Saharan Dust Events in the Dust Belt -Canary Islands- and the Observed Association with in-Hospital Mortality of Patients with Heart Failure




 ,
, 
Abstract
1. Introduction
2. Materials and Methods
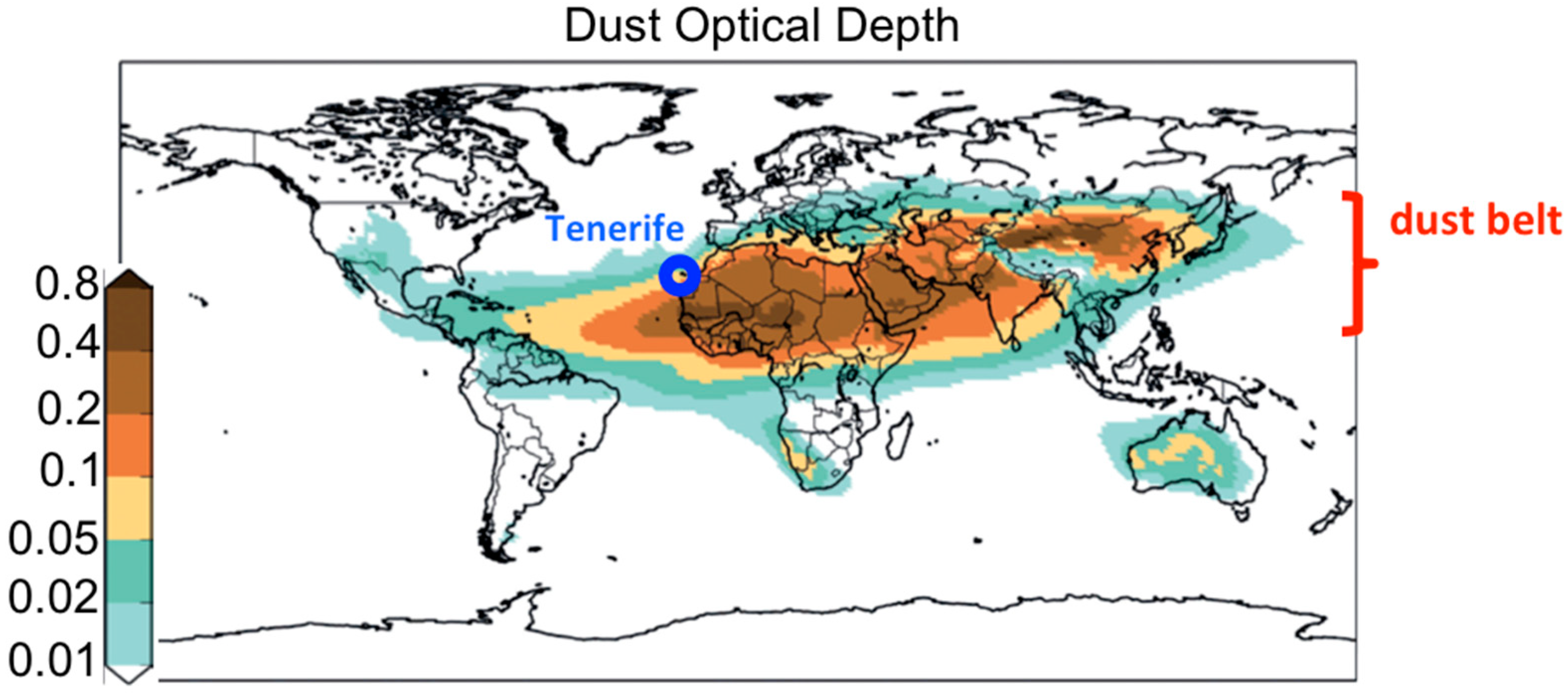
2.1. Study Region
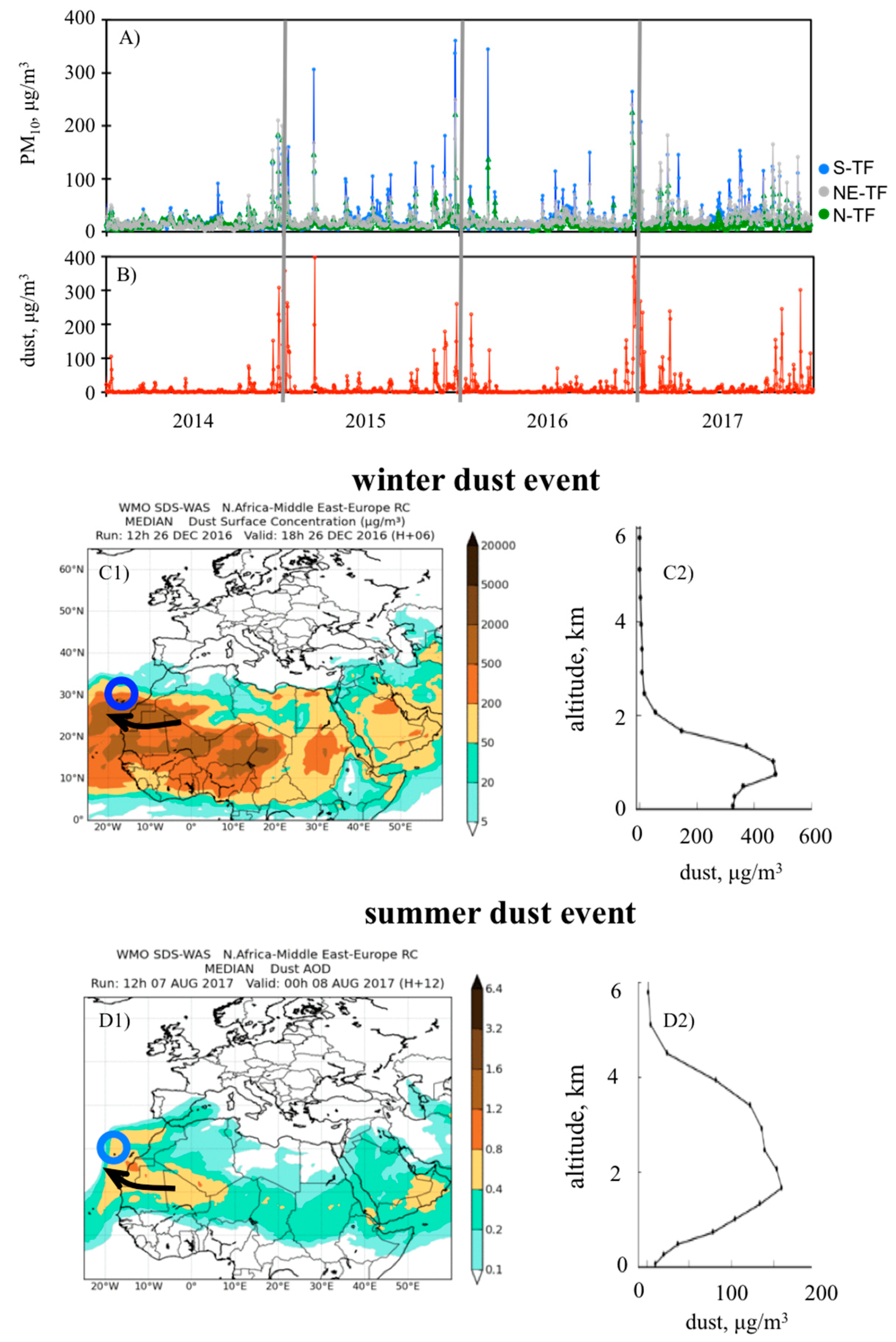
2.2. Dust Events
2.3. Medical Data
- demography—age and gender;
- cardiovascular risk factors—dichotomous variable reporting if the patient had hypertension, was a smoker, had diabetes mellitus or hypercholesterolemia;
- medical history—dichotomous variable on previous HF episodes, previous chronic ischemic heart disease (IHD), atrial fibrillation or chronic obstructive pulmonary disease (COPD);
- biochemistry—levels of hemoglobin (g/dL), brain natriuretic peptide (BNP: pg/mL) and sodium (mg/dL) were determined by analysis of blood samples;
- clinical data—data on the left ventricular ejection fraction (LVEF: %), hospital stay (d) and Charlson index;
- HF precipitating factors—therapeutic non-compliance, rapid atrial fibrillation, infections and unknown precipitating factors;
- in-hospital treatment—dichotomous variable reporting if patients received treatment with furosemide, spironolactone / eplerenone, beta blockers, angiotensin-converting enzyme inhibitor (ACEI) or angiotensin II receptor antagonists (ARA-II) during the period they stayed in the hospital.
