) | Recurrence | Log-Rank Test | |||
|---|---|---|---|---|---|---|
| (n, %) | 2-Year DF (95% CI) | χ2 | p | |||
| Age | <40 | 34 | 12 (35.3) | 0.66 (0.49–0.82) | 4.13 | 0.127 |
| 41–62 | 167 | 45 (26.6) | 0.79 (0.73–0.85) | |||
| ≥63 | 69 | 12 (17.4) | 0.84 (0.75–0.93) | |||
| FIGO stage | IIB | 215 | 45 (20.9) | 0.83 (0.77–0.88) | 15.84 | <0.001 |
| ≥IIB | 55 | 24 (43.6) | 0.63 (0.49–0.76) | |||
| Histology | SCC | 243 | 60 (24.7) | 0.79 (0.74–0.85) | 1.33 | 0.249 |
| AC/ASC | 27 | 9 (33.3) | 0.71 (0.53–0.90) | |||
| Size | <4.2 | 59 | 7 (11.9) | 0.95 (0.89–1.01) | 14.34 | 0.001 |
| 4.3–6.0 | 66 | 13 (19.7) | 0.86 (0.77–0.94) | |||
| ≥6.0 | 145 | 49 (33.8) | 0.69 (0.61–0.77) | |||
| SCC antigen | <23.3 | 223 | 48 (21.5) | 0.82 (0.77–0.87) | 21.74 | <0.001 |
| ≥23.3 | 47 | 21 (44.7) | 0.63 (0.49–0.77) | |||
| Hemoglobin | <12 | 150 | 45 (30.0) | 0.74 (0.67–0.81) | 3.92 | 0.048 |
| ≥12 | 120 | 24 (20.0) | 0.84 (0.78–0.91) | |||
| HPV status | Positive | 160 | 38 (23.8) | 0.81 (0.74–0.87) | 1.02 | 0.312 |
| Negative/Unknown | 110 | 31 (28.2) | 0.76 (0.67–0.84) | |||
| pSUVmax | <12.5 | 148 | 27 (18.2) | 0.88 (0.82–0.93) | 10.04 | 0.002 |
| ≥12.5 | 122 | 42 (34.4) | 0.68 (0.60–0.76) | |||
| nSUVmax | 4.2 | 195 | 30 (15.4) | 0.86 (0.81–0.91) | 49.06 | <0.001 |
| 4.3–5.8 | 24 | 10 (41.7) | 0.76 (0.57–0.94) | |||
| ≥5.8 | 51 | 29 (56.9) | 0.53 (0.39–0.67) | |||
| Variables | Sample Size (n) | Death | Log-Rank Test | |||
|---|---|---|---|---|---|---|
| (n, %) | 5-Year OS (95% CI) | χ2 | p | |||
| Age | <48 | 87 | 18 (20.7) | 0.80 (0.70–0.89) | 6.67 | 0.01 |
| ≥48 | 183 | 15 (8.2) | 0.89 (0.84–0.95) | |||
| FIGO stage | IIB | 215 | 22 (10.2) | 0.88 (0.83–0.93) | 6.49 | 0.011 |
| >IIB | 55 | 11 (20.0) | 0.75 (0.62–0.89) | |||
| Histology | SCC | 243 | 27 (11.1) | 0.87 (0.82–0.92) | 2.97 | 0.085 |
| AC/ASC | 27 | 6 (22.2) | 0.75 (0.55–0.95) | |||
| Size | <5.0 | 165 | 13 (7.9) | 0.93 (0.89–0.97) | 11.86 | 0.001 |
| ≥5.0 | 105 | 20 (19.0) | 0.73 (0.62–0.83) | |||
| SCC antigen | <21.6 | 217 | 20 (9.2) | 0.90 (0.86–0.94) | 10.36 | 0.001 |
| ≥21.6 | 53 | 13 (24.5) | 0.68 (0.53–0.83) | |||
| Hemoglobin | <11.7 | 129 | 20 (15.5) | 0.81 (0.73–0.89) | 3.31 | 0.069 |
| ≥11.7 | 141 | 13 (9.2) | 0.90 (0.84–0.95) | |||
| HPV status | Positive | 160 | 13 (8.1) | 0.89 (0.84–0.95) | 5.9 | 0.015 |
| Negative/Unknown | 110 | 20 (18.2) | 0.81 (0.73–0.90) | |||
| pSUVmax | <12.5 | 148 | 10 (6.8) | 0.92 (0.87–0.97) | 9.67 | 0.002 |
| ≥12.5 | 122 | 23 (18.9) | 0.79 (0.71–0.87) | |||
| nSUVmax | <4.2 | 195 | 16 (8.2) | 0.90 (0.86–0.95) | 12.86 | <0.001 |
| ≥4.2 | 75 | 17 (22.7) | 0.73 (0.60–0.86) | |||
| Variables | Univariate | Multivariate | |||
|---|---|---|---|---|---|
| HR (95% CI) | p | HR (95% CI) | p | ||
| Age | <40 | 2.26 (1.01–5.02) | 0.047 | 1.79 (0.79–4.07) | 0.164 |
| 41–62 | 1.54 (0.82–2.91) | 0.184 | 1.36 (0.70–2.64) | 0.36 | |
| ≥63 | 1 | 1 | |||
| FIGO stage | IIB | 1 | 1 | ||
| >IIB | 2.63 (1.60–4.33) | <0.001 | 2.07 (1.21–3.52) | 0.008 | |
| Histology | AC | 1 | |||
| AC/ASC | 1.53 (0.75–3.03) | 0.255 | |||
| Tumor size | <4.2 | 1 | 1 | ||
| 4.3–6.0 | 1.81 (0.72–4.55) | 0.205 | 1.42 (0.56–3.61) | 0.468 | |
| ≥6.0 | 3.60 (1.63–7.95) | 0.002 | 2.21 (0.97–5.04) | 0.059 | |