2.4. Statistical Analysis
3. Results
3.1. Dust Events
3.2. Impact of Dust on In-Hospital Mortality of Patients with HF
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- World Health Organization. Burden of Disease from Ambient and Household Air Pollution. 2014. Available online: http://www.who.int/phe/health_topics/outdoorair/databases/en/ (accessed on 27 January 2019).
- Araujo, J.A.; Nel, A.E. Particulate matter and atherosclerosis: Role of particle size, composition and oxidative stress. Part Fibre Toxicol. 2009, 6, 24. [Google Scholar] [CrossRef] [PubMed]
- Araujo, J.A. Particulate air pollution, systemic oxidative stress, inflammation, and atherosclerosis. Air Qual. Atmos. Health 2010, 4, 79–93. [Google Scholar] [CrossRef] [PubMed]
- Barajas, B.; Che, N.; Yin, F.; Rowshanrad, A.; Orozco, L.D.; Gong, K.W.; Wang, X.; Castellani, L.W.; Reue, K.; Lusis, A.J.; et al. NF-E2-related factor 2 promotes atherosclerosis by effects on plasma lipoproteins and cholesterol transport that overshadow antioxidant protection. Arterioscler Thromb. Vasc. Biol. 2011, 31, 58–66. [Google Scholar] [CrossRef] [PubMed]
- Romanoski, C.E.; Che, N.; Yin, F.; Mai, N.; Pouldar, D.; Civelek, M.; Pan, C.; Lee, S.; Vakili, L.; Yang, W.P.; et al. Network for Activation of Human Endothelial Cells by Oxidized Phospholipids: A Critical Role of HemeOxygenase 1. Circ. Res. 2011, 109, 27–41. [Google Scholar] [CrossRef] [PubMed]
- Miller, M.R.; McLean, S.G.; Akeem, R.D.; Lawal, O.; Araujo, J.A.; Shaw, C.A.; Mills, N.L.; Donaldson, K.; Newby, D.E.; Hadoke, P.W.F. Diesel exhaust particulate increases the size and complexity of lesions in atherosclerotic mice. Part. Fibre Toxicol. 2013, 10, 61. [Google Scholar] [CrossRef] [PubMed]
- Dominguez-Rodriguez, A.; Rodríguez, S.; Abreu-Gonzalez, P.; Avanzas, P. Impact of air pollution on inflammation, oxidative stress and 1-year prognosis in patients hospitalized for acute coronary syndrome: design of the AIRACOS study. Med. Clin. 2013, 141, 529–532. [Google Scholar] [CrossRef]
- De Longueville, F.; Hountondji, Y.C.; Henry, S.; Ozer, P. What do we knowabouteffects of desert dust on air quality and human health in West Africa compared to other regions? Sci. Total Environ. 2010, 409, 1–8. [Google Scholar] [CrossRef]
- Kojima, S.; Michikawa, T.; Ueda, K.; Sakamoto, T.; Matsui, K.; Kojima, T.; Tsujita, K.; Ogawa, H.; Nitta, H.; Takami, A. Asian dust exposure triggers acute myocardial infarction. Eur. Heart J. 2017, 38, 3202–3208. [Google Scholar] [CrossRef]
- Dominguez-Rodriguez, A.; Baez-Ferrer, N.; Rodríguez, S.; Abreu-Gonzalez, P.; González-ColaçoHarmand, M.; Amarnani-Amarnani, V.; Cuevas, E.; Consuegra-Sanchez, L.; Alonso-Perez, S.; Avanzas, P.; et al. Impacto de la exposición a la calima del polvo del Sáhara en los pacientes con insuficiencia cardiaca aguda atendidos en un servicio de urgencias. Emergencias 2019, 31, 161–166. [Google Scholar]
- Dominguez-Rodriguez, A.; Rodríguez, S.; Abreu-Gonzalez, P. The impact of naturally generated particulate matter emanating from desert dust storms and cardiovascular pathophysiology: An alarming worldwide reality. Eur. Heart J. 2019, 40, 2375–2376. [Google Scholar] [CrossRef]
- Münzel, T.; Lelieveld, J.; Rajagopalan, S.; Daiber, A. Contribution of airborne desert dust to air quality and cardiopulmonary disease. Eur. Heart J. 2019, 40, 2377–2378. [Google Scholar] [CrossRef] [PubMed]
- Prospero, J.M.; Ginoux, P.; Torres, O.; Nicholson, S.E.; Gill, T.E. Environmental characterization of global sources of atmospheric soil dust identified with the Nimbus 7 Total Ozone Mapping Spectrometer (TOMS) absorbing aerosol product. Rev. Geophys. 2002, 40, 1–31. [Google Scholar] [CrossRef]
- Deroubaix, A.; Martiny, N.; Chiapello, I.; Marticorena, B. Suitability of OMI aerosol index to reflect mineral dust surface conditions: Preliminary application for studying the link with meningitis epidemics in the Sahel. Remote Sens. Environ. 2013, 133, 116–127. [Google Scholar] [CrossRef]
- Rodríguez, S.; Cuevas, E.; Prospero, J.M.; Alastuey, A.; Querol, X.; López-Solano, J.; García, M.I.; Alonso-Pérez, S. Modulation of Saharan dust export by the North African dipole. Atmos. Chem. Phys. 2015, 15, 7471–7486. [Google Scholar] [CrossRef]
- Almeida-Silva, M.; Almeida, S.M.; Freitas, M.C.; Pio, C.A.; Nunes, T.; Cardoso, J. Impact of Sahara dust transport on Cape Verde atmospheric element particles. J. Toxicol. Environ. Health 2013, 76, 240–251. [Google Scholar] [CrossRef]
- Rodríguez, S.; Querol, X.; Alastuey, A.; Plana, F. Sources and processes affecting levels and composition of atmospheric aerosol in the western Mediterranean. J. Geophys. Res. 2002, 107, 4777. [Google Scholar] [CrossRef]
- Pey, J.; Querol, X.; Alastuey, A.; Forastiere, F.; Stafoggia, M. African dust outbreaks over the Mediterranean Basin during 2001–2011: PM10 concentrations, phenomenology and trends, and its relation with synoptic and mesoscale meteorology. Atmos. Chem. Phys. 2013, 13, 1395–1410. [Google Scholar] [CrossRef]
- Stafoggia, M.; Zauli-Sajani, S.; Pey, J.; Samoli, E.; Alessandrini, E.; Basagaña, X.; Cernigliaro, A.; Chiusolo, M.; Demaria, M.; Díaz, J.; et al. Desert Dust Outbreaks in Southern Europe: Contribution to Daily PM10 Concentrations and Short-Term Associations with Mortalityand Hospital Admissions. Environ. Health Perspect. 2016, 124, 413–419. [Google Scholar] [CrossRef]
- DeLongueville, F.; Ozer, P.; Doumbia, S.; Henry, S. Desert dust impacts on human health: an alarming worldwide reality and a need for studies in West Africa. Int. J. Biometeorol. 2013, 57, 1–19. [Google Scholar] [CrossRef]
- Kurmani, S.; Squire, I. Acute heart failure: definition, classification and epidemiology. Curr. Heart Fail. Rep. 2017, 14, 385–392. [Google Scholar] [CrossRef]
- Aguirre Tejedo, A.; Miró, Ò. Precipitating factors in acute heart failure: A review. Emergencias 2017, 29, 185–193. [Google Scholar] [PubMed]
- Rodríguez, S.; Guerra, J.C. Monitoring of ozone in a marine environment in Tenerife (Canary Islands). Atmos. Environ. 2001, 135, 1829–1841. [Google Scholar] [CrossRef]
- Guerra, J.C.; Rodríguez, S.; Arencibia, M.T.; García, M.D. Study on the formation and transport of ozone in relation to the air quality management and vegetation protection in Tenerife (Canary Islands). Chemosphere 2004, 56, 1157–1167. [Google Scholar] [CrossRef] [PubMed]
- Terradellas, E.; Basart, S.; Cuevas, E. Airborne Dust: From R&D to Operational Forecast. Available online: https://public.wmo.int/en/resources/library/airborne-dust-from-rd-operational-forecast (accessed on 27 January 2020).