| SCC antigen | <23.3 | 1 | 1 | ||
| ≥23.3 | 2.46 (1.47–4.12) | 0.001 | 1.48 (0.87–2.52) | 0.151 | |
| Hemoglobin | <12 | 1.64 (1.00–2.69) | 0.051 | ||
| ≥12 | 1 | ||||
| HPV status | Positive | 1 | |||
| Negative/Unknown | 1.28 (0.79–2.05) | 0.315 | |||
| pSUVmax | <12.5 | 1 | 1 | ||
| ≥12.5 | 2.14 (1.32–3.47) | 0.002 | 1.16 (0.68–1.98) | 0.59 | |
| nSUVmax | 4.2 | 1 | 1 | ||
| 4.3–5.8 | 2.28 (1.77–2.94) | <0.001 | 2.18 (1.04–4.58) | 0.04 | |
| ≥5.8 | 4.08 (2.35–7.08) | <0.001 | |||
| Variables | Level | Univariate | Multivariate | ||
|---|---|---|---|---|---|
| HR (95% CI) | p | HR (95% CI) | p | ||
| Age | <48 | 2.40 (1.21–4.76) | 0.013 | 2.07 (1.02–4.22) | 0.045 |
| ≥48 | 1 | 1 | |||
| FIGO stage | IIB | 1 | 1 | ||
| >IIB | 2.49 (1.48–6.03) | 0.014 | 1.96 (0.92–4.16) | 0.082 | |
| Histology | AC | 1 | |||
| AC/ASC | 2.14 (0.88–5.17) | 0.093 | |||
| Tumor size | <5.0 | 1 | 1 | ||
| ≥5.0 | 3.22 (1.59–6.50) | 0.001 | 1.81 (0.88–3.74) | 0.11 | |
| SCC antigen | <21.6 | 1 | 1 | ||
| ≥21.6 | 2.99 (1.48–6.03) | 0.002 | 1.33 (0.62–2.85) | 0.47 | |
| Hemoglobin | <11.7 | 1.89 (0.94–3.80) | 0.051 | ||
| ≥11.7 | 1 | ||||
| HPV status | Positive | 1 | 1 | ||
| Negative/Unknown | 2.32 (1.15–4.66) | 0.019 | 1.81 (0.88–3.74) | 0.11 | |
| pSUVmax | <12.5 | 1 | 1 | ||
| ≥12.5 | 3.06 (1.46–6.44) | 0.003 | 1.82 (0.83–3.97) | 0.134 | |
| nSUVmax | <4.2 | 1 | 1 | ||
| ≥4.2 | 3.23 (1.64–6.46) | 0.001 | 1.57 (1.07–2.31) | 0.02 | |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lee, W.K.; Chong, G.O.; Jeong, S.Y.; Lee, H.J.; Park, S.-H.; Ryu, J.M.; Choi, Y.S.; Kang, S.; Koo, Y.-J.; Lee, D.H.; et al. Prognosis-Predicting Model Based on [18F]fluorodeoxyglucose PET Metabolic Parameters in Locally Advanced Cervical Cancer Patients Treated with Concurrent Chemoradiotherapy: Multi-Center Retrospective Study. J. Clin. Med. 2020, 9, 427. https://doi.org/10.3390/jcm9020427
Lee WK, Chong GO, Jeong SY, Lee HJ, Park S-H, Ryu JM, Choi YS, Kang S, Koo Y-J, Lee DH, et al. Prognosis-Predicting Model Based on [18F]fluorodeoxyglucose PET Metabolic Parameters in Locally Advanced Cervical Cancer Patients Treated with Concurrent Chemoradiotherapy: Multi-Center Retrospective Study. Journal of Clinical Medicine. 2020; 9(2):427. https://doi.org/10.3390/jcm9020427
Chicago/Turabian StyleLee, Won Kee, Gun Oh Chong, Shin Young Jeong, Hyun Jung Lee, Shin-Hyung Park, Jung Min Ryu, Youn Seok Choi, Sungmin Kang, Yu-Jin Koo, Dae Hyung Lee, and et al. 2020. "Prognosis-Predicting Model Based on [18F]fluorodeoxyglucose PET Metabolic Parameters in Locally Advanced Cervical Cancer Patients Treated with Concurrent Chemoradiotherapy: Multi-Center Retrospective Study" Journal of Clinical Medicine 9, no. 2: 427. https://doi.org/10.3390/jcm9020427
APA StyleLee, W. K., Chong, G. O., Jeong, S. Y., Lee, H. J., Park, S.-H., Ryu, J. M., Choi, Y. S., Kang, S., Koo, Y.-J., Lee, D. H., Kong, E., & Lee, S.-W. (2020). Prognosis-Predicting Model Based on [18F]fluorodeoxyglucose PET Metabolic Parameters in Locally Advanced Cervical Cancer Patients Treated with Concurrent Chemoradiotherapy: Multi-Center Retrospective Study. Journal of Clinical Medicine, 9(2), 427. https://doi.org/10.3390/jcm9020427