- Atger, F. The skill of ensemble prediction systems. Mon. Weather Rev. 1999, 127, 1941–1953. [Google Scholar] [CrossRef]
- García-Castrillo, G.; Terradellas, E. Evaluation of the Dust Forecasts in the Canary Islands. Available online: https://sds-was.aemet.es/materials/technical-reports/SDSWASNAMEE20170002.pdf (accessed on 25 January 2020).
- Núñez, E.; Steyerberg, E.W.; Nuñez, J. Regression modeling strategies. Rev. Esp. Cardiol. 2011, 64, 501–507. [Google Scholar] [CrossRef] [PubMed]
- Rodríguez, S.; Alastuey, A.; Viana, M.M.; Querol, X. Studies of air pollution by particulate matter in the Canary Islands for the period 2007–2010. Air Qual. Rep. 2010. [Google Scholar]
- García, M.I.; Rodríguez, S.; Alastuey, A. Impact of North America on the aerosolcomposition in the North Atlantic free troposphere. Atmos. Chem. Phys. 2017, 17, 7387–7404. [Google Scholar] [CrossRef]
- Alonso-Pérez, S.; Cuevas, E.; Querol, X.; Guerra, J.C.; Pérez, C. African dust source regions for observed dust outbreaks over the Subtropical Eastern North Atlantic region, above 25° N. J. Arid Environ. 2012, 78, 100–109. [Google Scholar] [CrossRef]
- Tsamalis, C.; Chédin, A.; Pelon, J.; Capelle, V. The seasonal vertical distribution of the Saharan Air Layer and its modulation by the wind. Atmos. Chem. Phys. 2013, 13, 11235–11257. [Google Scholar] [CrossRef]
- Alastuey, A.; Querol, X.; Castillo, S.; Escudero, M.; Avila, A.; Cuevas, E.; Torres, C.; Romero, P.M.; Exposito, F.; Garcia, O.; et al. Characterisation of TSP and PM2.5 at Izaña and Sta. Cruz de Tenerife (Canary Islands, Spain) during a Saharan dust episode (July 2002). Atmos. Environ. 2005, 39, 4715–4728. [Google Scholar] [CrossRef]
- Dominguez-Rodriguez, A.; Rodríguez, S.; Abreu-Gonzalez, P.; Avanzas, P.; Juarez-Prera, R.A. Black carbon exposure, oxidative stress markers and major adverse cardiovascular events in patients with acute coronary syndromes. Int. J. Cardiol. 2015, 188, 47–49. [Google Scholar] [CrossRef] [PubMed]
- Linares, C.; Tobías, A.; Díaz, J. Is there new scientific evidence to justify reconsideration of the current WHO guidelines for particulate matter during dust intrusions? Sci. Total Environ. 2010, 408, 2283–2284. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| HF Mortality (n = 49) | HF no Mortality (n = 780) | p-Value | |
|---|---|---|---|
| Age, year | 73.5 ± 2 | 73.8 ± 1.5 | 0.25 |
| Female sex | 13 (26.5) | 220 (28.2) | 0.80 |
| Cardiovascular risk factors | |||
| Hypertension | 25 (51) | 500 (64.1) | 0.06 |
| Smoking | 24 (49) | 413 (52.9) | 0.58 |
| Diabetes mellitus | 20 (40.8) | 339 (43.5) | 0.71 |
| Hypercholesterolemia | 30 (61.2) | 454 (58.2) | 0.67 |
| Medical history | |||
| Previous HF episode | 33 (67.3) | 462 (59.2) | 0.26 |
| Previous chronic IHD | 8 (16.3) | 179 (22.9) | 0.28 |
| Atrial fibrillation | 10 (20.4) | 242 (31) | 0.11 |
| COPD | 12 (24.5) | 126 (16.2) | 0.12 |
| Biochemistry | |||
| Hemoglobin (g/dL) | 11.95 ± 1.65 | 11.73 ± 1.73 | 0.37 |
| BNP (pg/mL) | 1295.8 (937.8–1769) | 1339.6 (925.6-1961.8) | 0.29 |
| Sodium (mg/dL) | 138.31 ± 2.88 | 138.32 ± 3.15 | 0.98 |
| Clinical data | |||
| LVEF (%) | 49.47 ± 12.40 | 50.86 ± 11.04 | 0.39 |
| Hospital stay (d) | 10.59 ± 3.67 | 10.37 ± 3.77 | 0.66 |
| Charlson index | 4.73 ± 0.78 | 4.71 ± 0.74 | 0.84 |
| HF precipitating factors | 0.73 | ||
| Therapeutic non-compliance | 2 (4) | 59 (7.9) | |
| Rapid atrial fibrillation | 25 (52.1) | 365 (48.8) | |
| Infections | 12 (25) | 208 (27.7) | |
| Unknown precipitating factors | 14 (28.5) | 144 (18.4) | |
| In-hospital treatment | |||
| Furosemide | 49 (100) | 780 (100) | - |
| Spironolactone / Eplerenone | 31 (63.3) | 499 (64) | 0.92 |
| Beta blockers | 32 (65.3) | 462 (59.5) | 0.41 |
| ACEI | 36 (73.5) | 540 (69.2) | 0.53 |
| ARA-II | 13 (26.5) | 240 (30.8) | 0.53 |
| Number of patients exposed to PM10 ≥ 50 μg/m3 during Saharan dust events | 42 (85.7) | 318 (40.8) | <0.0001 |
| PM10 (μg/m3) | 84.7 (71.5–95.8) | 15.3 (9.7–26.4) | <0.0001 |
| PM2.5 (μg/m3) | 29.9 (23.3–36.1) | 6.9 (5.6–12.5) | <0.0001 |
| PM2.5-10 (μg/m3) | 57.6 (37.5–68.8) | 8.3 (5.6–13.9) | <0.0001 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dominguez-Rodriguez, A.; Baez-Ferrer, N.; Rodríguez, S.; Avanzas, P.; Abreu-Gonzalez, P.; Terradellas, E.; Cuevas, E.; Basart, S.; Werner, E. Saharan Dust Events in the Dust Belt -Canary Islands- and the Observed Association with in-Hospital Mortality of Patients with Heart Failure. J. Clin. Med. 2020, 9, 376. https://doi.org/10.3390/jcm9020376
Dominguez-Rodriguez A, Baez-Ferrer N, Rodríguez S, Avanzas P, Abreu-Gonzalez P, Terradellas E, Cuevas E, Basart S, Werner E. Saharan Dust Events in the Dust Belt -Canary Islands- and the Observed Association with in-Hospital Mortality of Patients with Heart Failure. Journal of Clinical Medicine. 2020; 9(2):376. https://doi.org/10.3390/jcm9020376
Chicago/Turabian StyleDominguez-Rodriguez, Alberto, Néstor Baez-Ferrer, Sergio Rodríguez, Pablo Avanzas, Pedro Abreu-Gonzalez, Enric Terradellas, Emilio Cuevas, Sara Basart, and Ernest Werner. 2020. "Saharan Dust Events in the Dust Belt -Canary Islands- and the Observed Association with in-Hospital Mortality of Patients with Heart Failure" Journal of Clinical Medicine 9, no. 2: 376. https://doi.org/10.3390/jcm9020376
APA StyleDominguez-Rodriguez, A., Baez-Ferrer, N., Rodríguez, S., Avanzas, P., Abreu-Gonzalez, P., Terradellas, E., Cuevas, E., Basart, S., & Werner, E. (2020). Saharan Dust Events in the Dust Belt -Canary Islands- and the Observed Association with in-Hospital Mortality of Patients with Heart Failure. Journal of Clinical Medicine, 9(2), 376. https://doi.org/10.3390/jcm9020376